
The Emotional Experience of Caring for Children in Pediatric Palliative Care: A Qualitative Study among a Home-Based Interdisciplinary Care Team
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Study Setting
2.3. Participants, Sampling Strategies, and Sample
2.4. Data Collection
2.5. Data Analysis
2.6. Rigor and Quality Criteria
2.7. Ethical Considerations
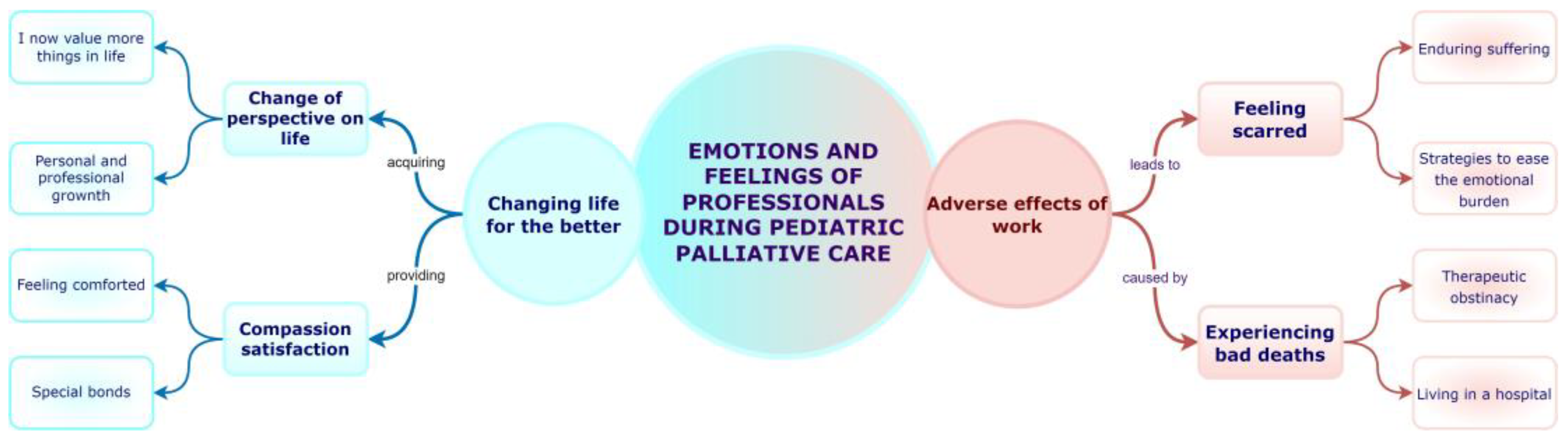
3. Results
3.1. Theme 1: Changing Life for the Better
3.1.1. Sub-Theme: Change of Perspective on Life
I Now Value More Things in Life
EPAD1: “I believe that it makes you value other things in your life more, it makes you say: “It’s good that I have a family, it’s good that they are well and it’s good that they are not affected by this type of disease. Because it is a physical and emotional wear and tear, not only for the patient, but also for everything it entails, which influences your professional, family, and social life.”
EPE5: “When you work here, when you see real dramas, you relativize. You relativize because you think that maybe a problem that you may have personally or a problem that may arise at work is not so important; and your priorities change. Your way of understanding the world changes, because you put on other lenses for your life. It teaches you to enjoy small moments that you didn’t notice before.”
EPE1: “One of the things I like the most about palliative work is that in the end it brings you face to face with what is most human. I have seen love scenes that I haven’t seen anywhere else. Parents with their children, between siblings, and between couples […] I have some scenes engraved in my head, of parents saying goodbye to their children, talking to them at the moment of death…of a love, of a generosity…that I say: God, how are they capable of doing that?”
Personal and Professional Growth
EPE5: “You can stop and think. Having a profession where one of the things you have to do as a professional is to stop and talk to yourself and stop and analyze how you feel and work through your feelings, well, I can’t think of many professions where that’s a requirement.”
EPM3: “It changes your outlook on life, if you see the people who work in palliative care, almost all of us tend to be quite nice, kind, and happy people, because I think you learn to value things: those that are important, those that aren’t, and to give them more value. You learn not to leave things for tomorrow; you see people dying every day, so you think: I could be next. You perceive life more intensely.”
EPE4: “It has changed me on a professional level, because it has made me learn more, it has made me try to be a better nurse, because they are very complex children and they require care that I, as a nurse, have had to learn little by little. Here I have been able to feel like a real nurse working. In other places where I have worked I felt more like a mere dispenser of medication, and here I feel that I can develop my profession much more because parents and children need care and a lot of health education.”
3.1.2. Sub-Theme: Compassion Satisfaction
Feeling Comforted
EPM1: “As painful as it is to have a child die, which I think is the most painful thing that can happen to someone, the fact that this makes it a little easier, a little more humane and less painful, comforts me.”
EPE3: “When you give, you are much happier. So, these children have given me life, they die, but they give me life. I am sure that these children leave a legacy here and they leave a purpose, they are here for a reason”.
EPE4: “For me, being able to help these families who are the lame limb of the health system, the most forgotten, seems incredible to me; it is one of the things that this service offers me the most…”.
EPE3: “When our service was created, the families of children with neurological, rare or neurovegetative diseases saw us as a blessing because they were no longer alone in their chronic life process. These children did not have a specialist or a medical care figure or a team to rely on, both psychologically and socially.”
EPM4: “When a family is very afraid of the death of their child, and you think it’s going to be a catastrophe, and then they tell you: he died peacefully, I’m happy despite what happened. Those are things you learn from, it’s a wonderful experience”.
Special Bonds
EPE5: “Besides, it is very enjoyable and creates a very special bond with the families, I find it very enriching, a privilege.”
EPE3: “The relationship is much closer, much more trusting because we enter their homes. The home is the most intimate place in a family, and you go in there, they open their hearts to strangers and ultimately, you establish such a strong relationship that when you leave, they say: I miss you, you are part of my family.”
3.2. Theme 2: Adverse Effects of Work
3.2.1. Sub-Theme: Feeling Scarred
Enduring Suffering
EPE3: “There have been times when I needed to take a break and then come back, because it’s really hard. We are dedicated to seeing children and people who suffer, and with these families you have a personal history between you and them, which no one else has, and that is added to your backpack. Therefore, the moment of a child’s death is very sad, however, it is also a very special moment, of introspection, of trying to give peace to that uneasiness that they have, the problem is that it also tires you, more than tiring, it leaves a scar...”
EPM5: “…the first patient that I saw die, I have the face, the expression engraved in my mind. It was in a nursing home, a child with a neurological disease and the nurse who had been on the team for a little longer, you know, she had to pull me along, encouraging me.”
EPE3: “Sometimes I think about it and I say: well, I think I’ve done my job, I’ve been doing it for a long time, let others come and follow... but then I have a conscience that tells me: don’t leave these children, are you going to leave them, are you going to abandon me too? Then you say: I’m not leaving! But many times it’s hard for me because of the work with the families who cry a lot at the end and you say: My God, I can’t do it anymore, I’m going to leave”.
Strategies to Ease the Emotional Burden
EPM6: “It is a different job because it’s a patient that you are going to see continuously, and when he’s ill, which is perhaps when you feel the most burdened, you have to see him even more. Therefore, there is less time to disconnect. So, it’s a more demanding job because it’s a child that you see many times, it’s a family with whom you talk many times about how the disease is worse, the symptoms are less easily controlled. These are very dense issues and you have an overload, but being able to count on another colleague who can stand in for you on the day when your neuron is frayed, in that sense it does help a lot.”
EPM4: “We also have strategies to get people’s pain out in the open: we have bereavement meetings to be able to express dissatisfactions, doubts, pains related to death, or the relationship with another partner, the family. You have to have strategies for airing unresolved conflicts or grief.”
EPTS2: “When I became pregnant, I informed the chief of service and told him: I don’t know if I will be able to continue doing this job when I become a mother. Because I thought I was going to put myself in the position of a mother instead of a professional, I was going to see my children dying and I was going to feel very sensitive. Then, in the end, I became a mother and it was very good for me to ask for a leave of absence, because I think this job is a big sacrifice and to have time to rest and to have long vacations, which are necessary in order to truly disconnect, a week’s vacation is not enough.”
3.2.2. Sub-Theme: Experiencing Bad Deaths
EPM4: “Here, in intensive care, I experienced very bad deaths with lack of information to the families, deaths without physical contact with the child, and in intensive care in Switzerland I experienced something very different: information, withdrawal of measures, I discovered the accompaniment of death thanks to the professionals there. That made me question things and I said: I want to do something about it when I come back. As I say: here I learned to intubate and there I learned to extubate.”
Therapeutic Obstinacy
EPE4: “In the ICU I have also seen a lot of obstinance, seeing intubated children in which most of the nursing staff suffered because they were undergoing another transplant, because they were dying badly, and they did not get to palliative care, not even close. What struck me most was the oncology part of the ICU, of transplants, of hemofilters, of going on and on, until they die badly, the parents in a bad way and the children even worse.”
EPM6: “In oncology patients there is brutal therapeutic obstinacy because it is very difficult to give up. Neurological children are different because they are children who are already born with a serious problem and who have had a serious problem all their lives. A child with cancer is a healthy child and suddenly a devastating disease appears that destroys all the grand schemes created up to that moment, but you do have the memory of a healthy child.”
Living in a Hospital
EPM7: “Seeing the suffering of children in the ICU, meeting many children who were born in a hospital and died in a hospital without going home, and who may have had minimal moments of wakefulness because they had to be sedated for multiple heart surgeries, complications of prematurity, children who have not been able to meet their siblings because they could not leave home and a child cannot enter an ICU, such as a sibling. When I saw that this existed, I said to myself: palliative care should help the child to live as a child! If you know he isn’t going to be cured, don’t condemn him to live in a hospital.”
4. Discussion
4.1. Theme 1: Changing Life for the Better
4.2. Theme 2: Adverse Effects of Work
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chambers, L. A Guide to Children’s Palliative Care: Supporting Babies, Children and Young People with Life-Limiting and Life-Threatening Conditions and Their Families, 4th ed.; Goldman, D.A., Ed.; Together for Short Lives: Bristol, UK, 2018; ISBN 189844739X. [Google Scholar]
- Benini, F.; Papadatou, D.; Bernadá, M.; Craig, F.; De Zen, L.; Downing, J.; Drake, R.; Friedrichsdorf, S.; Garros, D.; Giacomelli, L.; et al. International Standards for Pediatric Palliative Care: From IMPaCCT to GO-PPaCS. J. Pain Symptom Manag. 2022, 63, e529–e543. [Google Scholar] [CrossRef] [PubMed]
- Kase, S.M.; Waldman, E.D.; Weintraub, A.S. A Cross-Sectional Pilot Study of Compassion Fatigue, Burnout, and Compassion Satisfaction in Pediatric Palliative Care Providers in the United States. Palliat. Support. Care 2019, 17, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Rourke, M.T. Compassion Fatigue in Pediatric Palliative Care Providers. Pediatr. Clin. N. Am. 2007, 54, 631–644. [Google Scholar] [CrossRef]
- Groh, G.; Feddersen, B.; Führer, M.; Domenico Borasio, G. Specialized Home Palliative Care for Adults and Children: Differences and Similarities. J. Palliat. Med. 2014, 17, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee on Palliative and End-of-Life Care for Children and Their Families. When Children Die: Improving Palliative and End-of-Life Care for Children and Their Families; Field, M., Behrman, R., Eds.; National Academies Press: Washington, DC, USA, 2003; ISBN 978-0-309-08437-6.
- Jonas, D.; Scanlon, C.; Rusch, R.; Ito, J.; Joselow, M. Bereavement After a Child’s Death. Child Adolesc. Psychiatr. Clin. N. Am. 2018, 27, 579–590. [Google Scholar] [CrossRef]
- Figley, C. Compassion Fatigue as Secondary Traumatic Stress Disorder: An Overview. In Compassion Fatigue; Figley, C.R., Ed.; Taylor & Francis Group: New York, NY, USA, 1995; pp. 1–20. [Google Scholar]
- Maslach, C.; Jackson, S.E. The Measurement of Experienced Burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Stamm, B. Measuring Compassion Satisfaction as Well as Fatigue: Developmental History of the Compassion Satisfaction and Fatigue Test. In Treating Compassion Fatigue; Routledge: New York, NY, USA, 2002; pp. 107–119. [Google Scholar]
- Korones, D.N. Pediatric Palliative Care. Pediatr. Rev. 2007, 28, e46–e56. [Google Scholar] [CrossRef]
- Korzeniewska-Eksterowicz, A.; Przysło, Ł.; Grzelewski, T.; Stolarska, M.; Młynarski, W.; Stelmach, I.; Krakowiak, J.; Stelmach, W. Job Satisfaction among Health Professionals of Home Hospice for Children of Lodz Region. Adv. Palliat. Med. 2010, 9, 67–72. [Google Scholar]
- Liben, S.; Papadatou, D.; Wolfe, J. Paediatric Palliative Care: Challenges and Emerging Ideas. Lancet 2008, 371, 852–864. [Google Scholar] [CrossRef]
- McConnell, T.; Porter, S. The Experience of Providing End of Life Care at a Children’s Hospice: A Qualitative Study. BMC Palliat. Care 2017, 16, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for Reporting Qualitative Research: A Synthesis of Recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Yin, R.K. Case Study Research: Design and Methods, 4th ed.; SAGE: Thousand Oaks, CA, USA, 2009; ISBN 1412960991/9781412960991. [Google Scholar]
- Pope, C.; Mays, N. Qualitative Research in Health Care; Blackwell Publishing: Oxford, UK, 2006. [Google Scholar]
- Yin, R.K. Case Study Research: Design and Methods, 3rd ed.; SAGE: Thousand Oaks, CA, USA, 2003; Available online: https://books.google.es/books?id=BWea_9ZGQMwC&printsec=frontcover&hl=es#v=onepage&q&f=false (accessed on 27 April 2021)ISBN 076192552X/9780761925521.
- Vanwynsberghe, R.; Khan, S. Redefining Case Study. Int. J. Qual. Methods 2007, 6, 80–94. [Google Scholar] [CrossRef]
- Stake, R.E. The Art of Case Study Research. Available online: https://books.google.es/books?id=ApGdBx76b9kC&printsec=frontcover&dq=The+art+of+case+study+research&hl=es&sa=X&ved=2ahUKEwiI2Pz5mZ7wAhWrxIUKHcnsCWoQ6AEwAHoECAAQAg#v=onepage&q=Theartofcasestudyresearch&f=false (accessed on 27 April 2021).
- Cuidados Paliativos Pediátricos|Hospital Infantil Universitario Niño Jesús. Available online: https://www.comunidad.madrid/hospital/ninojesus/profesionales/servicios-medicos/cuidados-paliativos-pediatricos (accessed on 28 March 2023).
- Creswell, J.W.; Poth, C. Qualitative Inquiry & Research Design: Choosing among Five Approaches, 4th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2018; ISBN 1506330207. [Google Scholar]
- Carpenter, C.; Suto, M. Qualitative Research for Occupational and Physical Therapists: A Practical Guide; Blackwell Publishing Ltd.: Oxford, UK, 2008; ISBN 978-1-4051-4435-3. [Google Scholar]
- Miles, M.; Huberman, M.; Saldaña, J. Qualitative Data Analysis: A Methods Sourcebook, 4th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2019. [Google Scholar]
- Richards, L.; Morse, J.M. Readme First for a User’s Guide to Qualitative Methods, 3rd ed.; SAGE Publications: London, UK, 2012. [Google Scholar]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- ATLAS.Ti. The Qualitative Data Analysis & Research Software. Available online: https://atlasti.com/ (accessed on 25 May 2022).
- Software de Hojas de Cálculo Microsoft Excel|Microsoft 365. Available online: https://www.microsoft.com/es-es/microsoft-365/excel (accessed on 25 May 2022).
- Lincoln, Y.; Guba, E. Naturalistic Inquiry; Sage Publications: Newbury Park, CA, USA, 1985; ISBN 0803924313/9780803924314. [Google Scholar]
- Shenton, A. Strategies for Ensuring Trustworthiness in Qualitative Research Projects. Educ. Inf. 2004, 22, 63–75. [Google Scholar] [CrossRef] [Green Version]
- Houghton, C.; Casey, D.; Shaw, D.; Murphy, K. Rigour in Qualitative Case-Study Research. Nurse Res. 2013, 20, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Korstjens, I.; Moser, A. Series: Practical Guidance to Qualitative Research. Part 4: Trustworthiness and Publishing. Eur. J. Gen. Pract. 2018, 24, 120–124. [Google Scholar] [CrossRef] [Green Version]
- Tedeschi, R.G.; Calhoun, L.G. Posttraumatic growth: Conceptual foundations and empirical evidence. Psychol. Inq. 2004, 15, 1–18. [Google Scholar] [CrossRef]
- Beaune, L.; Muskat, B.; Anthony, S.J. The Emergence of Personal Growth amongst Healthcare Professionals Who Care for Dying Children. Palliat. Support. Care 2017, 16, 298–307. [Google Scholar] [CrossRef]
- Vishnevsky, T.; Quinlan, M.M.; Kilmer, R.P.; Cann, A.; Danhauer, S.C. “The Keepers of Stories”: Personal Growth and Wisdom Among Oncology Nurses. J. Holist. Nurs. 2015, 33, 326–344. [Google Scholar] [CrossRef]
- Conte, T.M. The Lived Experience of Work-Related Loss and Grief among Pediatric Oncology Nurses. J. Hosp. Palliat. Nurs. 2014, 16, 40–46. [Google Scholar] [CrossRef]
- Morrison, C.F.; Morris, E.J. The Practices and Meanings of Care for Nurses Working on a Pediatric Bone Marrow Transplant Unit. J. Pediatr. Oncol. Nurs. 2017, 34, 214–221. [Google Scholar] [CrossRef] [PubMed]
- El-bar, N.; Levy, A.; Wald, H.S.; Biderman, A. Compassion Fatigue, Burnout and Compassion Satisfaction among Family Physicians in the Negev Area—A Cross-Sectional Study. Isr. J. Health Policy Res. 2013, 2, 31. [Google Scholar] [CrossRef] [Green Version]
- Weintraub, A.S.; Geithner, E.M.; Stroustrup, A.; Waldman, E.D. Compassion Fatigue, Burnout and Compassion Satisfaction in Neonatologists in the US. J. Perinatol. 2016, 36, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Baer, T.E.; Feraco, A.M.; Sagalowsky, S.T.; Williams, D.; Litman, H.J.; Vinci, R.J. Pediatric Resident Burnout and Attitudes Toward Patients. Pediatrics 2017, 139, e20162163. [Google Scholar] [CrossRef] [Green Version]
- Dréano-Hartz, S.; Rhondali, W.; Ledoux, M.; Ruer, M.; Berthiller, J.; Schott, A.M.; Monsarrat, L.; Filbet, M. Burnout among Physicians in Palliative Care: Impact of Clinical Settings. Palliat. Support. Care 2016, 14, 402–410. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Varkey, P.; Boone, S.L.; Satele, D.V.; Sloan, J.A.; Shanafelt, T.D. Physician Satisfaction and Burnout at Different Career Stages. Mayo Clin. Proc. 2013, 88, 1358–1367. [Google Scholar] [CrossRef] [Green Version]
- Dyrbye, L.N.; West, C.P.; Satele, D.; Boone, S.; Tan, L.; Sloan, J.; Shanafelt, T.D. Burnout among U.S. Medical Students, Residents, and Early Career Physicians Relative to the General U.S. Population. Acad. Med. 2014, 89, 443–451. [Google Scholar] [CrossRef] [Green Version]
- Parola, V.; Coelho, A.; Cardoso, D.; Gea-Sanchez, M.; Blanco-Blanco, J.; Apóstolo, J. The Prevalence of Burnout in Health Professionals Working in Palliative Care: A Systematic Review Protocol. JBI Database Syst. Rev. Implement. Rep. 2016, 14, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Rizo-Baeza, M.; Mendiola-Infante, S.V.; Sepehri, A.; Palazón-Bru, A.; Gil-Guillén, V.F.; Cortés-Castell, E. Burnout Syndrome in Nurses Working in Palliative Care Units: An Analysis of Associated Factors. J. Nurs. Manag. 2018, 26, 19–25. [Google Scholar] [CrossRef]
- Klassen, A.; Gulati, S.; Dix, D. Health Care Providers’ Perspectives About Working With Parents of Children With Cancer: A Qualitative Study. J. Pediatr. Oncol. Nurs. 2012, 29, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Park, B.K. The Most Important Aspects for a Good Death: Perspectives from Parents of Children with Cancer. Inquiry 2021, 58, 1–12. [Google Scholar] [CrossRef]
- Taylor, M.R.; Barton, K.S.; Kingsley, J.M.; Heunis, J.; Rosenberg, A.R. Defining a “Good Death” in Pediatric Oncology: A Mixed Methods Study of Healthcare Providers. Children 2020, 7, 86. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.J.; Dupree, C.Y. Staff Experiences with End-of-Life Care in the Pediatric Intensive Care Unit. J. Palliat. Med. 2008, 11, 986–990. [Google Scholar] [CrossRef] [PubMed]
- Jameton, A. Nursing Practice: The Ethical Issues; Prentice-Hall: Englewood Cliffs, NJ, USA, 1984; ISBN 9780136274483. [Google Scholar]
- Dryden-Palmer, K.; Moore, G.; McNeil, C.; Larson, C.P.; Tomlinson, G.; Roumeliotis, N.; Janvier, A.; Parshuram, C.S. Moral Distress of Clinicians in Canadian Pediatric and Neonatal ICUs. Pediatr. Crit. Care Med. 2020, 21, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Maytum, J.C.; Heiman, M.B.; Garwick, A.W. Compassion Fatigue and Burnout in Nurses Who Work with Children with Chronic Conditions and Their Families. J. Pediatr. Health Care 2004, 18, 171–179. [Google Scholar] [CrossRef]
- Jonas, D.F.; Bogetz, J.F. Identifying the Deliberate Prevention and Intervention Strategies of Pediatric Palliative Care Teams Supporting Providers during Times of Staff Distress. J. Palliat. Med. 2016, 19, 679–683. [Google Scholar] [CrossRef]
- Pritchard, S.; Cuvelier, G.; Harlos, M.; Barr, R. Palliative Care in Adolescents and Young Adults with Cancer. Cancer 2011, 117, 2323–2328. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Reilly, S.; Morrison, L.J.; Carey, E.; Bernacki, R.; O’Neill, L.; Kapo, J.; Periyakoil, V.S.; deLima Thomas, J. Caring for Oneself to Care for Others: Physicians and Their Self-Care. J. Support. Oncol. 2013, 11, 75–81. [Google Scholar] [CrossRef] [Green Version]
- Kobler, K. Team Support with Unexpected Death. MCN Am. J. Matern. Nurs. 2014, 39, 148–154. [Google Scholar] [CrossRef]
- Arias-Casais, N.; Garralda, E.; Rhee, J.Y.; de Lima, L.; Pons, J.J.; Clark, D.; Hasselaar, J.; Ling, J.; Mosoiu, D.; Centeno, C. EAPC Atlas of Palliative Care in Europe 2019; EAPC Press: Vilvoorde, Belgium, 2019; ISBN 9789463883443. [Google Scholar]
- Muskat, B.; Greenblatt, A.; Anthony, S.; Beaune, L.; Hubley, P.; Newman, C.; Brownstone, D.; Rapoport, A. The Experiences of Physicians, Nurses, and Social Workers Providing End-of-Life Care in a Pediatric Acute-Care Hospital. Death Stud. 2020, 44, 105–116. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Participants | Number of Participants | Data Collection Tool | Time (min) |
|---|---|---|---|
| Professionals on the specialized home-based PPC team | 7 PCD, 5 PCN, 2 PCP, 2 PCSW, 1 PCPT, 1 PCA. | 18 semi-structured interviews and field notes | Total: 940 min; mean: 58 min |
| Research Areas | Questions |
|---|---|
| Care for children with palliative care needs and their families | How do you experience caring for children with incurable diseases whose prognosis is death before adulthood? How do you experience the relationship with the child and his/her family? Could you describe the relationship you establish with the children and families you care for? What do you think is the most relevant aspect of the relationship between PPC professionals and children and their families? What feelings do you have about caring for these children and their families? Do you consider that “living with death” in the course of your work has influenced you personally or professionally? How do you experience the worsening of children? How do you experience the death of children? Could you describe any experience that you consider important during the performance of your work, and explain how it may have affected you emotionally? |
| Self-perception of the professional role in PPC | How do you think families perceive your work within PPC? How do you consider that working at PPC has influenced you personally and professionally? |
| Communication and decision making | How is information handled and shared within the team? What is most relevant? How is the process of communication with the family? How is the decision-making process carried out? |
| Criteria | Techniques Performed and Application Procedures |
|---|---|
| Credibility | Investigator triangulation: team meetings were organized during the thematic analysis, the results were compared, and the final results were identified. Member checking: post interview participant member checking consisted of offering all participants the opportunity to review the audio or written records. |
| Transferability | In-depth descriptions of the study, providing data and describing the study design and its different sections (context, research team, reflexivity process, sampling, inclusion criteria, data collection, and analysis). |
| Dependability | Audit by an external researcher, responsible for the assessment of the study protocol, with a special focus on the method and process of implementation during the study. |
| Confirmability | Investigator triangulation, data collection triangulation. The process of reflexivity was conducted through the description of the researchers’ positioning; reflective debriefing by the researchers during data collection and analysis. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rico-Mena, P.; Güeita-Rodríguez, J.; Martino-Alba, R.; Castel-Sánchez, M.; Palacios-Ceña, D. The Emotional Experience of Caring for Children in Pediatric Palliative Care: A Qualitative Study among a Home-Based Interdisciplinary Care Team. Children 2023, 10, 700. https://doi.org/10.3390/children10040700
Rico-Mena P, Güeita-Rodríguez J, Martino-Alba R, Castel-Sánchez M, Palacios-Ceña D. The Emotional Experience of Caring for Children in Pediatric Palliative Care: A Qualitative Study among a Home-Based Interdisciplinary Care Team. Children. 2023; 10(4):700. https://doi.org/10.3390/children10040700
Chicago/Turabian StyleRico-Mena, Patricia, Javier Güeita-Rodríguez, Ricardo Martino-Alba, Marina Castel-Sánchez, and Domingo Palacios-Ceña. 2023. "The Emotional Experience of Caring for Children in Pediatric Palliative Care: A Qualitative Study among a Home-Based Interdisciplinary Care Team" Children 10, no. 4: 700. https://doi.org/10.3390/children10040700