
Imaging Changes and Immune-Checkpoint Expression on T Cells in Bronchoalveolar Lavage Fluid from Patients with Pulmonary Sarcoidosis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
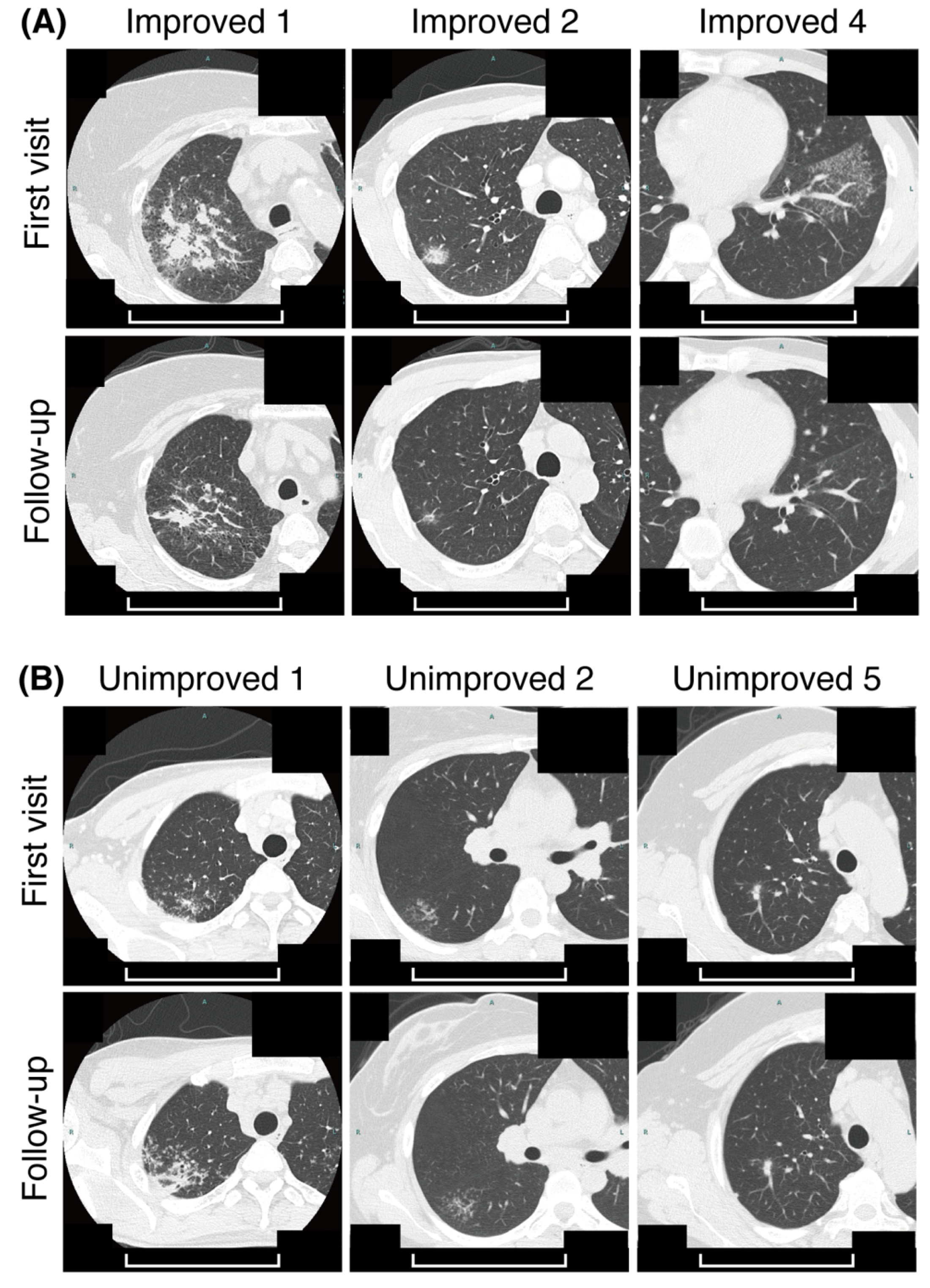
2.2. Criteria for CT Imaging Changes
2.3. Flow Cytometry
2.4. Immunofluorescence
2.5. ELISA
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. PD-1 Expression on CD4+ T Cells Was Higher in the Improved Group
3.3. TIM-3 Expression on CD4+ or CD8+ T Cells Was Higher in the Improved Group
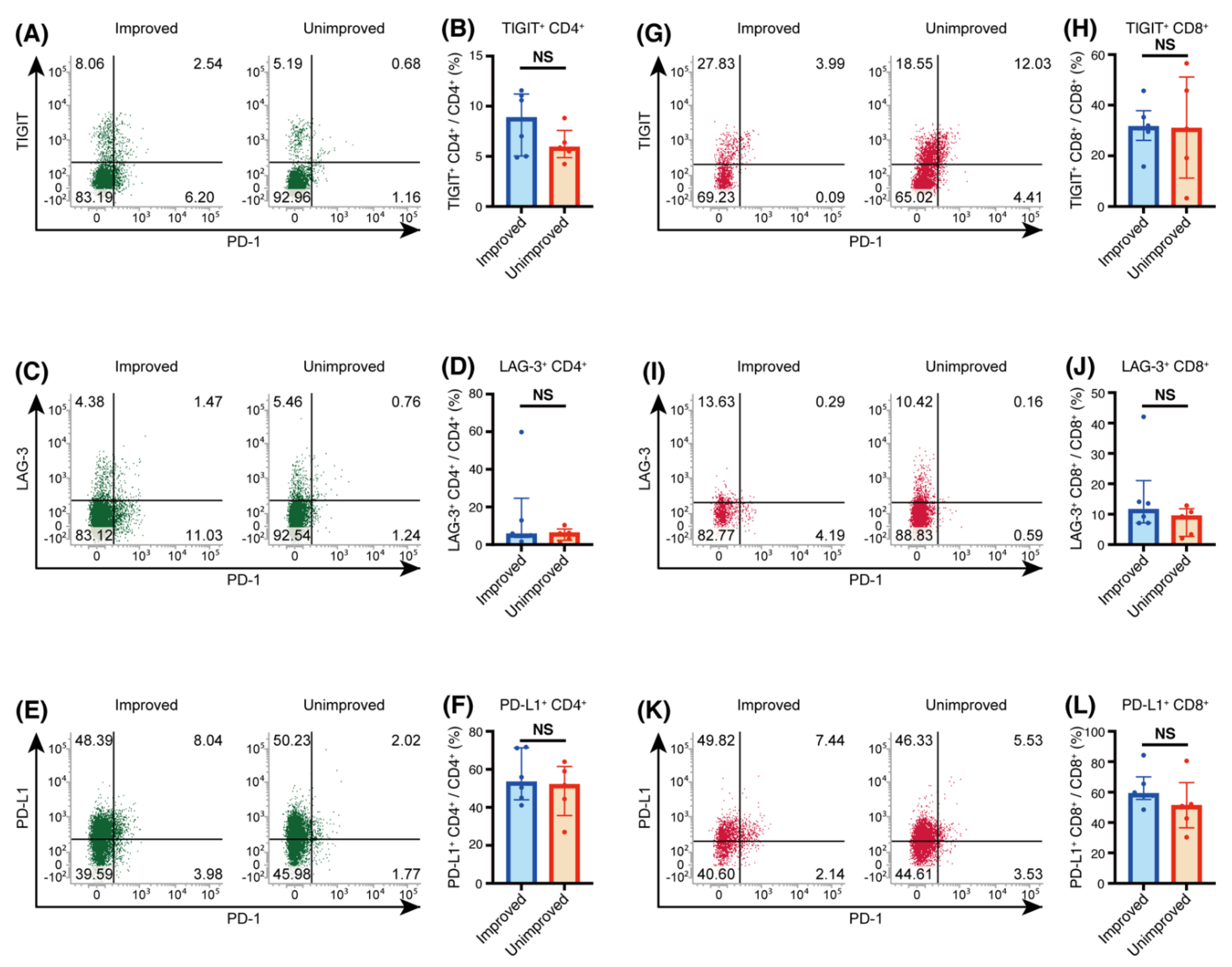
3.4. TIGIT, LAG-3 and PD-L1 Expression on T Cells from Sarcoidosis Patients
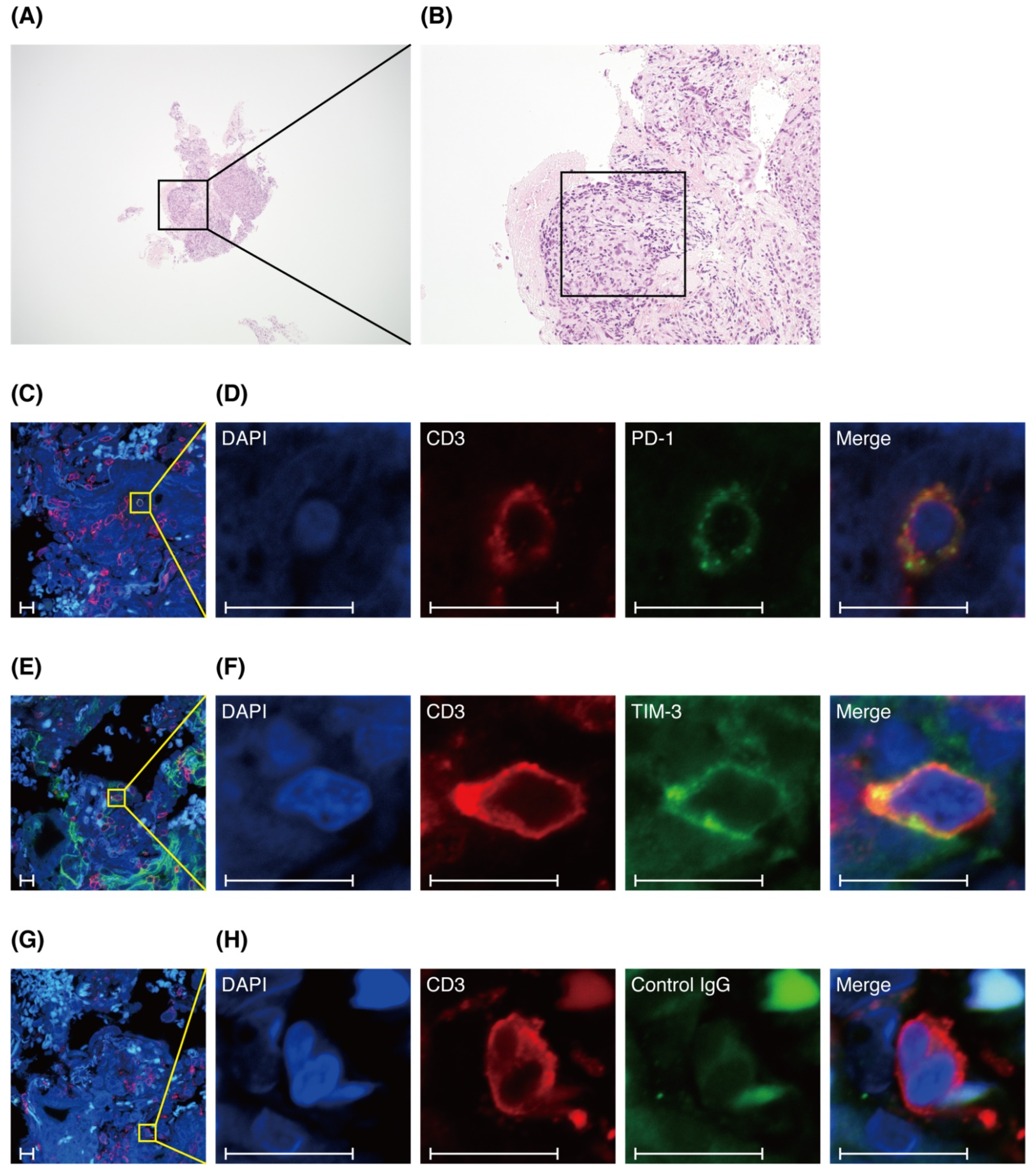
3.5. T Cells in Lung Specimens of Patients with Sarcoidosis Express PD-1 or TIM-3
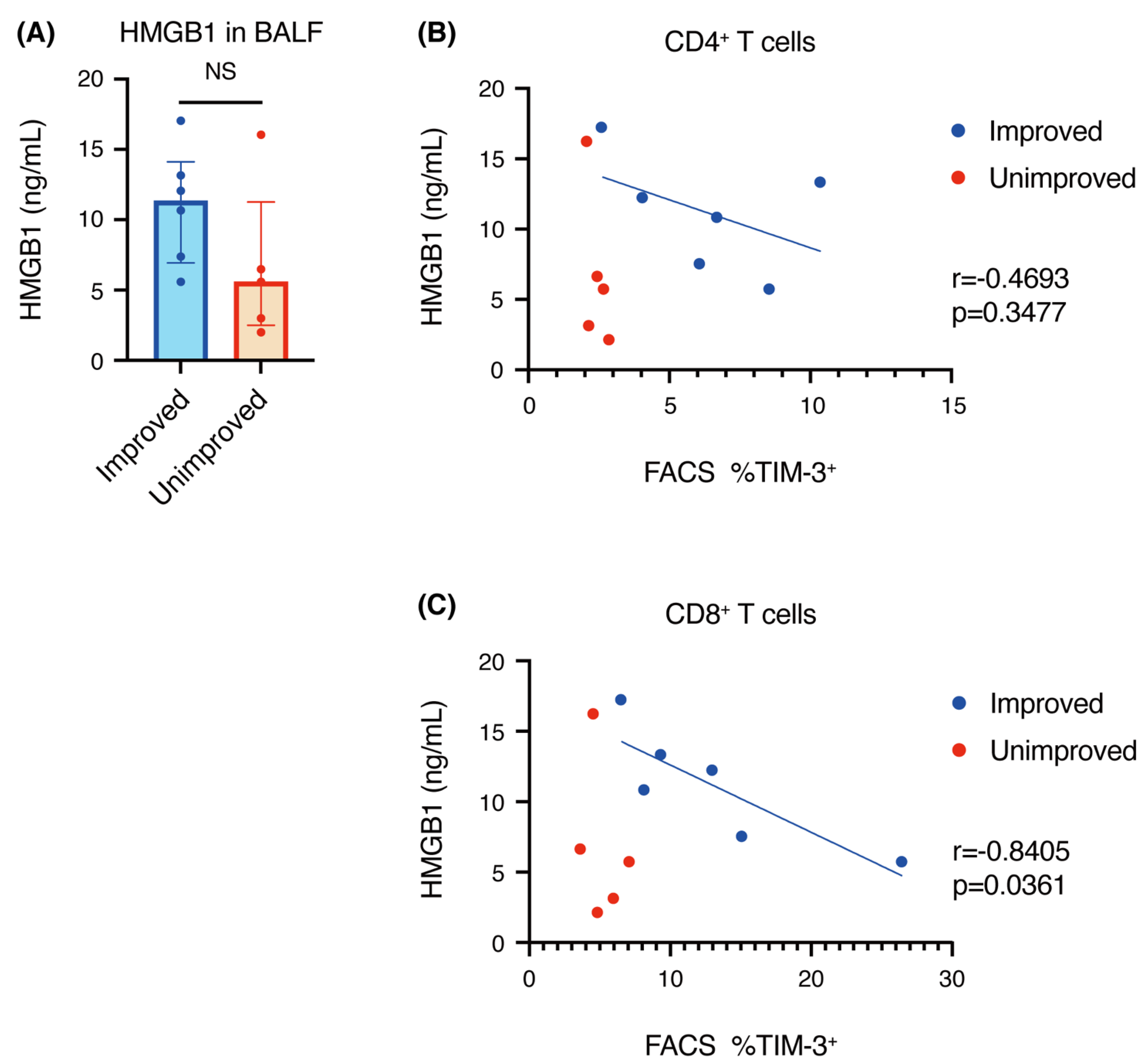
3.6. Correlation of HMGB1 Concentration with TIM-3+ T Cells
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grunewald, J.; Grutters, J.C.; Arkema, E.V.; Saketkoo, L.A.; Moller, D.R.; Müller-Quernheim, J. Sarcoidosis. Nat. Rev. Dis. Primers 2019, 5, 1–22. [Google Scholar] [CrossRef]
- Valeyre, D.; Prasse, A.; Nunes, H.; Uzunhan, Y.; Brillet, P.Y.; Müller-Quernheim, J. Sarcoidosis. Lancet 2014, 383, 1155–1167. [Google Scholar] [CrossRef]
- Oswald-Richter, K.A.; Richmond, B.W.; Braun, N.A.; Isom, J.; Abraham, S.; Taylor, T.R.; Drake, J.M.; Culver, D.A.; Wilkes, D.S.; Drake, W.P. Reversal of global CD4+ subset dysfunction is associated with spontaneous clinical resolution of pulmonary sarcoidosis. J. Immunol. 2013, 190, 5446–5453. [Google Scholar] [CrossRef] [Green Version]
- Qin, S.; Xu, L.; Yi, M.; Yu, S.; Wu, K.; Luo, S. Novel immune checkpoint targets: Moving beyond PD-1 and CTLA-4. Mol. Cancer 2019, 18, 155. [Google Scholar] [CrossRef] [PubMed]
- Ribas, A.; Wolchok, J.D. Cancer immunotherapy using checkpoint blockade. Science 2018, 359, 1350–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, A.C.; Joller, N.; Kuchroo, V.K. Lag-3, Tim-3, and TIGIT: Co-inhibitory receptors with specialized functions in immune regulation. Immunity 2016, 44, 989–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamada, N.; Maeyama, T.; Kawaguchi, T.; Yoshimi, M.; Fukumoto, J.; Yamada, M.; Yamada, S.; Kuwano, K.; Nakanishi, Y. The role of high mobility group box1 in pulmonary fibrosis. Am. J. Respir. Cell Mol. Biol. 2008, 39, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Suchankova, M.; Durmanova, V.; Tibenska, E.; Tedlova, E.; Majer, I.; Novosadova, H.; Demian, J.; Tedla, M.; Bucova, M. High mobility group box 1 protein in bronchoalveolar lavage fluid and correlation with other inflammatory markers in pulmonary diseases. Sarcoidosis Vasc. Diffuse Lung Dis. 2018, 35, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Hunninghake, G.W.; Costabel, U.; Ando, M.; Baughman, R.; Cordier, J.F.; du Bois, R.; Eklund, A.; Kitaichi, M.; Lynch, J.; Rizzato, G.; et al. Statement on sarcoidosis. Am. J. Respir. Crit. Care Med. 1999, 160, 736–755. [Google Scholar] [CrossRef]
- Scadding, J.G. Prognosis of intrathoracic sarcoidosis in England: A review of 136 cases after five years’ observation. Br. Med. J. 1961, 2, 1165–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, K.; Yanagihara, T.; Matsumoto, K.; Kusaba, H.; Yamauchi, T.; Ikematsu, Y.; Tanaka, K.; Otsubo, K.; Inoue, H.; Yoneshima, Y.; et al. Immune-checkpoint profiles for T cells in bronchoalveolar lavage fluid of patients with immune-checkpoint inhibitor-related interstitial lung disease. Int. Immunol. 2020, 32, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Braun, N.A.; Celada, L.J.; Herazo-Maya, J.D.; Abraham, S.; Shaginurova, G.; Sevin, C.M.; Grutters, J.; Culver, D.A.; Dworski, R.; Sheller, J.; et al. Blockade of the programmed death-1 pathway restores sarcoidosis CD4+ T-cell proliferative capacity. Am. J. Respir. Crit. Care Med. 2014, 190, 560–571. [Google Scholar] [CrossRef] [Green Version]
- Idali, F.; Wahlström, J.; Dahlberg, B.; Khademi, M.; Olsson, T.; Eklund, A.; Grunewald, J. Altered expression of T cell immunoglobulin-mucin (TIM) molecules in bronchoalveolar lavage CD4+ T cells in sarcoidosis. Respir. Res. 2009, 10, 42. [Google Scholar] [CrossRef] [Green Version]
- Wherry, E.J. T cell exhaustion. Nat. Immunol. 2011, 12, 492–499. [Google Scholar] [CrossRef]
- Cousin, S.; Toulmonde, M.; Kind, M.; Cazeau, A.L.; Bechade, D.; Coindre, J.M.; Italiano, A. Pulmonary sarcoidosis induced by the anti-PD1 monoclonal antibody pembrolizumab. Ann. Oncol. 2016, 27, 1178–1179. [Google Scholar] [CrossRef]
- Lomax, A.J.; McGuire, H.M.; McNeil, C.; Choi, C.J.; Hersey, P.; Karikios, D.; Shannon, K.; van Hal, S.; Carr, U.; Crotty, A.; et al. Immunotherapy-induced sarcoidosis in patients with melanoma treated with PD-1 checkpoint inhibitors: Case series and immunophenotypic analysis. Int. J. Rheum. Dis. 2017, 20, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Cotliar, J.; Querfeld, C.; Boswell, W.J.; Raja, N.; Raz, D.; Chen, R. Pembrolizumab-associated sarcoidosis. JAAD Case Rep. 2016, 2, 290–293. [Google Scholar] [CrossRef] [Green Version]
- Danlos, F.X.; Pagès, C.; Baroudjian, B.; Vercellino, L.; Battistella, M.; Mimoun, M.; Jebali, M.; Bagot, M.; Tazi, A.; Lebbè, C. Nivolumab-induced sarcoid-like granulomatous reaction in a patient with advanced melanoma. Chest 2016, 149, e133–e136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montaudié, H.; Pradelli, J.; Passeron, T.; Lacour, J.P.; Leroy, S. Pulmonary sarcoid-like granulomatosis induced by nivolumab. Br. J. Dermatol. 2017, 176, 1060–1063. [Google Scholar] [CrossRef]
- Gkiozos, I.; Kopitopoulou, A.; Kalkanis, A.; Vamvakaris, I.N.; Judson, M.A.; Syrigos, K.N. Sarcoidosis-like reactions induced by checkpoint inhibitors. J. Thorac. Oncol. 2018, 13, 1076–1082. [Google Scholar] [CrossRef] [Green Version]
- Kita, S.; Tsuda, T.; Sugisaki, K.; Miyazaki, E.; Matsumoto, T. Characterization of distribution of T lymphocyte subsets and activated T lymphocytes infiltrating into sarcoid lesions. Int. Med. 1995, 34, 847–855. [Google Scholar] [CrossRef] [Green Version]
- Kang, R.; Chen, R.; Zhang, Q.; Hou, W.; Wu, S.; Cao, L.; Huang, J.; Yu, Y.; Fan, X.G.; Yan, Z.; et al. HMGB1 in health and disease. Mol. Asp. Med. 2014, 40, 1–116. [Google Scholar] [CrossRef] [Green Version]
- Chiba, S.; Baghdadi, M.; Akiba, H.; Yoshiyama, H.; Kinoshita, I.; Dosaka-Akita, H.; Fujioka, Y.; Ohba, Y.; Gorman, J.V.; Colgan, J.D.; et al. Tumor-infiltrating DCs suppress nucleic acid-mediated innate immune responses through interactions between the receptor TIM-3 and the alarmin HMGB1. Nat. Immunol. 2012, 13, 832–842. [Google Scholar] [CrossRef] [PubMed]
- Dolina, J.S.; Braciale, T.J.; Hahn, Y.S. Liver-primed CD8+ T cells suppress antiviral adaptive immunity through galectin-9-independent T-cell immunoglobulin and mucin 3 engagement of high-mobility group box 1 in mice. Hepatology 2014, 59, 1351–1365. [Google Scholar] [CrossRef]
- Sundberg, E.; Fasth, A.E.; Palmblad, K.; Harris, H.E.; Andersson, U. High mobility group box chromosomal protein 1 acts as a proliferation signal for activated T lymphocytes. Immunobiology 2009, 214, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Scaffidi, P.; Misteli, T.; Bianchi, M.E. Release of chromatin protein HMGB1 by necrotic cells triggers inflammation. Nature 2002, 418, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Bell, C.W.; Pisetsky, D.S. The relationship between apoptosis and high-mobility group protein 1 release from murine macrophages stimulated with lipopolysaccharide or polyinosinic-polycytidylic acid. J. Immunol. 2007, 178, 6495–6503. [Google Scholar] [CrossRef] [Green Version]
- Andersson, U.; Harris, H.E. The role of HMGB1 in the pathogenesis of rheumatic disease. Biochim. Biophys. Acta 2010, 1799, 141–148. [Google Scholar] [CrossRef]
- Tang, R.; Rangachari, M.; Kuchroo, V.K. Tim-3: A co-receptor with diverse roles in T cell exhaustion and tolerance. Semin. Immunol. 2019, 42, 101302. [Google Scholar] [CrossRef]
- Morimoto, T.; Azuma, A.; Abe, S.; Usuki, J.; Kudoh, S.; Sugisaki, K.; Oritsu, M.; Nukiwa, T. Epidemiology of sarcoidosis in Japan. Eur. Respir. J. 2008, 31, 372–379. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis | Sex | Scadding Stage | Extrapulmonary Disease | Systemic Steroid | Macrophages (%) | Neutrophils (%) | Lymphocytes (%) | Eosinophils (%) | CD4/CD8 Ratio | |
|---|---|---|---|---|---|---|---|---|---|---|
| improved 1 | Histological | F | 2 | Skin, Muscle | No | 75.1 | 3.6 | 20.2 | 1.1 | 4.5 |
| improved 2 | Histological | M | 2 | No | No | 82.4 | 1 | 16.2 | 0.4 | 19.5 |
| improved 3 | Histological | F | 1 | Heart, Muscle | No | 49.3 | 0.2 | 50.1 | 0.4 | 9.6 |
| improved 4 | Histological | M | 2 | Eyes | No | 80.3 | 0.3 | 19.3 | 0.1 | 4.8 |
| improved 5 | Histological | F | 0 | Eyes, Skin | No | 52.7 | 0.3 | 46.9 | 0.1 | 7.3 |
| improved 6 | Clinical | F | 1 | Eyes, Heart, Spleen | No | 43.7 | 0.7 | 55.3 | 0.3 | 5 |
| unimproved 1 | Histological | F | 2 | Eyes, Nervous system | No | 55.4 | 0.9 | 43.3 | 0.4 | 11.9 |
| unimproved 2 | Histological | F | 2 | Eyes | No | 90.7 | 0.2 | 9.1 | 0 | 9.7 |
| unimproved 3 | Histological | F | 1 | Eyes, Parotid gland | No | 56.9 | 0.4 | 41.7 | 1.9 | 4.8 |
| unimproved 4 | Histological | F | 2 | Eyes, Skin, Muscle | No | 41.8 | 2.8 | 54.1 | 1.3 | 1.6 |
| unimproved 5 | Histological | F | 1 | Skin, Lymph nodes | No | 51.1 | 0.1 | 48.5 | 0.2 | 1.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotetsu, Y.; Yanagihara, T.; Suzuki, K.; Ando, H.; Eto, D.; Hata, K.; Arimura-Omori, M.; Yamamoto, Y.; Harada, E.; Hamada, N. Imaging Changes and Immune-Checkpoint Expression on T Cells in Bronchoalveolar Lavage Fluid from Patients with Pulmonary Sarcoidosis. Biomedicines 2021, 9, 1231. https://doi.org/10.3390/biomedicines9091231
Kotetsu Y, Yanagihara T, Suzuki K, Ando H, Eto D, Hata K, Arimura-Omori M, Yamamoto Y, Harada E, Hamada N. Imaging Changes and Immune-Checkpoint Expression on T Cells in Bronchoalveolar Lavage Fluid from Patients with Pulmonary Sarcoidosis. Biomedicines. 2021; 9(9):1231. https://doi.org/10.3390/biomedicines9091231
Chicago/Turabian StyleKotetsu, Yasuaki, Toyoshi Yanagihara, Kunihiro Suzuki, Hiroyuki Ando, Daisuke Eto, Kentaro Hata, Masako Arimura-Omori, Yuzo Yamamoto, Eiji Harada, and Naoki Hamada. 2021. "Imaging Changes and Immune-Checkpoint Expression on T Cells in Bronchoalveolar Lavage Fluid from Patients with Pulmonary Sarcoidosis" Biomedicines 9, no. 9: 1231. https://doi.org/10.3390/biomedicines9091231