
Diagnosis and Management of Cancer Treatment-Related Cardiac Dysfunction and Heart Failure in Children


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Pathophysiology of Cardiovascular Toxicity in Cancer Patients
2.1. Anthracyclines
2.2. Non-Anthracycline Agents
2.3. Radiation-Related Cardiotoxicity
2.4. Targeted Cancer Therapies
2.5. Hematopoietic Stem Cell Transplantation and Cellular Therapy
3. Oncological Cardiomyopathy and Heart Failure
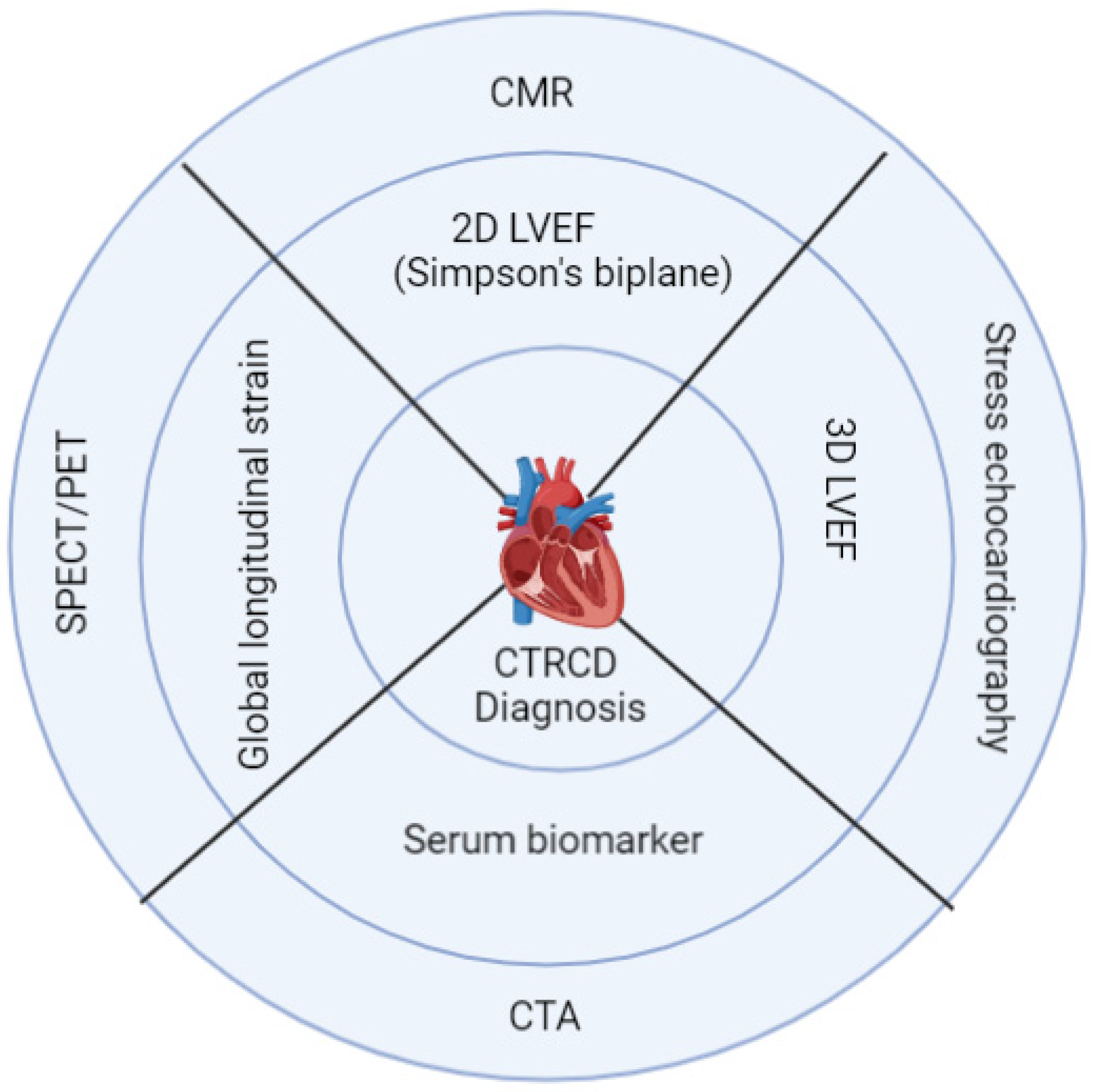
4. Diagnosis and Risk Stratification
4.1. Cardiac Biomarkers
4.2. Role of Echocardiography
4.2.1. 2D Echocardiography
4.2.2. 3D Echocardiography
4.2.3. Speckle-Tracking Global Longitudinal Strain
4.2.4. Tissue Doppler Imaging
4.2.5. Role of the Stress Test and Stress-Echocardiography
4.3. Role of CMR
4.4. Role of Cardiac Catheterization
4.5. Role of Advanced Imaging CT/SPECT/PET
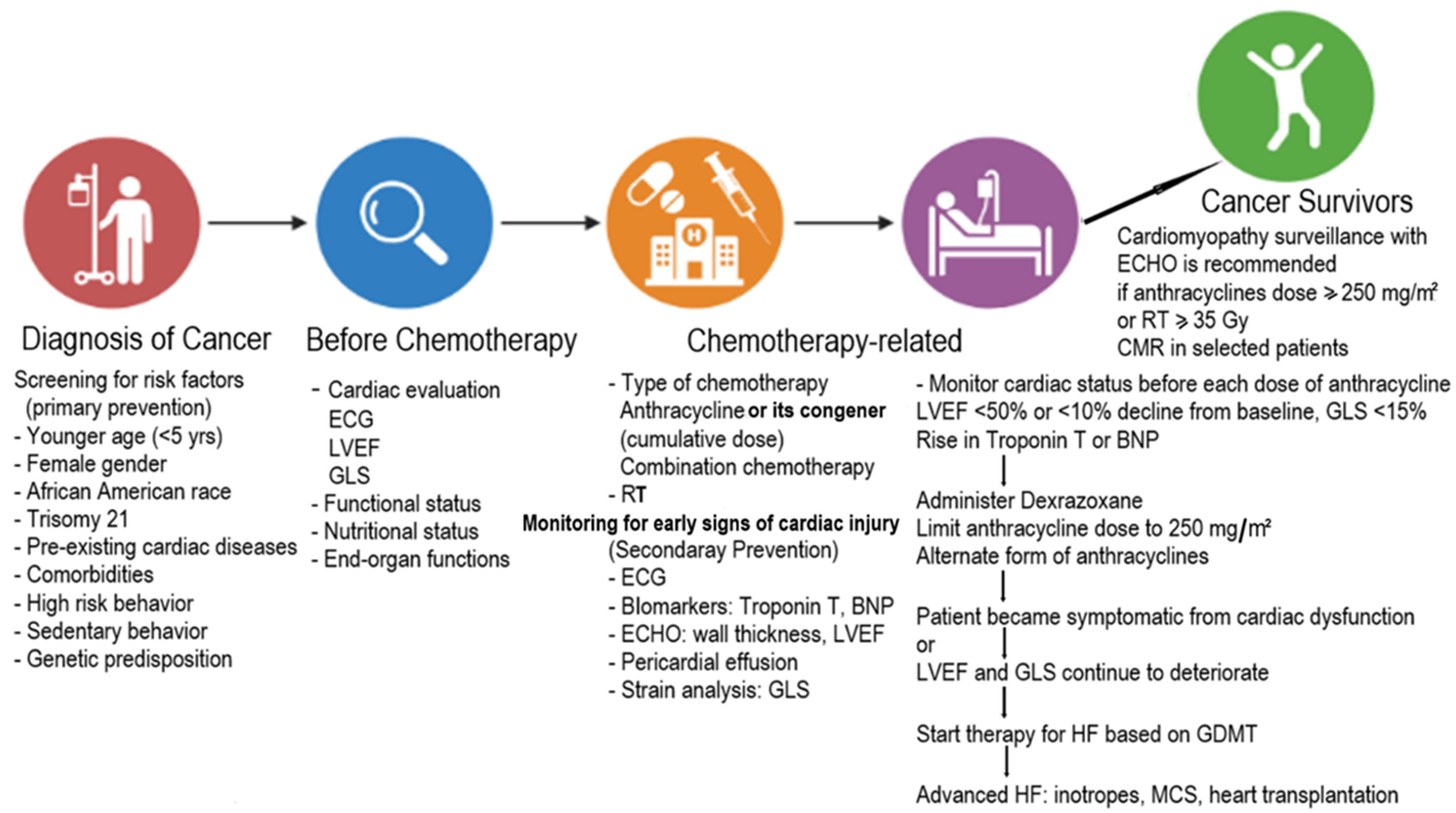
5. Management
5.1. Prevention
5.2. Treatment of HF
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Philadelphia: American Association for Cancer Research. Available online: http://www.CancerProgressReport.org (accessed on 30 September 2022).
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease 2019 Cancer Collaboration; Kocarnik, J.M.; Compton, K.; Dean, F.E.; Fu, W.; Gaw, B.L. Cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life years for 29 cancer groups from 2010 to 2019: A systematic analysis for the global burden of disease study 2019. JAMA Oncol. 2022, 8, 420–444. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Minotti, G.; Carver, J.; Franco, V.I. An Invitation from the Editors of Cardio-Oncology. Cardio-Oncology 2015, 1, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheuk, D.K.; Sieswerda, E.; van Dalen, E.C.; Postma, A.; Kremer, L.C. Medical interventions for treating anthracycline-induced symptomatic and asymptomatic cardiotoxicity during and after treatment for childhood cancer. Cochrane Database Syst. Rev. 2016, 8, CD008011. [Google Scholar] [CrossRef] [Green Version]
- Armenian, S.H.; Hudson, M.M.; Mulder, R.L.; Chen, M.H.; Constine, L.S.; Dwyer, M.; Nathan, P.C.; Tissing, W.J.E.; Shankar, S.; Sieswerda, E.; et al. Recommendations for cardiomyopathy surveillance for survivors of childhood cancer: A report from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol. 2015, 16, e123–e136. [Google Scholar] [CrossRef] [Green Version]
- Singal, P.K.; Iliskovic, N. Doxorubicin-induced cardiomyopathy. N. Eng. J. Med. 1998, 339, 900–905. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muoz, D.; ESC Scientific Document Group. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar]
- Lipshultz, E.R.; Chow, E.J.; Doody, D.R.; Armenian, S.H.; Asselin, B.L.; Baker, K.S.; Bhatia, S.; Constine, L.S.; Freyer, D.R.; Kopp, L.M.; et al. Cardiometabolic Risk in Childhood Cancer Survivors: A Report from the Children’s Oncology Group. Cancer Epidemiol. Biomark. Prev. 2022, 31, 536–542. [Google Scholar] [CrossRef]
- Kostakou, P.M.; Kouris, N.T.; Kostopoulos, V.S.; Damaskos, D.S.; Olympios, C.D. Cardio-oncology: A new and developing sector of research and therapy in the field of cardiology. Heart Fail. Rev. 2018, 24, 91–100. [Google Scholar] [CrossRef]
- American Association for Cancer Research. AACR Cancer Progress Report 2021. Available online: https://cancerprogressreport.aacr.org/wp-content/uploads/sites/2/2021/10/AACR_CPR_2021.pdf (accessed on 19 December 2021).
- Available online: http://survivorshipguidelines.org (accessed on 23 December 2021).
- Armenian, S.H.; Lacchetti, C.; Barac, A.; Carver, J.; Constine, L.S.; Denduluri, N.; Dent, S.; Douglas, P.S.; Durand, J.-B.; Ewer, M.; et al. Prevention and Monitoring of Cardiac Dysfunction in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2017, 35, 893–911. [Google Scholar] [CrossRef]
- Tan, C.; Tasaka, H.; Yu, K.-P.; Murphy, M.L.; Karnofsky, D.A. Daunomycin, an antitumor antibiotic, in the treatment of neoplastic disease. Clinical evaluation with special reference to childhood leukemia. Cancer 1967, 20, 333–353. [Google Scholar] [CrossRef] [PubMed]
- Swain, S.M.; Whaley, F.S.; Ewer, M.S. Congestive heart failure in patients treated with Doxorubicin: A retrospective analysis of three trials. Cancer 2003, 97, 2869–2879. [Google Scholar] [CrossRef] [PubMed]
- Kadan-Lottick, N.S.; Robison, L.L.; Gurney, J.G.; Neglia, J.P.; Yasui, Y.; Hayashi, R.; Hudson, M.; Greenberg, M.; Mertens, A.C. Childhood cancer survivors’ knowledge about their pastdiagnosis and treatment: Childhood Cancer Survivor Study. JAMA 2002, 287, 1832–1839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipshultz, S.E.; Miller, T.L.; Lipsitz, S.R.; Nueberg, D.S.; Dahlberg, S.E.; Colan, S.D. Continuous versus bolus infusion of Doxorubicin in children with ALL: Longterm Cardiac Outcomes. Pediatrics 2012, 130, 1003–1011. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Liu, X.; Bawa-Khalfe, T.; Lu, L.-S.; Lyu, Y.L.; Liu, L.F.; Yeh, E.T.H. Identification of the molecular basis of doxorubicin-induced cardiotoxicity. Nat. Med. 2012, 18, 1639–1642. [Google Scholar] [CrossRef]
- Songbo, M.; Lang, H.; Xinyong, C.; Bin, X.; Ping, Z.; Liang, S. Oxidative stress injury in doxorubicin-induced cardiotoxicity. Toxicol. Lett. 2019, 307, 41–48. [Google Scholar] [CrossRef]
- Menna, P.; Salvatorelli, E. Primary Prevention Strategies for Anthracycline Cardiotoxicity: A Brief Overview. Chemotherapy 2017, 62, 159–168. [Google Scholar] [CrossRef]
- Eder, A.R.; Arriaga, E.A. Capillary Electrophoresis Monitors Enhancement in Subcellular Reactive Oxygen Species Production upon Treatment with Doxorubicin. Chem. Res. Toxicol. 2006, 19, 1151–1159. [Google Scholar] [CrossRef] [Green Version]
- Ichikawa, Y.; Ghanefar, M.; Bayeva, M.; Wu, R.; Khechaduri, A.; Prasad, S.V.N.; Mutharasan, R.K.; Naik, T.J.; Ardehali, H. Cardiotoxicity of Doxorubicin is mediated through mitochondrial iron accumulation. J. Clin. Investig. 2014, 124, 617–630. [Google Scholar] [CrossRef] [Green Version]
- Lipshultz, S.E.; Rifai, N.; Dalton, V.M.; Levy, D.E.; Silverman, L.B.; Lipsitz, S.R.; Colan, S.D.; Asselin, B.L.; Barr, R.D.; Clavell, L.A.; et al. The Effect of Dexrazoxane on Myocardial Injury in Doxorubicin-Treated Children with Acute Lymphoblastic Leukemia. N. Engl. J. Med. 2004, 351, 145–153. [Google Scholar] [CrossRef]
- Akam-Venkata, J.; Franco, V.I.; Lipshultz, S.E. Late cardiotoxicities: Issues for childhood cancer survivors. Curr. Treat Options Cardiovasc. Med. 2016, 18, 47. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhu, Y.; Dong, S.; Zhang, A.; Lu, Y.; Li, Y.; Lv, S.; Zhang, J. Role of oxidative stress in cardiotoxicity of antineoplastic drugs. Life Sci. 2019, 232, 116526. [Google Scholar] [CrossRef] [PubMed]
- Gunturk, E.E.; Yucel, B.; Gunturk, I.; Yazici, C.; Yay, A.; Kose, K. The effects of N-acetylcysteine on cisplatin induced cardiotoxicity. Bratisl. Med, J. 2019, 120, 423–428. [Google Scholar] [CrossRef]
- Iqubal, A.; Iqubal, M.K.; Sharma, S.; Ansari, M.A.; Najmi, A.K.; Ali, S.M.; Ali, J.; Haque, S.E. Molecular mechanism involved in cyclophosphamide-induced cardiotoxicity: Old drug with a new vision. Life Sci. 2018, 218, 112–131. [Google Scholar] [CrossRef]
- Fabin, N.; Bergami, M.; Cenko, E.; Bugiardini, R.; Manfrini, O. The Role of Vasospasm and Microcirculatory Dysfunction in Fluoropyrimidine-Induced Ischemic Heart Disease. J. Clin. Med. 2022, 11, 1244. [Google Scholar] [CrossRef]
- Bansal, N.; Blanco, J.G.; Sharma, U.C.; Pokharel, S.; Shisler, S.; Lipshultz, S.E. Cardiovascular diseases in survivors of childhood cancer. Cancer Metastasis Rev. 2020, 39, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.D.; Cehic, D.A.; Morgia, M.; Bergom, C.; Toohey, J.; Guerrero, P.A.; Ferencik, M.; Kikuchi, R.; Carver, J.R.; Zaha, V.G.; et al. Cardiovascular Manifestations from Therapeutic Radiation: A Multidisciplinary Expert Consensus Statement from the International Cardio-Oncology Society. JACC Cardio. Oncol. 2021, 3, 360–380. [Google Scholar]
- Chow, E.; Doody, D.R.; Wilkeies, J.J.; Becker, J.J.; Chennupatio, S. Adverse events among chronic myelogenous leukemia patients treated with tyrosine kinase inhibitors: A real-world analysis of health plan enrollees. Leuk Lymphoma 2021, 62, 1203–1210. [Google Scholar]
- Patel, R.P.; Parikh, R.; Gunturu, K.S.; Tariq, R.Z.; Dani, S.S.; Ganatra, S.; Nohria, A. Cardiotoxicity of Immune Checkpoint Inhibitors. Curr. Oncol. Rep. 2021, 23, 1–9. [Google Scholar] [CrossRef]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.V.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D.; et al. Myocarditis in Patients Treated with Immune Checkpoint Inhibitors. J. Am. Coll. Cardiol. 2018, 71, 1755–1764. [Google Scholar]
- Moslehi, J.; Minamishima, Y.A.; Shi, J.; Neuberg, D.; Charytan, D.; Padera, R.F.; Signoretti, S.; Liao, R.; Kaelin, W.G. Loss of Hypoxia-Inducible Factor Prolyl Hydroxylase Activity in Cardiomyocytes Phenocopies Ischemic Cardiomyopathy. Circulation 2010, 122, 1004–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebb, D.; Meyers, P.; Grier, H.; Bernstein, M.; Gorlick, R.; Lipschultz, S.E. Phase II trial of trastuzumab in combination with cytotoxic chemotherapy for treatment of metastatic osteosarcoma with human epidermal growth factor receptor 2 overexpression: A report from Children’s oncology group. J. Clin. Oncol. 2012, 30, 2545–2551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotz, S.J.; Ryan, T.D.; Hlavaty, J.; George, S.A.; El-Bietar, J.; Dandoy, C. Cardiotoxicity and cardiomyopathy in children and young adult survivors of hematopoietic stem cell transplant. Pediatr. Blood Cancer 2017, 64, e26600. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Adams, M.J.; Colan, S.D.; Constine, L.S.; Herman, E.H.; Hsu, D.T.; Hudson, M.M.; Kremer, L.C.; Landy, D.C.; Miller, T.L.; et al. Long-term Cardiovascular Toxicity in Children, Adolescents, and Young Adults Who Receive Cancer Therapy: Pathophysiology, Course, Monitoring, Management, Prevention, and Research Directions: A scientific statement from the American Heart Association. Circulation 2013, 128, 1927–1995. [Google Scholar] [CrossRef]
- June, C.H.; Sadelain, M. Faculty Opinions recommendation of Chimeric antigen receptor therapy. N. Engl. J. Med. 2020, 379, 64–73. [Google Scholar] [CrossRef]
- Shalabi, H.; Sachdev, V.; Kulshreshtha, A.; Cohen, J.W.; Yates, B.; Rosing, D.R.; Sidenko, S.; Delbrook, C.; Mackall, C.; Wiley, B.; et al. impact of cytokine release syndrome on cardiac function following CD19 CAR-T cell therapy in children and young adults with hematological malignancies. J. Immunother. Cancer 2020, 8, e001159. [Google Scholar] [CrossRef]
- Burstein, D.S.; Maude, S.; Grupp, S.; Griffis, H.; Rossano, J.; Lin, K. Cardiac profile of chimeric antigen receptor T cell therapy in children: A single institution experience. Biol. Blood Marrow. Transplant. 2018, 24, 1590–1595. [Google Scholar] [CrossRef] [Green Version]
- Herrmann, J. Adverse cardiac effects of cancer therapies: Cardiotoxicity and arrhythmia. Nat. Rev. Cardiol. 2020, 17, 474–502. [Google Scholar] [CrossRef]
- Crillo, M.; Venturini, M.; Ciccarelli, L.; Coati, F.; Bortolami, O.; Verlato, G. Clinician versus nurse symptom reporting using the National Cancer Institute-Common Terminology Criteria for Adverse Events during chemotherapy: Results of a comparison based on patient’s self-reported questionnaire. Ann. Oncol. 2009, 20, 1229–1235. [Google Scholar]
- Piccart-Gebhart, M.J.; Procter, M.; Leyland-Jones, B.; Goldhirsch, A.; Untch, M.; Smith, I.; Gianni, L.; Baselga, J.; Bell, R.H.; Jackisch, C.; et al. Trastuzumab after Adjuvant Chemotherapy in HER2-Positive Breast Cancer. N. Engl. J. Med. 2005, 353, 1659–1672. [Google Scholar] [CrossRef] [Green Version]
- Oeffinger, K.C.; Mertens, A.C.; Sklar, C.A.; Kawashima, T.; Hudson, M.M.; Meadows, A.T.; Friedman, D.L.; Marina, N.; Hobbie, W.; Kadan-Lottick, N.S.; et al. Chronic Health Conditions in Adult Survivors of Childhood Cancer. N. Engl. J. Med. 2006, 355, 1572–1582. [Google Scholar] [CrossRef] [PubMed]
- Ganame, J.; Claus, P.; Eyskens, B.; Uyttebroeck, A.; Renard, M.; D’Hooge, J.; Gewillig, M.; Bijnens, B.; Sutherland, G.R.; Mertens, L. Acute Cardiac Functional and Morphological Changes After Anthracycline Infusions in Children. Am. J. Cardiol. 2007, 99, 974–977. [Google Scholar] [CrossRef] [PubMed]
- Nicol, M.; Baudet, M.; Cohen-Solal, A. Subclinical Left Ventricular Dysfunction During Chemotherapy. Card. Fail. Rev. 2019, 5, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Lipsitz, S.R.; Sallan, S.E. Chronic progressive cardiac dysfunction years after doxorubicin therapy for childhood acute lymphoblastic leukemia. J. Clin. Oncol. 2005, 23, 2629–2636. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Colan, S.D.; Gelber, R.D.; Perez-Atayde, A.R.; Sallan, S.E.; Sanders, S.P. Late Cardiac Effects of Doxorubicin Therapy for Acute Lymphoblastic Leukemia in Childhood. N. Engl. J. Med. 1991, 324, 808–815. [Google Scholar] [CrossRef]
- Lipshultz, S.E.; Franco, V.I.; Miller, T. Cardiovascular disease in adult survivors of childhood cancer. Annu. Rev. Med. 2015, 66, 161–176. [Google Scholar] [CrossRef] [Green Version]
- Simbre, V.C.; Adams, M.J.; Deshpande, S.S.; Duffy, S.A.; Miller, T.L.; Lipshultz, S.E. Cardiomyopathy caused by antineoplastic therapies. Curr. Treat. Options Cardiovasc. Med. 2001, 3, 493–505. [Google Scholar] [CrossRef]
- Das, B.; Deshpande, S.; Akam-Venkata, J.; Shakti, D.; Moskowitz, W.; Lipshultz, S.E. Heart Failure with Preserved Ejection Fraction in Children. Pediatr. Cardiol. 2022, 1–17. [Google Scholar] [CrossRef]
- Mulrooney, D.A.; Armstrong, G.T.; Huang, S.; Ness, K.K.; Ehrhardt, M.J.; Joshi, V.M.; Plana, J.C.; Soliman, E.Z.; Green, D.M.; Srivastava, D. Cardiac Outcomes in Adult Survivors of Childhood Cancer Exposed to Cardiotoxic Therapy: A Cross-sectional Study. Ann. Intern. Med. 2016, 164, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Fabiani, I.; Panichella, G.; Aimo, A.; Grigoratos, C.; Vergaro, G.; Pugliese, N.R.; Taddei, S.; Cardinale, D.M.; Passino, C.; Emdin, M.; et al. Subclinical cardiac damage in cancer patients before chemotherapy. Heart Fail. Rev. 2021, 27, 1091–1104. [Google Scholar] [CrossRef]
- Lyon, A.R.; Dent, S.; Stanway, S.; Earl, H.; Brezden-Masley, C.; Cohen-Solal, A.; Tocchetti, C.G.; Moslehi, J.J.; Groarke, J.D.; Bergler-Klein, J.; et al. Baseline cardiovascular risk assessment in cancer patients scheduled to receive cardiotoxic cancer therapies: A position statement and new risk assessment tools from the Cardio-Oncology Study Group of the Heart Failure Association of the European Society of Cardiology in collaboration with the International Cardio-Oncology Society. Eur. J. Heart Fail. 2020, 22, 1945–1960. [Google Scholar] [PubMed]
- Pudil, R.; Mueller, C.; Čelutkienė, J.; Henriksen, P.A.; Lenihan, D.; Dent, S.; Barac, A.; Stanway, S.; Moslehi, J.; Suter, T.M.; et al. Role of serum biomarkers in cancer patients receiving cardiotoxic cancer therapies: A position statement from the Cardio-Oncology Study Group of the Heart Failure Association and the Cardio-Oncology Council of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1966–1983. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Sandri, M.T.; Colombo, A.; Colombo, N.; Boeri, M.; Lamantia, G.; Civelli, M.; Peccatori, F.; Martinelli, G.; Fiorentini, C.; et al. Prognostic Value of Troponin I in Cardiac Risk Stratification of Cancer Patients Undergoing High-Dose Chemotherapy. Circulation 2004, 109, 2749–2754. [Google Scholar] [CrossRef] [Green Version]
- Lipshuntz, S.E.; Landy, D.C.; Lopez-Mitnik, G.; Lipsitz, S.R.; Hinkle, A.S.; Constine, L.S. Cardiovascular status of childhood cancer survivors exposed and unexposed to cardiotoxic therapy. J. Clin. Oncol. 2012, 30, 1050–1057. [Google Scholar] [CrossRef]
- Eliaz, I. The Role of Galectin-3 as a Marker of Cancer and Inflammation in a Stage IV Ovarian Cancer Patient with Underlying Pro-Inflammatory Comorbidities. Case Rep. Oncol. 2013, 6, 343–349. [Google Scholar] [CrossRef]
- Sawaya, H.; Sebag, I.A.; Plana, J.C.; Januzzi, J.L.; Ky, B.; Tan, T.C.; Cohen, V.; Banchs, J.; Carver, J.R.; Wiegers, S.E.; et al. Assessment of Echocardiography and Biomarkers for the Extended Prediction of Cardiotoxicity in Patients Treated with Anthracyclines, Taxanes, and Trastuzumab. Circ. Cardiovasc. Imaging 2012, 5, 596–603. [Google Scholar] [CrossRef] [Green Version]
- Tian, C.; Yang, Y.; Bai, B.; Wang, S.; Liu, M.; Sun, R.-C.; Yu, T.; Chu, X.-M. Potential of exosomes as diagnostic biomarkers and therapeutic carriers for doxorubicin-induced cardiotoxicity. Int. J. Biol. Sci. 2021, 17, 1328–1338. [Google Scholar] [CrossRef]
- Oikawa, M.; Yaegashi, D.; Yokokawa, T.; Misaka, T.; Sato, T.; Kaneshiro, T.; Kobayashi, A.; Yoshihisa, A.; Nakazato, K.; Ishida, T.; et al. D-Dimer Is a Predictive Factor of Cancer Therapeutics-Related Cardiac Dysfunction in Patients Treated with Cardiotoxic Chemotherapy. Front. Cardiovasc. Med. 2022, 8, 807754. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J. Am. Coll. Cardiol. 2017, 70, 776–803. [Google Scholar]
- Cardinale, D.; Colombo, A.; Bacchiani, G.; Tedeschi, I.; Meroni, C.A.; Veglia, F.; Civelli, M.; Lamantia, G.; Colombo, N.; Curigliano, G.; et al. Early Detection of Anthracycline Cardiotoxicity and Improvement with Heart Failure Therapy. Circulation 2015, 131, 1981–1988. [Google Scholar] [CrossRef] [Green Version]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M. Expert consensus for multi-modality imaging evaluation of adult patients during and after cancer therapy: A report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2014, 27, 911–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curigliano, G.; Lenihan, D.; Fradley, M.; Ganatra, S.; Barac, A.; Blaes, A.; Herrmann, J.; Porter, C.; Lyon, A.R.; Lancellotti, P.; et al. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations. Ann. Oncol. 2020, 31, 171–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheitlin, M.D.; Armstrong, W.F.; Aurigemma, G.P.; Beller, G.A.; Bierman, F.Z.; Davis, J.L.; Douglas, P.S.; Faxon, D.P.; Gillam, L.D.; Kimball, T.R.; et al. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: Summary article: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASE Committee to Update the 1997 Guidelines for the Clinical Application of Echocardiography). Circulation 2003, 108, 1146–1162. [Google Scholar] [PubMed] [Green Version]
- Čelutkienė, J.; Pudil, R.; López-Fernández, T.; Grapsa, J.; Nihoyannopoulos, P.; Bergler-Klein, J.; Cohen-Solal, A.; Farmakis, D.; Tocchetti, C.G.; von Haehling, S.; et al. Role of cardiovascular imaging in cancer patients receiving cardiotoxic therapies: A position statement on behalf of the Heart Failure Association (HFA), the European Association of Cardiovascular Imaging (EACVI) and the Cardio-Oncology Council of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2020, 22, 1504–1524. [Google Scholar]
- Čelutkienė, J.; Plymen, C.M.; Flachskampf, F.A.; De Boer, R.A.; Grapsa, J.; Manka, R.; Anderson, L.; Garbi, M.; Barberis, V.; Filardi, P.P.; et al. Innovative imaging methods in heart failure: A shifting paradigm in cardiac assessment. Position statement on behalf of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2018, 20, 1615–1633. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.W.; Finkelman, B.S.; Gulati, G.; Narayan, H.K.; Upshaw, J.; Narayan, V. Abnormalities in 3-dimensional left ventricular mechanics with anthracycline chemotherapy are associated with systolic and diastolic dysfunction. JACC Cardiovasc. Imaging 2018, 11, 1059–1068. [Google Scholar] [CrossRef]
- Beitner, N.; Jenner, J.; Sörensson, P. Comparison of Left Ventricular Volumes Measured by 3DE, SPECT and CMR. J. Cardiovasc. Imaging 2019, 27, 200–211. [Google Scholar] [CrossRef]
- Thavendiranathan, P.; Grant, A.D.; Negishi, T.; Plana, J.C.; Popovi, Z.B.; Marwick, T.H. Reproducibility of echocardiographic techniques for sequential assessment of left ventricular ejection fraction and volumes: Application to patients undergoing cancer chemotherapy. J. Am. Coll. Cardiol. 2013, 61, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Thavendiranathan, P.; Poulin, F.; Lim, K.D.; Plana, J.C.; Woo, A.; Marwick, T.H. Use of myocardial strain imaging by echocardiography for the early detection of cardiotoxicity in patients during and after cancer chemotherapy: A systematic review. J. Am. Coll Cardiol. 2014, 63, 2751–2768. [Google Scholar] [CrossRef] [Green Version]
- Plana, J.C.; Thavendiranathan, P.; Bucciarelli-Ducci, C.; Lancellotti, P. Multi-Modality Imaging in the Assessment of Cardiovascular Toxicity in the Cancer Patient. JACC: Cardiovasc. Imaging 2018, 11, 1173–1186. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, M.T.; Yucel, E.; Bouras, S.; Wang, L.; Fei, H.-W.; Halpern, E.F.; Scherrer-Crosbie, M. Myocardial Strain Is Associated with Adverse Clinical Cardiac Events in Patients Treated with Anthracyclines. J. Am. Soc. Echocardiogr. 2016, 29, 522–527.e3. [Google Scholar] [CrossRef] [PubMed]
- Amedro, P.; Vincenti, M.; Abassi, H.; Lanot, N.; De La Villeon, G.; Guillaumont, S.; Gamon, L.; Mura, T.; Lopez-Perrin, K.; Haouy, S.; et al. Use of speckle tracking echocardiography to detect late anthracycline-induced cardiotoxicity in childhood cancer: A prospective controlled cross-sectional study. Int. J. Cardiol. 2022, 354, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Akam-Venkata, J.; Kadiu, G.; Galas, J.; Lipshultz, S.E.; Aggarwal, S. Left ventricle segmental function in childhood cancer survivors using speckle-tracking echocardiography. Cardiol. Young 2019, 29, 1494–1500. [Google Scholar] [CrossRef] [PubMed]
- Thavendiranathan, P.; Negishi, T.; Somerset, E.; Negishi, K.; Penicka, M.; Lemieux, J.; Aakhus, S.; Miyazaki, S.; Shirazi, M.; Galderisi, M.; et al. Strain-Guided Management of Potentially Cardiotoxic Cancer Therapy. J. Am. Coll. Cardiol. 2020, 77, 392–401. [Google Scholar] [CrossRef]
- Keramida, K.; Farmakis, D. Right ventricular involvement in cancer therapy–related cardiotoxicity: The emerging role of strain echocardiography. Heart Fail. Rev. 2020, 26, 1189–1193. [Google Scholar] [CrossRef]
- Moslehi, J.J.; Witteles, R.M. Global Longitudinal Strain in Cardio-Oncology. J. Am. Coll. Cardiol. 2021, 77, 402–404. [Google Scholar] [CrossRef]
- Stoodley, P.W.; Richards, D.A.; Meikle, S.R.; Clarke, J.; Hui, R.; Thomas, L. The potential role of echocardiographic strain imaging for evaluating cardiotoxicity due to cancer therapy. Heart Lung Circ. 2011, 20, 3–9. [Google Scholar] [CrossRef]
- Rajapreyar, P. Tissue Doppler Imaging and Focal, Late-Onset Anthracycline-Induced Cardiovascular Disease in Long Term Survivors of Childhood Cancer: A Research Article. J. Clin. Diagn. Res. 2016, 10, SC01–SC04. [Google Scholar] [CrossRef]
- Dorup, I.; Levitt, G.; Sullivan, I.; Sorensen, K. Prospective longitudinal assessment of late anthracycline cardiotoxicity after childhood cancer: The role of diastolic function. Heart 2004, 90, 1214–1216. [Google Scholar] [CrossRef] [Green Version]
- Wolf, C.M.; Reiner, B.; Kühn, A.; Hager, A.; Müller, J.; Meierhofer, C.; Oberhoffer, R.; Ewert, P.; Schmid, I.; Weil, J. Subclinical Cardiac Dysfunction in Childhood Cancer Survivors on 10-Years Follow-Up Correlates with Cumulative Anthracycline Dose and Is Best Detected by Cardiopulmonary Exercise Testing, Circulating Serum Biomarker, Speckle Tracking Echocardiography, and Tissue Doppler Imaging. Front. Pediatr. 2020, 8, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novo, G.; Santoro, C.; Manno, G.; Di Lisi, D.; Esposito, R.; Mandoli, G.E.; Evola, V.; Pastore, M.C.; Sperlongano, S.; D’Andrea, A.; et al. Usefulness of stress echocardiography in the management of patients treated with anticancer drugs. J. Am. Soc. Echocardiogr. 2021, 34, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Klewer, S.E.; Goldberg, S.J.; Donnerstein, R.L.; Berg, R.A.; Hutter, J.J. Dobutamine stress echocardiography: A sensitive indicator of diminished myocardial function in asymptomatic doxorubicin-treated long-term survivors of childhood cancer. Am. Coll. Cardiol. 1992, 19, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, A.; Tunaoglu, F.S.; Pinarli, F.G.; Ilhan, M.; Oğuz, A.; Karadeniz, C.; Olguntürk, R.; Oğuz, D.; Kula, S. Early diagnosis of anthracycline toxicity in asymptomatic long-term survivors: Dobutamine stress echocardiography and tissue Doppler velocities in normal and abnormal myocardial wall motion. Eur. Heart J. Cardiovasc. Imaging 2010, 11, 814–822. [Google Scholar] [CrossRef] [Green Version]
- Jordan, J.H.; Todd, R.M.; Vasu, S.; Hundley, W.G. Cardiovascular Magnetic Resonance in the Oncology Patient. JACC: Cardiovasc. Imaging 2018, 11, 1150–1172. [Google Scholar] [CrossRef] [PubMed]
- Meyersohn, N.M.; Pursnani, A.; Neilan, T.G. Detection of Cardiac Toxicity Due to Cancer Treatment: Role of Cardiac MRI. Curr. Treat. Options Cardiovasc. Med. 2015, 17, 1–9. [Google Scholar] [CrossRef]
- Jordan, J.H.; Sukpraphrute, B.; Meléndez, G.C. Early myocardial strain changes during potentially cardiotoxic chemotherapy may occur as a result of reductions in left ventricular end-diastolic volume: The need to interpret left ventricular strain with volumes. Circulation 2017, 135, 2575–2577. [Google Scholar] [CrossRef]
- Neilan, T.G.; Coelho-Filho, O.R.; Pena-Herrera, D.; Shah, R.V.; Jerosch-Herold, M.; Francis, S.A.; Moslehi, J.; Kwong, R.Y. Left Ventricular Mass in Patients with a Cardiomyopathy After Treatment with Anthracyclines. Am. J. Cardiol. 2012, 110, 1679–1686. [Google Scholar] [CrossRef] [Green Version]
- De Ville de Goyet, M.; Brichard, B.; Robert, A.; Renard, L.; Veyckemans, F. Prospective cardiac MRI for the analysis of biventricular function in children undergoing cancer treatments. Pediatr. Blood Cancer. 2015, 62, 867–874. [Google Scholar] [CrossRef]
- Evin, M.; Cluzel, P.; Lamy, J.; Rosenbaum, D.; Kusmia, S.; Defrance, C.; Soulat, G.; Mousseaux, E.; Roux, C.; Clement, K.; et al. Assessment of left atrial function by MRI myocardial feature tracking. J. Magn. Reson. Imaging 2015, 42, 379–389. [Google Scholar] [CrossRef]
- Iliescu, C.A.; Grines, C.L.; Herrmann, J.; Yang, E.H.; Cilingiroglu, M.; Charitakis, K.; Hakeem, A.; Toutouzas, K.P.; Leesar, M.A.; Marmagkiolis, K. SCAI Expert consensus statement: Evaluation, management, and special considerations of cardio-oncology patients in the cardiac catheterization laboratory (endorsed by the cardiological society of India, and sociedad Latino Americana de Cardiologıa intervencionista). Catheter. Cardiovasc. Interv. 2016, 87, E202–E223. [Google Scholar] [PubMed]
- Lopez-Mattei, J.C.; Yang, E.H.; Ferencik, M.; Baldassarre, L.A.; Dent, S.; Budoff, M.J. Cardiac Computed Tomography in Cardio-Oncology: JACC: CardioOncology Primer. JACC Cardio Oncol. 2021, 3, 635–649. [Google Scholar] [CrossRef] [PubMed]
- McKillop, J.H.; Bristow MRGoris MLBillingham, M.E.; Bockemuehl, K. Sensitivity and specificity of radionuclide ejection fractions in doxorubicin cardiotoxicity. Am. Heart J. 1983, 106, 1048–1056. [Google Scholar] [CrossRef]
- Kelly, J.M.; Babich, J.W. PET Tracers for Imaging Cardiac Function in Cardio-oncology. Curr. Cardiol. Rep. 2022, 24, 247–260. [Google Scholar] [CrossRef] [PubMed]
- Bravo, P.E.; Bengel, F. The Role of Cardiac PET in Translating Basic Science into the Clinical Arena. J. Cardiovasc. Transl. Res. 2011, 4, 425–436. [Google Scholar] [CrossRef]
- Rischpler, C.; Nekolla, S.G.; Dregely, I.; Schwaiger, M. Hybrid PET/MR Imaging of the Heart: Potential, Initial Experiences, and Future Prospects. J. Nucl. Med. 2013, 54, 402–415. [Google Scholar] [CrossRef] [Green Version]
- Jones, L.W.; Liu, Q.; Armstrong, G.T.; Ness, K.K.; Yasui, Y.; Devine, K.; Tonorezos, E.; Soares-Miranda, L.; Sklar, C.A.; Douglas, P.S.; et al. Exercise and Risk of Major Cardiovascular Events in Adult Survivors of Childhood Hodgkin Lymphoma: A Report from the Childhood Cancer Survivor Study. J. Clin. Oncol. 2014, 32, 3643–3650. [Google Scholar] [CrossRef]
- Mishra, S.I.; Scherer, R.W.; Geigle, P.M.; Berlanstein, D.; Topaloglu, O.; Gotay, C.C.; Snyder, C. Exercise interventions on health-related quality of life for cancer survivors. Cochrane Database Syst. Rev. 2012, CF007566. [Google Scholar] [CrossRef]
- Lipshultz, S.E.; Scully, R.E.; Lipstitz, S.R.; Sallan, S.E.; Silverman, L.B.; Miller, T.L. Assessment of Dexrazoxane as a cardioprotectant in doxorubicin-treated children with high-risk acute lymphoblastic leukemia: Long-term follow-up of a prospective, randomized, multicentral trial. Lancet Oncol. 2010, 11, 950–961. [Google Scholar] [CrossRef] [Green Version]
- Hahn, V.S.; Lenihan, D.J.; Ky, B. Cancer Therapy–Induced Cardiotoxicity: Basic Mechanisms and Potential Cardioprotective Therapies. J. Am. Heart Assoc. 2014, 3, e000665. [Google Scholar] [CrossRef] [Green Version]
- Varghese, S.S.; Eekhoudt, C.R.; Jassal, D.S. Mechanisms of anthracycline-mediated cardiotoxicity and preventative strategies in women with breast cancer. Mol. Cell. Biochem. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lipshuntz, S.E. Dexrazoxane for protection against cardiotoxic effects of anthracyclines in children. J. Clin. Oncol. 1996, 14, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Lipsitz, S.R.; Sallan, S.E.; Ii, V.C.S.; Shaikh, S.L.; Mone, S.M.; Gelber, R.D.; Colan, S.D. Long-Term Enalapril Therapy or Left Ventricular Dysfunction in Doxorubicin-Treated Survivors of Childhood Cancer. J. Clin. Oncol. 2002, 20, 4517–4522. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Singh, S.K.; Agrawal, V.; Singh, T.B. Role of ACE inhibitors in anthracycline-induced cardiotoxicity: A randomized, double-blind, placebo-controlled trial. Pediatr. Blood Cancer 2018, 65, e27308. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Colombo, A.; Lamantia, G.; Colombo, N.; Civelli, M.; De Giacomi, G.; Rubino, M.; Veglia, F.; Fiorentini, C.; Cipolla, C.M. Early Anthracycline- induced cardiomyopathy: Clinical relevance and response to pharmacologic therapy. J. Am. Coll. Cardiol. 2010, 55, 213–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silber, J.H.; Cnaan, A.; Clark, B.J.; Paridon, S.M.; Chin, A.J.; Rychik, J.; Hogarty, A.N.; Cohen, M.I.; Barber, G.; Rutkowski, M.; et al. Enalapril to Prevent Cardiac Function Decline in Long-Term Survivors of Pediatric Cancer Exposed to Anthracyclines. J. Clin. Oncol. 2004, 22, 820–828. [Google Scholar] [CrossRef]
- Garg, R.; Yusuf, S.; Bussmann, W.D.; Sleight, P.; Uprichard, A.; Massie, B.; McGrath, B.; Nilsson, B.; Pitt, B.; Magnani, B.; et al. Overview of Randomized Trials of Angiotensin-Converting Enzyme Inhibitors on Mortality and Morbidity in Patients with Heart Failure. JAMA 1995, 273, 1450–1456. [Google Scholar] [CrossRef]
- Armenian, S.H.; Hudson, M.M.; Chen, M.H.; Colan, S.D.; Lindenfeld, L.; Mills, G.; Siyahian, A.; Gelehrter, S.; Dang, H.; Hein, W.; et al. Rationale and design of the Children’s Oncology Group (COG) study ALTE1621: A randomized, placebo-controlled trial to determine if low-dose Carvedilol can prevent anthracycline-related left ventricular remodeling in childhood cancer survivors at high risk for developing heart failure. BMC Cardiovasc. Disord. 2016, 16, 187. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.M.; Lopez-Mitnik, G.; Somarriba, G.; Lipsitz, S.R.; Hinkle, A.S.; Constine, L.S. Exercise capacity in long-term survivors in long-term survivors of pediatric cancer: An analysis from cardiac risk factors in childhood cancer survivors study. Pediatr. Blood Cancer 2013, 60, 663–668. [Google Scholar] [CrossRef]
- Acar, Z.; Kale, A.; Turgut, M.; Demircan, S.; Durna, K.; Demir, S.; Meriç, M.; Ağaç, M.T. Efficiency of Atorvastatin in the Protection of Anthracycline-Induced Cardiomyopathy. J. Am. Coll. Cardiol. 2011, 58, 988–989. [Google Scholar] [CrossRef] [Green Version]
- Kirk, R.; Dipchand, A.I.; Rosenthal, D.N.; Addonizio, L.; Burch, M.; Chrisant, M.; Dubin, A.; Everitt, M.; Gajarski, R.; Mertens, L. The International Society for Heart and Lung Trans-plantation Guidelines for the management of pediatric heart failure: Executive summary. J. Heart Lung Transplant. 2014, 33, 888–909. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Greiner, M.A.; Colan, S.D. Letter to Editor about “Doxoorubicin-induced cardiomyopathy”. N. Eng. J. Med. 1999, 340, 653–655. [Google Scholar]
- Das, B.; Moskowitz, W.; Butler, J. Current and Future Drug and Device Therapies for Pediatric Heart Failure Patients: Potential Lessons from Adult Trials. Children 2021, 8, 322. [Google Scholar] [CrossRef] [PubMed]
- Frey, M.K.; Arfsten, H.; Pavo, N.; Han, E.; Kastl, S.; Hülsmann, M.; Gyöngyösi, M.; Bergler-Klein, J. Sacubitril/valsartan is well tolerated in patients with long-standing heart failure and history of cancer and improves ventricular function: Real-world data. Cardio-Oncol. 2021, 7, 1–6. [Google Scholar] [CrossRef]
- Gregorietti, V.; Fernandez, T.L.; Costa, D.; Chahla, E.O.; Daniele, A.J. Use of Sacubitril/valsartan in patients with cardiotoxicity and heart failure due to chemotherapy. Cardio-Oncology 2020, 6, 1–6. [Google Scholar] [CrossRef]
- Gongora, C.A.; Drobni, Z.D.; Silva, T.Q.A.C.; Zafar, A.; Gong, J.; Zlotoff, D.A.; Gilman, H.K.; Hartmann, S.E.; Sama, S.; Nikolaidou, S.; et al. Sodium-Glucose Co-Transporter-2 Inhibitors and Cardiac Outcomes Among Patients Treated with Anthracyclines. JACC: Heart Fail. 2022, 10, 559–567. [Google Scholar] [CrossRef]
- Mehra, M.R.; Canter, C.E.; Hannan, M.M.; Semigran, M.J.; Uber, P.A.; Baran, D.A.; Danziger-Isakov, L.; Kirklin, J.K.; Kirk, R.; Kushwaha, S.S.; et al. The 2016 International Society for Heart Lung Transplantation listing criteria for heart transplantation: A 10-year update. J. Heart Lung Transplant. 2016, 35, 1–23. [Google Scholar] [CrossRef]
- Puri, K.; Denfield, S.W.; Adachi, I.; Dreyer, W.J.; Price, J.F.; Spinner, J.A.; Choudhry, S.; Brackett, J.; Santucci, G.; Rainusso, N.C.; et al. Ventricular assist device support for children with chemotherapy-induced cardiomyopathy and advanced heart failure: Perspectives gained from a single-center experience. Pediatr. Transplant. 2022, 26, e14286. [Google Scholar] [CrossRef]
- Schlam, I.; Lee, A.Y.; Li, S.; Sheikh, F.H.; Zaghlol, R.; Basyal, B.; Gallagher, C.; Molina, E.; Mahr, C.; Cheng, R.K.; et al. Left Ventricular Assist Devices in Patients with Active Malignancies. JACC Cardio Oncol. 2021, 3, 305–315. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Kim, Y.; Restrepo-Cordoba, M.A.; Lunde, I.G.; Wakimoto, H.; Smith, A.M.; Toepfer, C.N.; Getz, K.; Gorham, J.; Patel, P.; et al. Genetic Variants Associated with Cancer Therapy–Induced Cardiomyopathy. Circulation 2019, 140, 31–41. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hegazy, M.; Ghaleb, S.; Das, B.B. Diagnosis and Management of Cancer Treatment-Related Cardiac Dysfunction and Heart Failure in Children. Children 2023, 10, 149. https://doi.org/10.3390/children10010149
Hegazy M, Ghaleb S, Das BB. Diagnosis and Management of Cancer Treatment-Related Cardiac Dysfunction and Heart Failure in Children. Children. 2023; 10(1):149. https://doi.org/10.3390/children10010149
Chicago/Turabian StyleHegazy, Mohamed, Stephanie Ghaleb, and Bibhuti B Das. 2023. "Diagnosis and Management of Cancer Treatment-Related Cardiac Dysfunction and Heart Failure in Children" Children 10, no. 1: 149. https://doi.org/10.3390/children10010149