
Post-COVID-19 Patients Who Develop Lung Fibrotic-like Changes Have Lower Circulating Levels of IFN-β but Higher Levels of IL-1α and TGF-β

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Samples
2.2. Cytokine and Chemokine Measurements
2.3. C reactive Protein (CRP) and Complement Complex C5b-9 Measurements
2.4. LDH Levels
2.5. Chest CT Scans
2.6. Statistical Analysis
3. Results
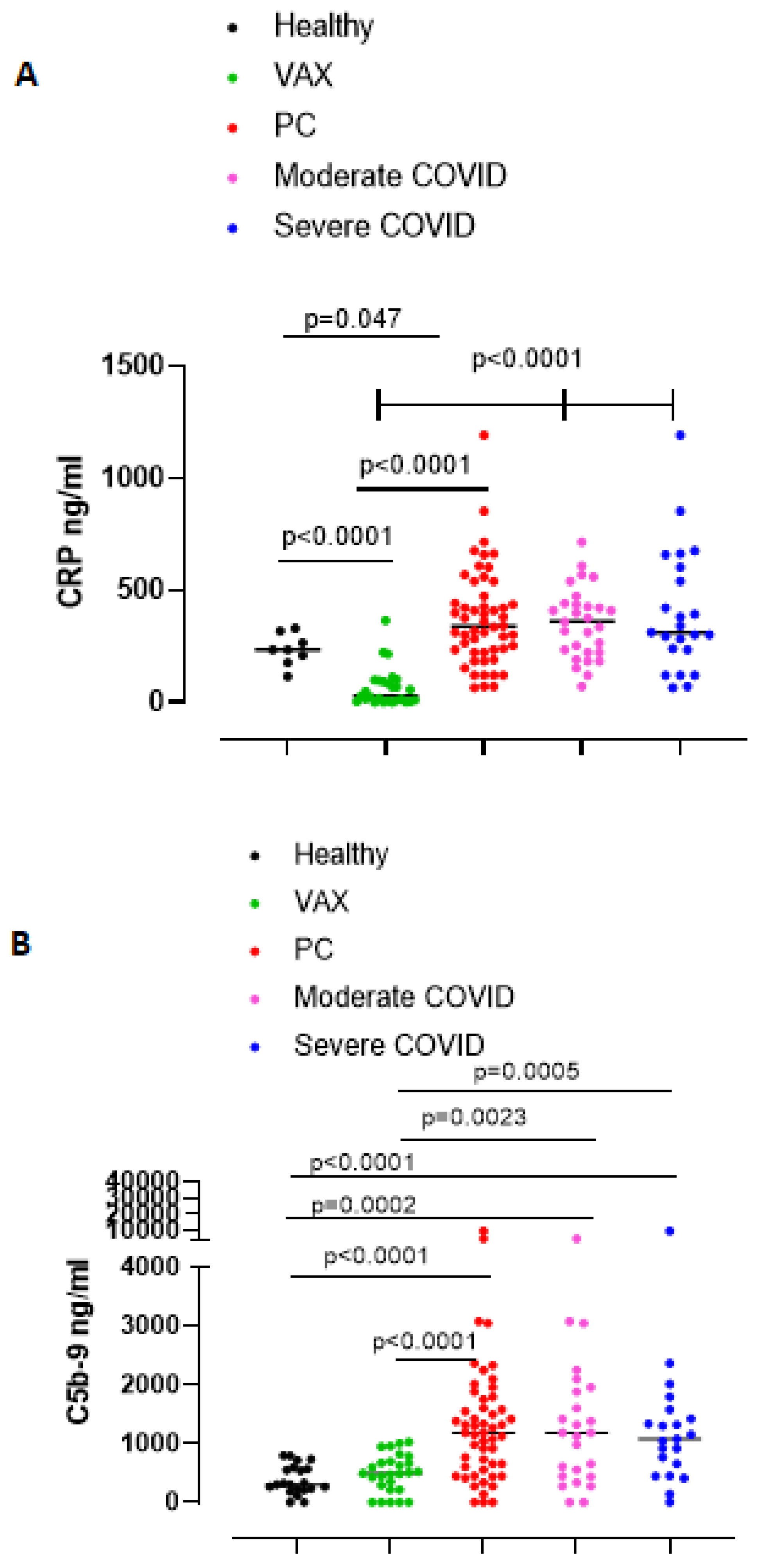
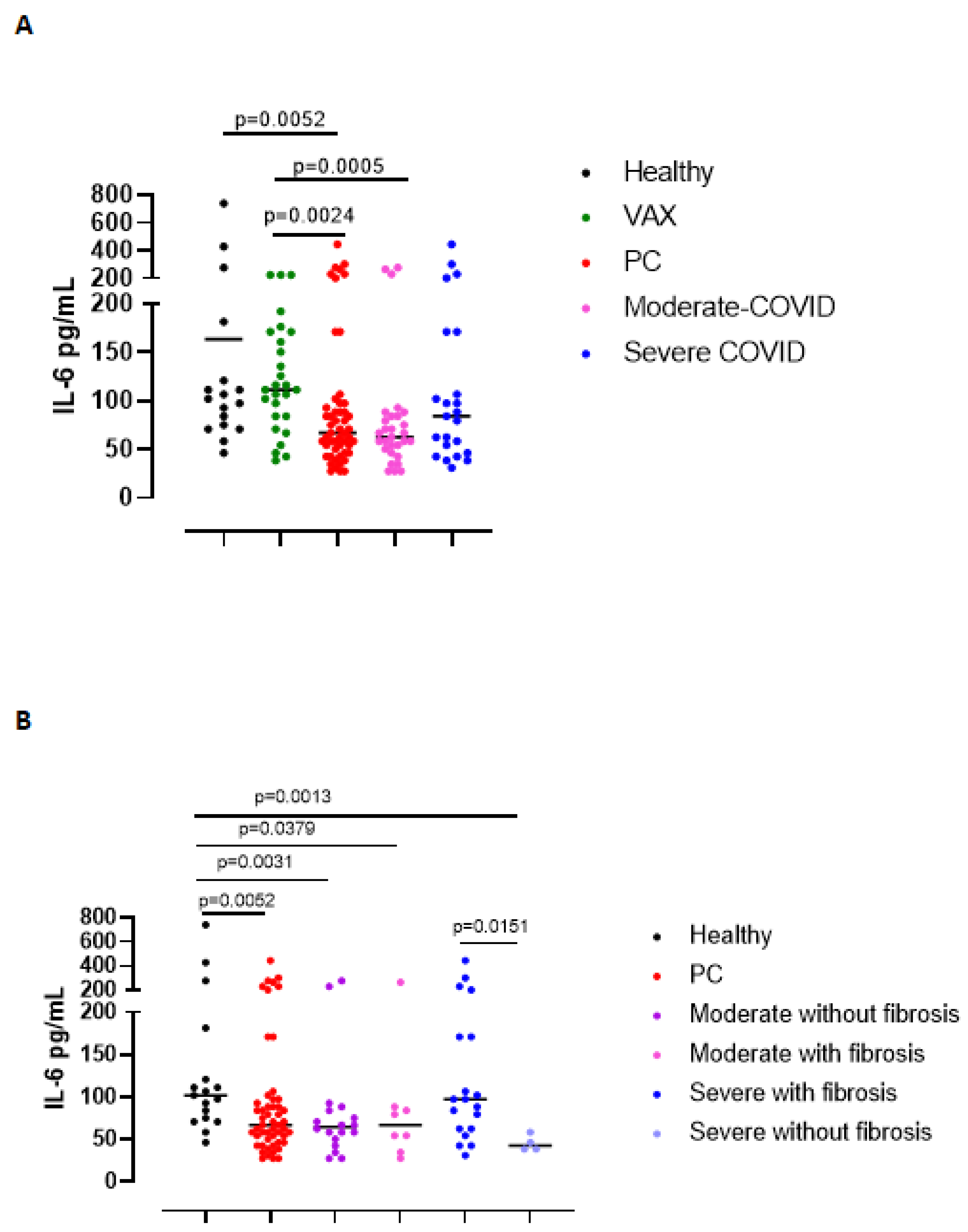
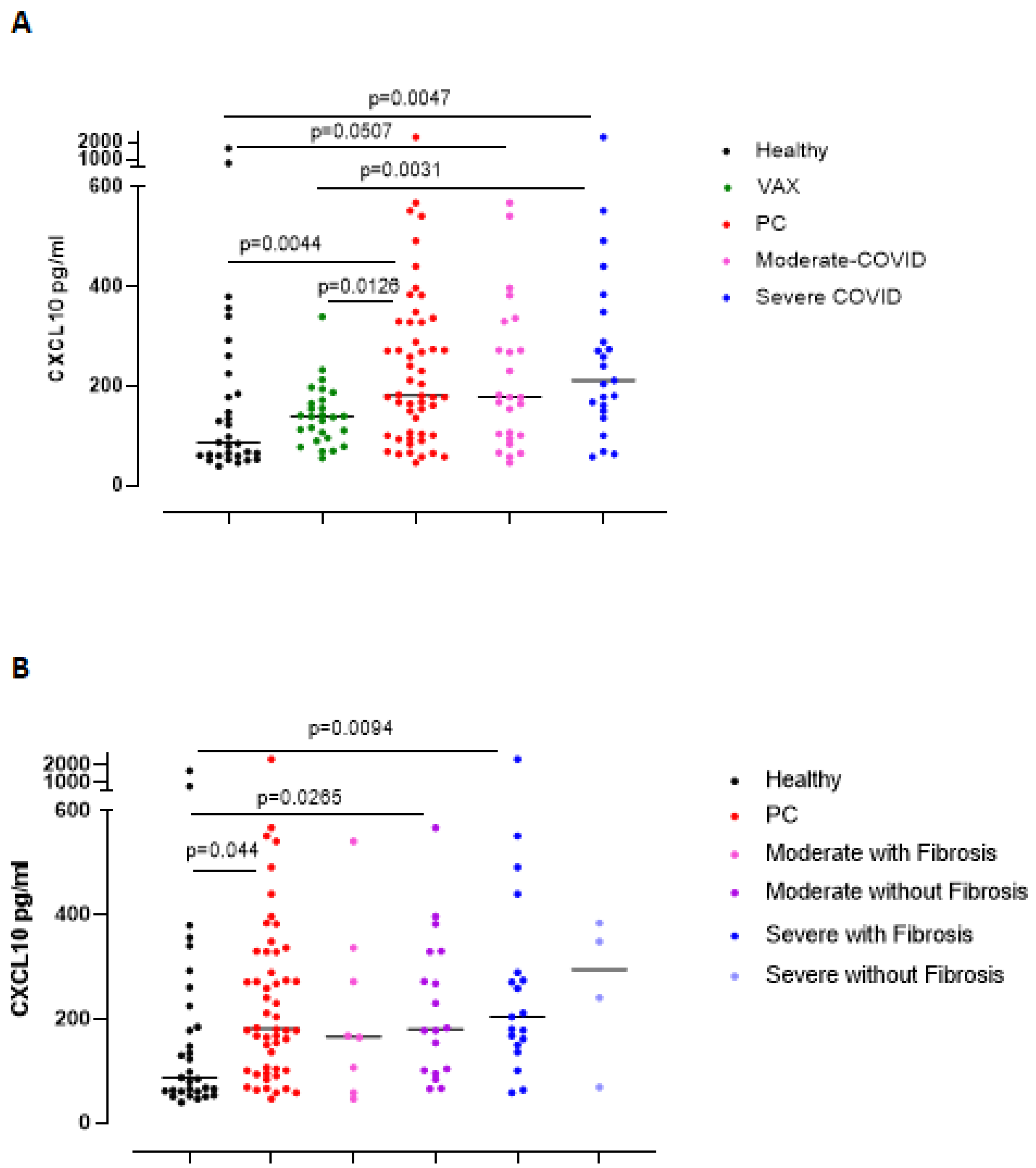
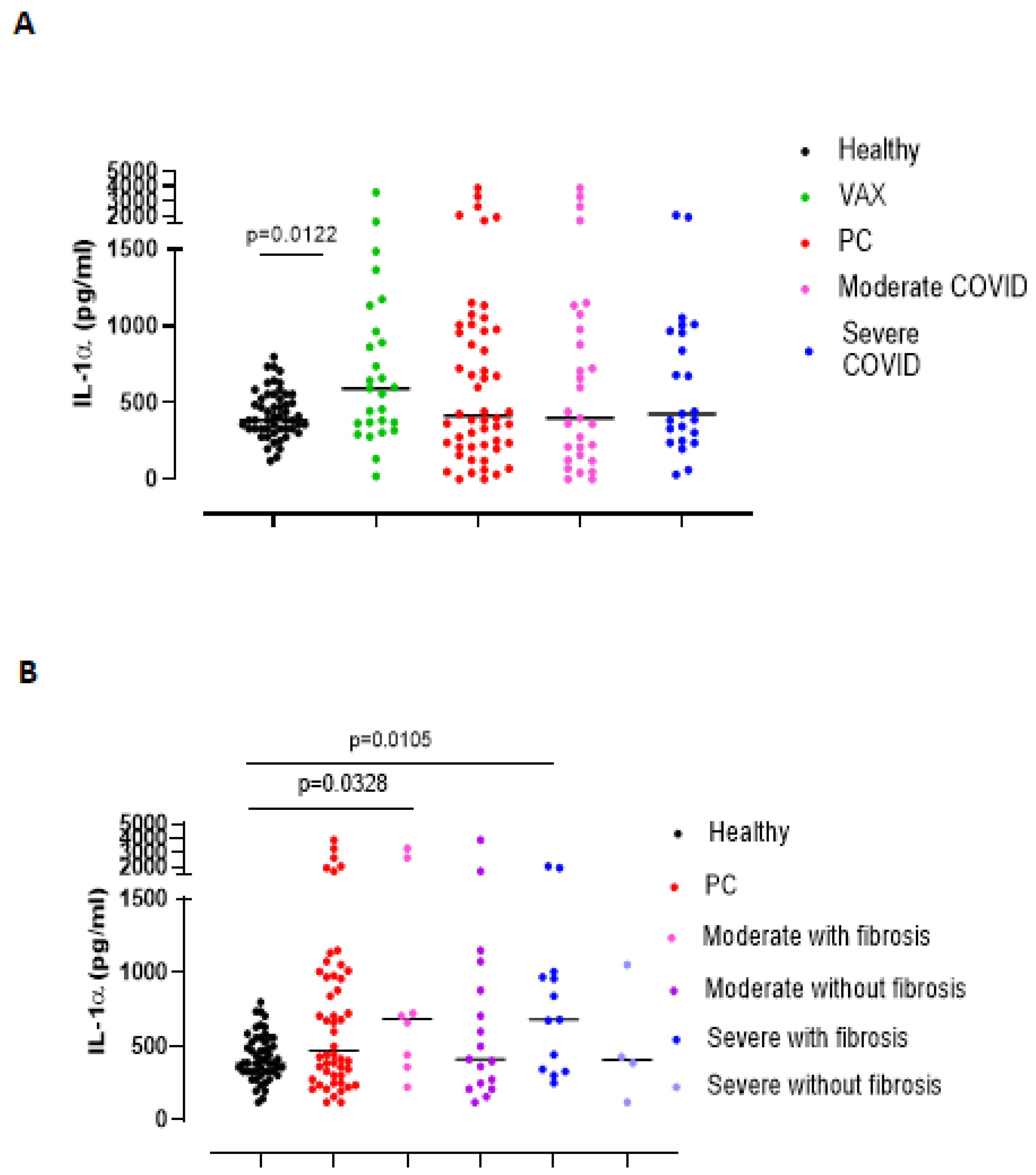
3.1. Circulating Levels of Inflammatory Markers Are Still Present in Post-COVID-19 Patients
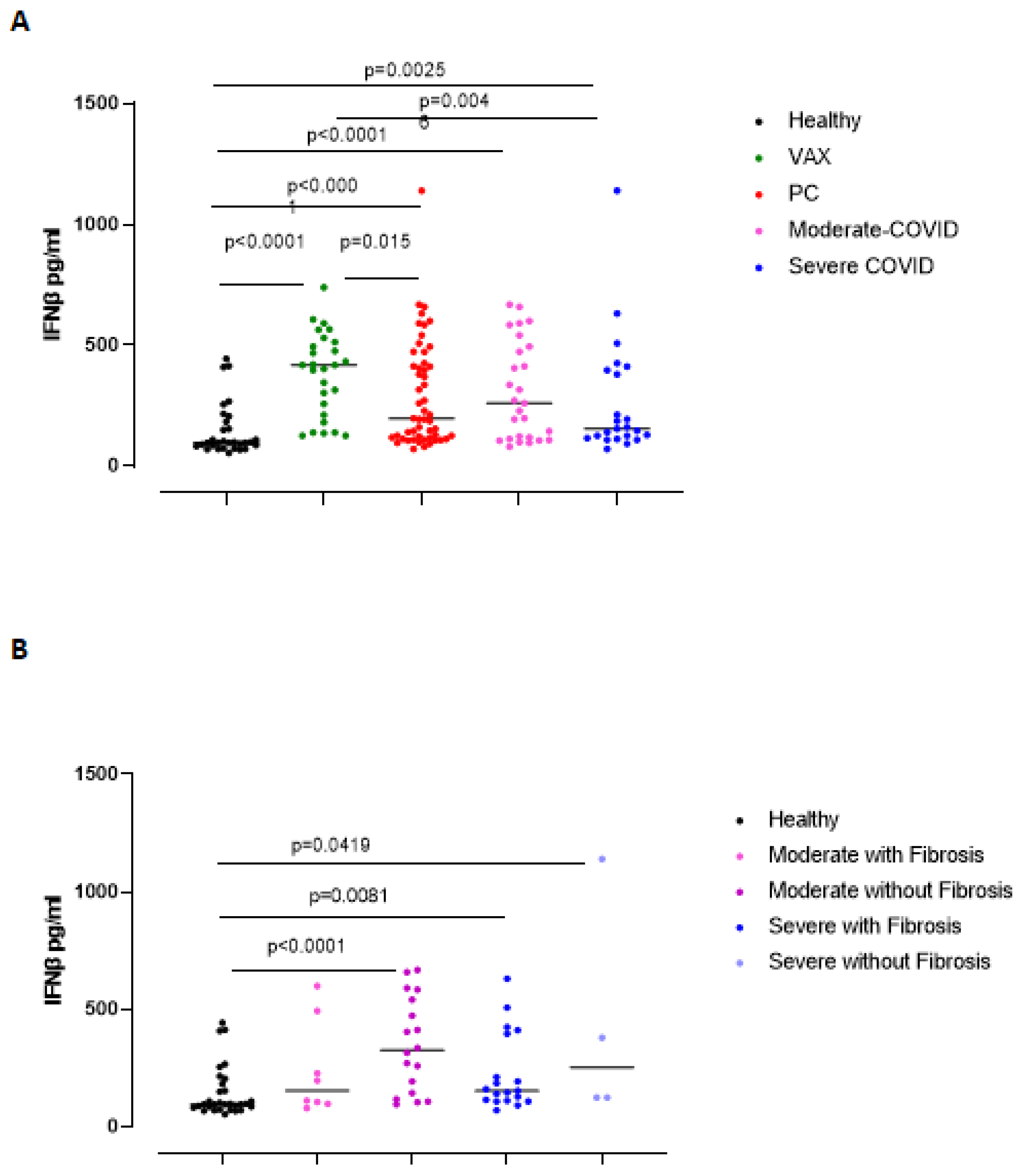
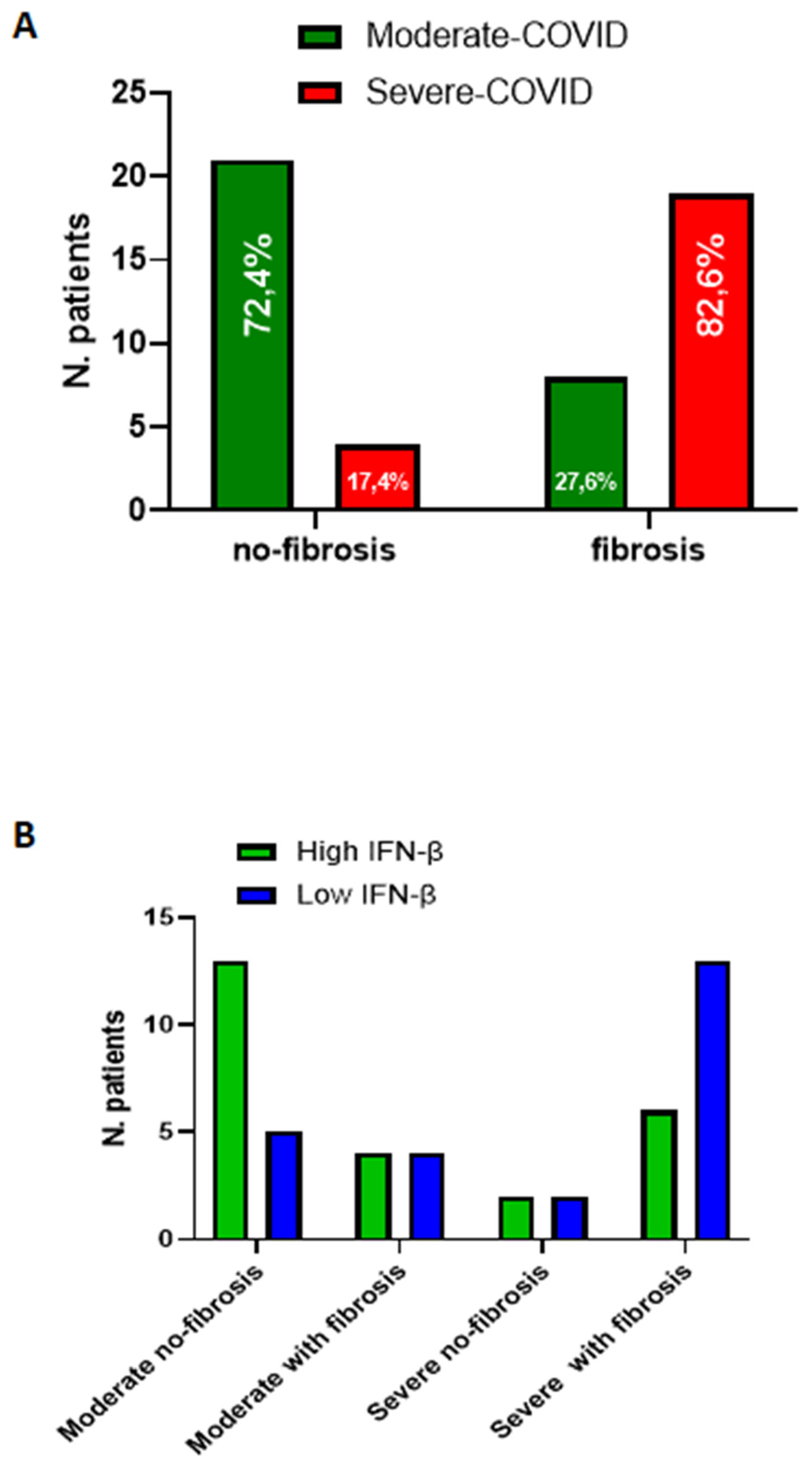
3.2. Circulating Levels of IFN-β Are Still High in Post-COVID-19 Patients Who Did Not Have Lung Fibrosis-like Changes Post Infection
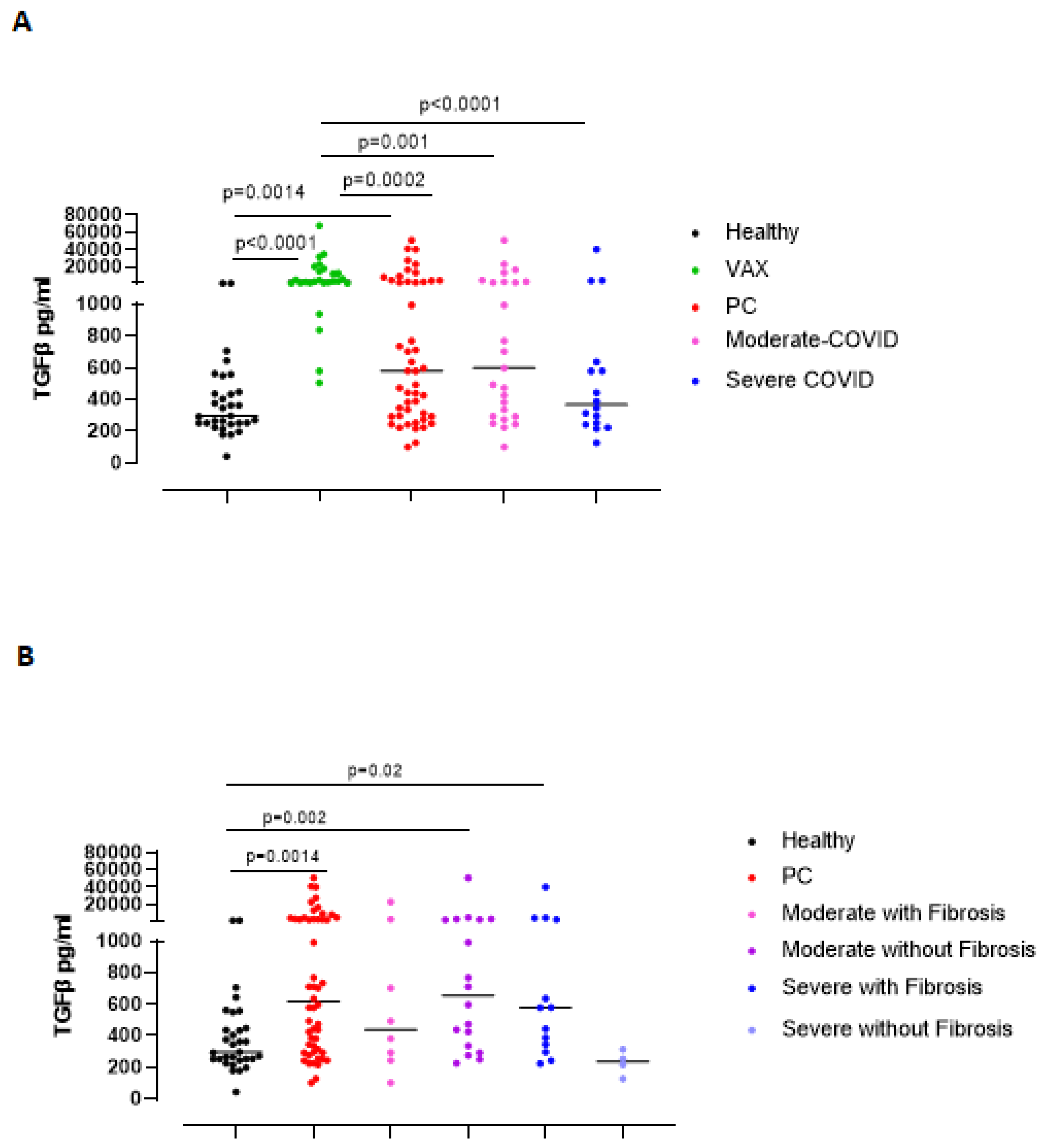
3.3. The Immunosuppressive/Pro-Fibrotic TGF-β Is Higher in Severe Post-COVID-19 Patients Who Had Pulmonary Fibrotic-like Events
3.4. Severe COVID-19 Patients Display Higher Susceptibility to Lung Fibrosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Colarusso, C.; Terlizzi, M.; Pinto, A.; Sorrentino, R. A lesson from a saboteur: High-MW kininogen impact in coronavirus-induced disease 2019. Br. J. Pharmacol. 2020, 177, 4866–4872. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Zhang, Q.; Bastard, P.; Liu, Z.; Le Pen, J.; Moncada-Velez, M.; Chen, J.; Ogishi, M.; Sabli, I.K.D.; Hodeib, S.; Korol, C.; et al. Inborn errors of type I IFN immunity in patients with life-threatening COVID-19. Science 2020, 370, eabd4570. [Google Scholar] [CrossRef]
- Bastard, P.; Rosen, L.B.; Zhang, Q.; Michailidis, E.; Hoffman, H.; Zhang, Y.; Dorgham, K.; Philippot, Q.; Rosain, J.; Béziat, V.; et al. Autoantibodies against type I IFNs in patients with life-threatening COVID-19. Science 2020, 370, eabd4585. [Google Scholar] [CrossRef]
- Callard, F.; Perego, E. How and why patients made Long Covid. Soc. Sci. Med. 2021, 268, 113426. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; Assaf, G.F.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.C.; Yu, C.J.; Chang, S.C.; Galvin, J.R.; Liu, H.M.; Hsiao, C.H.; Kuo, P.H.; Chen, K.Y.; Franks, T.J.; Huang, K.M.; et al. Pulmonary sequelae inconvalescent patients after severe acute respiratory syndrome: Evaluation with thin-section CT. Radiology 2005, 236, 1067–1075. [Google Scholar] [CrossRef] [PubMed]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time Course of Lung Changes at Chest CT during Recovery from Coronavirus Disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polidoro, R.B.; Hagan, R.S.; de Santis Santiago, R.; Schmidt, N.W. Overview: Systemic Inflammatory Response Derived From Lung Injury Caused by SARS-CoV-2 Infection Explains Severe Outcomes in COVID-19. Front. Immunol. 2020, 11, 1626. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Kunichoff, D.; Garshick, M.; Shah, B.; Pillinger, M.; Hochman, J.S.; Berger, J.S. C-reactive protein and clinical outcomes in patients with COVID-19. Eur. Heart J. 2021, 42, 2270–2279. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Jalkanen, J.; Hollmén, M.; Jalkanen, S. Interferon beta-1a for COVID-19: Critical importance of the administration route. Crit. Care 2020, 24, 335. [Google Scholar] [CrossRef] [PubMed]
- Buttmann, M.; Merzyn, C.; Rieckmann, P. Interferon-β induces transient systemic IP-10/CXCL10 chemokine release in patients with multiple sclerosis. J. Neuroimmunol. 2004, 156, 195–203. [Google Scholar] [CrossRef]
- Terlizzi, M.; Molino, A.; Colarusso, C.; Donovan, C.; Imitazione, P.; Somma, P.; Aquino, R.P.; Hansbro, P.M.; Pinto, A.; Sorrentino, R. Activation of the Absent in Melanoma 2 Inflammasome in Peripheral Blood Mononuclear Cells From Idiopathic Pulmonary Fibrosis Patients Leads to the Release of Pro-Fibrotic Mediators. Front. Immunol. 2018, 9, 670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borthwick, L.A. The IL-1 cytokine family and its role in inflammation and fibrosis in the lung. Semin. Immunopathol. 2016, 38, 517–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalli, G.; Colafrancesco, S.; Emmi, G.; Imazio, M.; Lopalco, G.; Maggio, M.C.; Sota, J.; Dinarelloh, C.A. Interleukin 1α: A comprehensive review on the role of IL-1α in the pathogenesis and treatment of autoimmune and inflammatory diseases. Autoimmun. Rev. 2021, 20, 102763. [Google Scholar] [CrossRef] [PubMed]
- Nigdelioglu, R.; Hamanaka, R.B.; Meliton, A.Y.; O’Leary, E.; Witt, L.J.; Cho, T.; Sun, K.; Bonham, C.; Wu, D.; Woods, P.S.; et al. Transforming growth factor (TGF)-β promotes de Novo serine synthesis for collagen production. J. Biol. Chem. 2016, 291, 27239–27251. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, T.; Krammer, F.; Iwasaki, A. The first 12 months of COVID-19: A timeline of immunological insights. Nat. Rev. Immunol. 2021, 21, 245–256. [Google Scholar] [CrossRef]
- Tale, S.; Ghosh, S.; Meitei, S.P.; Kolli, M.; Garbhapu, A.K.; Pudi, S. Post-COVID-19 pneumonia pulmonary fibrosis. QJM Int. J. Med. 2020, 113, 837–838. [Google Scholar] [CrossRef]
- DiPiazza, A.T.; Graham, B.S.; Ruckwardt, T.J. T cell immunity to SARS-CoV-2 following natural infection and vaccination. Biochem. Biophys. Res. Commun 2021, 538, 211–217. [Google Scholar] [CrossRef]
- Chung, J.Y.; Thone, M.N.; Kwon, J.Y. COVID-19 vaccines: The status and perspectives in delivery points of view. Adv. Drug Deliv. Rev. 2021, 170, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Malmström, J.; Lindberg, H.; Lindberg, C.; Bratt, C.; Wieslander, E.; Delander, E.; Särnstrand, B.; Burns, J.S.; Mose-Larsen, P.; Fey, S.; et al. Transforming growth factor-beta 1 specifically induce proteins involved in the myofibroblast contractile apparatus. Mol. Cell. Proteom. 2004, 3, 466–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Sex | Grade | Fibrosis-Like Changes | Comorbidities |
|---|---|---|---|---|
| #1 | F | Moderate | No | Hypertensive heart disease, type II diabetes mellitus, lymphatic stasis, cholangitis |
| #2 | M | Severe | Yes | None |
| #3 | F | Severe | Yes | Systemic arterial hypertension |
| #4 | M | Moderate | Yes | Systemic arterial hypertension, COPD, type II diabetes mellitus |
| #5 | M | Moderate | No | Intermittent bronchial asthma (treated with ICS/LABA as needed), obesity |
| #6 | M | Severe | Yes | Systemic arterial hypertension, dyslipidemia |
| #7 | F | Moderate | No | None |
| #8 | F | Moderate | Yes | Recurrent bronchitis, systemic arterial hypertension |
| #9 | F | Moderate | No | Diabetes mellitus |
| #10 | M | Moderate | No | Hypercholesterolemia, previous pneumonia (2018) |
| #11 | F | Severe | Yes | Systemic arterial hypertension, type 2 diabetes mellitus, hypercholesterolemia |
| #12 | M | Moderate | No | Systemic arterial hypertension |
| #13 | M | Moderate | Yes | Esophagogastroduodenitis, prostatitis |
| #14 | M | Moderate | No | None |
| #15 | M | Severe | Yes | Systemic arterial hypertension, ischemic heart disease, chronic renal failure, ischemic stroke |
| #16 | F | Severe | No | Allergic bronchial asthma |
| #17 | M | Severe | Yes | Systemic arterial hypertension |
| #18 | M | Severe | No | None |
| #19 | F | Moderate | No | Hashimoto’s thyroiditis |
| #20 | M | Severe | Yes | Thrombophlebitis of the right lower limb |
| #21 | M | Moderate | Yes | Chronic HBV-related liver disease, diabetes mellitus, systemic arterial hypertension, previous surgery for kidney stones |
| #22 | F | Moderate | Yes | Systemic arterial hypertension |
| #23 | F | Moderate | No | Bilateral hearing loss |
| #24 | F | Severe | No | Hypertensive heart disease, dysthyroidism, hypercholesterolemia, atopy and allergic rhinosinusitis |
| #25 | M | Severe | No | Gilbert’s syndrome, obesity |
| #26 | M | Moderate | No | Dilated cardiomyopathy |
| #27 | M | Moderate | No | None |
| #28 | F | Moderate | No | Gastroesophageal reflux, colon dyskinesia |
| #29 | M | Moderate | No | Hashimoto’s thyroiditis |
| #30 | F | Severe | Yes | Bronchial asthma, allergic rhinitis |
| #31 | M | Moderate | No | Hypercholesterolemia |
| #32 | F | Moderate | Yes | None |
| #33 | M | Moderate | No | None |
| #34 | Moderate | No | None | |
| #35 | F | Severe | Yes | Depressive syndrome |
| #36 | F | Severe | Yes | Hypothyroidism |
| #37 | M | Severe | Yes | Gastroesophageal reflux |
| #38 | F | Moderate | Yes | None |
| #39 | M | Moderate | No | None |
| #40 | M | Severe | Yes | Hypertension |
| #41 | M | Moderate | No | Chronic ischemic heart disease, chronic atrial fibrillation, type 2 diabetes mellitus, hypertension, dyslipidemia |
| #42 | M | Severe | Yes | None |
| #43 | F | Severe | Yes | None |
| #44 | M | Severe | Yes | Hypertension, gastroesophageal reflux disease, hemorrhoids |
| #45 | M | Severe | Yes | Hypertension, rheumatoid arthritis |
| #46 | M | Severe | Yes | Hypertension, type 2 diabetes mellitus |
| #47 | M | Severe | Yes | Hypertension, gastroesophageal reflux disease |
| #48 | F | Moderate | No | Sideropriva anemia-dystyroidism |
| #49 | M | Moderate | Yes | None |
| #50 | M | Moderate | No | Pulmonary emphysema |
| #51 | M | Moderate | No | None |
| #52 | M | Severe | Yes | None |
| Markers | Healthy | VAX | PC NO-Fibrosis Like Changes | PC Fibrosis Like Changes |
|---|---|---|---|---|
| CRP | 236.2 ± 25.11 | 66.2 ± 16.4 | Moderate: 360.9 ± 33.5 Severe: 376.5 ± 122.2 | Moderate: 302.8 ± 51 Severe: 405.3 ± 65.91 |
| C5b-9 | 382.5 ± 54.08 | 489.1 ± 62.38 | Moderate: 158.5 ± 279.8 Severe: 126.7 ± 274.6 | Moderate: 1058 ± 274.6 Severe: 1528 ± 488.1 |
| LDH | 183.9 ± 14.25 | 923.1 ± 150.5 | Moderate: 10904 ± 1171 Severe: 9370 ± 3114 | Moderate: 13565 ± 1768 Severe: 11496 ± 774.3 |
| IL-6 | 163.4 ± 42.71 | 122.7 ± 10.74 | Moderate: 81.89 ± 15.56 Severe: 45.48 ± 4.7 | Moderate: 86.11 ± 26.9 Severe: 130.2 ± 24.02 |
| IFN-β | 145.4 ± 19.3 | 381.8 ± 33.2 | Moderate: 349.1 ± 47.44 Severe: 442.6 ± 2.40 | Moderate: 239.3 ± 70.3 Severe: 226.4 ± 37.4 |
| CXCL-10 | 201.8 ± 55.4 | 141.4 ± 11.7 | Moderate: 221.1 ± 32.65 Severe: 260.3 ± 71 | Moderate: 211.4 ± 32.65 Severe: 339.9 ± 111.8 |
| IL-1α | 425.4 ± 21.1 | 764.3 ± 135.2 | Moderate: 630 ± 210.9 Severe: 481.8 ± 207.3 | Moderate: 1054 ± 431.4 Severe: 808.5 ± 168.7 |
| TGF-β | 393.8 ± 45.9 | 105.28 ± 298.7 | Moderate: 4260 ± 3122 Severe: 227.3 ± 39.1 | Moderate: 3606 ± 3238 Severe: 4358 ± 3283 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colarusso, C.; Maglio, A.; Terlizzi, M.; Vitale, C.; Molino, A.; Pinto, A.; Vatrella, A.; Sorrentino, R. Post-COVID-19 Patients Who Develop Lung Fibrotic-like Changes Have Lower Circulating Levels of IFN-β but Higher Levels of IL-1α and TGF-β. Biomedicines 2021, 9, 1931. https://doi.org/10.3390/biomedicines9121931
Colarusso C, Maglio A, Terlizzi M, Vitale C, Molino A, Pinto A, Vatrella A, Sorrentino R. Post-COVID-19 Patients Who Develop Lung Fibrotic-like Changes Have Lower Circulating Levels of IFN-β but Higher Levels of IL-1α and TGF-β. Biomedicines. 2021; 9(12):1931. https://doi.org/10.3390/biomedicines9121931
Chicago/Turabian StyleColarusso, Chiara, Angelantonio Maglio, Michela Terlizzi, Carolina Vitale, Antonio Molino, Aldo Pinto, Alessandro Vatrella, and Rosalinda Sorrentino. 2021. "Post-COVID-19 Patients Who Develop Lung Fibrotic-like Changes Have Lower Circulating Levels of IFN-β but Higher Levels of IL-1α and TGF-β" Biomedicines 9, no. 12: 1931. https://doi.org/10.3390/biomedicines9121931