
The Molecular and Histopathological Assessment of Inflammatory Status in Very and Extremely Premature Infants: A Prospective Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Inclusion Criteria and Study Variables
2.3. Study Methods
2.4. Statistical Analysis
3. Results
Patients’ Background Characteristics
4. Discussion
4.1. Literature Findings
4.2. Study Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Shankaran, S.; Laptook, A.R.; Walsh, M.C.; Hale, E.C.; Newman, N.S.; Schibler, K.; Carlo, W.A.; et al. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics 2010, 126, 443–456. [Google Scholar] [CrossRef] [PubMed]
- Salas, A.A.; Faye-Petersen, O.M.; Sims, B.; Peralta-Carcelen, M.; Reilly, S.D.; McGwin, G., Jr.; Carlo, W.A.; Ambalavanan, N. Histological characteristics of the fetal inflammatory response associated with neurodevelopmental impairment and death in extremely preterm infants. J. Pediatr. 2013, 163, 652–657.e1–2. [Google Scholar] [CrossRef] [PubMed]
- John, C.C.; Black, M.M.; Nelson, C.A., 3rd. Neurodevelopment: The Impact of Nutrition and Inflammation During Early to Middle Childhood in Low-Resource Settings. Pediatrics 2017, 139, S59–S71. [Google Scholar] [CrossRef]
- Orsaria, M.; Liviero, S.; Rossetti, E.; Pittini, C.; Driul, L.; Londero, A.P.; Mariuzzi, L. Placental acute inflammation infiltrates and pregnancy outcomes: A retrospective cohort study. Sci. Rep. 2021, 11, 24165. [Google Scholar] [CrossRef]
- Kim, C.J.; Romero, R.; Chaemsaithong, P.; Chaiyasit, N.; Yoon, B.H.; Kim, Y.M. Acute chorioamnionitis and funisitis: Definition, pathologic features, and clinical significance. Am. J. Obstet. Gynecol. 2015, 213, S29–S52. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Chaemsaithong, P.; Docheva, N.; Korzeniewski, S.J.; Kusanovic, J.P.; Yoon, B.H.; Kim, J.-S.; Chaiyasit, N.; Ahmed, A.I.; Qureshi, F.; et al. Clinical chorioamnionitis at term VI: Acute chorioamnionitis and funisitis according to the presence or absence of microorganisms and inflammation in the amniotic cavity. J. Perinat. Med. 2016, 44, 33–51. [Google Scholar] [CrossRef]
- Seong, J.S.; Park, C.-W.; Moon, K.C.; Park, J.S.; Jun, J.K. Necrotizing funisitis is an indicator that intra-amniotic inflammatory response is more severe and amnionitis is more frequent in the context of the extension of inflammation into Wharton’s jelly. Taiwan J. Obstet. Gynecol. 2021, 60, 840–850. [Google Scholar] [CrossRef]
- Lahra, M.M.; E Jeffery, H. A fetal response to chorioamnionitis is associated with early survival after preterm birth. Am. J. Obstet. Gynecol. 2004, 190, 147–151. [Google Scholar] [CrossRef]
- Dammann, O.; Allred, E.N.; Leviton, A.; Shen-Schwarz, S.; Heller, D.; Genest, D.R.; Collins, M.H. Fetal vasculitis in preterm newborns: Interrelationships, modifiers, and antecedents. Placenta 2004, 25, 788–796. [Google Scholar] [CrossRef]
- Redline, R.W.; Wilson-Costello, D.; Borawski, E.; A Fanaroff, A.; Hack, M. The relationship between placental and other perinatal risk factors for neurologic impairment in very low birth weight children. Pediatr. Res. 2000, 47, 721–726. [Google Scholar] [CrossRef] [Green Version]
- Dammann, O.; Leviton, A. Inflammatory brain damage in preterm newborns—Dry numbers, wet lab, and causal inferences. Early Hum. Dev. 2004, 79, 1–15. [Google Scholar] [CrossRef]
- Malaeb, S.; Dammann, O. Fetal inflammatory response and brain injury in the preterm newborn. J. Child Neurol. 2009, 24, 1119–1126. [Google Scholar] [CrossRef]
- Pacora, P.; Chaiworapongsa, T.; Maymon, E.; Kim, Y.M.; Gomez, R.; Yoon, B.H.; Ghezzi, F.; Berry, S.M.; Qureshi, F.; Jacques, S.M.; et al. Funisitis and chorionic vasculitis: The histological counterpart of the fetal inflammatory response syndrome. J. Matern. Fetal. Neonatal. Med. 2002, 11, 18–25. [Google Scholar] [CrossRef]
- Redline, R.W. Inflammatory responses in the placenta and umbilical cord. Semin. Fetal. Neonatal. Med. 2006, 11, 296–301. [Google Scholar] [CrossRef]
- Machin, G. Funisitis and chorionic vasculitis: Relation to chorioamnionitis, timing and scoring. Fetal. Pediatr. Pathol. 2011, 30, 414–430. [Google Scholar] [CrossRef] [PubMed]
- Hecht, J.L.; Allred, E.N.; Kliman, H.J.; Zambrano, E.; Doss, B.J.; Husain, A.; Pflueger, S.M.V.; Chang, C.-H.; Livasy, C.A.; Roberts, D.; et al. Histological characteristics of singleton placentas delivered before the 28th week of gestation. Pathology. 2008, 40, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.R.; Collins, M.H.; Genest, D.; Heller, D.; Shen-Schwarz, S.; Banagon, P.; Allred, E.N.; Leviton, A. Very low birthweight placenta: Clustering of morphologic characteristics. Pediatr. Dev. Pathol. 2000, 3, 431–438. [Google Scholar] [CrossRef]
- Lau, J.; Magee, F.; Qiu, Z.; Houbé, J.; Von Dadelszen, P.; Lee, S.K. Chorioamnionitis with a fetal inflammatory response is associated with higher neonatal mortality, morbidity, and resource use than chorioamnionitis displaying a maternal inflammatory response only. Am. J. Obstet. Gynecol. 2005, 193, 708–713. [Google Scholar] [CrossRef] [PubMed]
- Mestan, K.; Yu, Y.; Thorsen, P.; Skogstrand, K.; Matoba, N.; Liu, X.; Kumar, R.; Hougaard, D.M.; Gupta, M.; Pearson, C.; et al. Cord blood biomarkers of the fetal inflammatory response. J. Matern. Fetal. Neonatal. Med. 2009, 22, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Hillier, S.L.; Witkin, S.S.; A Krohn, M.; Watts, D.H.; Kiviat, N.B.; A Eschenbach, D. The relationship of amniotic fluid cytokines and preterm delivery, amniotic fluid infection, histologic chorioamnionitis, and chorioamnion infection. Obstet. Gynecol. 1993, 81, 941–948. [Google Scholar]
- Jacobsson, B.; Holst, R.-M.; Wennerholm, U.-B.; Andersson, B.; Lilja, H.; Hagberg, H. Monocyte chemotactic protein-1 in cervical and amniotic fluid: Relationship to microbial invasion of the amniotic cavity, intra-amniotic inflammation, and preterm delivery. Am. J. Obstet. Gynecol. 2003, 189, 1161–1167. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Gomez, R.; Galasso, M.; Munoz, H.; Acosta, L.; Yoon, B.H.; Svinarich, D.; Cotton, D.B. Macrophage inflammatory protein-1 alpha in term and preterm parturition: Effect of microbial invasion of the amniotic cavity. Am. J. Reprod. Immunol. 1994, 32, 108–113. [Google Scholar] [CrossRef]
- Park, C.-W.; Moon, K.C.; Park, J.S.; Jun, J.K.; Romero, R.; Yoon, B.H. The involvement of human amnion in histologic chorioamnionitis is an indicator that a fetal and an intra-amniotic inflammatory response is more likely and severe: Clinical implications. Placenta 2009, 30, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Yoon, B.H.; Romero, R.; Park, J.S.; Kim, M.; Oh, S.-Y.; Kim, C.J.; Jun, J.K. The relationship among inflammatory lesions of the umbilical cord (funisitis), umbilical cord plasma interleukin 6 concentration, amniotic fluid infection, and neonatal sepsis. Am. J. Obstet. Gynecol. 2000, 183, 1124–1129. [Google Scholar] [CrossRef]
- Kim, C.J.; Yoon, B.H.; Romero, R.; Bin Moon, J.; Kim, M.; Park, S.-S.; Chi, J.-G. Umbilical arteritis and phlebitis mark different stages of the fetal inflammatory response. Am. J. Obstet. Gynecol. 2001, 185, 496–500. [Google Scholar] [CrossRef] [PubMed]
- Rogers, B.B.; Alexander, J.M.; Head, J.; Mcintire, D.; Leveno, K.J. Umbilical vein interleukin-6 levels correlate with the severity of placental inflammation and gestational age. Hum. Pathol. 2002, 33, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Kim, H.-J.; Choi, S.-J.; Oh, S.-Y.; Kim, J.-S.; Roh, C.-R.; Kim, J.-H. Is there a stepwise increase in neonatal morbidities according to histological stage (or grade) of acute chorioamnionitis and funisitis?: Effect of gestational age at delivery. J. Perinat. Med. 2015, 43, 259–267. [Google Scholar] [CrossRef]
- Oh, J.-W.; Park, C.-W.; Moon, K.C.; Park, J.S.; Jun, J.K. The relationship among the progression of inflammation in umbilical cord, fetal inflammatory response, early-onset neonatal sepsis, and chorioamnionitis. PLoS ONE 2019, 14, e0225328. [Google Scholar] [CrossRef]
- Humberg, A.; Fortmann, I.; Siller, B.; Kopp, M.V.; Herting, E.; Gopel, W.; Hartel, C. German Neonatal Network, German Center for Lung Research and Priming Immunity at the beginning of life (PRIMAL) Consortium. Preterm birth and sustained inflammation: Consequences for the neonate. Semin. Immunopathol. 2020, 42, 451–468. [Google Scholar] [CrossRef]
- Goldstein, J.A.; Gallagher, K.; Beck, C.; Kumar, R.; Gernand, A.D. Maternal-Fetal Inflammation in the Placenta and the Developmental Origins of Health and Disease. Front. Immunol. 2020, 11, 531543. [Google Scholar] [CrossRef]
- Kim, C.J.; Yoon, B.H.; Kim, M.; Park, J.O.; Cho, S.Y.; Chi, J.-G. Histo-topographic distribution of acute inflammation of the human umbilical cord. Pathol. Int. 2001, 51, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.W.; Park, C.W.; Moon, K.C.; Park, J.S.; Jun, J.K. Fetal inflammatory response is positively correlated with the progress of inflammation in chorionic plate. Placenta 2020, 97, 6–17. [Google Scholar] [CrossRef] [PubMed]
- Para, R.; Romero, R.; Miller, D.; Galaz, J.; Done, B.; Peyvandipour, A.; Gershater, M.; Tao, L.; Motomura, K.; Ruden, D.M.; et al. The Distinct Immune Nature of the Fetal Inflammatory Response Syndrome Type I and Type II. Immunohorizons 2021, 5, 735–751. [Google Scholar] [CrossRef] [PubMed]
- Jung, E.; Romero, R.; Yeo, L.; Diaz-Primera, R.; Marin-Concha, J.; Para, R.; Lopez, A.M.; Pacora, P.; Gomez-Lopez, N.; Yoon, B.H.; et al. The fetal inflammatory response syndrome: The origins of a concept, pathophysiology, diagnosis, and obstetrical implications. Semin. Fetal. Neonatal. Med. 2020, 25, 101146. [Google Scholar] [CrossRef]
- Hatano, Y.; Tamada, M.; Shiga, T.; Niwa, A.; Kanayama, T.; Noguchi, K.; Morishige, K.-I.; Tomita, H.; Hara, A. Clinically relevant umbilical cord inflammation identified based on CD15-associated vasculitis patterning. Placenta 2021, 108, 39–46. [Google Scholar] [CrossRef]
- Glass, H.C.; Costarino, A.T.; Stayer, S.A.; Brett, C.M.; Cladis, F.; Davis, P. J Outcomes for extremely premature infants. Anesth. Analg. 2015, 120, 1337–1351. [Google Scholar] [CrossRef]
- Kamei, M.; Hussein, M.H.; Hattori, A.; Saleh, M.; Kakita, H.; Daoud, G.A.-H.; Ishiguro, A.; Namba, F.; Yazaki, M.; Goto, H.; et al. Oxidative and Inflammatory Markers Are Higher in Full-Term Newborns Suffering Funisitis, and Higher Oxidative Markers Are Associated with Admission. Children 2022, 9, 702. [Google Scholar] [CrossRef]
- Sanodze, N.; Uberi, N.; Uberi, E.; Kulumbegov, B. Parameters of Oxidative Metabolism in Neonates Suffering from Sepsis and Anemia. Georgian Med. News. 2006, 140, 65–67. [Google Scholar]
- Victor, V.M.; Rocha, M.; De la Fuente, M. Immune Cells: Free Radicals and Antioxidants in Sepsis. Int. Immunopharmacol. 2004, 4, 327–347. [Google Scholar] [CrossRef]
- Reuschel, E.; Toelge, M.; Entleutner, K.; Deml, L.; Seelbach-Goebel, B. Cytokine profiles of umbilical cord blood mononuclear cells upon in vitro stimulation with lipopolysaccharides of different vaginal gram-negative bacteria. PLoS ONE 2019, 14, e0222465. [Google Scholar] [CrossRef]
- Kunze, M.; Klar, M.; Morfeld, C.A.; Thorns, B.; Schild, R.L.; Markfeld-Erol, F.; Rasenack, R.; Proempeler, H.; Hentschel, R.; Schaefer, W.R. Cytokines in noninvasively obtained amniotic fluid as predictors of fetal inflammatory response syndrome. Am J. Obstet. Gynecol. 2016, 215, 96e1–98. [Google Scholar] [CrossRef] [PubMed]
- Ernst, W.; Kusi, E.; Malfertheiner, S.F.; Reuschel, E.; Deml, L.; Seelbach-Göbel, B. The effect of Indomethacin and Betamethasone on the cytokine response of human neonatal mononuclear cells to gram-positive bacteria. Cytokine 2015, 73, 91–100. [Google Scholar] [CrossRef]
- Miller, S.P.; Mayer, E.E.; Clyman, R.I.; Glidden, D.V.; Hamrick, S.E.; Barkovich, A.J. Prolonged indomethacin exposure is associated with decreased white matter injury detected with magnetic resonance imaging in premature newborns at 24 to 28 weeks’ gestation at birth. Pediatrics 2006, 117, 1626–1631. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Elices, C.; Chato-Astrain, J.; González-González, A.; Sánchez-Porras, D.; Carriel, V.; Fernández-Valadés, R.; Sánchez-Quevedo, M.D.C.; Alaminos, M.; Garzón, I. Histological Profiling of the Human Umbilical Cord: A Potential Alternative Cell Source in Tissue Engineering. J. Pers. Med. 2022, 12, 648. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total (n = 30) | EPI (n = 10) | VPI (n = 20) | p-Value |
|---|---|---|---|---|
| Weight, grams (mean ± SD) | 1291.8 ± 405.8 | 871.5 ± 241.6 | 1502.0 ± 292.2 | <0.001 |
| Weight range | <0.001 | |||
| 500–1000 g | 8 (26.7%) | 7 (70.0%) | 1 (5.0%) | |
| 1000–1500 g | 14 (46.6%) | 3 (30.0%) | 11 (55.0%) | |
| 1500–2000 g | 8 (26.7%) | 0 (0.0%) | 8 (40.0%) | |
| Gender | 0.795 | |||
| Male | 16 (53.3%) | 5 (50.0%) | 11 (55.0%) | |
| Female | 14 (46.7%) | 5 (50.0%) | 9 (45.0%) | |
| Gestational age (weeks) | – | |||
| 24–25 | 2 (6.7%) | 2 (20.0%) | 0 (0.0%) | |
| 26–27 | 8 (26.7%) | 8 (80.0%) | 0 (0.0%) | |
| 28–29 | 3 (10.0%) | 0 (0.0%) | 3 (15.0%) | |
| 30–31 | 17 (56.6%) | 0 (0.0%) | 17 (85.0%) |
| Inflammatory Markers | Total (n = 30) | EPI (n = 10) | VPI (n = 20) | p-Value |
|---|---|---|---|---|
| IL-6, (mean ± SD) | 319.1 ± 78.6 | 638.2 ± 122.7 | 151.1 ± 26.7 | <0.001 |
| CRP at birth, (mean ± SD) | 5.5 ± 1.1 | 6.0 ± 1.8 | 4.6 ± 2.6 | 0.138 |
| CRP at 4 days, (mean ± SD) | 10.0 ± 0.9 | 7.2 ± 3.2 | 11.0 ± 1.3 | <0.001 |
| LDH at birth, (mean ± SD) | 596.5 ± 46.3 | 851.8 ± 72.2 | 468.9 ± 108.2 | <0.001 |
| LDH at 4 days, (mean ± SD) | 698.0 ± 45.6 | 962.3 ± 69.9 | 565.9 ± 119.0 | <0.001 |
| IL-6 (N: <6.6 pg/mL) | 0.128 | |||
| Pathological | 26 (86.7%) | 10 (100%) | 16 (80.0%) | |
| Normal | 4 (13.3%) | 0 (0.0%) | 4 (20.0%) | |
| CRP (N: <5 mg/dL) | 0.704 | |||
| Pathological | 26 (86.7%) | 9 (90.0%) | 17 (85.0%) | |
| Normal | 4 (13.3%) | 1 (10.0%) | 3 (15.0%) | |
| LDH (N: 120–246 UI/L) | 0.472 | |||
| Pathological | 29 (96.7%) | 10 (100%) | 19 (95.0%) | |
| Normal | 1 (3.3%) | 0 (0.0%) | 1 (5.0%) |
| EPI (n = 10) | VPI (n = 20) | |||||
|---|---|---|---|---|---|---|
| Markers | At Birth | At 4 Days | p-Value | At Birth | At 4 Days | p-Value |
| CRP (mean ± SD), mg/dL | 6.0 ± 1.8 | 7.2 ± 3.2 | 0.315 | 4.6 ± 2.6 | 11.0 ± 1.3 | <0.001 |
| LDH (mean ± SD), UI/L | 851.8 ± 72.2 | 962.3 ± 69.9 | 0.003 | 468.9 ± 108.2 | 565.9 ± 119.0 | 0.010 |
| Level of Inflammation | EPI (n = 10) | VPI (n = 20) | p-Value |
|---|---|---|---|
| UC stage of inflammation | 0.902 | ||
| S0 | 4 (40.0%) | 11 (55.0%) | |
| S1 | 1 (10.0%) | 1 (5.0%) | |
| S2 | 1 (10.0%) | 2 (10.0%) | |
| S3 | 2 (20.0%) | 4 (20.0%) | |
| S4 | 2 (20.0%) | 2 (10.0%) | |
| FIR | 0.606 | ||
| Stage 1 | 5 (50.0%) | 13 (65.0%) | |
| Stage 2 | 2 (20.0%) | 4 (20.0%) | |
| Stage 3 | 3 (30.0%) | 3 (15.0%) |
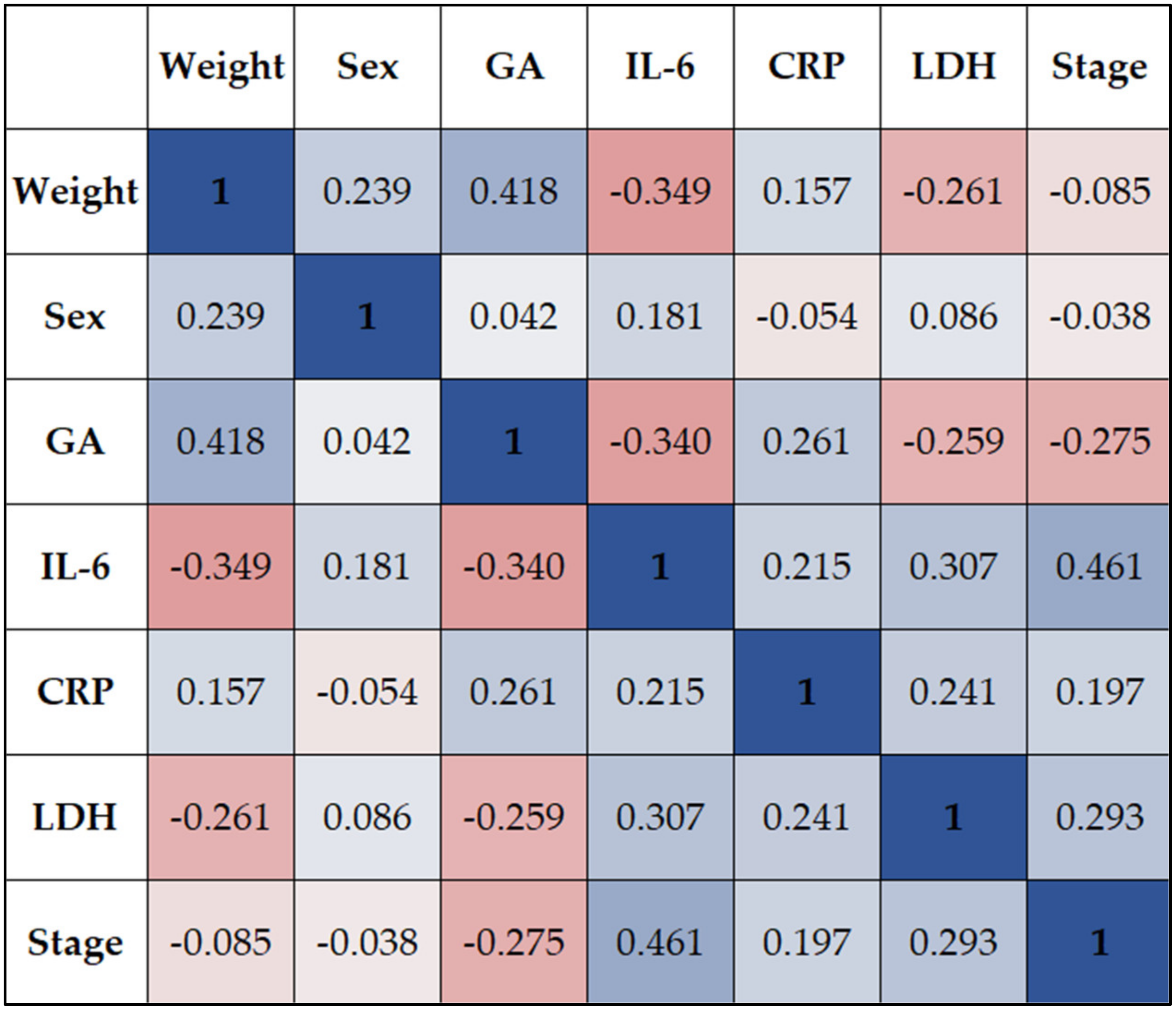
| Weight | Sex | GA | IL-6 | CRP | LDH | Stage | ||
|---|---|---|---|---|---|---|---|---|
| Weight | Rho | 1 | 0.239 | 0.418 ** | −0.349 ** | 0.157 | −0.261 * | −0.085 |
| p-value | - | 0.106 | 0.003 | 0.003 | 0.230 | 0.022 | 0.087 | |
| Sex | Rho | 0.239 | 1 | 0.042 | 0.181 | −0.054 | 0.086 | −0.038 |
| p-value | 0.106 | - | 0.378 | 0.244 | 0.423 | 0.624 | 0.466 | |
| GA | Rho | 0.418 ** | 0.042 | 1 | −0.340 * | 0.261 | −0.259 * | −0.275 |
| p-value | 0.003 | 0.378 | - | 0.038 | 0.056 | 0.030 | 0.063 | |
| IL-6 | Rho | −0.349 ** | 0.181 | −0.340 * | 1 | 0.215 ** | 0.307 ** | 0.461 ** |
| p-value | 0.003 | 0.244 | 0.038 | - | 0.000 | 0.002 | 0.000 | |
| CRP | Rho | 0.157 | −0.054 | 0.261 | 0.215 ** | 1 | 0.241 * | 0.197 |
| p-value | 0.230 | 0.423 | 0.056 | 0.000 | - | 0.027 | 0.064 | |
| LDH | Rho | −0.261 * | 0.086 | −0.259 * | 0.307 ** | 0.241 * | 1 | 0.293 ** |
| p-value | 0.022 | 0.624 | 0.030 | 0.002 | 0.027 | - | 0.006 | |
| Stage | Rho | −0.085 | −0.038 | −0.275 | 0.461 ** | 0.197 | 0.293 ** | 1 |
| p-value | 0.087 | 0.466 | 0.063 | 0.000 | 0.064 | 0.006 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borțea, C.I.; Enatescu, I.; Pantea, M.; Dima, M.; Iacob, E.R.; Dumitru, C.; Popescu, A.; Stoica, F.; Heredea, R.E.; Iacob, D. The Molecular and Histopathological Assessment of Inflammatory Status in Very and Extremely Premature Infants: A Prospective Study. Children 2023, 10, 352. https://doi.org/10.3390/children10020352
Borțea CI, Enatescu I, Pantea M, Dima M, Iacob ER, Dumitru C, Popescu A, Stoica F, Heredea RE, Iacob D. The Molecular and Histopathological Assessment of Inflammatory Status in Very and Extremely Premature Infants: A Prospective Study. Children. 2023; 10(2):352. https://doi.org/10.3390/children10020352
Chicago/Turabian StyleBorțea, Claudia Ioana, Ileana Enatescu, Manuela Pantea, Mirabela Dima, Emil Radu Iacob, Catalin Dumitru, Alin Popescu, Florina Stoica, Rodica Elena Heredea, and Daniela Iacob. 2023. "The Molecular and Histopathological Assessment of Inflammatory Status in Very and Extremely Premature Infants: A Prospective Study" Children 10, no. 2: 352. https://doi.org/10.3390/children10020352