
Masked Randomized Trial of Epinephrine versus Vasopressin in an Ovine Model of Perinatal Cardiac Arrest
 , , and
, , and
Abstract
:1. Introduction
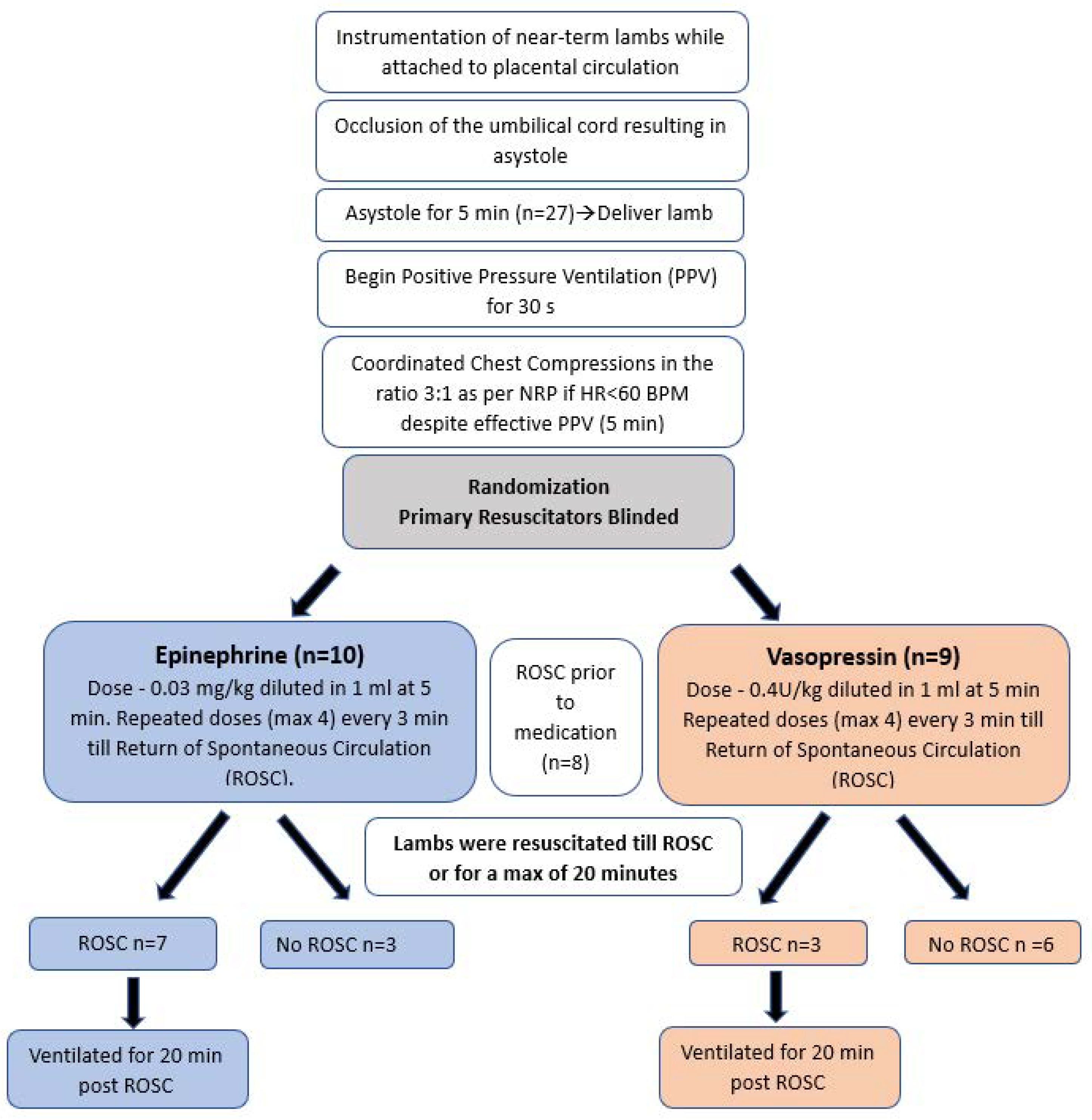
2. Materials and Methods
3. Results
3.1. Return of Spontaneous Circulation
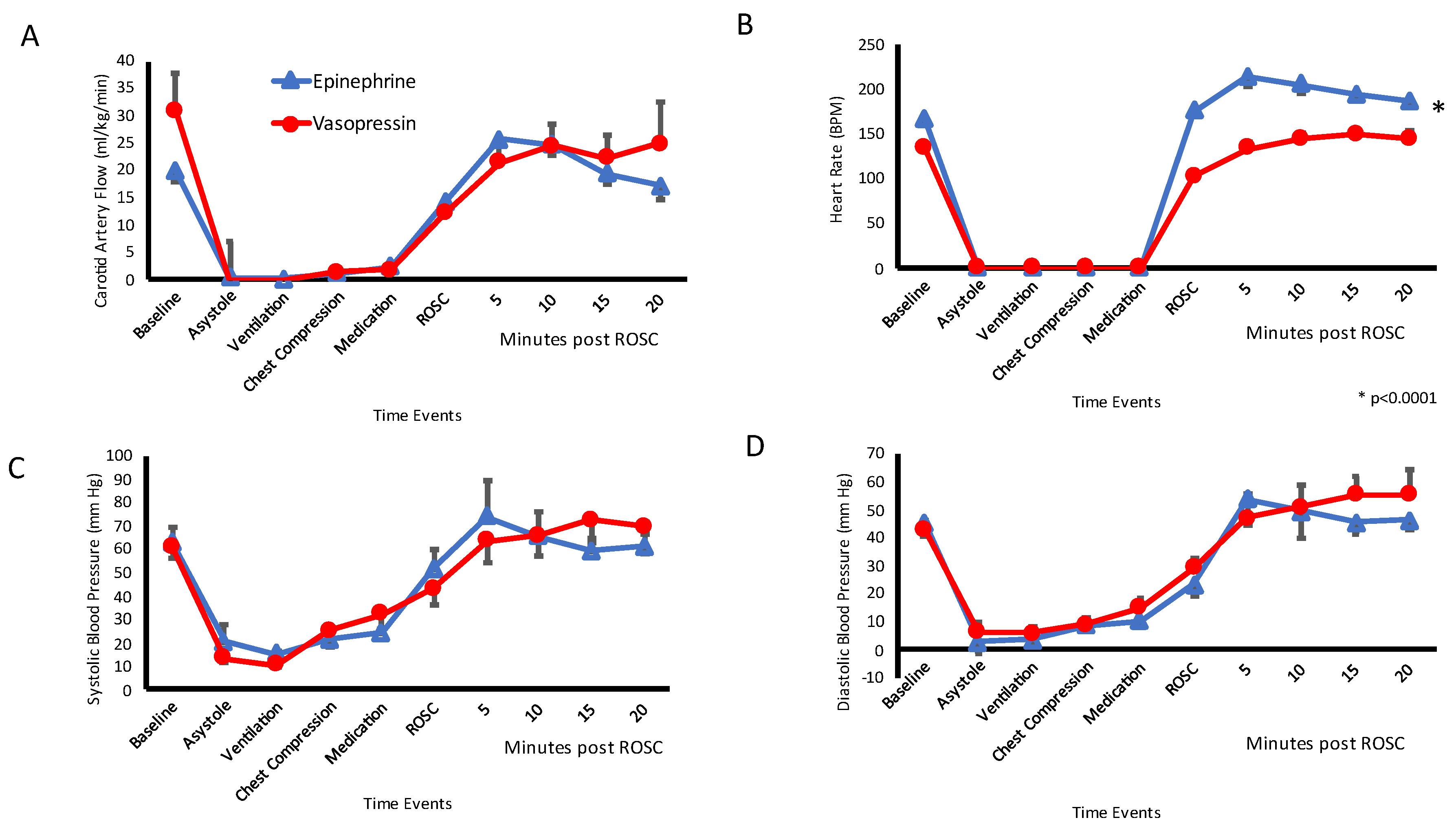
3.2. Systemic Hemodynamics
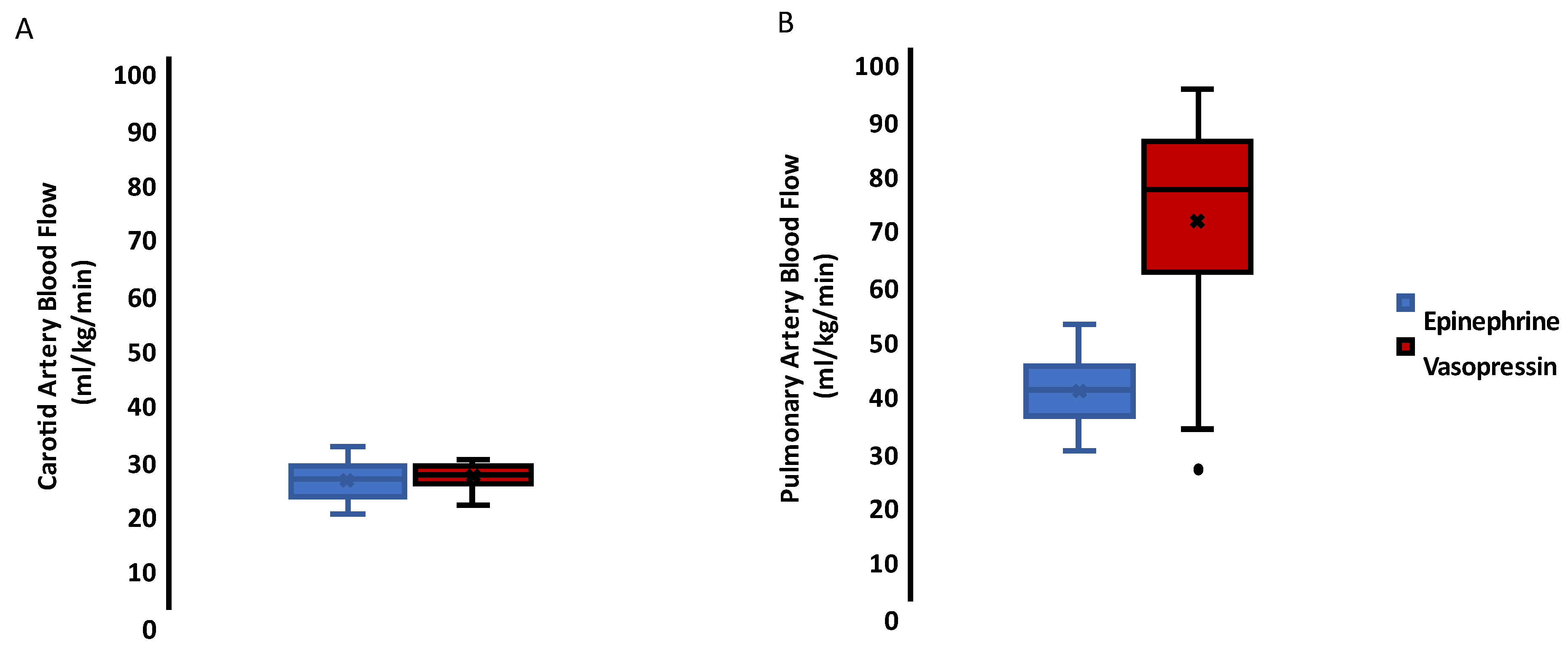
3.3. Carotid and Pulmonary Hemodynamics
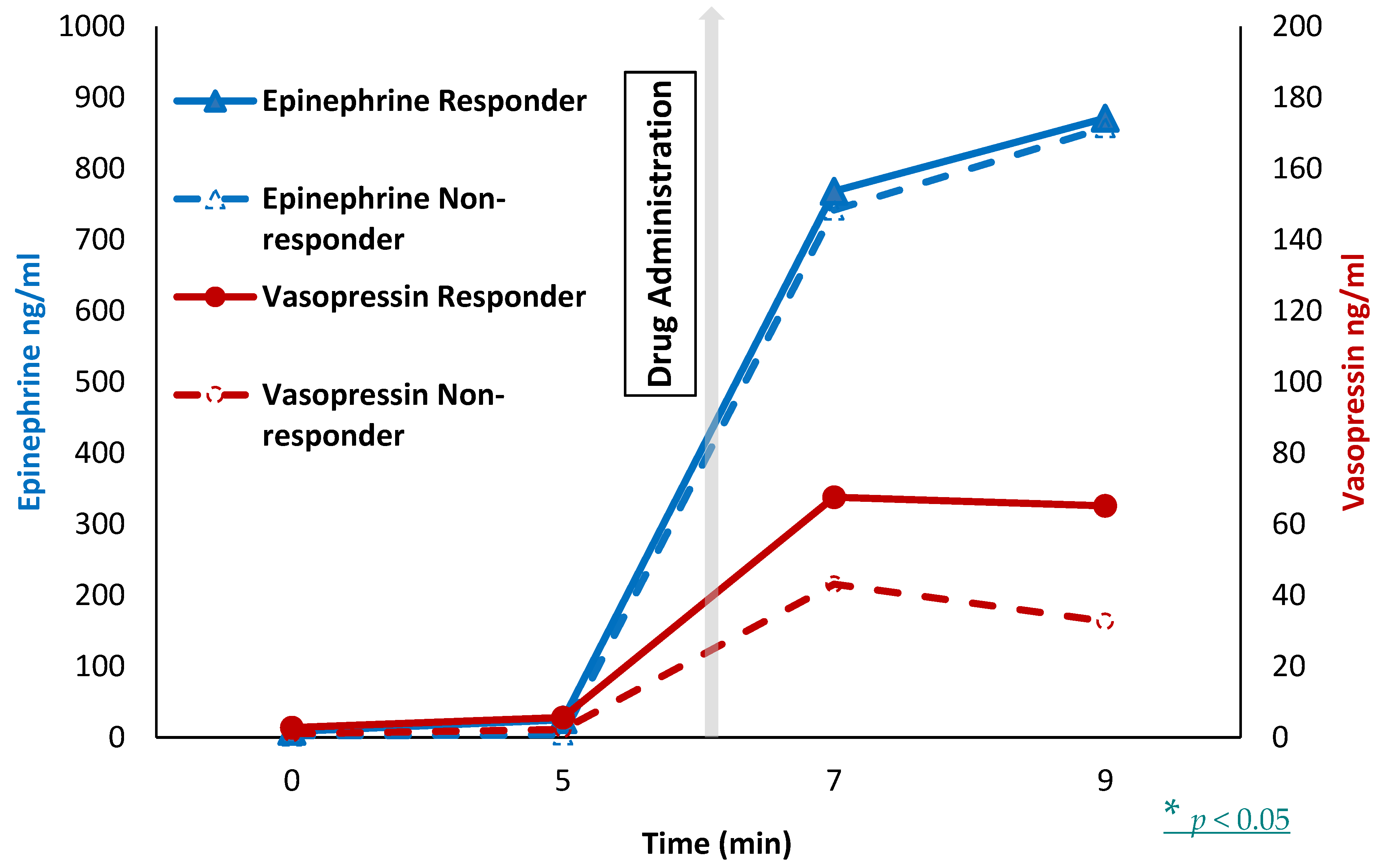
3.4. Plasma Drug Level
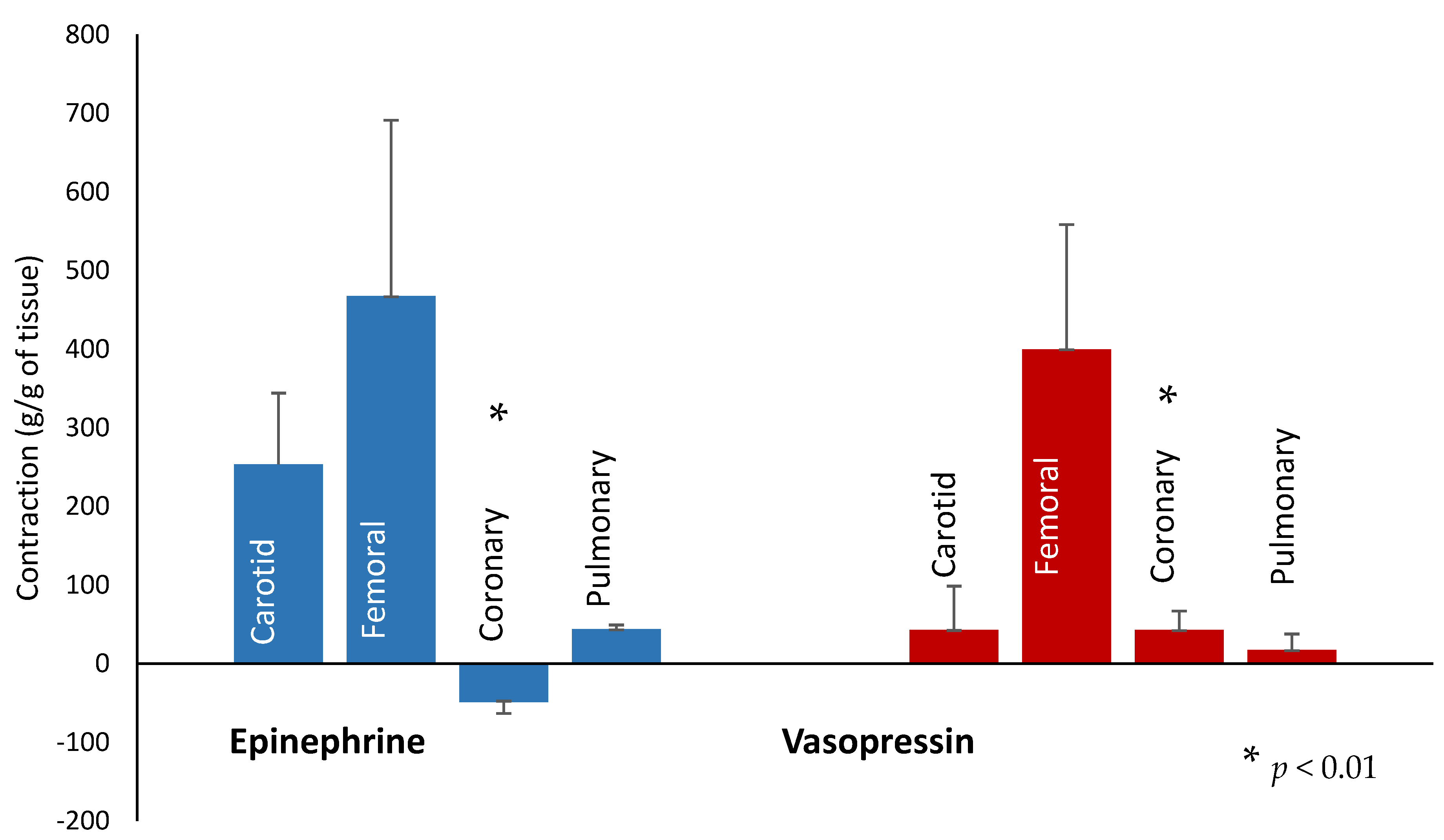
3.5. In-Vitro Vessel Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sharrow, D.; Hug, L.; You, D.; Alkema, L.; Black, R.; Cousens, S.; Croft, T.; Gaigbe-Togbe, V.; Gerland, P.; Guillot, M.; et al. Global, regional, and national trends in under-5 mortality between 1990 and 2019 with scenario-based projections until 2030: A systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. Lancet Glob. Health 2022, 10, e195–e206. [Google Scholar] [CrossRef]
- GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef]
- WHO. Newborn Mortality. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/levels-and-trends-in-child-mortality-report-2021 (accessed on 10 January 2023).
- Harrington, D.J.; Redman, C.W.; Moulden, M.; Greenwood, C.E. The long-term outcome in surviving infants with Apgar zero at 10 min: A systematic review of the literature and hospital-based cohort. Am. J. Obstet. Gynecol. 2007, 196, 463.e1–463.e5. [Google Scholar] [CrossRef]
- Wyckoff, M.H.; Salhab, W.A.; Heyne, R.J.; Kendrick, D.E.; Stoll, B.J.; Laptook, A.R. Outcome of extremely low birth weight infants who received delivery room cardiopulmonary resuscitation. J. Pediatr. 2012, 160, 239–244.e2. [Google Scholar] [CrossRef] [PubMed]
- Wyckoff, M.H.; Wyllie, J.; Aziz, K.; De Almeida, M.F.; Fabres, J.; Fawke, J.; Guinsburg, R.; Hosono, S.; Isayama, T.; Kapadia, V.S.; et al. Neonatal Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 2020, 142 (Suppl. 1), S185–S221. [Google Scholar] [CrossRef]
- Sobotka, K.S.; Polglase, G.R.; Schmölzer, G.M.; Davis, P.G.; Klingenberg, C.; Hooper, S.B. Effects of chest compressions on cardiovascular and cerebral hemodynamics in asphyxiated near-term lambs. Pediatr. Res. 2015, 78, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Weil, M.H.; Sun, S.; Noc, M.; Yang, L.; Gazmuri, R.J. Epinephrine increases the severity of postresuscitation myocardial dysfunction. Circulation 1995, 92, 3089–3093. [Google Scholar] [CrossRef]
- Gedeborg, R.; Silander, H.C.; Ronne-Engström, E.; Rubertsson, S.; Wiklund, L. Adverse effects of high-dose epinephrine on cerebral blood flow during experimental cardiopulmonary resuscitation. Crit. Care. Med. 2000, 28, 1423–1430. [Google Scholar] [CrossRef] [PubMed]
- Lindner, K.H.; Prengel, A.W.; Pfenninger, E.G.; Lindner, I.M.; Strohmenger, H.-U.; Georgieff, M.; Lurie, K.G. Vasopressin improves vital organ blood flow during closed-chest cardiopulmonary resuscitation in pigs. Circulation 1995, 91, 215–221. [Google Scholar] [CrossRef]
- Lindner, K.H.; Dirks, B.; Strohmenger, H.U.; Prengel, A.W.; Lindner, I.M.; Lurie, K.G. Randomised comparison of epinephrine and vasopressin in patients with out-of-hospital ventricular fibrillation. Lancet 1997, 349, 535–537. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, V.; Lindner, K.H.; Prengel, A.W.; Maier, C.; Voelckel, W.; Lurie, K.G.; Strohmenger, H.U. Vasopressin improves vital organ blood flow after prolonged cardiac arrest with post countershock pulseless electrical activity in pigs. Crit. Care Med. 1999, 27, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Voelckel, W.G.; Lurie, K.G.; Lindner, K.H.; Zielinski, T.; McKnite, S.; Krismer, A.C.; Wenzel, V. Vasopressin improves survival after cardiac arrest in hypovolemic shock. Anesth. Analg. 2000, 91, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Cardona, V.Q.; Menkiti, O. Use of vasopressin in persistent pulmonary hypertension of the newborn: A case series. SAGE Open Med. Case Rep. 2022, 10, 2050313X221102289. [Google Scholar] [CrossRef]
- McNamara, P.J.; Engelberts, D.; Finelli, M.; Adeli, K.; Kavanagh, B.P. Vasopressin improves survival compared with epinephrine in a neonatal piglet model of asphyxial cardiac arrest. Pediatr. Res. 2014, 75, 738–748. [Google Scholar] [CrossRef] [PubMed]
- Korkames, G.; Brink, H.; Peitz, G. Effect of norepinephrine versus vasopressin on pulmonary artery pressure. Critical Care Medicine. 2022, 50, 546. [Google Scholar] [CrossRef]
- Eisenach, J.C.; Tong, C.; Stump, D.A.; Block, S.M. Vasopressin and fetal cerebrovascular regulation. Am. J. Physiol. 1992, 263, R376–R381. [Google Scholar] [CrossRef]
- Vali, P.; Gugino, S.; Koenigsknecht, C.; Helman, J.; Chandrasekharan, P.; Rawat, M.; Lakshminrusimha, S.; Nair, J. The Perinatal Asphyxiated Lamb Model: A Model for Newborn Resuscitation. J. Vis. Exp. 2018, 138, 57553. [Google Scholar]
- Otto, C.W.; Yakaitis, R.W. The role of epinephrine in CPR: A reappraisal. Ann. Emerg. Med. 1984, 13, 840–843. [Google Scholar] [CrossRef]
- Otto, C.W.; Yakaitis, R.W.; Blitt, C.D. Mechanism of action of epinephrine in resuscitation from asphyxial arrest. Crit. Care Med. 1981, 9, 364–365. [Google Scholar] [CrossRef]
- Redding, J.S.; Pearson, J.W. Evaluation of drugs for cardiac resuscitation. Anesthesiology 1963, 24, 203–207. [Google Scholar] [CrossRef]
- Wyckoff, M.H.; Perlman, J.M. Use of high-dose epinephrine and sodium bicarbonate during neonatal resuscitation: Is there proven benefit? Clin. Perinatol. 2006, 33, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Ditchey, R.V.; Lindenfeld, J. Failure of epinephrine to improve the balance between myocardial oxygen supply and demand during closed-chest resuscitation in dogs. Circulation 1988, 78, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Evora, P.R.B.; Pearson, P.J.; Rodrigues, A.J.; Viaro, F.; Schaff, H.V. Effect of arginine vasopressin on the canine epicardial coronary artery: Experiments on V1-receptor-mediated production of nitric oxide. Arq. Bras. Cardiol. 2003, 80, 483–494. [Google Scholar] [CrossRef] [PubMed]
- Voelckel, W.G.; Lurie, K.G.; McKnite, S.; Zielinski, T.; Lindstrom, P.; Peterson, C.; Wenzel, V.; Lindner, K.H.; Benditt, D. Effects of epinephrine and vasopressin in a piglet model of prolonged ventricular fibrillation and cardiopulmonary resuscitation. Crit. Care Med. 2002, 30, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Borgeat, A.; Popovic, V.; Nicole, A.; Schwander, D. Acute pulmonary oedema following administration of ornithine-8-vasopressin. Br. J. Anaesth. 1990, 65, 548–551. [Google Scholar] [CrossRef]
- Fox, A.W.; May, R.E.; Mitch, W.E. Comparison of peptide and nonpeptide receptor-mediated responses in rat tail artery. J. Cardiovasc. Pharmacol. 1992, 20, 282–289. [Google Scholar] [CrossRef]
- McIntyre, K.M. Vasopressin in asystolic cardiac arrest. N. Engl. J. Med. 2004, 350, 179–181. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, V.; Krismer, A.C.; Arntz, H.R.; Sitter, H.; Stadlbauer, K.H.; Lindner, K.H. A comparison of vasopressin and epinephrine for out-of-hospital cardiopulmonary resuscitation. N. Engl. J. Med. 2004, 350, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Sankaran, D.; Molloy, E.J.; Lakshminrusimha, S. Is epinephrine effective during neonatal resuscitation? Pediatr. Res. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Vali, P.; Chandrasekharan, P.; Rawat, M.; Gugino, S.; Koenigsknecht, C.; Helman, J.; Mathew, B.; Berkelhamer, S.; Nair, J.; Wyckoff, M.; et al. Hemodynamics and gas exchange during chest compressions in neonatal resuscitation. PLoS ONE 2017, 12, e0176478. [Google Scholar] [CrossRef]
- Enomoto, M.; Pan, J.; Shifrin, Y.; Belik, J. Age dependency of vasopressin pulmonary vasodilatory effect in rats. Pediatr. Res. 2014, 75, 315–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, S.; Gottschling, S.; Baghai, A.; Wurm, D.; Gortner, L. Arginine-vasopressin in catecholamine-refractory septic versus non-septic shock in extremely low birth weight infants with acute renal injury. Crit. Care 2006, 10, R71. [Google Scholar] [CrossRef] [PubMed]
- Sankaran, D.; Chandrasekharan, P.K.; Gugino, S.F.; Koenigsknecht, C.; Helman, J.; Nair, J.; Mathew, B.; Rawat, M.; Vali, P.; Nielsen, L.; et al. Randomised trial of epinephrine dose and flush volume in term newborn lambs. Arch. Dis. Child. Fetal. Neonatal. Ed. 2021, 106, 578–583. [Google Scholar] [CrossRef]
- Link, M.S.; Berkow, L.C.; Kudenchuk, P.J.; Halperin, H.R.; Hess, E.P.; Moitra, V.K.; Neumar, R.W.; O’Neil, B.J.; Paxton, J.H.; Silvers, S.M.; et al. Part 7: Adult Advanced Cardiovascular Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132 (Suppl. 2), S444–S464. [Google Scholar] [CrossRef] [PubMed]
- Mukoyama, T.; Kinoshita, K.; Nagao, K.; Tanjoh, K. Reduced effectiveness of vasopressin in repeated doses for patients undergoing prolonged cardiopulmonary resuscitation. Resuscitation 2009, 80, 755–761. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Epinephrine (n = 10) | Vasopressin (n = 9) |
|---|---|---|
| Weight (Kg) | 4.3 ± 1.2 | 4.3 ± 0.7 |
| Sex | 5 F, 5 M | 7 F, 2 M |
| Baseline pH | 7.21 ± 0.24 | 7.24 ± 0.06 |
| Baseline PaCO2 (mm Hg) | 66 ± 21 | 63 ± 2 |
| Baseline PaO2 (mm Hg) | 20 ± 3 | 22 ± 6 |
| Baseline Lactate (mM/L) | 3 ± 1 | 3 ± 1 |
| Baseline CA Flow (mL/kg/min) | 24 ± 5 | 29 ± 12 |
| Baseline PA Flow (mL/kg/min) | 19 ± 18 | 19 ± 15 |
| Time to Asystole (min) | 14 ± 6 | 16 ± 5 |
| Arterial pH at asystole | 6.88 ± 0.06 | 6.86 ± 0.05 |
| PaCO2 (mm Hg) at asystole | 139 ± 16 | 135 ± 14 |
| PaO2 (mm Hg) at asystole | 6 ± 3 | 7 ± 3 |
| Arterial Lactate (mM/L) at asystole | 9 ± 1.5 | 9 ± 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rawat, M.; Gugino, S.; Koenigsknecht, C.; Helman, J.; Nielsen, L.; Sankaran, D.; Nair, J.; Chandrasekharan, P.; Lakshminrusimha, S. Masked Randomized Trial of Epinephrine versus Vasopressin in an Ovine Model of Perinatal Cardiac Arrest. Children 2023, 10, 349. https://doi.org/10.3390/children10020349
Rawat M, Gugino S, Koenigsknecht C, Helman J, Nielsen L, Sankaran D, Nair J, Chandrasekharan P, Lakshminrusimha S. Masked Randomized Trial of Epinephrine versus Vasopressin in an Ovine Model of Perinatal Cardiac Arrest. Children. 2023; 10(2):349. https://doi.org/10.3390/children10020349
Chicago/Turabian StyleRawat, Munmun, Sylvia Gugino, Carmon Koenigsknecht, Justin Helman, Lori Nielsen, Deepika Sankaran, Jayasree Nair, Praveen Chandrasekharan, and Satyan Lakshminrusimha. 2023. "Masked Randomized Trial of Epinephrine versus Vasopressin in an Ovine Model of Perinatal Cardiac Arrest" Children 10, no. 2: 349. https://doi.org/10.3390/children10020349