
The Relationship between Dietary Habits and Periodontal Pathogens in a Sample of Romanian Children and Adolescents: A Cross-Sectional Study


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Study Design and Participants
2.3. Questionnaire
2.4. Periodontal Pathogens
2.5. Statistical Analysis
3. Results
- -
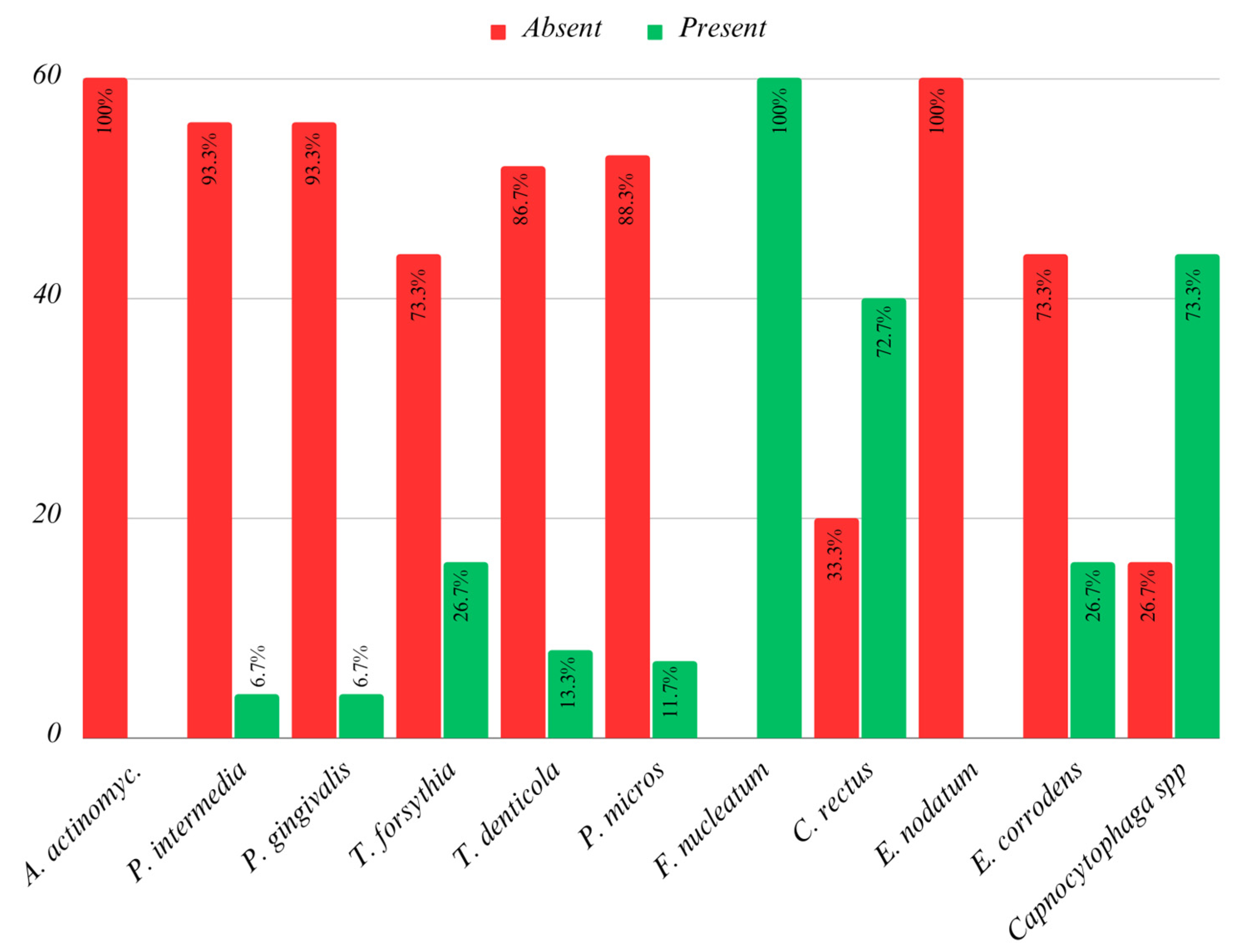
- A. actinomycetemcomitans was absent in 100% of cases.
- -
- P. intermedia was found in 6.7% of cases.
- -
- P. gingivalis was detected in 6.6% of cases.
- -
- T. forsythia was present in 26.7% of cases.
- -
- F. nucleatum/periodonticum was found in 100% of cases.
- -
- E. corrodens was present in 26.7% of cases.

- -
- Tannerella forsythia: A lack of breastfeeding was significantly more frequently associated with positive results, indicating its presence in the collected samples.
- -
- Fusobacterium nucleatum: Breastfeeding durations of up to 3 months and up to 12 months were significantly more frequently associated with results indicating its presence in the collected samples.
- -
- Campylobacter rectus: A lack of breastfeeding was significantly more frequently associated with results indicating the presence of this microorganism in the subgingival samples. Simultaneously, a duration of breastfeeding of up to 6 months was significantly more frequently associated with results indicating its absence from the collected samples.
- -
- Eikenella corrodens: A lack of breastfeeding was significantly more frequently associated with its presence in the collected samples. Conversely, a duration of breastfeeding of up to 18 months was significantly more frequently associated with its absence from the collected samples.

{kind=link}
{kind=link}
{kind=link}
| P. intermedia | P. gingivalis | T. forsythia | T. denticola | P. micros | F. nucleatum | C. rectus | E. corrodens | Capnocytophaga spp. | |
|---|---|---|---|---|---|---|---|---|---|
| Duration | Negative | ||||||||
| No breastf. | 10 (17.9%) | 12 (21.4%) | 6 (13.6%) | 8 (15.4%) | 9 (17.0%) | 0 (0.0%) | 0 (0.0%) | 5 (11.4%) | 4 (25.0%) |
| 3 months | 6 (10.7%) | 6 (10.7%) | 6 (13.6%) | 6 (11.5%) | 6 (11.3%) | 0 (0.0%) | 2 (10.0%) | 6 (13.6%) | 0 (0.0%) |
| 6 months | 12 (21.4%) | 10 (17.9%) | 8 (18.2%) | 12 (23.1%) | 10 (18.9%) | 0 (0.0%) | 8 (40.0%) | 10 (22.7%) | 6 (37.5%) |
| 12 months | 7 (12.5%) | 7 (12.5%) | 7 (15.9%) | 7 (13.5%) | 7 (13.2%) | 0 (0.0%) | 2 (10.0%) | 4 (9.1%) | 2 (12.5%) |
| 18 months | 11 (19.6%) | 11 (19.6%) | 7 (15.9%) | 9 (17.3%) | 11 (20.8%) | 0 (0.0%) | 6 (30.0%) | 11 (25.0%) | 4 (25.0%) |
| >18 months | 10 (17.9%) | 10 (17.9%) | 10 (22.7%) | 10 (19.2%) | 10 (18.9%) | 0 (0.0%) | 2 (10.0%) | 8 (18.2%) | 0 (0.0%) |
| Weak positive | |||||||||
| No breastf. | 0 (0.0%) | 0 (0.0%) | 2 (25.0%) | 4 (50.0%) | 1 (20.0%) | 7 (38.9%) | 7 (26.9%) | 7 (43.8%) | 3 (12.5%) |
| 3 months | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 4 (15.4%) | 0 (0.0%) | 6 (25.0%) |
| 6 months | 0 (0.0%) | 2 (100%) | 2 (25.0%) | 2 (25.0%) | 4 (80.0%) | 2 (11.1%) | 2 (7.7%) | 4 (25.0%) | 5 (20.8%) |
| 12 months | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 3 (16.7%) | 2 (7.7%) | 3 (18.8%) | 1 (4.2%) |
| 18 months | 0 (0.0%) | 0 (0.0%) | 4 (50.0%) | 2 (25.0%) | 0 (0.0%) | 5 (27.8%) | 3 (11.5%) | 0 (0.0%) | 4 (16.7%) |
| >18 months | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (5.6%) | 8 (30.8%) | 2 (12.5%) | 5 (20.8%) |
| Positive | |||||||||
| No breastf. | 2 (50.0%) | 0 (0.0%) | 4 (50.0%) | 0 (0.0%) | 2 (100%) | 5 (13.2%) | 5 (35.7%) | 0 (0.0%) | 3 (18.8%) |
| 3 months | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 4 (10.5%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 6 months | 2 (50.0%) | 2 (100%) | 4 (50.0%) | 0 (0.0%) | 0 (0.0%) | 12 (31.6%) | 4 (28.6%) | 0 (0.0%) | 3 (18.8%) |
| 12 months | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 2 (5.3%) | 3 (21.4%) | 0 (0.0%) | 3 (18.8%) |
| 18 months | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 6 (15.8%) | 2 (14.3%) | 0 (0.0%) | 3 (18.8%) |
| >18 months | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 9 (23.7%) | 0 (0.0%) | 0 (0.0%) | 4 (25.0%) |
| Intense positive | |||||||||
| No breastf. | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 2 (50.0%) |
| 3 months | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 2 (50.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 6 months | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 12 months | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 2 (50.0%) | 0 (0.0%) | 0 (0.0%) | 1 (25.0%) |
| 18 months | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| >18 months | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (25.0%) |
| p * | 0.494 | 0.272 | 0.019 | 0.219 | 0.071 | 0.002 | 0.002 | 0.013 | 0.087 |
- -
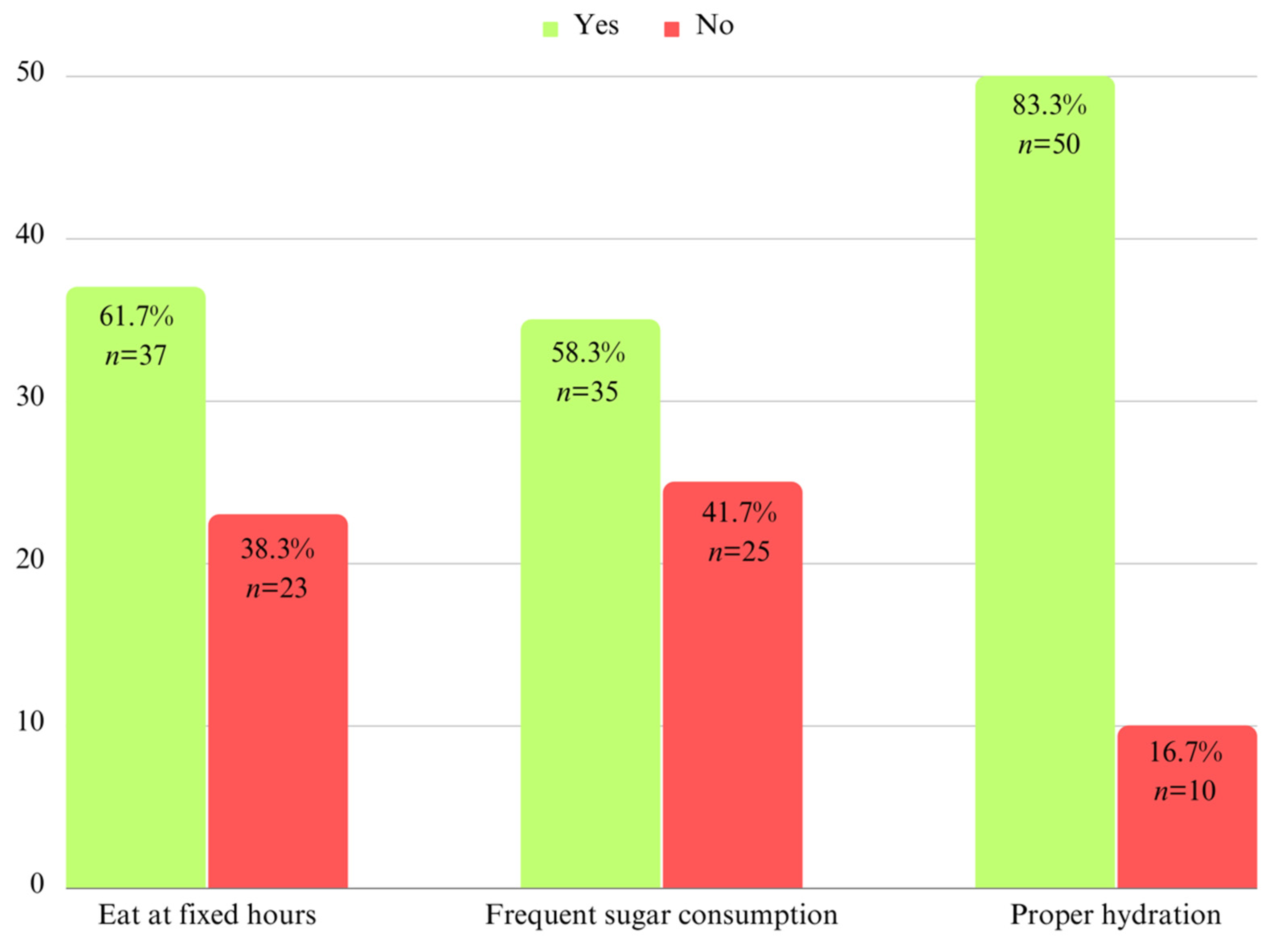
- Feeding at Fixed Hours: Statistically significant results were observed for P. intermedia (p = 0.018), P. micros (p = 0.027), and F. nucleatum (p = 0.031).
- P. intermedia and F. nucleatum: Feeding at fixed hours was significantly more frequently associated with the presence of these microorganisms.
- P. micros: The lack of feeding at fixed hours was significantly more frequently associated with results indicating the presence of this microorganism in the collected samples.
- -
- Frequent Consumption of Sweets: Statistically significant results were only observed for Capnocytophaga spp. (p = 0.007). This microorganism was found in children with a frequent consumption of sweets.
- -
- Proper Hydration: Statistically significant results were obtained for T. forsythia (p = 0.031), P. micros (p = 0.005), and Capnocytophaga spp. (p = 0.008).
- T. forsythia, P. micros, and Capnocytophaga spp.: The presence of these microorganisms was noted in children who did not maintain age-appropriate hydration.
| P. intermedia | P. gingivalis | T. forsythia | T. denticola | P. micros | F. nucleatum | C. rectus | E. corrodens | Capnocytophaga spp. | |
|---|---|---|---|---|---|---|---|---|---|
| Fixed hours | Negative | ||||||||
| No | 19 (33.9%) | 23 (41.1%) | 13 (29.5%) | 19 (36.5%) | 21 (39.6%) | 0 (0.0%) | 8 (40.0%) | 16 (36.4%) | 8 (50.0%) |
| Yes | 37 (66.1%) | 33 (58.9%) | 31 (70.5%) | 33 (63.5%) | 32 (60.45) | 0 (0.0%) | 12 (60.0%) | 28 (63.6%) | 8 (50.0%) |
| Weak positive | |||||||||
| No | 0 (0.0%) | 0 (0.0%) | 4 (50.0%) | 4 (50.0%) | 0 (0.0%) | 11 (47.8%) | 9 (34.6%) | 7 (43.8%) | 6 (25.0%) |
| Yes | 0 (0.0%) | 2 (100%) | 4 (50.0%) | 4 (50.0%) | 5 (100%) | 7 (52.2%) | 17 (65.4%) | 9 (56.3%) | 18 (75.0%) |
| Positive | |||||||||
| No | 4 (100%) | 0 (0.0%) | 6 (75.0%) | 0 (0.0%) | 2 (100%) | 12 (52.5%) | 6 (42.9%) | 0 (0.0%) | 3 (37.5%) |
| Yes | 0 (0.0%) | 2 (100%) | 2 (25.0%) | 0 (0.0%) | 0 (0.0%) | 26 (47.5%) | 8 (57.1%) | 0 (0.0%) | 10 (62.5%) |
| Intense positive | |||||||||
| No | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 3 (75.0%) |
| Yes | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 4 (100%) | 0 (0.0%) | 0 (0.0%) | 1 (25.0%) |
| p * | 0.018 | 0.403 | 0.057 | 0.468 | 0.027 | 0.031 | 0.839 | 0.765 | 0.165 |
| Sweets | Negative | ||||||||
| No | 23 (41.1%) | 23 (41.1%) | 17 (38.6%) | 19 (36.5%) | 21 (39.6%) | 0 (0.0%) | 8 (40.0%) | 20 (45.5%) | 12 (75.0%) |
| Yes | 33 (58.9%) | 33 (58.9%) | 27 (61.4%) | 33 (63.5%) | 32 (60.4%) | 0 (0.0%) | 12 (60.0%) | 24 (54.5%) | 4 (25.0%) |
| Weak positive | |||||||||
| No | 0 (0.0%) | 0 (0.0%) | 2 (25.0%) | 6 (75.0%) | 4 (80.0%) | 7 (38.9%) | 12 (46.2%) | 5 (31.3%) | 7 (29.2%) |
| Yes | 0 (0.0%) | 2 (100%) | 6 (75.0%) | 2 (25.0%) | 1 (20.0%) | 11 (61.1%) | 14 (53.8%) | 11 (68.7%) | 17 (70.8%) |
| Positive | |||||||||
| No | 2 (50.0%) | 2 (100%) | 6 (75.0%) | 0 (0.0%) | 0 (0.0%) | 18 (47.4%) | 5 (35.7%) | 0 (0.0%) | 6 (37.5%) |
| Yes | 2 (50.0%) | 0 (0.0%) | 2 (25.0%) | 0 (0.0%) | 2 (100%) | 20 (52.6%) | 9 (64.35) | 0 (0.0%) | 10 (62.5%) |
| Intense positive | |||||||||
| No | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Yes | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 4 (100%) | 0 (0.0%) | 0 (0.0%) | 4 (100%) |
| p * | 1.000 | 0.148 | 0.107 | 0.057 | 0.111 | 0.208 | 0.842 | 0.386 | 0.007 |
| Hydration | Negative | ||||||||
| No | 10 (17.9%) | 10 (17.9%) | 6 (13.6%) | 8 (15.4%) | 6 (11.3%) | 0 (0.0%) | 4 (20.0%) | 8 (18.2%) | 4 (25.0%) |
| Yes | 46 (82.1%) | 46 (82.1%) | 38 (86.4%) | 44 (84.6%) | 47 (88.7%) | 0 (0.0%) | 16 (80.0%) | 36 (81.8%) | 12 (75.0%) |
| Weak positive | |||||||||
| No | 0 (0.0%) | 0 (0.0%) | 4 (50.0%) | 2 (25.0%) | 2 (40.0%) | 5 (27.8%) | 3 (11.5%) | 2 (12.5%) | 1 (4.2%) |
| Yes | 0 (0.0%) | 2 (100%) | 4 (50.0%) | 6 (75.0%) | 3 (60.0%) | 13 (72.2%) | 23 (88.5%) | 14 (87.5%) | 23 (95.8%) |
| Positive | |||||||||
| No | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 2 (100%) | 5 (13.2%) | 3 (21.4%) | 0 (0.0%) | 2 (12.5%) |
| Yes | 4 (100%) | 2 (100%) | 8 (100%) | 0 (0.0%) | 0 (0.0%) | 33 (86.8%) | 11 (78.6%) | 0 (0.0%) | 14 (87.5%) |
| Intense positive | |||||||||
| No | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 3 (75.0%) |
| Yes | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 4 (100%) | 0 (0.0%) | 0 (0.0%) | 1 (25.0%) |
| p * | 1.000 | 1.000 | 0.031 | 1.000 | 0.005 | 0.349 | 0.740 | 0.715 | 0.008 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fan, W.; Liu, C.; Zhang, Y.; Yang, Z.; Li, J.; Huang, S. Epidemiology and associated factors of gingivitis in adolescents in Guangdong Province, Southern China: A cross-sectional study. BMC Oral Health 2021, 21, 311. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S. EFP Workshop Participants and Methodological Consultants. Treatment of stage I–III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Xu, J.; Li, S.; Wang, X.; Liu, J.; Li, X. The prevalence of gingivitis and related risk factors in schoolchildren aged 6–12 years old. BMC Oral Health 2022, 22, 623. [Google Scholar] [CrossRef]
- Funieru, C.; Klinger, A.; Băicuș, C.; Funieru, E.; Dumitriu, H.T.; Dumitriu, A. Epidemiology of gingivitis in schoolchildren in Bucharest, Romania: A cross-sectional study. J. Periodontal Res. 2017, 52, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Primers 2017, 3, 17038. [Google Scholar] [CrossRef] [PubMed]
- Marsh, P.D. Dental plaque as a biofilm: The significance of pH in health and caries. Compend. Contin. Educ. Dent. 2009, 30, 76–78, 80, 83–87; quiz 88, 90. [Google Scholar] [PubMed]
- Morrison, A.G.; Sarkar, S.; Umar, S.; Lee, S.T.M.; Thomas, S.M. The Contribution of the Human Oral Microbiome to Oral Disease: A Review. Microorganisms 2023, 11, 318. [Google Scholar] [CrossRef]
- Scannapieco, F.A.; Dongari-Bagtzoglou, A. Dysbiosis revisited: Understanding the role of the oral microbiome in the pathogenesis of gingivitis and periodontitis: A critical assessment. J. Periodontol. 2021, 92, 1071–1078. [Google Scholar] [CrossRef]
- Shahoumi, L.A.; Saleh, M.H.A.; Meghil, M.M. Virulence Factors of the Periodontal Pathogens: Tools to Evade the Host Immune Response and Promote Carcinogenesis. Microorganisms 2023, 11, 115. [Google Scholar]
- Santigli, E.; Leitner, E.; Wimmer, G.; Kessler, H.H.; Feierl, G.; Grube, M.; Eberhard, K.; Klug, B. Accuracy of commercial kits and published primer pairs for the detection of periodontopathogens. Clin. Oral Investig. 2016, 20, 2515–2528. [Google Scholar] [CrossRef]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Zohaib, S.; Almas, K. The Role of Nutrition in Periodontal Health: An Update. Nutrients 2016, 8, 530. [Google Scholar] [CrossRef] [PubMed]
- Martinon, P.; Fraticelli, L.; Giboreau, A.; Dussart, C.; Bourgeois, D.; Carrouel, F. Nutrition as a Key Modifiable Factor for Periodontitis and Main Chronic Diseases. J. Clin. Med. 2021, 10, 197. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.R.O.; Batista, R.F.L.; Ladeira, L.L.C.; Thomaz, E.B.A.F.; Alves, C.M.C.; Saraiva, M.C.; Silva, A.A.M.; Brondani, M.A.; Ribeiro, C.C.C. Higher sugar intake is associated with periodontal disease in adolescents. Clin. Oral Investig. 2021, 25, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, P. Sugars and Dental Caries: Evidence for Setting a Recommended Threshold for Intake. Adv. Nutr. 2016, 7, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Rippe, J.M.; Angelopoulos, T.J. Relationship between Added Sugars Consumption and Chronic Disease Risk Factors: Current Understanding. Nutrients 2016, 8, 697. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-R. Analysis of the Effect of Daily Water Intake on Oral Health: Result from Seven Waves of a Population-Based Panel Study. Water 2021, 13, 2716. [Google Scholar] [CrossRef]
- Taba, M., Jr.; Souza, S.L.; Mariguela, V.C. Periodontal disease: A genetic perspective. Braz. Oral Res. 2012, 26, 32–38. [Google Scholar] [CrossRef]
- Sulyanto, R.M.; Thompson, Z.A.; Beall, C.J.; Leys, E.J.; Griffen, A.L. The Predominant Oral Microbiota Is Acquired Early in an Organized Pattern. Sci. Rep. 2019, 9, 10550. [Google Scholar] [CrossRef]
- Šutej, I.; Božić, D.; Peroš, K.; Plančak, D. Cigarette smoking and its consequences on periodontal health in teenagers: A cross-sectional study. Cent. Eur. J. Public Health 2021, 29, 311–316. [Google Scholar] [CrossRef]
- Ogbanga, N.; Nelson, A.; Ghignone, S.; Voyron, S.; Lovisolo, F.; Sguazzi, G.; Renò, F.; Migliario, M.; Gino, S.; Procopio, N. The Oral Microbiome for Geographic Origin: An Italian Study. Forensic Sci. Int. Genet. 2023, 64, 102841. [Google Scholar] [CrossRef]
- Al-Tairi, N.; Al-Radom, J. Prevalence and etiology of pediatric maxillofacial fractures in a group of Yemeni children and adolescents. Open J. Stomatol. 2021, 11, 179–187. [Google Scholar] [CrossRef]
- Available online: https://www.healthline.com/health/how-much-water-should-I-drink#recommendations (accessed on 2 September 2023).
- Available online: https://www.hain-lifescience.de/produkte/mikrobiologie/dental/micro-ident-und-micro-identplus.html (accessed on 2 September 2023).
- Urbán, E.; Terhes, G.; Radnai, M.; Gorzó, I.; Nagy, E. Detection of periodontopathogenic bacteria in pregnant women by traditional anaerobic culture method and by a commercial molecular genetic method. Anaerobe 2010, 16, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Mboowa, G.; Ocheng, F.; Okeng, A.; Bwanga, F. Periodontopathogenic bacterial species among patients with periodontal diseases at Mulago Hospital Dental Clinic in Kampala, Uganda: A cross-section study. J. Dent. Oral Hyg. 2014, 6, 58–63. [Google Scholar]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Chen, H.; Zhang, R.; Cheng, R.; Xu, T.; Zhang, T.; Hong, X.; Zhao, X.; Wu, Y.; Cheng, L.; Hu, T. Gingival bleeding and calculus among 12-year-old Chinese adolescents: A multilevel analysis. BMC Oral Health 2020, 20, 147. [Google Scholar] [CrossRef] [PubMed]
- Jaghasi, I.; Hatahet, W.; Dashash, M. Dietary patterns and oral health in schoolchildren from Damascus, Syrian Arab Republic. East. Mediterr. Health J. 2012, 18, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Kusama, T.; Nakazawa, N.; Takeuchi, K.; Kiuchi, S.; Osaka, K. Free Sugar Intake and Periodontal Diseases: A Systematic Review. Nutrients 2022, 14, 4444. [Google Scholar] [CrossRef] [PubMed]
- Fidler Mis, N.; Braegger, C.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.D.; Hojsak, I.; Hulst, J.; Indrio, F.; Lapillonne, A.; et al. Sugar in Infants, Children and Adolescents: A Position Paper of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 681–696. [Google Scholar] [CrossRef]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef]
- Larson, N.; Story, M. A review of snacking patterns among children and adolescents: What are the implications of snacking for weight status? Child Obes. 2013, 9, 104–115. [Google Scholar] [CrossRef]
- Fulkerson, J.A.; Neumark-Sztainer, D.; Story, M. Adolescent and parent views of family meals. J. Am. Diet Assoc. 2006, 106, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Boyland, E.J.; Nolan, S.; Kelly, B.; Tudur-Smith, C.; Jones, A.; Halford, J.C.; Robinson, E. Advertising as a cue to consume: A systematic review and meta-analysis of the effects of acute exposure to unhealthy food and nonalcoholic beverage advertising on intake in children and adults. Am. J. Clin. Nutr. 2016, 103, 519–533. [Google Scholar] [CrossRef] [PubMed]
- Cortelli, J.R.; Fernandes, C.B.; Costa, F.O.; Cortelli, S.C.; Kajiya, M.; Howell, S.C.; Kawai, T. Detection of periodontal pathogens in newborns and children with mixed dentition. Eur. J. Clin. Microbiol. Infect Dis. 2011, 31, 1041–1050. [Google Scholar] [CrossRef] [PubMed]
- Ballesta-Mudarra, S.; Machuca-Portillo, G.; Torres-Lagares, D.; Rodríguez-Caballero, Á.; Yáñez-Vico, R.M.; Solano-Reina, E.; Perea-Pérez, E. Determination of periodontopathogens in patients with Cri du chat syndrome. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e883–e887. [Google Scholar] [CrossRef] [PubMed]
- Motoc, G.V.; Juncar, R.I.; Moca, A.E.; Motoc, O.; Vaida, L.L.; Juncar, M. The Relationship between Age, Gender, BMI, Diet, Salivary pH and Periodontal Pathogenic Bacteria in Children and Adolescents: A Cross-Sectional Study. Biomedicines 2023, 11, 2374. [Google Scholar] [CrossRef] [PubMed]
- Untch, M.; Schlagenhauf, U. Inter- and intra-test agreement of three commercially available molecular diagnostic tests for the identification of periodontal pathogens. Clin. Oral Investig. 2015, 19, 2045–2052. [Google Scholar] [CrossRef]
- Calniceanu, H.; Stratul, S.I.; Rusu, D.; Jianu, A.; Boariu, M.; Nica, L.; Ogodescu, A.; Sima, L.; Bolintineanu, S.; Anghel, A.; et al. Changes in clinical and microbiological parameters of the periodontium during initial stages of orthodontic movement in patients with treated severe periodontitis: A longitudinal site-level analysis. Exp. Ther. Med. 2020, 20, 199. [Google Scholar] [CrossRef]
- Bale, B.F.; Doneen, A.L.; Vigerust, D.J. High-risk periodontal pathogens contribute to the pathogenesis of atherosclerosis. Postgrad. Med. J. 2017, 93, 215–220. [Google Scholar] [CrossRef]
- Fukui, K.; Kato, N.; Kato, H.; Watanabe, K.; Tatematsu, N. Incidence of Prevotella intermedia and Prevotella nigrescens carriage among family members with subclinical periodontal disease. J. Clin. Microbiol. 1999, 37, 3141–3145. [Google Scholar] [CrossRef]
- Riggio, M.P.; Lennon, A.; Smith, A. Detection of Peptostreptococcus micros DNA in clinical samples by PCR. J. Med. Microbiol. 2001, 50, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Lohinai, Z.; Keremi, B.; Szöko, E.; Tábi, T.; Szabo, C.; Tulassay, Z.; DiCesare, J.C.; Davis, C.A.; Collins, L.M.; Levine, M. Biofilm Lysine Decarboxylase, a New Therapeutic Target for Periodontal Inflammation. J. Periodontol. 2015, 86, 1176–1184. [Google Scholar] [CrossRef] [PubMed]
- Shiga, Y.; Hosomi, N.; Nezu, T.; Nishi, H.; Aoki, S.; Nakamori, M.; Ishikawa, K.; Kinoshita, N.; Imamura, E.; Ueno, H.; et al. Association between periodontal disease due to Campylobacter rectus and cerebral microbleeds in acute stroke patients. PLoS ONE 2020, 15, e0239773. [Google Scholar] [CrossRef] [PubMed]
- Lalla, E.; Kaplan, S.; Chang, S.M.; Roth, G.A.; Celenti, R.; Hinckley, K.; Greenberg, E.; Papapanou, P.N. Periodontal infection profiles in type 1 diabetes. J. Clin. Periodontol. 2006, 33, 855–862. [Google Scholar] [CrossRef]
- Jolivet-Gougeon, A.; Bonnaure-Mallet, M. Screening for prevalence and abundance of Capnocytophaga spp. by analyzing NGS data: A scoping review. Oral Dis. 2021, 27, 1621–1630. [Google Scholar] [CrossRef] [PubMed]
- Wehrens, S.M.T.; Christou, S.; Isherwood, C.; Middleton, B.; Gibbs, M.A.; Archer, S.N.; Skene, D.J.; Johnston, J.D. Meal Timing Regulates the Human Circadian System. Curr. Biol. 2017, 27, 1768–1775.e3. [Google Scholar] [CrossRef] [PubMed]
- Paoli, A.; Tinsley, G.; Bianco, A.; Moro, T. The Influence of Meal Frequency and Timing on Health in Humans: The Role of Fasting. Nutrients 2019, 11, 719. [Google Scholar] [CrossRef] [PubMed]
- Galczak-Kondraciuk, A.; Stempel, P.; Czeczelewski, J. Assessment of nutritional behaviours of children aged 7-12 attending to primary schools in Biala Podlaska, Poland. Rocz. Panstw. Zakl. Hig. 2018, 69, 71–77. [Google Scholar] [PubMed]
- Tennert, C.; Reinmuth, A.C.; Bremer, K.; Al-Ahmad, A.; Karygianni, L.; Hellwig, E.; Vach, K.; Ratka-Krüger, P.; Wittmer, A.; Woelber, J.P. An oral health optimized diet reduces the load of potential cariogenic and periodontal bacterial species in the supragingival oral plaque: A randomized controlled pilot study. Microbiologyopen 2020, 9, e1056. [Google Scholar] [CrossRef]
- Gupta, V.; Dawar, A.; Bhadauria, U.S.; Purohit, B.M.; Nilima, N. Sugar-sweetened beverages and periodontal disease: A systematic review. Oral Dis. 2022; ahead of print. [Google Scholar] [CrossRef]
- Hong, J.; Whelton, H.; Douglas, G.; Kang, J. Consumption frequency of added sugars and UK children’s dental caries. Community Dent. Oral Epidemiol. 2018, 46, 457–464. [Google Scholar] [CrossRef]
- García-Quintana, A.; Frattaroli-Pericchi, A.; Feldman, S.; Luengo, J.; Acevedo, A.M. Initial oral microbiota and the impact of delivery mode and feeding practices in 0 to 2 month-old infants. Braz. Oral Res. 2023, 37, e078. [Google Scholar] [CrossRef]
- Arishi, R.A.; Lai, C.T.; Geddes, D.T.; Stinson, L.F. Impact of breastfeeding and other early-life factors on the development of the oral microbiome. Front. Microbiol. 2023, 14, 1236601. [Google Scholar] [CrossRef]


| P. intermedia | P. gingivalis | T. forsythia | T. denticola | P. micros | F. nucleatum | C. rectus | E. corrodens | Capnocytophaga spp. | |
|---|---|---|---|---|---|---|---|---|---|
| Meals/day | Negative | ||||||||
| 4 | 30 (53.6%) | 30 (53.6%) | 24 (54.5%) | 28 (53.8%) | 29 (54.7%) | 9 (50.0%) | 12 (60.0%) | 25 (56.8%) | 6 (37.5%) |
| 5 | 13 (23.2%) | 13 (23.2%) | 13 (29.5%) | 13 (25.0%) | 11 (20.8%) | 3 (16.7%) | 2 (10.0%) | 9 (20.5%) | 2 (12.5%) |
| >5 | 13 (23.2%) | 13 (23.2%) | 7 (16.0%) | 11 (21.2%) | 13 (24.5%) | 6 (33.3%) | 6 (30.0%) | 10 (22.7%) | 8 (50.0%) |
| Weak positive | |||||||||
| 4 | 0 (0.0%) | 0 (0.0%) | 4 (50.0%) | 4 (50.0%) | 3 (60.0%) | 0 (0.0%) | 15 (57.7%) | 7 (43.8%) | 22 (91.6%) |
| 5 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 2 (40.0%) | 0 (0.0%) | 6 (23.1%) | 4 (25.0%) | 1 (4.2%) |
| >5 | 0 (0.0%) | 2 (100%) | 4 (50.0%) | 4 (50.0%) | 0 (0.0%) | 0 (0.0%) | 5 (19.2%) | 5 (31.3%) | 1 (4.2%) |
| Positive | |||||||||
| 4 | 2 (50.0%) | 2 (100%) | 4 (50.0%) | 0 (0.0%) | 0 (0.0%) | 20 (52.65) | 5 (35.7%) | 0 (0.0%) | 2 (12.5%) |
| 5 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 9 (23.7%) | 5 (35.7%) | 0 (0.0%) | 10 (62.5%) |
| >5 | 2 (50.0%) | 0 (0.0%) | 4 (50.0%) | 0 (0.0%) | 2 (100%) | 9 (23.7%) | 4 (28.6%) | 0 (0.0%) | 4 (25.0%) |
| Intense positive | |||||||||
| 4 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 3 (75.05) | 0 (0.0%) | 0 (0.0%) | 2 (50.0%) |
| 5 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (25.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| >5 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 2 (50.0%) |
| p * | 0.517 | 0.208 | 0.030 | 0.102 | 0.099 | 0.809 | 0.363 | 0.681 | <0.001 |
| Sweets/day | Negative | ||||||||
| 1 | 35 (62.5%) | 33 (58.9%) | 25 (56.8%) | 29 (55.8%) | 33 (62.3%) | 0 (0.0%) | 16 (80.0%) | 29 (65.9%) | 16 (100%) |
| 2–3 | 20 (35.7%) | 22 (39.3%) | 18 (40.9%) | 22 (42.3%) | 19 (35.85) | 0 (0.0%) | 4 (20.0%) | 14 (31.8%) | 0 (0.0%) |
| >3 | 1 (1.8%) | 1 (1.8%) | 1 (2.3%) | 1 (1.9%) | 1 (1.9%) | 0 (0.0%) | 0 (0.0%) | 1 (2.3%) | 0 (0.0%) |
| Weak positive | |||||||||
| 1 | 0 (0.0%) | 2 (100%) | 6 (75.0%) | 8 (100%) | 4 (80.0%) | 9 (50.0%) | 15 (57.7%) | 8 (50.0%) | 10 (41.75) |
| 2–3 | 0 (0.0%) | 0 (0.0%) | 2 (25.0%) | 0 (0.0%) | 1 (20.0%) | 8 (44.4%) | 11 (42.3%) | 8 (50.0%) | 14 (58.3%) |
| >3 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (5.6%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Positive | |||||||||
| 1 | 2 (50.0%) | 2 (100%) | 6 (75.0%) | 0 (0.0%) | 0 (0.0%) | 27 (71.1%) | 6 (42.9%) | 0 (0.0%) | 10 (62.5%) |
| 2–3 | 2 (50.0%) | 0 (0.0%) | 2 (25.0%) | 0 (0.0%) | 2 (100%) | 11 (28.9%) | 7 (50.0%) | 0 (0.0%) | 6 (37.5%) |
| >3 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (7.1%) | 0 (0.0%) | 0 (0.0%) |
| Intense positive | |||||||||
| 1 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (25.0%) | 0 (0.0%) | 0 (0.0%) | 1 (25.0%) |
| 2–3 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 3 (75.0%) | 0 (0.0%) | 0 (0.0%) | 2 (50.0%) |
| >3 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (25.0%) |
| p * | 0.649 | 0.439 | 0.642 | 0.030 | 0.267 | 0.102 | 0.079 | 0.443 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Motoc, G.V.; Juncar, R.I.; Moca, A.E.; Motoc, O.; Moca, R.T.; Țig, I.A.; Vaida, L.L.; Juncar, M. The Relationship between Dietary Habits and Periodontal Pathogens in a Sample of Romanian Children and Adolescents: A Cross-Sectional Study. Children 2023, 10, 1779. https://doi.org/10.3390/children10111779
Motoc GV, Juncar RI, Moca AE, Motoc O, Moca RT, Țig IA, Vaida LL, Juncar M. The Relationship between Dietary Habits and Periodontal Pathogens in a Sample of Romanian Children and Adolescents: A Cross-Sectional Study. Children. 2023; 10(11):1779. https://doi.org/10.3390/children10111779
Chicago/Turabian StyleMotoc, Georgiana Veronica, Raluca Iulia Juncar, Abel Emanuel Moca, Ovidiu Motoc, Rahela Tabita Moca, Ioan Andrei Țig, Luminița Ligia Vaida, and Mihai Juncar. 2023. "The Relationship between Dietary Habits and Periodontal Pathogens in a Sample of Romanian Children and Adolescents: A Cross-Sectional Study" Children 10, no. 11: 1779. https://doi.org/10.3390/children10111779