
Development and Pilot Study of a Pediatric Screening for Feeding and Swallowing Disorders in Infants and Children: The Pediatric Screening–Priority Evaluation Dysphagia (PS–PED)
 ,
,
Abstract
:1. Introduction
2. Methods
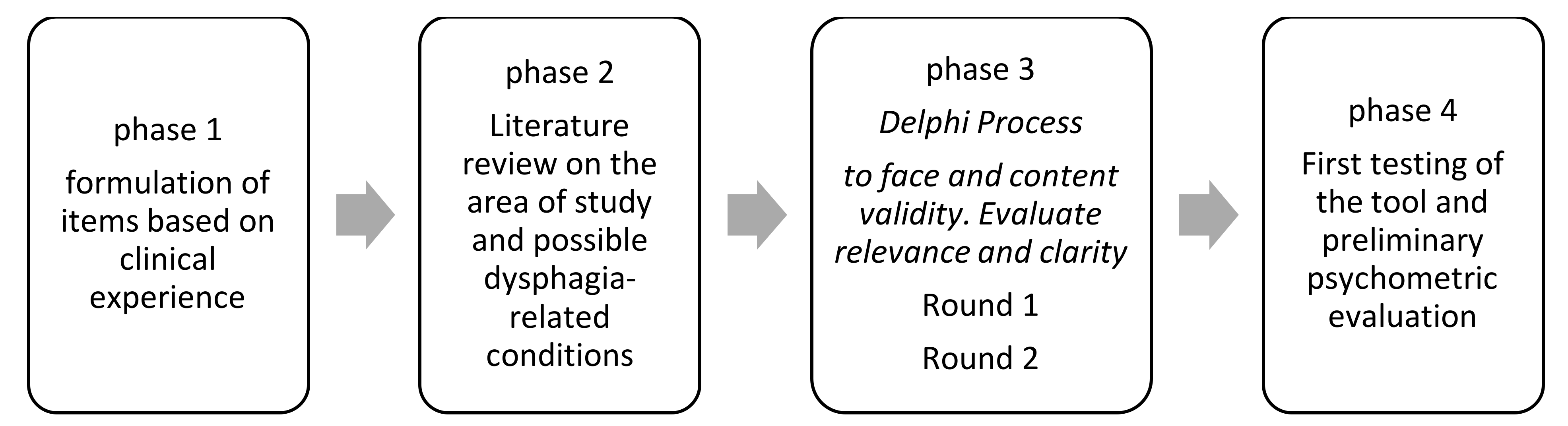
2.1. Study Design
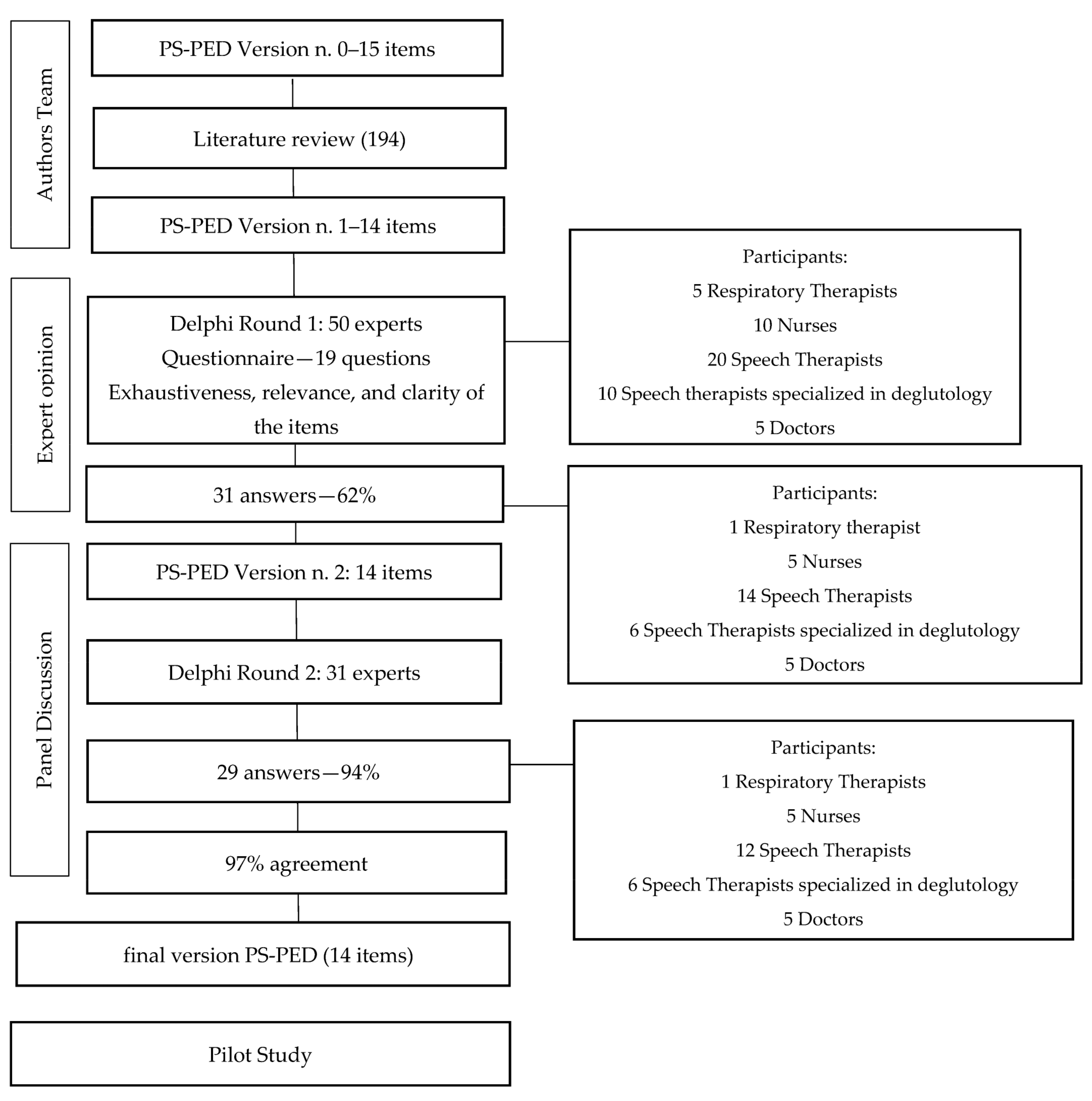
2.2. Step 1 and 2: Tool Development and Literature Review
2.3. Step 3: Modified Delphi Study
2.4. Panel Information
2.5. Step 4: Pilot Study
2.6. Translation and Cultural Adaptation
3. Results
3.1. Literature Review
3.2. Modified Delphi study
3.3. Pilot Study
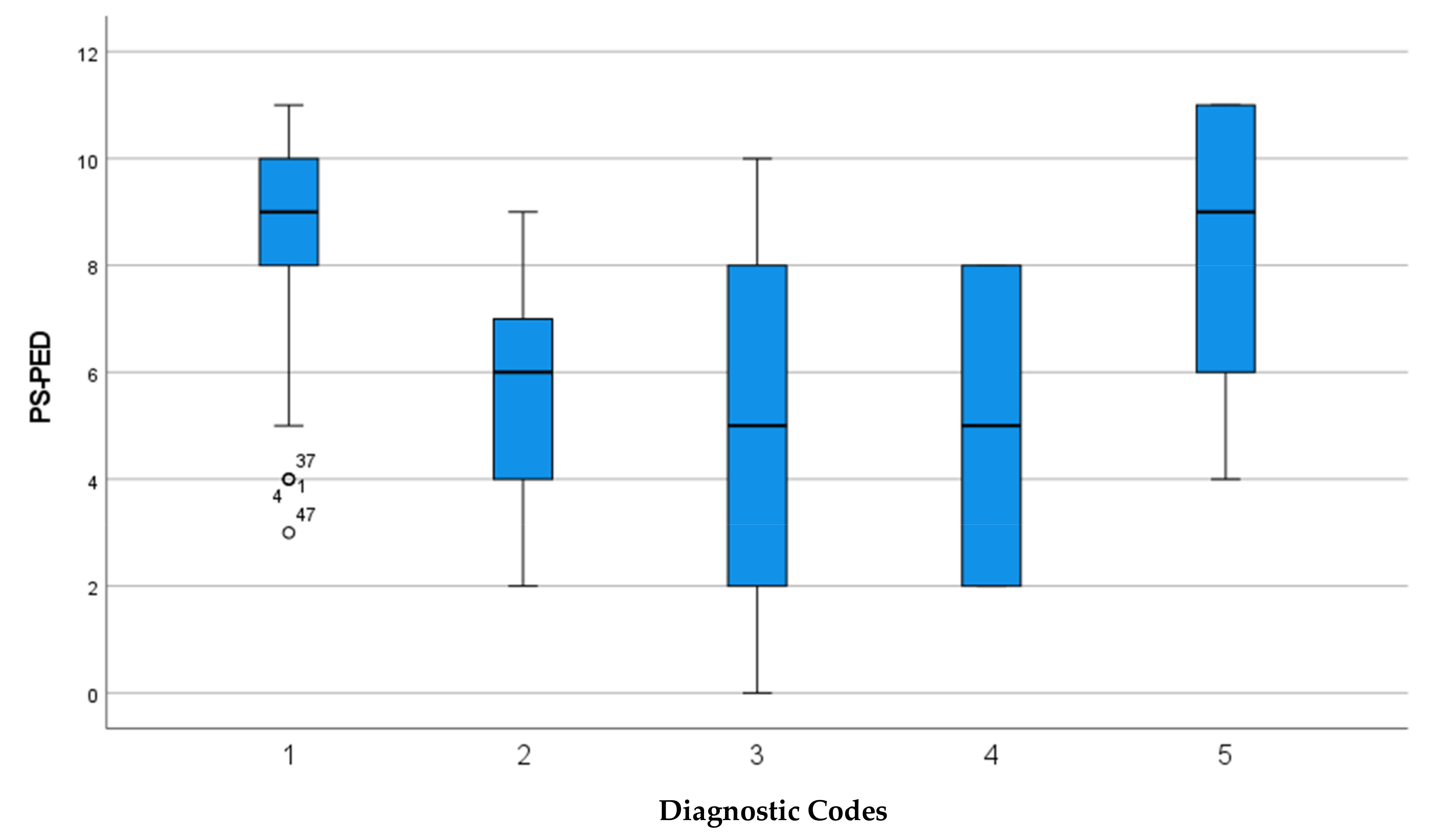
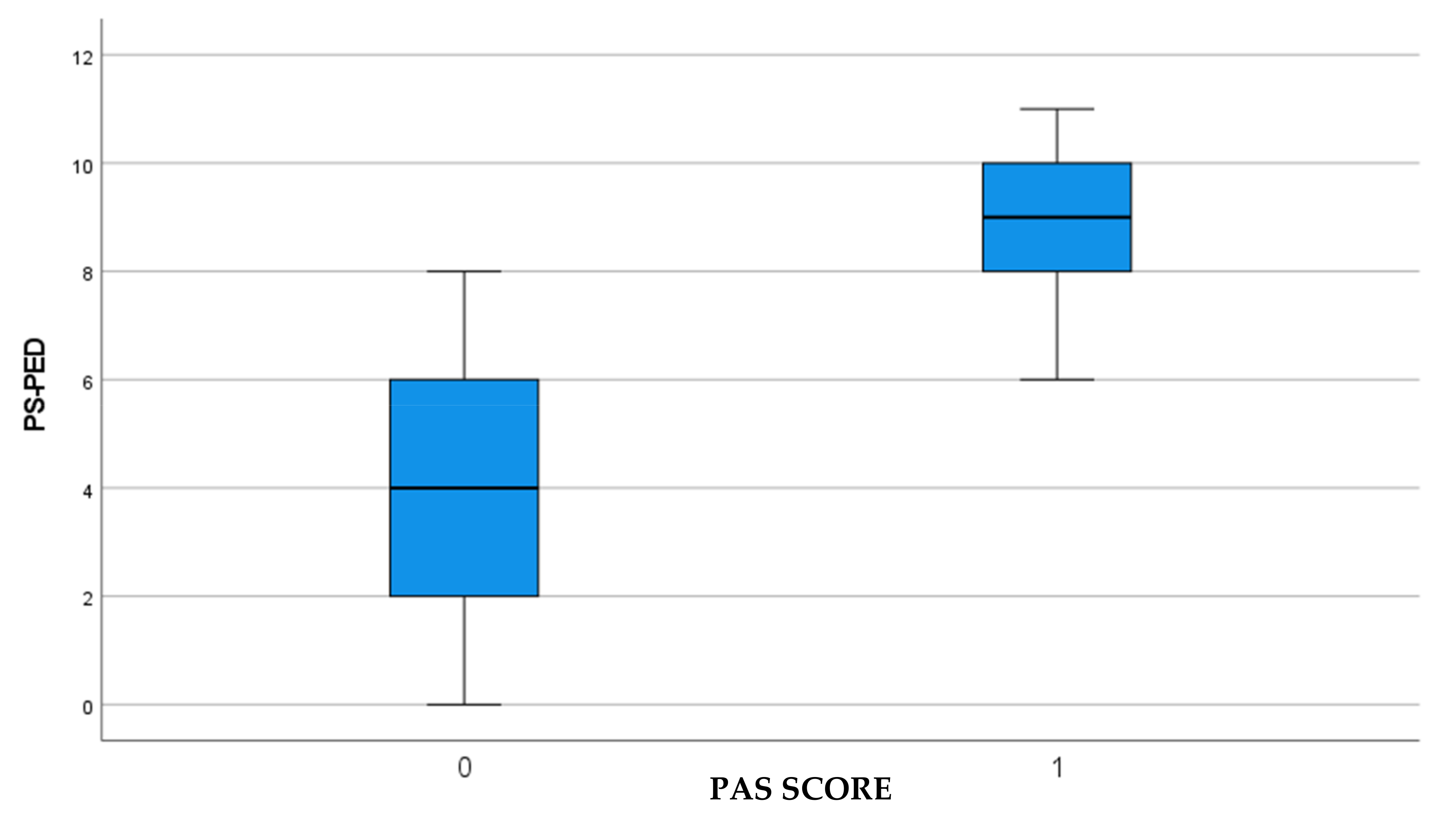
3.4. Data Analysis
4. Discussion
5. Limits
6. Future Prospects
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Duffy, K.L. Dysphagia in Children. Curr. Probl. Pediatr. Adolesc. Health Care 2018, 48, 71–73. [Google Scholar] [CrossRef] [PubMed]
- Lefton-Greif, M.; Arvedson, J. Pediatric Feeding/Swallowing: Yesterday, Today, and Tomorrow. In Seminars in Speech and Language; Thieme Medical Publishers: New York, NY, USA, 2016; Volume 37, pp. 298–309. [Google Scholar] [CrossRef]
- Horton, J.; Atwood, C.; Gnagi, S.; Teufel, R.; Clemmens, C. Temporal Trends of Pediatric Dysphagia in Hospitalized Patients. Dysphagia 2018, 33, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Steele, C.M.; Mukherjee, R.; Kortelainen, J.M.; Pölönen, H.; Jedwab, M.; Brady, S.L.; Theimer, K.B.; Langmore, S.; Riquelme, L.F.; Swigert, N.B.; et al. Development of a Non-Invasive Device for Swallow Screening in Patients at Risk of Oropharyngeal Dysphagia: Results from a Prospective Exploratory Study. Dysphagia 2019, 34, 698–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, P.A.; Santos, C.A.d.; Firmino, H.H.; Rosa, C.d.O.B. The Importance of Dysphagia Screening and Nutritional Assessment in Hospitalized Patients. Einstein 2018, 16, eAO4189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, L.; Love, C.P. Screening for Dysphagia and Aspiration in Acute Stroke: A Systematic Review. Dysphagia 2001, 16, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Speyer, R.; Cordier, R.; Parsons, L.; Denman, D.; Kim, J.-H. Psychometric Characteristics of Non-Instrumental Swallowing and Feeding Assessments in Pediatrics: A Systematic Review Using COSMIN. Dysphagia 2018, 33, 1–14. [Google Scholar] [CrossRef] [PubMed]
- American Speech-Language-Hearing Association (ASHA) 2019. Available online: https://www.asha.org/ (accessed on 13 March 2023).
- European Society for Swallowing Disorders 2012. Available online: https://essd.org/ (accessed on 23 March 2023).
- Etges, C.L.; Barbosa, L.D.R.; de Almeida, M.C.; Cardoso, F. Development of the Pediatric Dysphagia Risk Screening Instrument (PDRSI). Codas 2020, 32, e20190061. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, M.B.; Mayfield, E.B.; Gross, R.D. Clinical Decision Making in the ICU: Dysphagia Screening, Assessment, and Treatment. In Seminars in Speech and Language; Thieme Medical Publishers: New York, NY, USA, 2019; Volume 40, pp. 170–187. [Google Scholar] [CrossRef]
- Colombo, C.; Catastini, P.; Brivio, A.; Acone, B.; Dang, P.; Quattrucci, S. Delphi Poll to Assess Consensus on Issues Influencing Long-Term Adherence to Treatments in Cystic Fibrosis among Italian Health Care Professionals. Patient Prefer. Adherence 2018, 12, 2233–2241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hundleby, J.D.; Nunnally, J. Psychometric Theory. Am. Educ. Res. J. 2006, 5, 431–433. [Google Scholar] [CrossRef]
- Monticone, M.; Galeoto, G.; Berardi, A.; Tofani, M. Psychometric Properties of Assessment Tools. In Measuring Spinal Cord Injury; Springer International Publishing: Berlin/Heidelberg, Germany, 2021; pp. 7–15. [Google Scholar]
- Arvedson, J.C. Assessment of Pediatric Dysphagia and Feeding Disorders: Clinical and Instrumental Approaches. Dev. Disabil. Res. Rev. 2008, 14, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Hartnick, C.J.; Cotton, R.T. Congenital Laryngeal Anomalies. Otolaryngol. Clin. N. Am. 2000, 33, 1293–1308. [Google Scholar] [CrossRef] [PubMed]
- Onesimo, R.; Sforza, E.; Giorgio, V.; Rigante, D.; Kuczynska, E.; Leoni, C.; Agazzi, C.; Limongelli, D.; Cerchiari, A.; Tartaglia, M.; et al. Predicting the clinical trajectory of feeding and swallowing abilities in CHARGE syndrome. Eur. J. Pediatr. 2023, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Umay, E.; Eyigor, S.; Giray, E.; Karadag Saygi, E.; Karadag, B.; Durmus Kocaaslan, N.; Yuksel, D.; Demir, A.M.; Tutar, E.; Tikiz, C.; et al. Pediatric Dysphagia Overview: Best Practice Recommendation Study by Multidisciplinary Experts. World J. Pediatr. 2022, 18, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Banzato, A.; Cerchiari, A.; Pezzola, S.; Ranucci, M.; Scarfò, E.; Berardi, A.; Tofani, M.; Galeoto, G. Evaluation of the Effectiveness of Functional Chewing Training Compared with Standard Treatment in a Population of Children with Cerebral Palsy: A Systematic Review of Randomized Controlled Trials. Children 2022, 9, 1876. [Google Scholar] [CrossRef] [PubMed]
- Speyer, R.; Cordier, R.; Farneti, D.; Nascimento, W.; Pilz, W.; Verin, E.; Walshe, M.; Woisard, V. White Paper by the European Society for Swallowing Disorders: Screening and Non-Instrumental Assessment for Dysphagia in Adults. Dysphagia 2022, 37, 333–349. [Google Scholar] [CrossRef] [PubMed]
- Suiter, D.M.; Leder, S.B.; Karas, D.E. The 3-Ounce (90-Cc) Water Swallow Challenge: A Screening Test for Children with Suspected Oropharyngeal Dysphagia. Otolaryngol.-Head Neck Surg. 2009, 140, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Sung, C.K.; Damrose, E.J. Improvement in the Reflux Symptom Index Following Surgery for Cricopharyngeal Dysfunction. J. Voice 2017, 31, 86–89. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Electronic Databases |
|---|
| PubMed, Scopus, Web of Science, and CINAHL |
| Search Statements |
| Swallowing disorders OR dysphagia AND infants AND children AND tracheostomy; swallowing disorders OR dysphagia AND infants AND children AND congenital heart disease; swallowing disorders OR dysphagia AND infants AND children AND neurologic diagnosis; swallowing disorders OR dysphagia AND infants AND children AND cerebral palsy; swallowing disorders OR dysphagia AND infants AND children AND gastroesophageal reflux; swallowing disorders OR dysphagia AND infants AND children AND feeding tube; swallowing disorders OR dysphagia AND infants AND children AND time mealtime; swallowing disorders OR dysphagia AND infants AND children AND lung infection; swallowing disorders OR dysphagia AND infants AND children AND esophageal atresia; swallowing disorders OR dysphagia AND infants AND children AND epilepsy; swallowing disorders OR dysphagia AND infants AND children AND delay feeding abilities. |
| Domain | Number of Items | Items | Response SCORE | |
|---|---|---|---|---|
| YES | NO | |||
| Clinical history | 4 | 1. Neurological diagnosis | 1 | 0 |
| 2. Epilepsy medications | 1 | 0 | ||
| 3. Heart disease | 1 | 0 | ||
| 4. Structural anomalies of the digestive and respiratory systems | 1 | 0 | ||
| Health status | 7 | 5. Tracheal tube | 1 | 0 |
| 6. Decreased Alertness | 1 | 0 | ||
| 7. Malnutrition and/or poor growth | 1 | 0 | ||
| 8. Recurrent respiratory tract infections | 1 | 0 | ||
| 9. Use of the suction machine/aspirator | 1 | 0 | ||
| 10. Lack of head control and/or postural instability | 1 | 0 | ||
| 11. gastrointestinal diseases (gag reflex, vomit, constipation, GERD) | 1 | 0 | ||
| Feeding conditions | 3 | 12. Parenteral/Enteral nutrition (nasogastric tube, gastrostomy tube, etc.) | 1 | 0 |
| 13. Feeding with consistency and unsuitable food for the child’s development stage | 1 | 0 | ||
| 14. Prolonged mealtime (over 50 min) | 1 | 0 | ||
| Characteristics | n | % |
|---|---|---|
| Gender | ||
| Males | 24 | 40% |
| Females | 36 | 60% |
| Range age | 0.3 to 17 years | |
| Mean age | ||
| Standard deviation | ||
| Medical Diagnosis | ||
| 1. Neurological Neuromuscular | 27 | 45% |
| 2. Structural anomalies digestive and respiratory systems | 9 | 15% |
| 3. Other | 6 | 10% |
| 4. Heart Disease | 4 | 6% |
| 5. Genetic Syndrome | 12 | 20% |
| Domain | Items | No | Yes | ||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Clinical History | 1. Neurological diagnosis | 24 | 40.7 | 35 | 59.3 |
| 2. Epilepsy medications | 42 | 71.2 | 17 | 28.8 | |
| 3. Heart disease | 50 | 84.7 | 9 | 15.3 | |
| 4. Structural anomalies of the digestive and respiratory systems | 32 | 54.2 | 27 | 45.8 | |
| Health status | 5. Tracheal tube | 44 | 74.6 | 15 | 25.4 |
| 6. Decreased Alertness | 51 | 86.4 | 8 | 13.6 | |
| 7. Malnutrition and/or poor growth | 32 | 54.2 | 27 | 45.8 | |
| 8. Recurrent respiratory tract infections | 19 | 32.2 | 40 | 67.8 | |
| 9. Use of the suction machine/aspirator | 26 | 44.1 | 33 | 55.9 | |
| 10. Postural instability and lack of control | 24 | 40.7 | 35 | 59.3 | |
| 11. gastrointestinal diseases (gag reflex, vomit, constipation, GERD) | 18 | 30.5 | 41 | 69.5 | |
| Feeding conditions | 12. Parenteral/Enteral nutrition (nasogastric tube, gastrostomy tube, etc.) | 18 | 30.5 | 41 | 69.5 |
| 13. feeding with consistency and unsuitable food for the child’s development stage | 6 | 10.2 | 53 | 89.8 | |
| 14. Prolonged mealtime (over 50 min) | 8 | 13.6 | 51 | 86.4 | |
| Mean | Std. Deviation | Scale Mean if Item Deleted | Scale Variance if Item Deleted | Corrected Item-Total Correlation | Cronbach’s Alpha if Item Deleted | |
|---|---|---|---|---|---|---|
| Item 1 | 0.59 | 0.495 | 6.73 | 7.270 | 0.316 | 0.708 |
| Item 2 | 0.29 | 0.457 | 7.03 | 7.551 | 0.239 | 0.717 |
| Item 3 | 0.15 | 0.363 | 7.17 | 8.350 | −0.058 | 0.742 |
| Item 4 | 0.46 | 0.502 | 6.86 | 8.671 | −0.190 | 0.769 |
| Item 5 | 0.25 | 0.439 | 7.07 | 8.133 | 0.014 | 0.741 |
| Item 6 | 0.14 | 0.345 | 7.19 | 7.637 | 0.316 | 0.708 |
| Item 7 | 0.46 | 0.502 | 6.86 | 7.257 | 0.314 | 0.708 |
| Item 8 | 0.68 | 0.471 | 6.64 | 6.440 | 0.710 | 0.656 |
| Item 9 | 0.56 | 0.501 | 6.76 | 6.701 | 0.543 | 0.677 |
| Item 10 | 0.59 | 0.495 | 6.73 | 6.787 | 0.514 | 0.681 |
| Item 11 | 0.69 | 0.464 | 6.63 | 6.928 | 0.498 | 0.685 |
| Item 12 | 0.69 | 0.464 | 6.63 | 6.893 | 0.513 | 0.683 |
| Item 13 | 0.90 | 0.305 | 6.42 | 7.317 | 0.576 | 0.688 |
| Item 14 | 0.86 | 0.345 | 6.46 | 7.149 | 0.591 | 0.682 |
| Total | 7.36 | 2.92 |
| N | Mean | Std. Deviation | Std. Error Mean | t-Test | ||
|---|---|---|---|---|---|---|
| PS–PED | PAS Negative | 21 | 4.14 | 2.081 | 0.454 | <0.01 |
| PAS Positive | 38 | 9.13 | 1.398 | 0.227 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerchiari, A.; Tofani, M.; Giordani, C.; Franceschetti, S.; Capuano, E.; Pizza, F.; Della Bella, G.; Raponi, M.; Biondo, G. Development and Pilot Study of a Pediatric Screening for Feeding and Swallowing Disorders in Infants and Children: The Pediatric Screening–Priority Evaluation Dysphagia (PS–PED). Children 2023, 10, 638. https://doi.org/10.3390/children10040638
Cerchiari A, Tofani M, Giordani C, Franceschetti S, Capuano E, Pizza F, Della Bella G, Raponi M, Biondo G. Development and Pilot Study of a Pediatric Screening for Feeding and Swallowing Disorders in Infants and Children: The Pediatric Screening–Priority Evaluation Dysphagia (PS–PED). Children. 2023; 10(4):638. https://doi.org/10.3390/children10040638
Chicago/Turabian StyleCerchiari, Antonella, Marco Tofani, Carolina Giordani, Silvia Franceschetti, Eleonora Capuano, Francesca Pizza, Gessica Della Bella, Massimiliano Raponi, and Giorgia Biondo. 2023. "Development and Pilot Study of a Pediatric Screening for Feeding and Swallowing Disorders in Infants and Children: The Pediatric Screening–Priority Evaluation Dysphagia (PS–PED)" Children 10, no. 4: 638. https://doi.org/10.3390/children10040638