
Appendicitis and Peritonitis in Children with a Ventriculo-Peritoneal Shunt

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Identification
2.2. Study Protocol
2.3. Follow-Up
2.4. Statistical Analysis
2.5. Diagnostic Algorithm
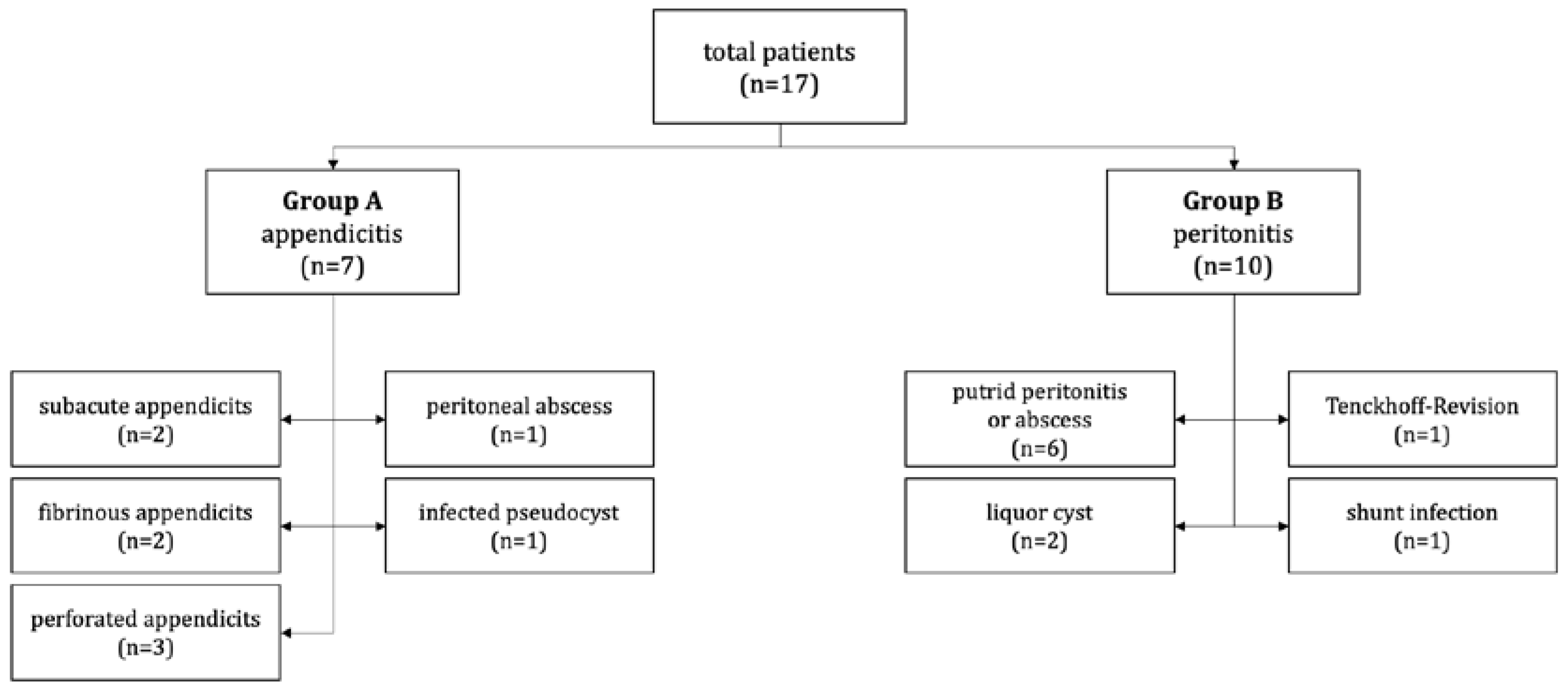
3. Results
3.1. Group A: Appendicitis (n = 7)
3.2. Group B: Peritonitis (n = 10)
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferreira Furtado, L.M.; da Costa Val Filho, J.A.; Moreira Faleiro, R.; Lima Vieira, J.A.; Dantas dos Santos, A.K. Abdominal Complications Related to Ventriculoperitoneal Shunt Placement: A Comprehensive Review of Literature. Cureus 2021, 13, e13230. [Google Scholar] [CrossRef] [PubMed]
- Mortellaro, V.E.; Chen, M.K.; Pincus, D.; Kays, D.W.; Islam, S.; Beierle, E.A. Infectious Risk to Ventriculo-Peritoneal Shunts from Gastrointestinal Surgery in the Pediatric Population. J. Pediatr. Surg 2009, 44, 1201–1205. [Google Scholar] [CrossRef] [PubMed]
- Dalfino, J.C.; Adamo, M.A.; Gandhi, R.H.; Boulos, A.S.; Waldm An, J.B. Conservative Management of Ventriculoperitoneal Shunts in the Setting of Abdominal and Pelvic Infections: Clinical Article. J. Neurosurg. Pediatr. 2012, 9, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, P.D.; Jayamohan, J.; Kelly, D.F.; Drysdale, S.B. Does Appendicitis in a Child with a Ventriculoperitoneal Shunt Necessitate Shunt Revision? Arch. Dis. Child 2019, 104, 607–609. [Google Scholar] [CrossRef] [PubMed]
- Bhangu, A.; Søreide, K.; Di Saverio, S.; Assarsson, J.H.; Drake, F.T. Acute Appendicitis: Modern Understanding of Pathogenesis, Diagnosis, and Management. Lancet 2015, 386, 1278–1287. [Google Scholar] [CrossRef] [PubMed]
- Almaramhy, H.H. Acute Appendicitis in Young Children Less than 5 Years: Review Article. Ital. J. Pediatr. 2017, 43, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, S.E.; Levy, M.L.; McComb, J.G.; Masri-Lavine, L. Does Age or Other Factors Influence the Incidence of Ventriculoperitoneal Shunt Infections? Pediatr. Neurosurg. 1999, 30, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Burhan, B.; Serdar, K.B.; Abdurrahman, A.; Edip, A.M.; Ebuzer, D. Abdominal Complications of Ventriculoperitoneal Shunt in Pediatric Patients: Experiences of a Pediatric Surgery Clinic. World Neurosurg. 2018, 118, e129–e136. [Google Scholar] [CrossRef] [PubMed]
- Hanak, B.W.; Bonow, R.H.; Harris, C.A.; Browd, S.R. Cerebrospinal Fluid Shunting Complications in Children. Pediatr. Neurosurg. 2017, 52, 381–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, J.J.; Walker, C.T.; Jacobson, M.; Phillips, V.; Silberstein, H.J. Revision Rate of Pediatric Ventriculoperitoneal Shunts after 15 Years: Clinical Article. J. Neurosurg. Pediatr. 2013, 11, 15–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, D.B.; Hill, J.G.; Thacker, P.G.; Rumboldt, Z.; Huda, W.; Ashley, B.; Hulsey, T.; Russell, W.S. The Role of Limited Head Computed Tomography in the Evaluation of Pediatric Ventriculoperitoneal Shunt Malfunction. Pediatr. Emerg. Care 2016, 32, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Bolster, F.; Fardanesh, R.; Morgan, T.; Katz, D.S.; Daly, B. Cross-Sectional Imaging of Thoracic and Abdominal Complications of Cerebrospinal Fluid Shunt Catheters. Emerg. Radiol. 2016, 23, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.D.; Riva-Cambrin, J.; Srivastava, R.; Bratton, S.L.; Dean, J.M.; Kestle, J.R.W. Hospital Care for Children with Hydrocephalus in the United States: Utilization, Charges, Comorbidities, and Deaths. J. Neurosurg. Pediatr. 2008, 1, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Jayanth, A.; Benabbas, R.; Chao, J.; Sinert, R. Diagnostic Modalities to Determine Ventriculoperitoneal Shunt Malfunction: A Systematic Review and Meta-Analysis. Am. J. Emerg. Med. 2021, 39, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Nadia, Y.; Basilotta Márquez, I.; Mengide, J.P.; Liñares, J.M.; Saenz, A.; Argañaraz, R.; Mantese, B. Abdominal Complications in Patients with a Ventriculoperitoneal Shunt: Proposal for Management Recommendations from a Single Pediatric Tertiary Center. Child’s Nerv. Syst. 2021, 37, 2223–2232. [Google Scholar] [CrossRef]
- Enger, P.Ø.; Svendsen, F.; Sommerfelt, K.; Wester, K. Shunt Revisions in Children—Can They Be Avoided? Pediatr. Neurosurg. 2005, 41, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.D.; Hall, M.; Riva-Cambrin, J.; Albert, J.E.; Jeffries, H.E.; LaFleur, B.; Dean, J.M.; Kestle, J.R.W.; Kestle, J.; Simon, T.; et al. Infection Rates Following Initial Cerebrospinal Fluid Shunt Placement across Pediatric Hospitals in the United States: Clinical Article. J. Neurosurg. Pediatr. 2009, 4, 156–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.-C.; Lee, H.J.; Sung, J.-N.; Cho, B.-K. Cerebrospinal Fluid Shunt Infection in Children: Efficiency of Management Protocol, Rate of Persistent Shunt Colonization, and Significance of ‘off-Antibiotics’ Trial. Child’s Nerv. Syst. 1999, 15, 38–43. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group A (n = 7) Appendicitis | IQR | Group B (n = 10) Peritonitis | IQR | p | |
|---|---|---|---|---|---|
| male (n) | 1 (14.3%) | 5 (50.0%) | - | ||
| female (n) | 6 (85.7%) | 5 (50.0%) | - | ||
| age at operation (m) | 34.0 (7.0–195.0) | 17.0–47.0 | 71.0 (9.0–180.0) | 31.0–163.0 | 0.2489 |
| height (cm) | 87.0 (59.0–168.0) | 71.8–127.5 | 100.0 (61.0–163.0) | 79.5–138.0 | 0.6891 |
| weight (kg) | 11.1 (5.5–82.0) | 8.4–43.8 | 17.0 (5.8–63.0) | 9.0–52.5 | 0.8866 |
| BMI | 15.5 (12.4–29.0) | 13.5–22.8 | 15.6 (12.0–23.7) | 12.6–21.7 | 0.8568 |
| preoperative CRP (mg/dL) | 152.0 (25.0–363.0) | 123.0–327.0 | 104.0 (0.0–305.0) | 16.3–256.3 | 0.3551 |
| temperature (°C) | 39.0 (37.7–40.7) | 38.0–40.2 | 38.4 (36.7–39.0) | 37.3–38.7 | 0.0925 |
| leucocytes (x 109/l) | 13.9 (2.5–27.2) | 11.0–22.7 | 19.5 (7.1–29.5) | 12.0–25.2 | 0.3622 |
| age at first shunt placement (m) | 7.5 (0.0–194.0) | 1.5–67.3 | 4.5 (2.0–150.0) | 2.0–45.0 | 0.7960 |
| age at last shunt placement (m) | 17.5 (6.0–194.0) | 6.8–77.0 | 20.0 (6.0–150.0) | 8.0–108.0 | 0.9499 |
| shunt duration (m) | 4.0 (0.0–40.0) | 0.8–15.3 | 5.0 (0.0–64.0) | 0.3–18.8 | 0.6992 |
| operation time (min) | 123.0 (73.0–200.0) | 93.0–166.0 | 97.0 (38.0–290.0) | 53.0–162.5 | 0.6707 |
| shunt externalization (n) | 7 (100.0%) | 8 (80.0%) | |||
| time to shunt reimplantation (d) | 20.0 (3.0–28.0) | 8.5–27.5 | 14.0 (0.0–25.0) | 7.0–15.0 | 0.3316 |
| hospital length of stay (d) | 25.0 (11.0–40.0) | 18.0–36.0 | 26.0 (4.0–62.0) | 18.3–42.3 | 0.6072 |
| Group A (n = 7) | Group B (n = 10) | |
|---|---|---|
| Post-hemorrhagic Hydrocephalus | 3 | 5 |
| Hydrocephalus (no specification) | 1 | 2 |
| Hydrocephalus at birth | 0 | 2 |
| Hydrocephalus by tumor | 1 | 1 |
| Hydrocephalus by malformation | 1 | 0 |
| Hydrocephalus occlusus | 1 | 0 |
| Group A (n = 7) | Group B (n = 10) | |
|---|---|---|
| Nitroimidazole | ||
| Metronidazole | 7 | 3 |
| Glycopeptide | ||
| Vancomycin | 4 | 6 |
| Teicoplanin | 0 | 1 |
| Cephalosporine | ||
| Cefuroxime | 4 | 2 |
| Cefotaxime | 2 | 2 |
| Ceftriaxone | 1 | 1 |
| Cefazoline | 0 | 1 |
| Ceftazidime | 0 | 1 |
| Carbapenems | ||
| Meropenem | 1 | 3 |
| Penicillin | ||
| Ampicillin/Sulbactam | 2 | 1 |
| Piperacillin/Tazobactam | 0 | 2 |
| Penicillin G | 0 | 1 |
| Flucloxacillin | 1 | 0 |
| Aminoglycoside | ||
| Tobramycin | 2 | 2 |
| Macrolide | ||
| Erythromycin | 2 | 0 |
| Fluocinolone | ||
| Ciprofloxacin | 0 | 1 |
| Sulphonamide | ||
| Cotrimoxazole | 1 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fröschle, G.M.C.; Hagens, J.; Mannweiler, P.; Groth, F.S.; Kammler, G.; Reinshagen, K.; Tomuschat, C. Appendicitis and Peritonitis in Children with a Ventriculo-Peritoneal Shunt. Children 2023, 10, 571. https://doi.org/10.3390/children10030571
Fröschle GMC, Hagens J, Mannweiler P, Groth FS, Kammler G, Reinshagen K, Tomuschat C. Appendicitis and Peritonitis in Children with a Ventriculo-Peritoneal Shunt. Children. 2023; 10(3):571. https://doi.org/10.3390/children10030571
Chicago/Turabian StyleFröschle, Glenn M. C., Johanna Hagens, Philip Mannweiler, Friederike Sophie Groth, Gertrud Kammler, Konrad Reinshagen, and Christian Tomuschat. 2023. "Appendicitis and Peritonitis in Children with a Ventriculo-Peritoneal Shunt" Children 10, no. 3: 571. https://doi.org/10.3390/children10030571