
Metabolic Fatty Liver Disease in Children: A Growing Public Health Problem


Abstract
:1. Introduction
2. General Information on Pediatric MAFLD
2.1. Risk Factors and Epidemiology
2.2. Histological Differences between Pediatric and Adult MAFLD
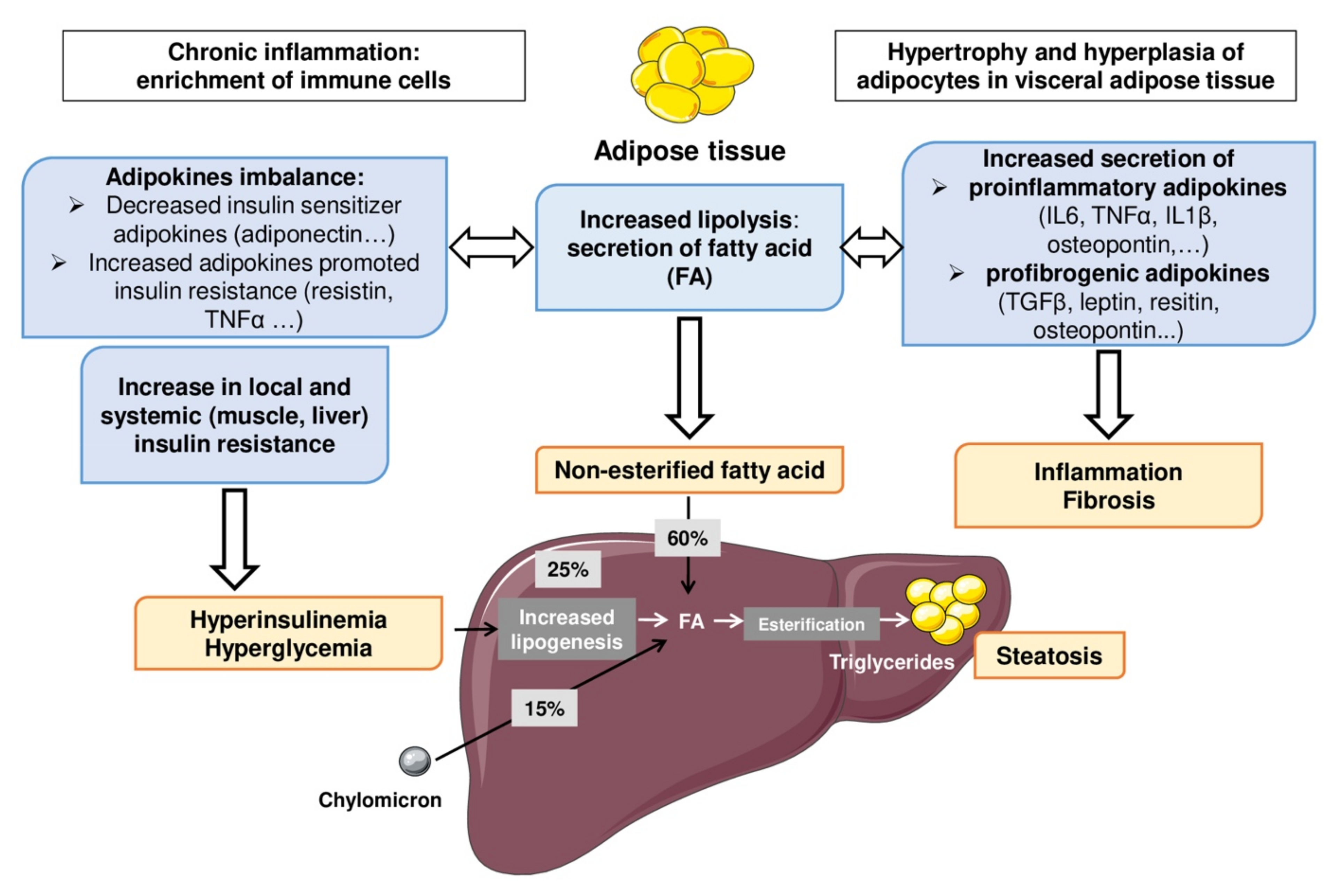
2.3. Pathogenesis of Pediatric MAFLD
2.4. Intra and Extrahepatic Mechanisms
2.5. Involvement of Genetic and Epigenetic Factors
3. Medical Diagnosis
3.1. Liver Biopsy
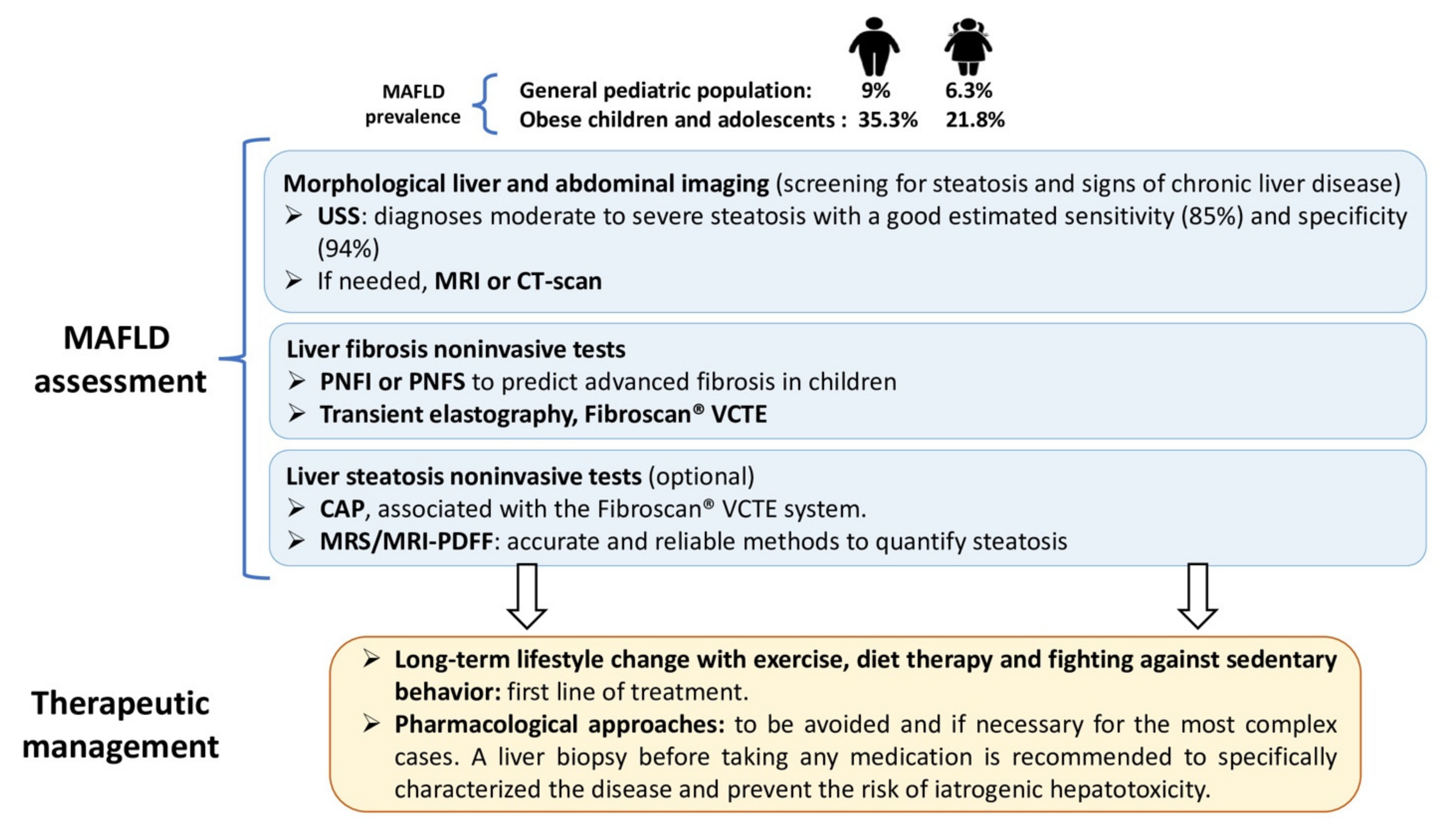
3.2. Noninvasive Methods
3.2.1. Simple Serum Biomarkers
3.2.2. Imaging
Imaging for the Diagnosis and Quantification of Steatosis (USS, CAP, MRI PDFF)
Imaging for the Diagnosis of Cirrhosis and Portal Hypertension
3.2.3. Noninvasive Tests Used to Diagnose and Stage Liver Fibrosis
Serum Markers
Liver Stiffness Measurement
- Transient elastography, VCTE. This noninvasive method was validated for the assessment of moderate to severe liver fibrosis in pediatric MAFLD [52]. However, the size of the cohort was small (n = 54) and only Asian children were included. Different sizes of FibroScan® probes according to the morphology of the patient are available. The S probe should be more appropriate to the thoracic perimeter of children with obesity. Current evidence supports the use of Fibroscan® for the evaluation of MAFLD in the pediatric population [61].
- Magnetic resonance imaging, magnetic resonance elastography (MRE). MRE could more accurately detect advanced fibrosis because this technique is less influenced by abdominal adiposity and assesses a much larger liver volume. A recent study has showed an interest in the use of this imagery. However, this pediatric cohort was limited by the very low prevalence of advanced fibrosis [62].
- Point-shear wave elastography (pSWE). pSWE reveals precise sensitivity of marked fibrosis and has high success rates in discriminating severe from low-grade fibrosis in pediatric liver diseases. It is even more marked in the more severe forms. Shear wave elastographic values were more correlated with liver fibrosis when cirrhotic liver tissue was compared with normal tissue. However, the validity rates for differentiating low-grade liver fibrosis from nonpathological liver tissue were inconsistent. These results should be considered with great caution because of the very small number of patients with MAFLD included in that study (n = 11) [63].
- Bidimensional shear wave elastography (2D-SWE). Values of liver stiffness on 2D-SWE are sensitive to levels of fibrosis and necroinflammation. This technique can ensure excellent diagnostic performance for assessing liver fibrosis in pediatrics. However, potential confounding factors, such as necroinflammatory activity or the level of transaminases should be considered. A recent study including a limited number of MAFLD (5 out of 30 patients) and young patients has been published but requires further investigations [64].
4. Potential Recommendations
4.1. Medical Follow-Up
4.2. Therapeutic Management and Recommendations
4.2.1. Nondrug Strategies
4.2.2. Pharmacological Approaches
4.2.3. Surgical Measures
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AASLD | American Association for the Study of Liver Diseases |
| ALT | alanine transaminase |
| AST | aspartate transaminase |
| BMI | body mass index |
| CAP | controlled attenuation parameter |
| EASD | European Association for the Study of Diabetes |
| EASL | European Association for the Study of the Liver |
| EASO | European Association for the Study of Obesity |
| ENPP1 | ectonucleotide pyrophosphatase phosphodiesterase 1 |
| ESPGHAN | European Society of Pediatric Gastroenterology, Hepatology and Nutrition |
| FIB-4 | fibrosis-4 |
| GCKR | glucokinase regulator |
| GGT | gamma-glutamyltransferase |
| GWAS | genome-wide association studies |
| HSL | hormone-sensitive lipase |
| IR | insulin resistance |
| MAFLD | metabolic associated fatty liver diseases |
| MRE | magnetic resonance elastography |
| MRI-PDFF | magnetic resonance (MR) imaging–proton density fat fraction |
| MRS-PDFF | MR spectroscopy–proton density fat fraction |
| NAFL | nonalcoholic fatty liver |
| NAFLD | nonalcoholic fatty liver disease |
| NASPGHAN | North American Society for Pediatric Gastroenterology, Hepatology and Nutrition |
| NASH | nonalcoholic steatohepatitis |
| PNFI | Pediatric NAFLD Fibrosis Index |
| PNFS | Pediatric NAFLD Fibrosis Score |
| PNPLA3 | patatin-like phospholipase domain-containing protein 3 |
| PPAR | peroxisome proliferator-activated receptor |
| RCT | randomized clinical trial |
| SIRT1 | sirtuin-1 |
| TE | transient elastography |
| TM6SF2 | transmembrane 6 superfamily member 2 |
| USS | ultrasound scan |
| VLDL | very low density lipoprotein |
References
- Swinburn, B.A. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 11. [Google Scholar] [CrossRef]
- Eslam, M. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 17. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Cho, Y.; Jeong, S.W.; Kim, S.U.; Lee, J.-W. On behalf of Korean NAFLD Study Group From nonalcoholic fatty liver disease to metabolic-associated fatty liver disease: Big wave or ripple? Clin. Mol. Hepatol. 2021, 27, 257–269. [Google Scholar] [CrossRef]
- Flisiak-Jackiewicz, M.; Bobrus-Chociej, A.; Wasilewska, N.; Lebensztejn, D.M. From Nonalcoholic Fatty Liver Disease (NAFLD) to Metabolic Dysfunction-Associated Fatty Liver Disease (MAFLD)—New Terminology in Pediatric Patients as a Step in Good Scientific Direction? J. Clin. Med. 2021, 10, 924. [Google Scholar] [CrossRef] [PubMed]
- Di Sessa, A.; Guarino, S.; Umano, G.R.; Arenella, M.; Alfiero, S.; Quaranta, G.; Miraglia del Giudice, E.; Marzuillo, P. MAFLD in Obese Children: A Challenging Definition. Children 2021, 8, 247. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Tacke, F.; Arrese, M.; Chander Sharma, B.; Mostafa, I.; Bugianesi, E.; Wai-Sun Wong, V.; Yilmaz, Y.; George, J.; Fan, J.; et al. Global Perspectives on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis: Hepatology. Hepatology 2019, 69, 2672–2682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuel, V.T. Nonalcoholic Fatty Liver Disease as a Nexus of Metabolic and Hepatic Diseases. Cell Metab. 2019, 27, 22–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lallukka, S. Non-alcoholic fatty liver disease and risk of type 2 diabetes. Best Pract. 2016, 30, 385–395. [Google Scholar] [CrossRef] [Green Version]
- Targher, G.; Bonora, E. Risk of Cardiovascular Disease in Patients with Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2010, 363, 1341–1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lonardo, A.; Mantovani, A.; Lugari, S.; Targher, G. Epidemiology and pathophysiology of the association between NAFLD and metabolically healthy or metabolically unhealthy obesity. Ann. Hepatol. 2020, 19, 359–366. [Google Scholar] [CrossRef]
- Pulgaron, E.R.; Delamater, A.M. Obesity and Type 2 Diabetes in Children: Epidemiology and Treatment. Curr. Diab. Rep. 2014, 14, 508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef] [Green Version]
- Anderson, E.L.; Howe, L.D.; Jones, H.E.; Higgins, J.P.T.; Lawlor, D.A.; Fraser, A. The Prevalence of Non-Alcoholic Fatty Liver Disease in Children and Adolescents: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0140908. [Google Scholar] [CrossRef] [Green Version]
- Schwimmer, J.B.; Deutsch, R.; Kahen, T.; Lavine, J.E.; Behling, C. Prevalence of Fatty Liver in Children and Adolescents. Pediatrics 2006, 118, 1388–1393. [Google Scholar] [CrossRef] [PubMed]
- Vos, M.B.; Abrams, S.H.; Barlow, S.E.; Caprio, S.; Daniels, S.R.; Kohli, R.; Mouzaki, M.; Sathya, P.; Schwimmer, J.B.; Sundaram, S.S.; et al. NASPGHAN Clinical Practice Guideline for the Diagnosis and Treatment of Nonalcoholic Fatty Liver Disease in Children: Recommendations from the Expert Committee on NAFLD (ECON) and the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN). J. Pediatr. Gastroenterol. Nutr. 2017, 64, 319–334. [Google Scholar] [PubMed] [Green Version]
- Nobili, V.; Alisi, A.; Valenti, L.; Miele, L.; Feldstein, A.E.; Alkhouri, N. NAFLD in children: New genes, new diagnostic modalities and new drugs. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 517–530. [Google Scholar] [CrossRef] [PubMed]
- Kleiner, D.E.; Makhlouf, H.R. Histology of NAFLD and NASH in Adults and Children. Clin. Liver. Dis. 2016, 20, 293–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, N.P.; Schwimmer, J.B. The Progression and Natural History of Pediatric Nonalcoholic Fatty Liver Disease. Clin. Liver Dis. 2016, 20, 325–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luci, C.; Bourinet, M.; Leclère, P.S.; Anty, R.; Gual, P. Chronic Inflammation in Non-Alcoholic Steatohepatitis: Molecular Mechanisms and Therapeutic Strategies. Front. Endocrinol. 2020, 11, 597648. [Google Scholar] [CrossRef]
- Luci, C.; Vieira, E.; Bourinet, M.; Rousseau, D.; Bonnafous, S.; Patouraux, S.; Lefevre, L.; Larbret, F.; Prod’homme, V.; Iannelli, A.; et al. SYK-3BP2 Pathway Activity in Parenchymal and Myeloid Cells Is a Key Pathogenic Factor in Metabolic Steatohepatitis. Cell. Mol. Gastroenterol. Hepatol. 2022, 13, 173–191. [Google Scholar] [CrossRef] [PubMed]
- Michalsky, M.; Reichard, K.; Inge, T.; Pratt, J.; Lenders, C. ASMBS pediatric committee best practice guidelines. Surg. Obes. Relat. Dis. 2012, 8, 1–7. [Google Scholar] [CrossRef]
- Gual, P.; Marchand-Brustel, Y.L.; Tanti, J.-F. Positive and negative regulation of insulin signaling through IRS-1 phosphorylation. Biochimie 2005, 87, 99–109. [Google Scholar] [CrossRef]
- Caturano, A.; Acierno, C.; Nevola, R.; Pafundi, P.C.; Galiero, R.; Rinaldi, L.; Salvatore, T.; Adinolfi, L.E.; Sasso, F.C. Non-Alcoholic Fatty Liver Disease: From Pathogenesis to Clinical Impact. Processes 2021, 9, 135. [Google Scholar] [CrossRef]
- Clemente, M.G.; Mandato, C.; Poeta, M.; Vajro, P. Pediatric non-alcoholic fatty liver disease: Recent solutions, unresolved issues, and future research directions. World J. Gastroenterol. 2016, 22, 8078. [Google Scholar] [CrossRef]
- Galiero, R.; Caturano, A.; Vetrano, E.; Cesaro, A.; Rinaldi, L.; Salvatore, T.; Marfella, R.; Sardu, C.; Moscarella, E.; Gragnano, F.; et al. Pathophysiological mechanisms and clinical evidence of relationship between Nonalcoholic fatty liver disease (NAFLD) and cardiovascular disease. Rev. Cardiovasc. Med. 2021, 22, 755. [Google Scholar] [CrossRef] [PubMed]
- Chatelier, E.L. Richness of human gut microbiome correlates with metabolic markers. Nature 2013, 500, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Mouries, J. Microbiota-driven gut vascular barrier disruption is a prerequisite for non-alcoholic steatohepatitis development. J. Hepatol. 2019, 71, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, L.-F.; Luo, W.-H.; Wu, L.-H.; He, X.-X.; Xia, H.H.-X.; Chen, Y. Fecal Microbiota Transplantation for the Treatment of Nonalcoholic Fatty Liver Disease. Explor. Res. Hypothesis Med. 2019, 4, 12–18. [Google Scholar] [CrossRef]
- Kalliomaki, M.; Collado, M.C.; Salminen, S.; Isolauri, E. Early differences in fecal microbiota composition in children may predict overweight. Am. J. Clin. Nutr. 2008, 87, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Sookoian, S.; Pirola, C.J. Liver tissue microbiota in nonalcoholic liver disease: A change in the paradigm of host-bacterial interactions. Hepatobiliary Surg. Nutr. 2021, 10, 337–349. [Google Scholar] [CrossRef]
- Guercio Nuzio, S.; Di Stasi, M.; Pierri, L.; Troisi, J.; Poeta, M.; Bisogno, A.; Belmonte, F.; Tripodi, M.; Di Salvio, D.; Massa, G.; et al. Multiple gut-liver axis abnormalities in children with obesity with and without hepatic involvement: Gut-liver axis, pediatric obesity, NAFLD. Pediatr. Obes. 2017, 12, 446–452. [Google Scholar] [CrossRef]
- Castillo-Leon, E.; Cioffi, C.E.; Vos, M.B. Perspectives on youth-onset nonalcoholic fatty liver disease. Endocrinol. Diabetes Metab. 2020, 3, e00184. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Valenti, L.; Romeo, S. Genetics and epigenetics of NAFLD and NASH: Clinical impact. J. Hepatol. 2018, 68, 268–279. [Google Scholar] [CrossRef]
- Caussy, C.; Soni, M.; Cui, J.; Bettencourt, R.; Schork, N.; Chen, C.-H.; Ikhwan, M.A.; Bassirian, S.; Cepin, S.; Gonzalez, M.P.; et al. Nonalcoholic fatty liver disease with cirrhosis increases familial risk for advanced fibrosis. J. Clin. Invest. 2017, 127, 2697–2704. [Google Scholar] [CrossRef] [Green Version]
- Dongiovanni, P.; Stender, S.; Pietrelli, A.; Mancina, R.M.; Cespiati, A.; Petta, S.; Pelusi, S.; Pingitore, P.; Badiali, S.; Maggioni, M.; et al. Causal relationship of hepatic fat with liver damage and insulin resistance in nonalcoholic fatty liver. J. Intern. Med. 2018, 283, 356–370. [Google Scholar] [CrossRef]
- Dongiovanni, P.; Valenti, L.; Rametta, R.; Daly, A.K.; Nobili, V.; Mozzi, E.; Leathart, J.B.S.; Pietrobattista, A.; Burt, A.D.; Maggioni, M.; et al. Genetic variants regulating insulin receptor signalling are associated with the severity of liver damage in patients with non-alcoholic fatty liver disease. Gut 2010, 59, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Suomela, E. Childhood predictors of adult fatty liver. The Cardiovascular Risk in Young Finns Study. J. Hepatol. 2016, 65, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahimlou, M. Dietary supplements and pediatric non-alcoholic fatty liver disease: Present and the future. World J. Hepatol. 2015, 7, 2597. [Google Scholar] [CrossRef] [PubMed]
- Querter, I.; Pauwels, N.S.; De Bruyne, R.; Dupont, E.; Verhelst, X.; Devisscher, L.; Van Vlierberghe, H.; Geerts, A.; Lefere, S. Maternal and Perinatal Risk Factors for Pediatric Nonalcoholic Fatty Liver Disease: A Systematic Review. Clin. Gastroenterol. Hepatol. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Hagström, H.; Simon, T.G.; Roelstraete, B.; Stephansson, O.; Söderling, J.; Ludvigsson, J.F. Maternal obesity increases the risk and severity of NAFLD in offspring. J. Hepatol. 2021, 75, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Ayonrinde, O.T.; Oddy, W.H.; Adams, L.A.; Mori, T.A.; Beilin, L.J.; de Klerk, N.; Olynyk, J.K. Infant nutrition and maternal obesity influence the risk of non-alcoholic fatty liver disease in adolescents. J. Hepatol. 2017, 67, 568–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, M.; Grab, J.; Dodge, J.L.; Gunderson, E.P.; Rubin, J.; Irani, R.A.; Cedars, M.; Terrault, N. Non-alcoholic fatty liver disease in pregnancy is associated with adverse maternal and perinatal outcomes. J. Hepatol. 2020, 73, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.; Valenti, L.; Scorletti, E.; Byrne, C.; Nobili, V. Nonalcoholic Fatty Liver Disease in Children. Semin. Liver Dis. 2018, 38, 001–013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caussy, C.; Tripathi, A.; Humphrey, G.; Bassirian, S.; Singh, S.; Faulkner, C.; Bettencourt, R.; Rizo, E.; Richards, L.; Xu, Z.Z.; et al. A gut microbiome signature for cirrhosis due to nonalcoholic fatty liver disease. Nat. Commun. 2019, 10, 1406. [Google Scholar] [CrossRef]
- Bae-Gartz, I.; Kasper, P.; Großmann, N.; Breuer, S.; Janoschek, R.; Kretschmer, T.; Appel, S.; Schmitz, L.; Vohlen, C.; Quaas, A.; et al. Maternal exercise conveys protection against NAFLD in the offspring via hepatic metabolic programming. Sci. Rep. 2020, 10, 15424. [Google Scholar] [CrossRef]
- Ornellas, F. Obese fathers lead to an altered metabolism and obesity in their children in adulthood: Review of experimental and human studies. J. Pediatr. 2017, 93, 551–559. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Bussler, S.; Vogel, M.; Pietzner, D.; Harms, K.; Buzek, T.; Penke, M.; Händel, N.; Körner, A.; Baumann, U.; Kiess, W.; et al. New pediatric percentiles of liver enzyme serum levels (alanine aminotransferase, aspartate aminotransferase, γ-glutamyltransferase): Effects of age, sex, body mass index, and pubertal stage. Hepatology 2018, 68, 1319–1330. [Google Scholar] [CrossRef] [Green Version]
- Shannon, A.; Alkhouri, N.; Carter-Kent, C.; Monti, L.; Devito, R.; Lopez, R.; Feldstein, A.E.; Nobili, V. Ultrasonographic Quantitative Estimation of Hepatic Steatosis in Children With NAFLD. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 190–195. [Google Scholar] [CrossRef] [Green Version]
- Vajro, P.; Lenta, S.; Socha, P.; Dhawan, A.; McKiernan, P.; Baumann, U.; Durmaz, O.; Lacaille, F.; McLin, V.; Nobili, V. Diagnosis of Nonalcoholic Fatty Liver Disease in Children and Adolescents: Position Paper of the ESPGHAN Hepatology Committee. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 700–713. [Google Scholar] [CrossRef]
- D’Hondt, A.; Rubesova, E.; Xie, H.; Shamdasani, V.; Barth, R.A. Liver Fat Quantification by Ultrasound in Children: A Prospective Study. Am. J. Roentgenol. 2021, 217, 996–1006. [Google Scholar] [CrossRef]
- Shin, J. Quick assessment with controlled attenuation parameter for hepatic steatosis in children based on MRI-PDFF as the gold standard. BMC Pediatr. 2019, 19, 112. [Google Scholar] [CrossRef] [Green Version]
- Alkhouri, N.; Mansoor, S.; Giammaria, P.; Liccardo, D.; Lopez, R.; Nobili, V. The Development of the Pediatric NAFLD Fibrosis Score (PNFS) to Predict the Presence of Advanced Fibrosis in Children with Nonalcoholic Fatty Liver Disease. PLoS ONE 2014, 9, e104558. [Google Scholar]
- Di Martino, M.; Pacifico, L.; Bezzi, M.; Di Miscio, R.; Sacconi, B.; Chiesa, C.; Catalano, C. Comparison of magnetic resonance spectroscopy, proton density fat fraction and histological analysis in the quantification of liver steatosis in children and adolescents. World J. Gastroenterol. 2016, 22, 8812. [Google Scholar] [CrossRef] [PubMed]
- Berzigotti, A.; Tsochatzis, E.; Boursier, J.; Castera, L.; Cazzagon, N.; Friedrich-Rust, M.; Petta, S.; Thiele, M. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis–2021 update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef] [PubMed]
- Wan, F.; Pan, F.; Ayonrinde, O.T.; Adams, L.A.; Mori, T.A.; Beilin, L.J.; O’Sullivan, T.A.; Olynyk, J.K.; Oddy, W.H. Validation of fatty liver disease scoring systems for ultrasound diagnosed non-alcoholic fatty liver disease in adolescents. Dig. Liver Dis. 2021, 53, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Nobili, V.; Alisi, A.; Vania, A.; Tiribelli, C.; Pietrobattista, A.; Bedogni, G. The pediatric NAFLD fibrosis index: A predictor of liver fibrosis in children with non-alcoholic fatty liver disease. BMC Med. 2009, 7, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Lédinghen, V.; Le Bail, B.; Rebouissoux, L.; Fournier, C.; Foucher, J.; Miette, V.; Castéra, L.; Sandrin, L.; Merrouche, W.; Lavrand, F.; et al. Liver Stiffness Measurement in Children Using FibroScan: Feasibility Study and Comparison With Fibrotest, Aspartate Transaminase to Platelets Ratio Index, and Liver Biopsy. J. Pediatr. Gastroenterol. Nutr. 2007, 45, 443–450. [Google Scholar] [CrossRef] [Green Version]
- Nobili, V.; Parkes, J.; Bottazzo, G.; Marcellini, M.; Cross, R.; Newman, D.; Vizzutti, F.; Pinzani, M.; Rosenberg, W.M. Performance of ELF Serum Markers in Predicting Fibrosis Stage in Pediatric Non-Alcoholic Fatty Liver Disease. Gastroenterology 2009, 136, 160–167. [Google Scholar] [CrossRef]
- Chen, B.R.; Pan, C.Q. Non-invasive assessment of fibrosis and steatosis in pediatric non-alcoholic fatty liver disease. Clin. Res. Hepatol. Gastroenterol. 2022, 46, 101755. [Google Scholar] [CrossRef] [PubMed]
- Xanthakos, S.A.; Trout, A.T.; Dillman, J.R. Magnetic resonance elastography assessment of fibrosis in children with NAFLD: Promising but not perfect. Hepatology 2017, 66, 1373–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özkan, M.B.; Bilgici, M.C.; Eren, E.; Caltepe, G.; Yilmaz, G.; Kara, C.; Gun, S. Role of Point Shear Wave Elastography in the Determination of the Severity of Fibrosis in Pediatric Liver Diseases With Pathologic Correlations: Point Shear Wave Elastography in Pediatric Liver Diseases. J. Ultrasound Med. 2017, 36, 2337–2344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Choi, Y.H.; Cho, Y.J.; Lee, S.B.; Cheon, J.-E.; Kim, W.S.; Ko, J.S.; Koh, J.; Kang, G.H. The usefulness of noninvasive liver stiffness assessment using shear-wave elastography for predicting liver fibrosis in children. BMC Med. Imaging 2021, 21, 68. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, A.E.; Charatcharoenwitthaya, P.; Treeprasertsuk, S.; Benson, J.T.; Enders, F.B.; Angulo, P. The natural history of non-alcoholic fatty liver disease in children: A follow-up study for up to 20 years. Gut 2009, 58, 1538–1544. [Google Scholar] [CrossRef] [PubMed]
- Carriere, C.; Thibault, H.; Barat, P.; Guemazi-Kheffi, F.; Mellouet-Fort, B.; Ancillon, L.; Bertrand, A.; Quinart, S.; Guilmin-Crépon, S.; Arsan, A.; et al. Short-term and long-term positive outcomes of the multidisciplinary care implemented by the French health networks for the prevention and care of paediatric overweight and obesity. Pediatr. Obes. 2019, 14, e12522. [Google Scholar] [CrossRef] [PubMed]
- Tricò, D.; Caprio, S.; Umano, G.R.; Pierpont, B.; Nouws, J.; Galderisi, A.; Kim, G.; Mata, M.M.; Santoro, N. Metabolic Features of Nonalcoholic Fatty Liver (NAFL) in Obese Adolescents: Findings From a Multiethnic Cohort. Hepatology 2018, 68, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeVore, S.; Kohli, R.; Lake, K.; Nicholas, L.; Dietrich, K.; Xanthakos, S.A. A Multidisciplinary Clinical Program is Effective in Stabilizing BMI and Reducing Transaminase Levels in Pediatric Patients with NAFLD. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 119–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Ruiz, K.; Ramírez-Vélez, R.; Correa-Bautista, J.E.; Peterson, M.D.; García-Hermoso, A. The Effects of Exercise on Abdominal Fat and Liver Enzymes in Pediatric Obesity: A Systematic Review and Meta-Analysis. Child. Obes. 2017, 13, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A.; Heisel, W.E.; Afshin, A.; Jensen, M.D.; Dietz, W.H.; Long, M.; Kushner, R.F.; Daniels, S.R.; Wadden, T.A.; Tsai, A.G.; et al. The Science of Obesity Management: An Endocrine Society Scientific Statement. Endocr. Rev. 2018, 39, 79–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flisiak-Jackiewicz, M.; Lebensztejn, D.M. Update on pathogenesis, diagnostics and therapy of nonalcoholic fatty liver disease in children. Clin. Exp. Hepatol. 2019, 5, 11–21. [Google Scholar] [CrossRef]
- Lavine, J.E. Effect of Vitamin E or Metformin for Treatment of Nonalcoholic Fatty Liver Disease in Children and Adolescents: The TONIC Randomized Controlled Trial. JAMA 2011, 305, 1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vos, M.B.; Jin, R.; Konomi, J.V.; Cleeton, R.; Cruz, J.; Karpen, S.; Rodriguez, D.S.; Frediani, J.K.; McCracken, C.; Welsh, J. A randomized, controlled, crossover pilot study of losartan for pediatric nonalcoholic fatty liver disease. Pilot Feasibility Stud. 2018, 4, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratziu, V.; Harrison, S.A.; Francque, S.; Bedossa, P.; Lehert, P.; Serfaty, L.; Romero-Gomez, M.; Boursier, J.; Abdelmalek, M.; Caldwell, S.; et al. Elafibranor, an Agonist of the Peroxisome Proliferator–Activated Receptor–α and –δ, Induces Resolution of Nonalcoholic Steatohepatitis Without Fibrosis Worsening. Gastroenterology 2016, 150, 1147–1159.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, B.; Lu, L.G. Efficacy and safety of drugs for nonalcoholic steatohepatitis. J. Dig. Dis. 2021, 22, 72–82. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Gaunt, P.; Aithal, G.P.; Barton, D.; Hull, D.; Parker, R.; Hazlehurst, J.M.; Guo, K.; Abouda, G.; Aldersley, M.A.; et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): A multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet 2016, 387, 679–690. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, R.M.; Steen, O. Semaglutide: Review and Place in Therapy for Adults With Type 2 Diabetes. Can. J. Diabetes 2019, 43, 136–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toyama, T.; Neuen, B.L.; Jun, M.; Ohkuma, T.; Neal, B.; Jardine, M.J.; Heerspink, H.L.; Wong, M.G.; Ninomiya, T.; Wada, T.; et al. Effect of SGLT2 inhibitors on cardiovascular, renal and safety outcomes in patients with type 2 diabetes mellitus and chronic kidney disease: A systematic review and meta-analysis. Diabetes Obes. Metab. 2019, 21, 1237–1250. [Google Scholar] [CrossRef] [Green Version]
- Pasternak, B.; Wintzell, V.; Eliasson, B.; Svensson, A.M.; Franzén, S.; Gudbjörnsdottir, S.; Hveem, K.; Jonasson, C.; Melbye, M.; Svanström, H.; et al. Use of Glucagon-Like Peptide 1 Receptor Agonists and Risk of Serious Renal Events: Scandinavian Cohort Study. Diabetes Care 2020, 43, 10. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Pratt, J.S.A.; Browne, A.; Browne, N.T.; Bruzoni, M.; Cohen, M.; Desai, A.; Inge, T.; Linden, B.C.; Mattar, S.G.; Michalsky, M.; et al. ASMBS pediatric metabolic and bariatric surgery guidelines, 2018. Surg. Obes. Relat. Dis. 2018, 14, 882–901. [Google Scholar] [CrossRef] [PubMed]
- Facn, M.M. The Benefit of Sleeve Gastrectomy in Obese Adolescents on Nonalcoholic Steatohepatitis and Hepatic Fibrosis. J. Pediatr. 2017, 180, 31–37.e2. [Google Scholar]
- Lassailly, G.; Caiazzo, R.; Ntandja-Wandji, L.-C.; Gnemmi, V.; Baud, G.; Verkindt, H.; Ningarhari, M.; Louvet, A.; Leteurtre, E.; Raverdy, V.; et al. Bariatric Surgery Provides Long-term Resolution of Nonalcoholic Steatohepatitis and Regression of Fibrosis. Gastroenterology 2020, 159, 1290–1301.e5. [Google Scholar] [CrossRef] [PubMed]
- Nobili, V.; Vajro, P.; Dezsofi, A.; Fischler, B.; Hadzic, N.; Jahnel, J.; Lamireau, T.; McKiernan, P.; McLin, V.; Socha, P.; et al. Indications and Limitations of Bariatric Intervention in Severely Obese Children and Adolescents With and Without Nonalcoholic Steatohepatitis: ESPGHAN Hepatology Committee Position Statement. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 550–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chavez-Tapia, N.C.; Tellez-Avila, F.I.; Barrientos-Gutierrez, T.; Mendez-Sanchez, N.; Lizardi-Cervera, J.; Uribe, M. Bariatric surgery for non-alcoholic steatohepatitis in obese patients. Cochrane Database Syst. Rev. 2010, CD007340. [Google Scholar] [CrossRef]
- Shingina, A.; DeWitt, P.E.; Dodge, J.L.; Biggins, S.W.; Gralla, J.; Sprague, D.; Bambha, K. Future Trends in Demand for Liver Transplant: Birth Cohort Effects Among Patients With NASH and HCC. Transplantation 2019, 103, 140–148. [Google Scholar] [CrossRef]
- Popkin, B.M.; Corvalan, C.; Grummer-Strawn, L.M. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet 2020, 395, 65–74. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Variant | Function | Clinical Form | Reference |
|---|---|---|---|---|
| PNPLA3 | I148M | Lipid droplets remodeling | NAFL with the risk of progressive steatosis | [33] |
| TM6SF2 | E167K | Impact VLDL-mediated lipid secretion leading to fat accumulation in liver | NAFL | [32] |
| GCKR | rs1260326 | Inhibition of glucokinase enzymatic activity and modulation of hepatic lipogenesis | NAFL | [32] |
| IFNL4 | rs368234815 δG | Increase fat accumulation | NAFL | [16] |
| Indexes Scores | Clinical and Biological Data | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Age | BMI | WC (cm) | Fasted TG | ALT | AST | Platelet Count (109/L) | Albumin (g/dL) | Reference | |
| APRI | X | X | X | [57] | |||||
| FIB-4 | X | X | X | X | [57] | ||||
| PNFI | X | X | X | [58] | |||||
| PNFS | X | X | X | X | X | X | [53] | ||
| Clinical Trial | State | Sample and Size | Drug | Target | Potential Side Effects |
|---|---|---|---|---|---|
| NCT01913470 | Phase IIa | 11–19 years old N = 12 | Losartan | Angiotensin II receptor antagonist | No specific side effect reported |
| NCT03883607 | Phase IIa | 8–17 years old N = 10 | Elafibranor | PPAR-α and PPAR-δ | No specific side effect reported |
| NCT03867487 | Phase IIa (suspended due to COVID-19 pandemic) | 12–20 years old N = 40 (estimated enrollment) | Empagliflozin | SGLT-2 | In adult, urinary tract infections |
| NCT05067621 | Phase III (ongoing patient recruitment) | 10–21 years old N = 60 (estimated enrollment) | Liraglutide | GLP-1 receptor agonists | Gastrointestinal symptoms |
| NCT03919929 | Phase III (ongoing patient recruitment) | 12–21 years old N = 50 (estimated enrollment) | Semaglutide | GLP-1 receptor agonists | Gastrointestinal symptoms |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le Garf, S.; Nègre, V.; Anty, R.; Gual, P. Metabolic Fatty Liver Disease in Children: A Growing Public Health Problem. Biomedicines 2021, 9, 1915. https://doi.org/10.3390/biomedicines9121915
Le Garf S, Nègre V, Anty R, Gual P. Metabolic Fatty Liver Disease in Children: A Growing Public Health Problem. Biomedicines. 2021; 9(12):1915. https://doi.org/10.3390/biomedicines9121915
Chicago/Turabian StyleLe Garf, Sébastien, Véronique Nègre, Rodolphe Anty, and Philippe Gual. 2021. "Metabolic Fatty Liver Disease in Children: A Growing Public Health Problem" Biomedicines 9, no. 12: 1915. https://doi.org/10.3390/biomedicines9121915