

Is Greater Social Support from Parents and Friends Related to Higher Physical Activity Levels among Adolescents?
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Gender, Age, Body Mass Index, Biological Maturation, Education, Socioeconomic Status
2.2. Social Support from Parents or Guardians and Friends
2.3. Adolescents’ Moderate-to-Vigorous Physical Activity (MVPA)
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide Trends in Body-Mass Index, Underweight, Overweight, and Obesity from 1975 to 2016: A Pooled Analysis of 2416 Population-Based Measurement Studies in 128.9 Million Children, Adolescents, and Adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Aubert, S.; Barnes, J.D.; Abdeta, C.; Nader, P.A.; Adeniyi, A.F.; Aguilar-Farias, N.; Tenesaca, D.S.A.; Bhawra, J.; Brazo-Sayavera, J.; Cardon, G.; et al. Global Matrix 3.0 Physical Activity Report Card Grades for Children and Youth: Results and Analysis from 49 Countries. J. Phys. Act. Health 2018, 15, S251–S273. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Hermoso, A.; López-Gil, J.F.; Ramírez-Vélez, R.; Alonso-Martínez, A.M.; Izquierdo, M.; Ezzatvar, Y. Adherence to aerobic and muscle-strengthening activities guidelines: A systematic review and meta-analysis of 3.3 million participants across 32 countries. Br. J. Sports Med. 2023, 57, 225–229. [Google Scholar] [CrossRef]
- Laird, Y.; Fawkner, S.; Kelly, P.; McNamee, L.; Niven, A. The role of social support on physical activity behavior in adolescent girls: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 79. [Google Scholar] [CrossRef] [Green Version]
- Laird, Y.; Fawkner, S.; Niven, A. A grounded theory of how social support influences physical activity in adolescent girls. Int. J. Qual. Stud. Health Well-Being 2018, 13, 1435099. [Google Scholar] [CrossRef] [Green Version]
- Tcymbal, A.; Demetriou, Y.; Kelso, A.; Wolbring, L.; Wunsch, K.; Wäsche, H.; Woll, A.; Reimers, A.K. Effects of the built environment on physical activity: A systematic review of longitudinal studies taking sex/gender into account. Environ. Health Prev. Med. 2020, 25, 75. [Google Scholar] [CrossRef]
- Nordbø, E.C.A.; Nordh, H.; Raanaas, R.K.; Aamodt, G. Promoting activity participation and well-being among children and adolescents: A systematic review of neighborhood built-environment determinants. JBI Évid. Synth. 2020, 18, 370–458. [Google Scholar] [CrossRef]
- Tassitano, R.M.; Weaver, R.G.; Tenório, M.C.M.; Brazendale, K.; Beets, M.W. Physical activity and sedentary time of youth in structured settings: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 160. [Google Scholar] [CrossRef] [PubMed]
- Rosselli, M.; Ermini, E.; Tosi, B.; Boddi, M.; Stefani, L.; Toncelli, L.; Modesti, P.A. Gender differences in barriers to physical activity among adolescents. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1582–1589. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Andrés, M.; Bartolomé-Gutiérrez, R.; Rodríguez-Martín, B.; Pardo-Guijarro, M.J.; Garrido-Miguel, M.; Martínez-Vizcaíno, V. Barriers and Facilitators to Leisure Physical Activity in Children: A Qualitative Approach Using the Socio-Ecological Model. Int. J. Environ. Res. Public Health 2020, 17, 3033. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C. A review of correlates of physical activity of children and adolescents. Med. Sci. Sports Exerc. 2000, 32, 963–975. [Google Scholar] [CrossRef]
- Sallis, J.F.; Owen, N.; Fisher, E.B. Ecological models of health behavior. In Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 465–485. [Google Scholar]
- Mendonça, G.; Cheng, L.A.; Mélo, E.N.; de Farias Júnior, J.C. Physical activity and social support in adolescents: A systematic review. Health Educ. Res. 2014, 29, 822–839. [Google Scholar] [CrossRef]
- Cheng, L.A.; Mendonça, G.; Júnior, J.C.D.F. Physical activity in adolescents: Analysis of the social influence of parents and friends. J. Pediatr. 2014, 90, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Su, D.L.Y.; Tang, T.C.W.; Chung, J.S.K.; Lee, A.S.Y.; Capio, C.M.; Chan, D.K.C. Parental Influence on Child and Adolescent Physical Activity Level: A Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 16861. [Google Scholar] [CrossRef]
- Camargo, E.M.; Santos, M.P.M.; Ribeiro, A.G.P.; Mota, J.; de Campos, W. Interação dos fatores sociodemográficos na associação entre fatores psicossociais e transporte ativo para a escola. Cad. Saúde Pública 2020, 36, e00102719. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behavior. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Chaput, J.-P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO guidelines on physical activity and sedentary behavior for children and adolescents aged 5–17 years: Summary of the evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Tanner, J.M. Growth at Adolescence, 2nd ed.; Blackwell: Oxford, UK, 1962. [Google Scholar]
- Associação Brasileira de Empresas de Pesquisa; Critério de Classificação Econômica Brasil: São Paulo, Brazil, 2016; pp. 1–6.
- Farias Júnior, J.C.; Mendonça, G.; Florindo, A.A.; Barros, M.V.G. Fidedignidade e validade de uma escala de avaliação do apoio social para prática de atividade física para adolescentes: Escala ASAFA. Rev. Bras. Epidemiol. 2014, 17, 355–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Júnior, J.C.D.F.; Lopes, A.D.S.; Mota, J.; Santos, M.P.; Ribeiro, J.; Hallal, P.C. Validade e reprodutibilidade de um questionário para medida de atividade física em adolescentes: Uma adaptação do Self-Administered Physical Activity Checklist. Rev. Bras. Epidemiol. 2012, 15, 198–210. [Google Scholar] [CrossRef] [Green Version]
- Sallis, J.F.; Strikmiller, P.K.; Harsha, D.W.; Feldman, H.A.; Ehlinger, S.; Stone, E.J.; Williston, J.; Woods, S. Validation of interviewer- and self-administered physical activity checklists for fifth grade students. Med. Sci. Sports Exerc. 1996, 28, 840–851. [Google Scholar] [CrossRef] [PubMed]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Marshall, S.J.; Biddle, S. The transtheoretical model of behavior change: A meta-analysis of applications to physical activity and exercise. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2001, 23, 229–246. [Google Scholar] [CrossRef]
- Spencer, L.; Adams, T.B.; Malone, S.; Roy, L.; Yost, E. Applying the Transtheoretical Model to Exercise: A Systematic and Comprehensive Review of the Literature. Health Promot. Pract. 2006, 7, 428–443. [Google Scholar] [CrossRef]
- Lisboa, T.; Da Silva, W.R.; Silva, D.A.S.; Felden, P.G.; Pelegrini, A.; Lopes, J.d.J.D.; Beltrame, T.S. Social support from family and friends for physical activity in adolescence: Analysis with structural equation modeling. Cad. Saude Publica 2021, 37, e00196819. [Google Scholar] [CrossRef]
- Khan, A.; Uddin, R. Parental and peer supports are associated with an active lifestyle of adolescents: Evidence from a population-based survey. Public Health 2020, 188, 1–3. [Google Scholar] [CrossRef]
- Lawler, M.; Heary, C.; Nixon, E. Peer Support and Role Modeling Predict Physical Activity Change among Adolescents over Twelve Months. J. Youth Adolesc. 2020, 49, 1503–1516. [Google Scholar] [CrossRef]
- Petersen, T.L.; Møller, L.B.; Brønd, J.C.; Jepsen, R.; Grøntved, A. Association between parent and child physical activity: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 67. [Google Scholar] [CrossRef]
- Pluta, B.; Korcz, A.; Krzysztoszek, J.; Bronikowski, M.; Bronikowska, M. Associations between adolescents’ physical activity behavior and their perceptions of parental, peer and teacher support. Arch. Public Health = Arch. Belg. Sante Publique 2020, 78, 106. [Google Scholar] [CrossRef] [PubMed]
- Messing, S.; Rütten, A.; Abu-Omar, K.; Ungerer-Röhrich, U.; Goodwin, L.; Burlacu, I.; Gediga, G. How Can Physical Activity Be Promoted among Children and Adolescents? A Systematic Review of Reviews across Settings. Front. Public Health 2019, 7, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoehner, C.M.; Ribeiro, I.C.; Parra, D.C.; Reis, R.S.; Azevedo, M.R.; Hino, A.A.; Soares, J.; Hallal, P.C.; Simões, E.J.; Brownson, R.C. Physical Activity Interventions in Latin America: Expanding and classifying the evidence. Am. J. Prev. Med. 2013, 44, e31–e40. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | Male (n = 875; 44.1%) | Female (n = 1109; 55.9%) | Total | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | p * | n | % | ||
| Age | 15 years | 261 | 41.8 | 363 | 58.2 | 0.124 | 624 | 31.5 |
| 16 years | 317 | 44.3 | 399 | 55.7 | 716 | 36.1 | ||
| 17 years | 297 | 46.1 | 347 | 53.9 | 644 | 32.4 | ||
| BMI ¥ | No excess weight | 744 | 85.0 | 996 | 89.8 | 0.001 | 1740 | 87.7 |
| Excess weight | 131 | 15.0 | 113 | 10.2 | 244 | 12.3 | ||
| Father’s Education | Up to Elementary School | 238 | 38.1 | 387 | 61.9 | 0.003 | 625 | 31.5 |
| High School | 405 | 47.2 | 453 | 52.8 | 858 | 43.2 | ||
| University | 232 | 46.3 | 269 | 53.7 | 501 | 25.3 | ||
| Mother’s Education | Up to Elementary School | 245 | 39.0 | 384 | 61.0 | 0.006 | 629 | 31.7 |
| High School | 398 | 46.3 | 461 | 53.7 | 859 | 43.3 | ||
| University | 232 | 46.8 | 264 | 53.2 | 496 | 25.0 | ||
| SES | Low | 140 | 40.0 | 210 | 60.0 | 0.005 | 350 | 17.6 |
| Intermediate | 538 | 43.4 | 702 | 56.6 | 1240 | 62.5 | ||
| High | 197 | 50.0 | 197 | 50.0 | 394 | 19.9 | ||
| Social Support | Male (n = 875; 44.1%) | Female (n = 1109; 55.9%) | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | p * | n | % | % | ||
| Parents: To Encourage | Never | 170 | 19.4 | 240 | 21.6 | 0.285 | 410 | 20.7 | 100 |
| Sometimes | 473 | 54.1 | 604 | 54.3 | 1077 | 54.3 | |||
| Always | 232 | 26.5 | 265 | 23.9 | 497 | 25.0 | |||
| Parents: To Practice | Never | 322 | 36.8 | 455 | 41.0 | 0.086 | 777 | 39.2 | 100 |
| Sometimes | 434 | 49.6 | 530 | 47.8 | 964 | 48.6 | |||
| Always | 119 | 13.6 | 124 | 11.2 | 243 | 12.2 | |||
| Parents: To Transport | Never | 425 | 48.6 | 541 | 48.8 | 0.443 | 966 | 48.7 | 100 |
| Sometimes | 262 | 29.9 | 353 | 31.8 | 615 | 31.0 | |||
| Always | 188 | 21.5 | 215 | 19.4 | 403 | 20.3 | |||
| Parents: To Attend | Never | 370 | 42.3 | 500 | 45.1 | 0.382 | 870 | 43.9 | 100 |
| Sometimes | 365 | 41.7 | 450 | 40.6 | 815 | 41.1 | |||
| Always | 140 | 07.1 | 159 | 08.0 | 299 | 15.0 | |||
| Parents: To Comment | Never | 324 | 37.0 | 449 | 40.5 | 0.059 | 773 | 39.0 | 100 |
| Sometimes | 341 | 39.0 | 375 | 33.8 | 716 | 36.1 | |||
| Always | 210 | 24.0 | 285 | 25.7 | 495 | 24.9 | |||
| Friends: To Encourage | Never | 324 | 37.0 | 445 | 40.1 | 0.370 | 769 | 38.8 | 100 |
| Sometimes | 355 | 40.6 | 426 | 38.4 | 781 | 39.4 | |||
| Always | 196 | 22.4 | 238 | 21.5 | 434 | 21.8 | |||
| Friends: To Practice | Never | 229 | 26.2 | 348 | 31.4 | 0.019 * | 577 | 29.1 | 100 |
| Sometimes | 370 | 42.3 | 460 | 41.5 | 830 | 41.8 | |||
| Always | 276 | 31.5 | 301 | 7.1 | 577 | 29.1 | |||
| Friends: To Invite | Never | 243 | 27.8 | 376 | 33.9 | 0.014 * | 619 | 31.2 | 100 |
| Sometimes | 381 | 43.5 | 440 | 39.7 | 821 | 41.4 | |||
| Always | 251 | 28.7 | 293 | 26.4 | 544 | 27.4 | |||
| Friends: To Attend | Never | 421 | 48.1 | 520 | 46.9 | 0.748 | 941 | 47.4 | 100 |
| Sometimes | 309 | 35.3 | 410 | 37.0 | 719 | 36.2 | |||
| Always | 145 | 16.6 | 179 | 16.1 | 324 | 16.4 | |||
| Friends: To Comment | Never | 425 | 48.6 | 566 | 51.0 | 991 | 49.9 | 100 | |
| Sometimes | 308 | 35.2 | 363 | 32.7 | 671 | 33.9 | |||
| Always | 142 | 16.2 | 180 | 16.2 | 322 | 16.2 | |||
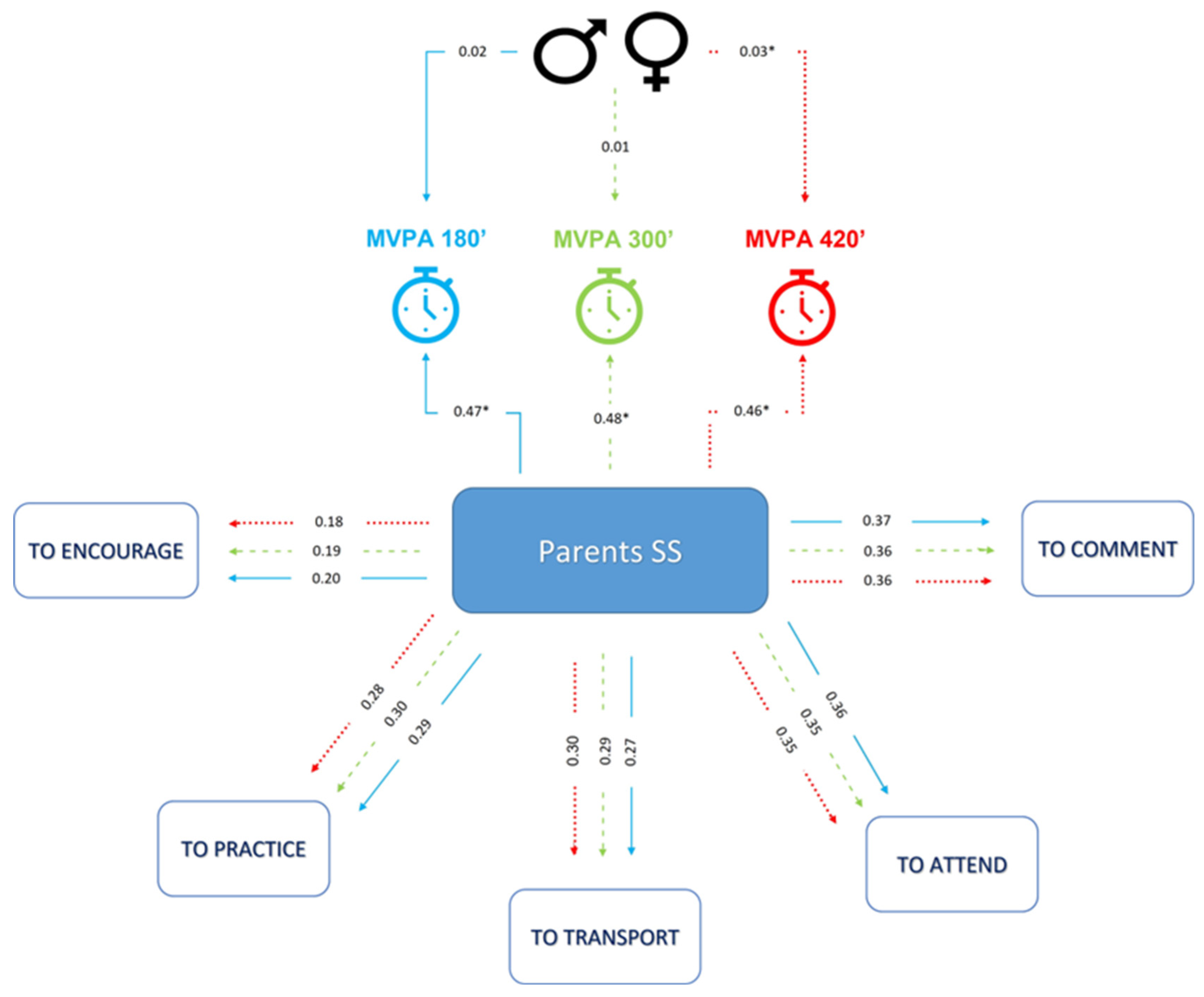
| Physical Activity Duration | Social Support | Direct Effect | p |
|---|---|---|---|
| 180 min/week | Parents | 0.1467 | <0.001 |
| Gender | 0.022 | 0.080 | |
| 300 min/week | Parents | 0.478 | <0.001 |
| Gender | 0.014 | 0.140 | |
| 420 min/week | Parents | 0.455 | <0.001 |
| Gender | 0.026 | <0.001 | |
| 180 min/week | Friends | 0.238 | <0.001 |
| Gender | 0.028 | <0.001 | |
| 300 min/week | Friends | 0.236 | <0.001 |
| Gender | 0.021 | <0.001 | |
| 420 min/week | Friends | 0.212 | <0.001 |
| Gender | 0.032 | 0.020 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Camargo, E.M.; da Costa, C.G.; Piola, T.S.; Bacil, E.D.A.; López-Gil, J.F.; de Campos, W. Is Greater Social Support from Parents and Friends Related to Higher Physical Activity Levels among Adolescents? Children 2023, 10, 701. https://doi.org/10.3390/children10040701
de Camargo EM, da Costa CG, Piola TS, Bacil EDA, López-Gil JF, de Campos W. Is Greater Social Support from Parents and Friends Related to Higher Physical Activity Levels among Adolescents? Children. 2023; 10(4):701. https://doi.org/10.3390/children10040701
Chicago/Turabian Stylede Camargo, Edina Maria, Cristiane Galvão da Costa, Thiago Silva Piola, Eliane Denise Araújo Bacil, José Francisco López-Gil, and Wagner de Campos. 2023. "Is Greater Social Support from Parents and Friends Related to Higher Physical Activity Levels among Adolescents?" Children 10, no. 4: 701. https://doi.org/10.3390/children10040701