
Current Overview on Therapeutic Potential of Vitamin D in Inflammatory Lung Diseases

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Method of Literature Search
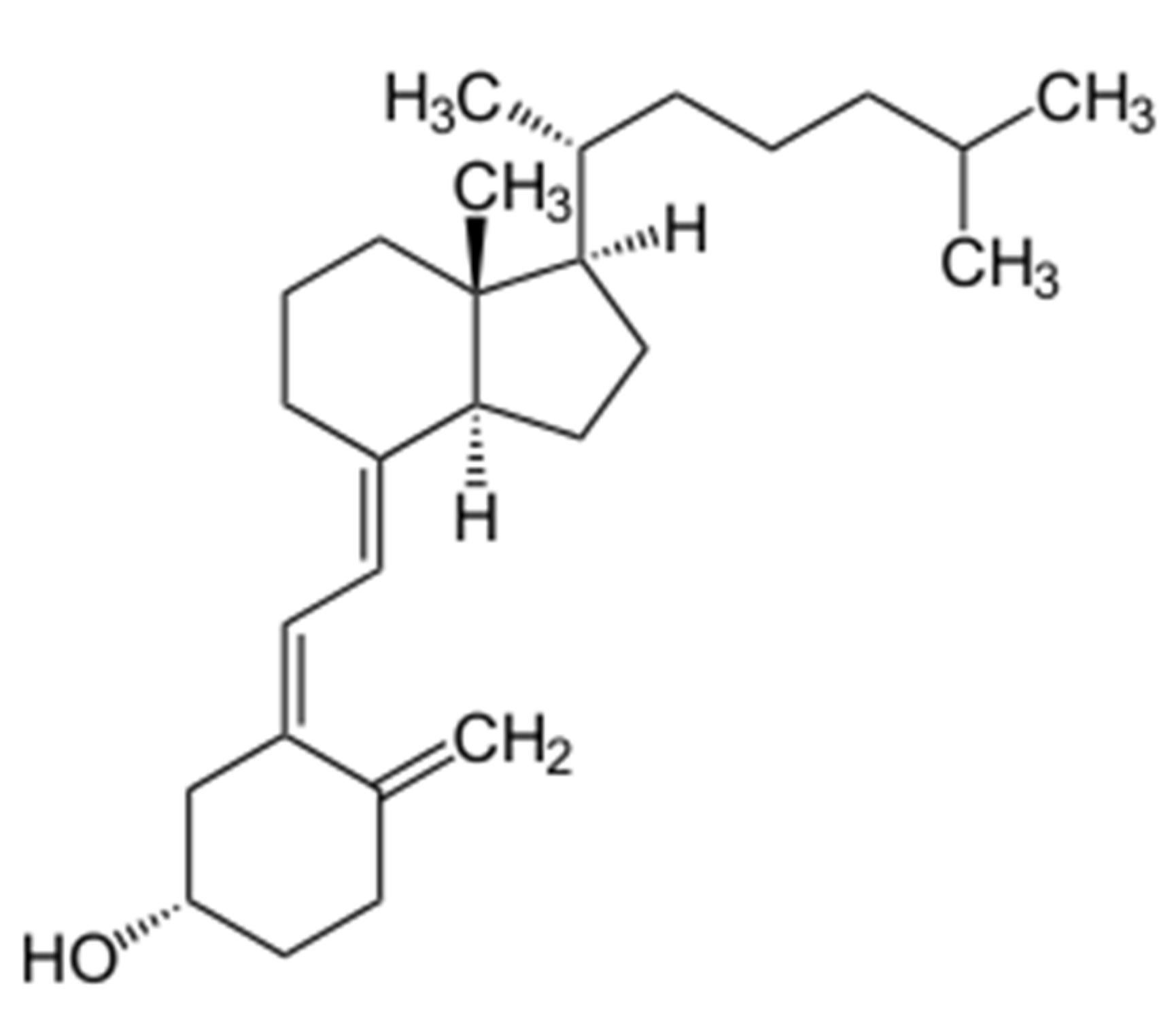
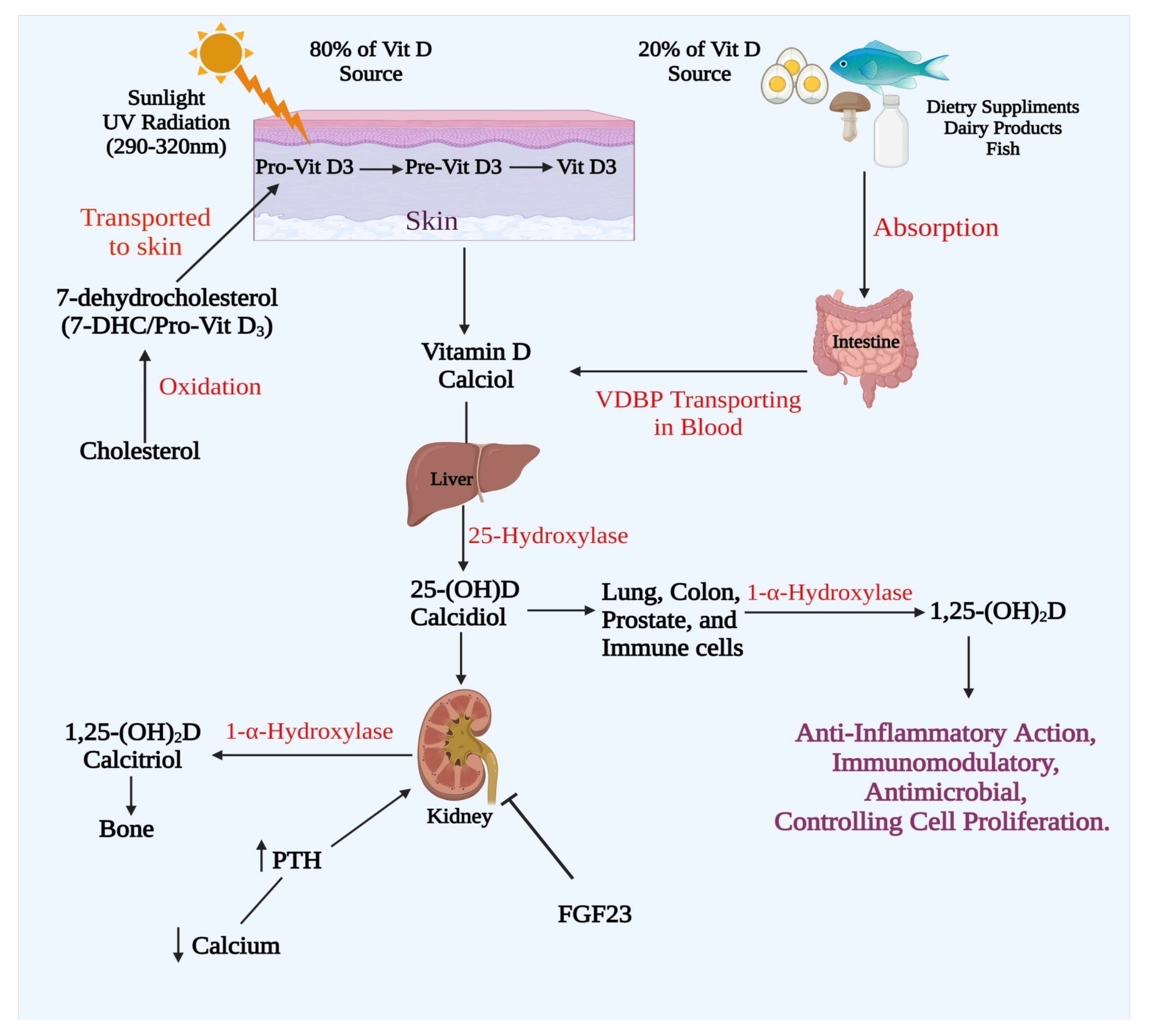
3. The Metabolism of Vitamin D
4. Conventional Metabolic Pathway
5. Alternative Metabolic Pathway
6. Vitamin D Metabolism and Hormonal Regulation
7. Vitamin D Consumption and Status
8. Inflammatory Lung Diseases
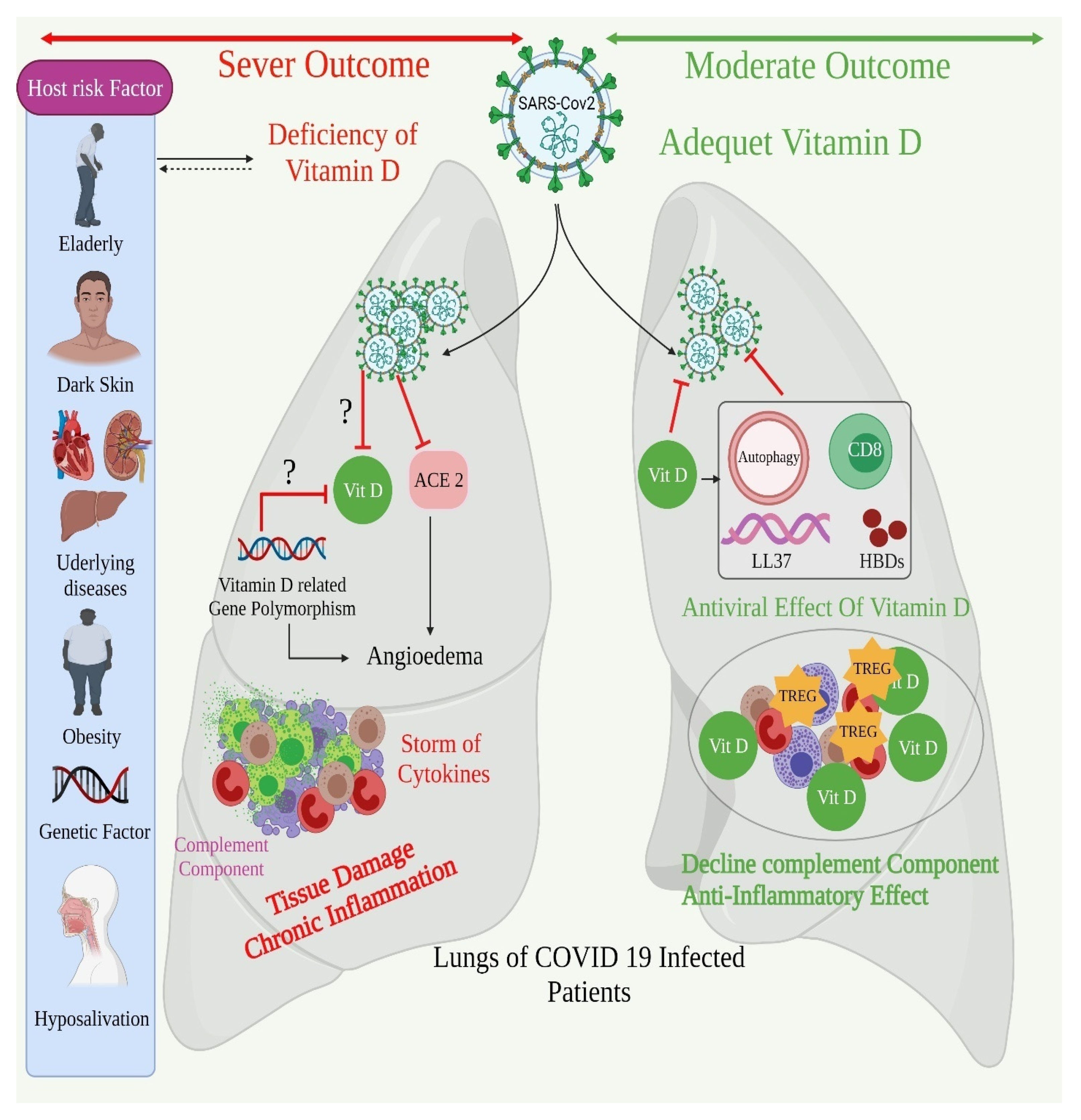
8.1. Inflammation Mechanism in Lung Diseases
8.2. The Anti-Inflammatory Property of Vitamin D
8.3. Vitamin D Dysregulation in Inflammatory Lung Diseases
9. Vitamin D-Based Therapy in Asthma
10. Vitamin D Based Therapy in COPD
11. Vitamin D Based Therapy in Lung Cancer
12. Vitamin D Based Therapy in Pulmonary and Cystic Fibrosis
13. Vitamin D Based Therapy in Pulmonary Infection including COVID-19
13.1. Pneumonia
13.2. Tuberculosis
13.3. COVID-19
14. Excessive Use of Vitamin D Pharmaceutical Formulations
15. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abrishami, A.; Dalili, N.; Mohammadi Torbati, P.; Asgari, R.; Arab-Ahmadi, M.; Behnam, B.; Sanei-Taheri, M. Possible association of vitamin D status with lung involvement and outcome in patients with COVID-19: A retrospective study. Eur. J. Nutr. 2021, 60, 2249–2257. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Arora, S.; Khan, S.; Mohsin, M.; Mohan, A.; Manda, K.; Syed, M.A. Vitamin D and its therapeutic relevance in pulmonary diseases. J. Nutr. Biochem. 2021, 90, 108571. [Google Scholar] [CrossRef] [PubMed]
- Alavi Foumani, A.; Mehrdad, M.; Jafarinezhad, A.; Nokani, K.; Jafari, A. Impact of vitamin D on spirometry findings and quality of life in patients with chronic obstructive pulmonary disease: A randomized, double-blinded, placebo-controlled clinical trial. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 1495–1501. [Google Scholar] [CrossRef] [Green Version]
- Al-Beltagi, M.; Rowiesha, M.; Elmashad, A.; Elrifaey, S.M.; Elhorany, H.; Koura, H.G. Vitamin D status in preterm neonates and the effects of its supplementation on respiratory distress syndrome. Pediatr. Pulmonol. 2020, 55, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Dixit, D.; Bridgeman, M.B.; Madduri, R.P.; Kumar, S.T.; Cawley, M.J. Pharmacological Management and Prevention of Exacerbations of Chronic Obstructive Pulmonary Disease in Hospitalized Patients. Pharm. Ther. 2016, 41, 703–712. [Google Scholar]
- Royce, S.G.; Moodley, Y.; Samuel, C.S. Novel therapeutic strategies for lung disorders associated with airway remodelling and fibrosis. Pharm. Ther. 2014, 141, 250–260. [Google Scholar] [CrossRef]
- Cazzola, M.; Page, C.P.; Calzetta, L.; Matera, M.G. Pharmacology and therapeutics of bronchodilators. Pharmacol. Rev. 2012, 64, 450–504. [Google Scholar] [CrossRef]
- Balcells, M.E.; Yokobori, N.; Hong, B.Y.; Corbett, J.; Cervantes, J. The lung microbiome, vitamin D, and the tuberculous granuloma: A balance triangle. Microb. Pathog. 2019, 131, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Bilezikian, J.P.; Bikle, D.; Hewison, M.; Lazaretti-Castro, M.; Formenti, A.M.; Gupta, A.; Madhavan, M.V.; Nair, N.; Babalyan, V.; Hutchings, N.; et al. Mechanisms in Endocrinology: Vitamin D and COVID-19. Eur. J. Endocrinol. 2020, 183, R133–R147. [Google Scholar] [CrossRef]
- Brehm, J.M. Vitamin D and asthma-life after VIDA? Curr. Allergy Asthma Rep. 2014, 14, 461. [Google Scholar] [CrossRef] [Green Version]
- Brumpton, B.M.; Langhammer, A.; Henriksen, A.H.; Camargo, C.A., Jr.; Chen, Y.; Romundstad, P.R.; Mai, X.M. Vitamin D and Lung Function Decline in Adults with Asthma: The HUNT Study. Am. J. Epidemiol. 2016, 183, 739–746. [Google Scholar] [CrossRef] [Green Version]
- Cannell, J.J.; Vieth, R.; Umhau, J.C.; Holick, M.F.; Grant, W.B.; Madronich, S.; Garland, C.F.; Giovannucci, E. Epidemic influenza and vitamin D. Epidemiol. Infect. 2006, 134, 1129–1140. [Google Scholar] [CrossRef] [PubMed]
- Cantorna, M.T. Vitamin D and Lung Infection. Infect. Immun. 2016, 84, 3094–3096. [Google Scholar] [CrossRef] [Green Version]
- Cepeda, S.J.; Zenteno, A.D.; Fuentes, S.C.; Bustos, B.R. Vitamin D and pediatrics respiratory diseases. Rev. Chil. Pediatr. 2019, 90, 94–101. [Google Scholar] [CrossRef] [Green Version]
- Chen, F.Y.; Xiao, M.; Ling, B.; Liu, L.; Chen, L. Vitamin D does not improve lung function decline in COPD: A meta-analysis. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 8637–8644. [Google Scholar] [CrossRef]
- Chen, L.; Wilson, R.; Bennett, E.; Zosky, G.R. Identification of vitamin D sensitive pathways during lung development. Respir. Res. 2016, 17, 47. [Google Scholar] [CrossRef] [Green Version]
- Chesdachai, S.; Tangpricha, V. Treatment of vitamin D deficiency in cystic fibrosis. J. Steroid Biochem. Mol. Biol. 2016, 164, 36–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chishimba, L.; Thickett, D.R.; Stockley, R.A.; Wood, A.M. The vitamin D axis in the lung: A key role for vitamin D-binding protein. Thorax 2010, 65, 456–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dancer, R.C.; Parekh, D.; Lax, S.; D’Souza, V.; Zheng, S.; Bassford, C.R.; Park, D.; Bartis, D.G.; Mahida, R.; Turner, A.M.; et al. Vitamin D deficiency contributes directly to the acute respiratory distress syndrome (ARDS). Thorax 2015, 70, 617–624. [Google Scholar] [CrossRef] [Green Version]
- Foong, R.E.; Zosky, G.R. Vitamin D deficiency and the lung: Disease initiator or disease modifier? Nutrients 2013, 5, 2880–2900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganji, V.; Al-Obahi, A.; Yusuf, S.; Dookhy, Z.; Shi, Z. Serum vitamin D is associated with improved lung function markers but not with prevalence of asthma, emphysema, and chronic bronchitis. Sci. Rep. 2020, 10, 11542. [Google Scholar] [CrossRef]
- Gao, Y.; Zhao, Q.; Qiu, X.; Zhuang, Y.; Yu, M.; Dai, J.; Cai, H.; Yan, X. Vitamin D levels are prognostic factors for connective tissue disease associated interstitial lung disease (CTD-ILD). Aging 2020, 12, 4371–4378. [Google Scholar] [CrossRef] [PubMed]
- Gnagnarella, P.; Raimondi, S.; Aristarco, V.; Johansson, H.A.; Bellerba, F.; Corso, F.; Gandini, S. Vitamin D Receptor Polymorphisms and Cancer. Adv. Exp. Med. Biol. 2020, 1268, 53–114. [Google Scholar] [CrossRef]
- Gold, D.R.; Litonjua, A.A.; Carey, V.J.; Manson, J.E.; Buring, J.E.; Lee, I.M.; Gordon, D.; Walter, J.; Friedenberg, G.; Hankinson, J.L.; et al. Lung VITAL: Rationale, design, and baseline characteristics of an ancillary study evaluating the effects of vitamin D and/or marine omega-3 fatty acid supplements on acute exacerbations of chronic respiratory disease, asthma control, pneumonia and lung function in adults. Contemp. Clin. Trials 2016, 47, 185–195. [Google Scholar] [CrossRef]
- González Jiménez, D.; Muñoz Codoceo, R.; Garriga García, M.; Molina Arias, M.; Alvarez Beltran, M.; García Romero, R.; Martínez Costa, C.; Meavilla Olivas, S.M.; Peña Quintana, L.; Gallego Gutierrez, S.; et al. Vitamin D and Chronic Lung Colonization in Pediatric and Young Adults Cystic Fibrosis Patients. Nutr. Hosp. 2015, 32, 1629–1635. [Google Scholar] [CrossRef] [PubMed]
- Guijarro, T.; Magro-Lopez, E.; Manso, J.; Garcia-Martinez, R.; Fernandez-Aceñero, M.J.; Liste, I.; Zambrano, A. Detrimental pro-senescence effects of vitamin D on lung fibrosis. Mol. Med. 2018, 24, 64. [Google Scholar] [CrossRef] [PubMed]
- Richart, T.; Thijs, L.; Nawrot, T.; Yu, J.; Kuznetsova, T.; Balkestein, E.J.; Struijker-Boudier, H.A.; Staessen, J.A. The metabolic syndrome and carotid intima-media thickness in relation to the parathyroid hormone to 25-OH-D(3) ratio in a general population. Am. J. Hypertens. 2011, 24, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Rudnicki, M.; Thode, J.; Jørgensen, T.; Heitmann, B.L.; Sørensen, O.H. Effects of age, sex, season and diet on serum ionized calcium, parathyroid hormone and vitamin D in a random population. J. Intern. Med. 1993, 234, 195–200. [Google Scholar] [CrossRef]
- Samefors, M.; Östgren, C.J.; Mölstad, S.; Lannering, C.; Midlöv, P.; Tengblad, A. Vitamin D deficiency in elderly people in Swedish nursing homes is associated with increased mortality. Eur. J. Endocrinol. 2014, 170, 667–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, S.C.; Agrawal, D.K. Vitamin D and Bronchial Asthma: An Overview of Data From the Past 5 Years. Clin. Ther. 2017, 39, 917–929. [Google Scholar] [CrossRef] [Green Version]
- Pelaia, G.; Cuda, G.; Vatrella, A.; Gallelli, L.; Fratto, D.; Gioffrè, V.; D’Agostino, B.; Caputi, M.; Maselli, R.; Rossi, F.; et al. Effects of hydrogen peroxide on MAPK activation, IL-8 production and cell viability in primary cultures of human bronchial epithelial cells. J. Cell. Biochem. 2004, 93, 142–152. [Google Scholar] [CrossRef]
- Han, H.; Chung, S.I.; Park, H.J.; Oh, E.Y.; Kim, S.R.; Park, K.H.; Lee, J.H.; Park, J.W. Obesity-induced Vitamin D Deficiency Contributes to Lung Fibrosis and Airway Hyperresponsiveness. Am. J. Respir. Cell Mol. Biol. 2021, 64, 357–367. [Google Scholar] [CrossRef]
- Hansdottir, S.; Monick, M.M. Vitamin D effects on lung immunity and respiratory diseases. Vitam. Horm. 2011, 86, 217–237. [Google Scholar] [CrossRef] [Green Version]
- Hoffer, L.J.; Robitaille, L.; Swinton, N.; Agulnik, J.; Cohen, V.; Small, D.; Pepe, C.; Eintracht, S. Appropriate vitamin D loading regimen for patients with advanced lung cancer. Nutr. J. 2016, 15, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelaia, G.; Vatrella, A.; Busceti, M.T.; Gallelli, L.; Calabrese, C.; Terracciano, R.; Maselli, R. Cellular mechanisms underlying eosinophilic and neutrophilic airway inflammation in asthma. Mediat. Inflamm. 2015, 2015, 879783. [Google Scholar] [CrossRef]
- Hoong, C.W.S.; Huilin, K.; Cho, S.; Aravamudan, V.M.; Lin, J.H.X. Are Adequate Vitamin D Levels Helpful in Fighting COVID-19? A Look at the Evidence. Horm. Metab. Res. Horm. Stoffwechs. Horm. Metab. 2020, 52, 775–783. [Google Scholar] [CrossRef]
- Iqbal, S.F.; Freishtat, R.J. Mechanism of action of vitamin D in the asthmatic lung. J. Investig. Med. Off. Publ. Am. Fed. Clin. Res. 2011, 59, 1200–1202. [Google Scholar] [CrossRef] [Green Version]
- Jain, S.K.; Parsanathan, R. Can Vitamin D and L-Cysteine Co-Supplementation Reduce 25(OH)-Vitamin D Deficiency and the Mortality Associated with COVID-19 in African Americans? J. Am. Coll. Nutr. 2020, 39, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Jakovac, H. COVID-19 and vitamin D-Is there a link and an opportunity for intervention? Am. J. Physiol. Endocrinol. Metab. 2020, 318, E589. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Greenberg, L.; Hooper, R.L.; Mathyssen, C.; Rafiq, R.; de Jongh, R.T.; Camargo, C.A.; Griffiths, C.J.; Janssens, W.; Martineau, A.R. Vitamin D to prevent exacerbations of COPD: Systematic review and meta-analysis of individual participant data from randomised controlled trials. Thorax 2019, 74, 337–345. [Google Scholar] [CrossRef] [Green Version]
- Kho, A.T.; Sharma, S.; Qiu, W.; Gaedigk, R.; Klanderman, B.; Niu, S.; Anderson, C.; Leeder, J.S.; Weiss, S.T.; Tantisira, K.G. Vitamin D related genes in lung development and asthma pathogenesis. BMC Med. Genom. 2013, 6, 47. [Google Scholar] [CrossRef] [Green Version]
- Worm, M.; Heine, G.; Radbruch, A. Immunomodulation by vitamin D. Allergol. Sel. 2018, 2, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Herr, C.; Greulich, T.; Koczulla, R.A.; Meyer, S.; Zakharkina, T.; Branscheidt, M.; Eschmann, R.; Bals, R. The role of vitamin D in pulmonary disease: COPD, asthma, infection, and cancer. Respir. Res. 2011, 12, 31. [Google Scholar] [CrossRef] [Green Version]
- Ford, E.S.; Mannino, D.M. Prospective association between lung function and the incidence of diabetes: Findings from the National Health and Nutrition Examination Survey Epidemiologic Follow-up Study. Diabetes Care 2004, 27, 2966–2970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloc, M.; Ghobrial, R.M.; Lipińska-Opałka, A.; Wawrzyniak, A.; Zdanowski, R.; Kalicki, B.; Kubiak, J.Z. Effects of vitamin D on macrophages and myeloid-derived suppressor cells (MDSCs) hyperinflammatory response in the lungs of COVID-19 patients. Cell. Immunol. 2021, 360, 104259. [Google Scholar] [CrossRef]
- Konstantinopoulou, S.; Tapia, I.E. Vitamin D and the lung. Paediatr. Respir. Rev. 2017, 24, 39–43. [Google Scholar] [CrossRef]
- Kose, M.; Bastug, O.; Sonmez, M.F.; Per, S.; Ozdemir, A.; Kaymak, E.; Yahşi, H.; Ozturk, M.A. Protective effect of vitamin D against hyperoxia-induced lung injury in newborn rats. Pediatr. Pulmonol. 2017, 52, 69–76. [Google Scholar] [CrossRef]
- Lee, J.; Park, H.K.; Kwon, M.J.; Ham, S.Y.; Lim, S.Y.; Song, J.U. Decreased lung function is associated with vitamin D deficiency in apparently health, middle aged Koreans: The Kangbuk Samsung Health Study. Eur. J. Clin. Nutr. 2021, 75, 501–512. [Google Scholar] [CrossRef]
- Litonjua, A.A.; Carey, V.J.; Laranjo, N.; Stubbs, B.J.; Mirzakhani, H.; O’Connor, G.T.; Sandel, M.; Beigelman, A.; Bacharier, L.B.; Zeiger, R.S.; et al. Six-Year Follow-up of a Trial of Antenatal Vitamin D for Asthma Reduction. N. Engl. J. Med. 2020, 382, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Loukou, I.; Boutopoulou, B.; Fouzas, S.; Douros, K. Vitamin D and Cystic Fibrosis Lung Disease. Mini Rev. Med. Chem. 2015, 15, 974–983. [Google Scholar] [CrossRef]
- Loukou, I.; Moustaki, M.; Sardeli, O.; Plyta, M.; Douros, K. Association of vitamin D status with lung function measurements in children and adolescents with cystic fibrosis. Pediatr. Pulmonol. 2020, 55, 1375–1380. [Google Scholar] [CrossRef] [PubMed]
- Lykkedegn, S.; Sorensen, G.L.; Beck-Nielsen, S.S.; Christesen, H.T. The impact of vitamin D on fetal and neonatal lung maturation. A systematic review. Am. J. Physiol. Lung Cell. Mol. Physiol. 2015, 308, L587–L602. [Google Scholar] [CrossRef] [PubMed]
- Mak, G.; Hanania, N.A. Vitamin D and asthma. Curr. Opin. Pulm. Med. 2011, 17, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Manavi, K.R.; Alston-Mills, B.P.; Thompson, M.P. History of tobacco, vitamin D and women. Int. J. Vitam. Nutr. Res. 2020, 90, 389–394. [Google Scholar] [CrossRef]
- Mandell, E.W.; Ryan, S.; Seedorf, G.J.; Gonzalez, T.; Smith, B.J.; Fleet, J.C.; Abman, S.H. Maternal Vitamin D Deficiency Causes Sustained Impairment of Lung Structure and Function and Increases Susceptibility to Hyperoxia-induced Lung Injury in Infant Rats. Am. J. Respir. Cell Mol. Biol. 2020, 63, 79–91. [Google Scholar] [CrossRef]
- Martín Giménez, V.M.; Inserra, F.; Tajer, C.D.; Mariani, J.; Ferder, L.; Reiter, R.J.; Manucha, W. Lungs as target of COVID-19 infection: Protective common molecular mechanisms of vitamin D and melatonin as a new potential synergistic treatment. Life Sci. 2020, 254, 117808. [Google Scholar] [CrossRef]
- Martineau, A.R.; Jolliffe, D.A.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; Goodall, E.C.; et al. Vitamin D supplementation to prevent acute respiratory infections: Individual participant data meta-analysis. Health Technol. Assess. 2019, 23, 1–44. [Google Scholar] [CrossRef]
- Mirzakhani, H.; Litonjua, A.A.; McElrath, T.F.; O’Connor, G.; Lee-Parritz, A.; Iverson, R.; Macones, G.; Strunk, R.C.; Bacharier, L.B.; Zeiger, R.; et al. Early pregnancy vitamin D status and risk of preeclampsia. J. Clin. Investig. 2016, 126, 4702–4715. [Google Scholar] [CrossRef] [Green Version]
- Mohan, M.; Cherian, J.J.; Sharma, A. Exploring links between vitamin D deficiency and COVID-19. PLoS Pathog. 2020, 16, e1008874. [Google Scholar] [CrossRef]
- Litonjua, A.A.; Carey, V.J.; Laranjo, N.; Harshfield, B.J.; McElrath, T.F.; O’Connor, G.T.; Sandel, M.; Iverson, R.E., Jr.; Lee-Paritz, A.; Strunk, R.C.; et al. Effect of Prenatal Supplementation With Vitamin D on Asthma or Recurrent Wheezing in Offspring by Age 3 Years: The VDAART Randomized Clinical Trial. JAMA 2016, 315, 362–370. [Google Scholar] [CrossRef]
- Forno, E.; Bacharier, L.B.; Phipatanakul, W.; Guilbert, T.W.; Cabana, M.D.; Ross, K.; Covar, R.; Gern, J.E.; Rosser, F.J.; Blatter, J.; et al. Effect of Vitamin D3 Supplementation on Severe Asthma Exacerbations in Children With Asthma and Low Vitamin D Levels: The VDKA Randomized Clinical Trial. JAMA 2020, 324, 752–760. [Google Scholar] [CrossRef] [PubMed]
- Win, S.S.; Camargo, C.A., Jr.; Khaw, K.T.; Lawes, C.M.M.; Sluyter, J.; Waayer, D.; Toop, L.; Scragg, R. Cross-sectional associations of vitamin D status with asthma prevalence, exacerbations, and control in New Zealand adults. J. Steroid Biochem. Mol. Biol. 2019, 188, 1–7. [Google Scholar] [CrossRef] [PubMed]
- McGlade, J.P.; Gorman, S.; Zosky, G.R.; Larcombe, A.N.; Sly, P.D.; Finlay-Jones, J.J.; Turner, D.J.; Hart, P.H. Suppression of the asthmatic phenotype by ultraviolet B-induced, antigen-specific regulatory cells. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2007, 37, 1267–1276. [Google Scholar] [CrossRef] [PubMed]
- Nikolac Gabaj, N.; Unic, A.; Miler, M.; Pavicic, T.; Culej, J.; Bolanca, I.; Herman Mahecic, D.; Milevoj Kopcinovic, L.; Vrtaric, A. In sickness and in health: Pivotal role of vitamin D. Biochem. Med. 2020, 30, 020501. [Google Scholar] [CrossRef] [PubMed]
- Norton, R.; O’Connell, M.A. Vitamin D: Potential in the prevention and treatment of lung cancer. Anticancer Res. 2012, 32, 211–221. [Google Scholar] [PubMed]
- Oliveira, M.S.; Matsunaga, N.Y.; Rodrigues, M.L.E.; Morcillo, A.M.; de Oliveira Ribeiro, M.A.G.; Ribeiro, A.F.; de Fátima, C.P.S.M.; Nogueira, R.J.N.; Pereira, M.C.; Ribeiro, J.D.; et al. Lung disease and vitamin D levels in cystic fibrosis infants and preschoolers. Pediatr. Pulmonol. 2019, 54, 563–574. [Google Scholar] [CrossRef]
- Ong, J.S.; Gharahkhani, P.; An, J.; Law, M.H.; Whiteman, D.C.; Neale, R.E.; MacGregor, S. Vitamin D and overall cancer risk and cancer mortality: A Mendelian randomization study. Hum. Mol. Genet. 2018, 27, 4315–4322. [Google Scholar] [CrossRef]
- Pfeffer, P.E.; Hawrylowicz, C.M. Vitamin D and lung disease. Thorax 2012, 67, 1018–1020. [Google Scholar] [CrossRef] [Green Version]
- Pincikova, T.; Paquin-Proulx, D.; Sandberg, J.K.; Flodström-Tullberg, M.; Hjelte, L. Vitamin D treatment modulates immune activation in cystic fibrosis. Clin. Exp. Immunol. 2017, 189, 359–371. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; He, J.; Yu, M.; Sun, J. The efficacy of vitamin D therapy for patients with COPD: A meta-analysis of randomized controlled trials. Ann. Palliat. Med. 2020, 9, 1219. [Google Scholar] [CrossRef] [PubMed]
- Rafiq, R.; Prins, H.J.; Boersma, W.G.; Daniels, J.M.; den Heijer, M.; Lips, P.; de Jongh, R.T. Effects of daily vitamin D supplementation on respiratory muscle strength and physical performance in vitamin D-deficient COPD patients: A pilot trial. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 2583–2592. [Google Scholar] [CrossRef] [Green Version]
- Panahi, Y.; Darvishi, B.; Jowzi, N.; Beiraghdar, F.; Sahebkar, A. Chlorella vulgaris: A Multifunctional Dietary Supplement with Diverse Medicinal Properties. Curr. Pharm. Des. 2016, 22, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Maretzke, F.; Bechthold, A.; Egert, S.; Ernst, J.B.; Melo van Lent, D.; Pilz, S.; Reichrath, J.; Stangl, G.I.; Stehle, P.; Volkert, D.; et al. Role of Vitamin D in Preventing and Treating Selected Extraskeletal Diseases—An Umbrella Review. Nutrients 2020, 12, 969. [Google Scholar] [CrossRef] [Green Version]
- Marzetti, E.; Calvani, R.; Cesari, M.; Buford, T.W.; Lorenzi, M.; Behnke, B.J.; Leeuwenburgh, C. Mitochondrial dysfunction and sarcopenia of aging: From signaling pathways to clinical trials. Int. J. Biochem. Cell Biol. 2013, 45, 2288–2301. [Google Scholar] [CrossRef] [Green Version]
- Ramnath, N.; Kim, S.; Christensen, P.J. Vitamin D and lung cancer. Expert Rev. Respir. Med. 2011, 5, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Rozmus, D.; Ciesielska, A.; Płomiński, J.; Grzybowski, R.; Fiedorowicz, E.; Kordulewska, N.; Savelkoul, H.; Kostyra, E.; Cieślińska, A. Vitamin D Binding Protein (VDBP) and Its Gene Polymorphisms—The Risk of Malignant Tumors and Other Diseases. Int. J. Mol. Sci. 2020, 21, 7822. [Google Scholar] [CrossRef] [PubMed]
- Schapochnik, A.; da Silva, M.R.; Leal, M.P.; Esteves, J.; Hebeda, C.B.; Sandri, S.; de Fátima Teixeira da Silva, D.; Farsky, S.H.; Marcos, R.L.; Lino-Dos-Santos-Franco, A. Vitamin D treatment abrogates the inflammatory response in paraquat-induced lung fibrosis. Toxicol. Appl. Pharmacol. 2018, 355, 60–67. [Google Scholar] [CrossRef]
- Schrumpf, J.A.; van der Does, A.M.; Hiemstra, P.S. Impact of the Local Inflammatory Environment on Mucosal Vitamin D Metabolism and Signaling in Chronic Inflammatory Lung Diseases. Front. Immunol. 2020, 11, 1433. [Google Scholar] [CrossRef]
- Schwalfenberg, G.K. A review of the critical role of vitamin D in the functioning of the immune system and the clinical implications of vitamin D deficiency. Mol. Nutr. Food Res. 2011, 55, 96–108. [Google Scholar] [CrossRef]
- Shojaeefar, E.; Malih, N.; Rezaei, N. The possible double-edged sword effects of vitamin D on COVID-19: A hypothesis. Cell Biol. Int. 2021, 45, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Soe, H.H.; Abas, A.B.; Than, N.N.; Ni, H.; Singh, J.; Said, A.R.; Osunkwo, I. Vitamin D supplementation for sickle cell disease. Cochrane Database Syst. Rev. 2020, 1, Cd010858. [Google Scholar] [CrossRef]
- Akiba, T.; Morikawa, T.; Odaka, M.; Nakada, T.; Kamiya, N.; Yamashita, M.; Yabe, M.; Inagaki, T.; Asano, H.; Mori, S.; et al. Vitamin D Supplementation and Survival of Patients with Non-small Cell Lung Cancer: A Randomized, Double-Blind, Placebo-Controlled Trial. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2018, 24, 4089–4097. [Google Scholar] [CrossRef] [Green Version]
- Greenwald, P.; Anderson, D.; Nelson, S.A.; Taylor, P.R. Clinical trials of vitamin and mineral supplements for cancer prevention. Am. J. Clin. Nutr. 2007, 85, 314s–317s. [Google Scholar] [CrossRef]
- Evans, J.R.; Lawrenson, J.G. Antioxidant vitamin and mineral supplements for preventing age-related macular degeneration. Cochrane Database Syst. Rev. 2017, 7, Cd000253. [Google Scholar] [CrossRef]
- Hoyt, M.; Reger, M.; Marley, A.; Fan, H.; Liu, Z.; Zhang, J. Vitamin K intake and prostate cancer risk in the Prostate, Lung, Colorectal, and Ovarian Cancer (PLCO) Screening Trial. Am. J. Clin. Nutr. 2019, 109, 392–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solidoro, P.; Bellocchia, M.; Facchini, F. The immunobiological and clinical role of vitamin D in obstructive lung diseases. Minerva Med. 2016, 107, 12–19. [Google Scholar]
- Sulli, A.; Gotelli, E.; Casabella, A.; Paolino, S.; Pizzorni, C.; Alessandri, E.; Grosso, M.; Ferone, D.; Smith, V.; Cutolo, M. Vitamin D and Lung Outcomes in Elderly COVID-19 Patients. Nutrients 2021, 13, 717. [Google Scholar] [CrossRef] [PubMed]
- Sundararaman, A.; Ray, M.; Ravindra, P.V.; Halami, P.M. Role of probiotics to combat viral infections with emphasis on COVID-19. Appl. Microbiol. Biotechnol. 2020, 104, 8089–8104. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, E.R.; Goleva, E.; Jackson, L.P.; Stevens, A.D.; Leung, D.Y. Vitamin D levels, lung function, and steroid response in adult asthma. Am. J. Respir. Crit. Care Med. 2010, 181, 699–704. [Google Scholar] [CrossRef] [Green Version]
- Tangpricha, V.; Lukemire, J.; Chen, Y.; Binongo, J.N.G.; Judd, S.E.; Michalski, E.S.; Lee, M.J.; Walker, S.; Ziegler, T.R.; Tirouvanziam, R.; et al. Vitamin D for the Immune System in Cystic Fibrosis (DISC): A double-blind, multicenter, randomized, placebo-controlled clinical trial. Am. J. Clin. Nutr. 2019, 109, 544–553. [Google Scholar] [CrossRef]
- Alvarez, J.A.; Chong, E.Y.; Walker, D.I.; Chandler, J.D.; Michalski, E.S.; Grossmann, R.E.; Uppal, K.; Li, S.; Frediani, J.K.; Tirouvanziam, R.; et al. Plasma metabolomics in adults with cystic fibrosis during a pulmonary exacerbation: A pilot randomized study of high-dose vitamin D(3) administration. Metab. Clin. Exp. 2017, 70, 31–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drent, M.; Wijnen, P.; Bast, A. Pharmacogenetic variants and vitamin K deficiency: A risk factor or trigger for fibrosing interstitial pneumonias? Curr. Opin. Pulm. Med. 2018, 24, 287–295. [Google Scholar] [CrossRef]
- Grossmann, R.E.; Zughaier, S.M.; Liu, S.; Lyles, R.H.; Tangpricha, V. Impact of vitamin D supplementation on markers of inflammation in adults with cystic fibrosis hospitalized for a pulmonary exacerbation. Eur. J. Clin. Nutr. 2012, 66, 1072–1074. [Google Scholar] [CrossRef] [Green Version]
- Todd, J.J.; Pourshahidi, L.K.; McSorley, E.M.; Madigan, S.M.; Magee, P.J. Vitamin D: Recent advances and implications for athletes. Sports Med. 2015, 45, 213–229. [Google Scholar] [CrossRef] [PubMed]
- Tzilas, V.; Bouros, E.; Barbayianni, I.; Karampitsakos, T.; Kourtidou, S.; Ntassiou, M.; Ninou, I.; Aidinis, V.; Bouros, D.; Tzouvelekis, A. Vitamin D prevents experimental lung fibrosis and predicts survival in patients with idiopathic pulmonary fibrosis. Pulm. Pharmacol. Ther. 2019, 55, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Verleden, S.E.; Vos, R.; Geenens, R.; Ruttens, D.; Vaneylen, A.; Dupont, L.J.; Verleden, G.M.; van Raemdonck, D.E.; Vanaudenaerde, B.M. Vitamin D deficiency in lung transplant patients: Is it important? Transplantation 2012, 93, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Tan, Z.X.; Fu, L.; Fan, Y.J.; Luo, B.; Zhang, Z.H.; Xu, S.; Chen, Y.H.; Zhao, H.; Xu, D.X. Gestational vitamin D deficiency impairs fetal lung development through suppressing type II pneumocyte differentiation. Reprod. Toxicol. 2020, 94, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Jing, H.; Wei, Q.; Wei, G.; Heng, Z. Associations of the risk of lung cancer with serum 25-hydroxyvitamin D level and dietary vitamin D intake: A dose-response PRISMA meta-analysis. Medicine 2018, 97, e12282. [Google Scholar] [CrossRef]
- Yao, L.; Shi, Y.; Zhao, X.; Hou, A.; Xing, Y.; Fu, J.; Xue, X. Vitamin D attenuates hyperoxia-induced lung injury through downregulation of Toll-like receptor 4. Int. J. Mol. Med. 2017, 39, 1403–1408. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Yang, J.; Chen, J.; Luo, Q.; Zhang, Q.; Zhang, H. Vitamin D alleviates lipopolysaccharide-induced acute lung injury via regulation of the renin-angiotensin system. Mol. Med. Rep. 2017, 16, 7432–7438. [Google Scholar] [CrossRef] [Green Version]
- Zdrenghea, M.T.; Makrinioti, H.; Bagacean, C.; Bush, A.; Johnston, S.L.; Stanciu, L.A. Vitamin D modulation of innate immune responses to respiratory viral infections. Rev. Med Virol. 2017, 27. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, S.; Che, X.; Li, X. Vitamin D and lung cancer risk: A comprehensive review and meta-analysis. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 2015, 36, 299–305. [Google Scholar] [CrossRef]
- Zheng, S.; Yang, J.; Hu, X.; Li, M.; Wang, Q.; Dancer, R.C.A.; Parekh, D.; Gao-Smith, F.; Thickett, D.R.; Jin, S. Vitamin D attenuates lung injury via stimulating epithelial repair, reducing epithelial cell apoptosis and inhibits TGF-β induced epithelial to mesenchymal transition. Biochem. Pharmacol. 2020, 177, 113955. [Google Scholar] [CrossRef]
- Zhu, M.; Wang, T.; Wang, C.; Ji, Y. The association between vitamin D and COPD risk, severity, and exacerbation: An updated systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2597–2607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, J.; Tinkov, A.; Strand, T.A.; Alehagen, U.; Skalny, A.; Aaseth, J. Early Nutritional Interventions with Zinc, Selenium and Vitamin D for Raising Anti-Viral Resistance Against Progressive COVID-19. Nutrients 2020, 12, 2358. [Google Scholar] [CrossRef]
- Gallelli, L.; Zhang, L.; Wang, T.; Fu, F. Severe Acute Lung Injury Related to COVID-19 Infection: A Review and the Possible Role for Escin. J. Clin. Pharmacol. 2020, 60, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Bae, M.; Kim, H. Mini-Review on the Roles of Vitamin C, Vitamin D, and Selenium in the Immune System against COVID-19. Molecules 2020, 25, 5346. [Google Scholar] [CrossRef] [PubMed]
- Bergman, P. The link between vitamin D and COVID-19: Distinguishing facts from fiction. J. Intern. Med. 2021, 289, 131–133. [Google Scholar] [CrossRef]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [Green Version]
- Mercola, J.; Grant, W.B.; Wagner, C.L. Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity. Nutrients 2020, 12, 3361. [Google Scholar] [CrossRef]
- Mitchell, F. Vitamin-D and COVID-19: Do deficient risk a poorer outcome? Lancet Diabetes Endocrinol. 2020, 8, 570. [Google Scholar] [CrossRef]
- Kumar, R.; Rathi, H.; Haq, A.; Wimalawansa, S.J.; Sharma, A. Putative roles of vitamin D in modulating immune response and immunopathology associated with COVID-19. Virus Res. 2021, 292, 198235. [Google Scholar] [CrossRef] [PubMed]
- Entrenas Castillo, M.; Entrenas Costa, L.M.; Vaquero Barrios, J.M.; Alcalá Díaz, J.F.; López Miranda, J.; Bouillon, R.; Quesada Gomez, J.M. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef]
- Jovic, T.H.; Ali, S.R.; Ibrahim, N.; Jessop, Z.M.; Tarassoli, S.P.; Dobbs, T.D.; Holford, P.; Thornton, C.A.; Whitaker, I.S. Could Vitamins Help in the Fight Against COVID-19? Nutrients 2020, 12, 2550. [Google Scholar] [CrossRef]
- Mudde, A.H.; van den Berg, H.; Boshuis, P.G.; Breedveld, F.C.; Markusse, H.M.; Kluin, P.M.; Bijvoet, O.L.; Papapoulos, S.E. Ectopic production of 1,25-dihydroxyvitamin D by B-cell lymphoma as a cause of hypercalcemia. Cancer 1987, 59, 1543–1546. [Google Scholar] [CrossRef]
- Dinour, D.; Davidovits, M.; Aviner, S.; Ganon, L.; Michael, L.; Modan-Moses, D.; Vered, I.; Bibi, H.; Frishberg, Y.; Holtzman, E.J. Maternal and infantile hypercalcemia caused by vitamin-D-hydroxylase mutations and vitamin D intake. Pediatr. Nephrol. 2015, 30, 145–152. [Google Scholar] [CrossRef]
- Jacobus, C.H.; Holick, M.F.; Shao, Q.; Chen, T.C.; Holm, I.A.; Kolodny, J.M.; Fuleihan, G.E.; Seely, E.W. Hypervitaminosis D associated with drinking milk. N. Engl. J. Med. 1992, 326, 1173–1177. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study Type | Study Design | Parameter Examined | Findings | Ref |
|---|---|---|---|---|
| Clinical Trial | At 3 US centers, Placebo controlled randomized double-blind trial in woman, Placebo (n = 436) v/s 4000 IU/d vitamin D (n = 447), administered parentally. | Through the age of three, parents reported having asthma or recurrent wheeze, according to a physician’s diagnosis; Level of calcitriol in pregnant woman 3rd trimester. | Supplementing with 4400 IU/d vitamin D vs. 400 IU/d vitamin D substantially enhanced vitamin D levels in pregnant mothers at risk of getting an asthmatic child. At age three, their children had a 6.1 percent declined asthma incidence and recurrent wheeze, although this did not reach statistical significance. | [60] |
| Placebo-controlled, randomized double-blind trial, Physician diagnosed children between ages 5–13 years with moderate to severe asthma, Vitamin D3 60,000 IU/month for v/s Placebo. | Asthma exacerbation | At 6 months, the D3 treated group had a significantly higher reduction in asthma severity as per GINA standards. | [61] | |
| Cross-sectional Studies | 5110 Physician diagnosed asthma patients of age between 50–84 years treated with vitamin D supplement. | Asthma exacerbation. | Asthmatic individuals with vitamin d Deficiency are more inclined to seek emergency medical attention for their asthma and have poor asthma management. | [62] |
| Preclinical Studies | BALB/c mice | Measurement of in vivo AHR; cytokine production and proliferative reactions to OVA;inflammatory cells. | Suppresses AHR and airway cellular response; Reduces the severity of asthma by reducing mediator release. | [63] |
| Sprague–Dawley rats; Vitamin D 100 ng/mL | Airway remodeling; Asthma exacerbation. | Vitamin D treatment reduced airway remodeling in asthma patients by inhibiting the Wnt/β-catenin signaling pathway. | [57] |
| Study Type | Study Design | Parameter Examined | Findings | Ref |
|---|---|---|---|---|
| Clinical Studies | Multi-center, randomized, double-blind, placebo-controlled intervention trial, age > 40 years, 16,800 IU vitamin D3 (n = 120) v/s placebo (n = 120) weekly and orally. | COPD exacerbation, Total lung capacity, and maximum respiratory mouth pressure. | [72] | |
| Randomized clinical study with a double-blind placebo control, 88 severe COPD patients, placebo receive 100,000 IU vitamin D monthly for six months. | FEV1, COPD exacerbation. | Improved FEV1, Reduces COPD exacerbation. | [40] | |
| Controlled, randomized, double-blind trial, 50–58 year patents, 200,000 IU followed by 100,000 IU vitamin D monthly for 1.1 years (n = 226) v/s placebo (n = 216). | FEV1, COPD exacerbation. | Only smokers benefitted from vitamin D supplementation, particularly those with vitamin D insufficiency or COPD. | [73] | |
| Multi-center, randomized, double-blind, placebo-controlled intervention trial, Vitamin D3 (n = 122) v/s Placebo (n = 118) | COPD exacerbation. | Vitamin D3 supplementation reduced the severity of COPD exacerbations in those with mild to severe COPD. | [74] |
| Study Type | Study Design | Parameter Examined | Findings | Ref |
|---|---|---|---|---|
| Clinical Studies | Double-blind, randomized trial, Vitamin D 1200 IU/d (n = 77) v/s placebo (n = 78) | Overall survival and relapse-free survival. | Patients with early-stage lung adenocarcinoma may benefit from vitamin D therapy. | [82] |
| Preclinical Studies | A/J Mouse model, Vitamin D3 (2.5 or 5 microgram/Kg diet) | Tumor incidence and tumor cell differentiation. | Reduces incidence of the tumor as well as having combating potential against lung carcinogenesis. | [83] |
| Mouse model of N-nitroso-tris-chloroethyl urea; Vitamin D3 2000 IU/Kg. | The premalignant tumors progressing of Carcinoma | Reduces proliferation, development of premalignant lesion, swelling of squamous cell carcinoma of the lung. | [84] | |
| In vitro studies | NCI-H1975 and A549 tumor cells | Metastasis, tumor cell apoptosis. | The tumor cell growth, infiltration, and metastasis are inhibited, while tumor cell apoptosis is promoted. | [85] |
| Study Type | Study Design | Parameter Examined | Findings | Ref |
|---|---|---|---|---|
| Clinical Studies | Randomized open-labeled intervention, 16 Cystic fibrosis patients receive Vitamin D3 35,000 IU/week for age < 16 years or 50,000 IU/week for age > 16 years for 3 months | T cell activation, myeloid dendritic cells. | In people with CF, vitamin D has a wide range of immunomodulatory effects | [91] |
| Multicenter, randomized, double-blind, placebo-controlled intervention trial, 23 CF patients chronically affected withP. aeruginosa receive 1000 IU/d for 3 months v/s Placebo orally. | Quantification of IL-17A and IL-23. | Vitamin D had an anti-inflammatory impact, lowering the levels of IL-17A and IL-23 in CF patients’ airways. Vitamin D supplementation is recommended for CF patients. | [17] | |
| Preclinical Studies | C57/BL6 male mice, Vitamin D I.P. daily at a dose of 5 μg/kg. | Leucocyte count, estimation of inflammatory mediators. | Vitamin D decreases leucocyte count; reduces the level of MMP-9, TGF-β IL-17, and IL-6; beneficial effect in PF treatment | [19] |
| C57/BL6 mice treated with bleomycin, Vitamin D 1 μg/kg/day between 3rd day–13th days. | Level of hydroxyproline, Masson Trichrome staining and level of mRNA α-SMA, col3a1 and col1a1. | Up-regulation of mRNA of VDR level, Vitamin D hasthe potential of combating IPF. | [92] | |
| In vitro Studies | Human myofibroblasts, Alveolar epithelial cells type II | DNA damaging | In the vicinity of a DNA damaging chemical in PF, vitamin D had an unexpectedly negative effect. | [93] |
| Study Type | Study Design | Parameter Examined | Findings | Ref |
|---|---|---|---|---|
| Clinical Trials | Multi center, open-label, randomized controlled trial, Vitamin D 50,000 IU daily orally to 260 COVID19 Patients of age ≥ 65 years. | All Causes of mortality. | Vitamin D supplementation at high doses might be an efficient, well-tolerated, and quickly available therapy for COVID-19. | [112] |
| Household cluster-randomized with a planned pragmatic, double-blinded trial, 2700 subjects 1:1 ratio vitamin D 3200 IU/d v/s Placebo. | The likelihood of hospitalization and/or fatality among newly diagnosed people. | Lowering hospitalization and/or death rates in recently diagnosed patients, as well as avoiding infection within their intimate infected persons | [113] | |
| Open-label randomized parallel pilot, double-blinded trial, 76 COVID-19 hospitalized patients. | ICU admissions and fatalities rate | The use of calcifediol has been shown to minimize the requirement for ICU care in individuals who require hospitalization. COVID-19 | [109] | |
| Randomized Multicenter clinical trials, 69 COVID-19-positive patients, 5000 IU/d (n = 36); 1000 IU/d (n = 33) for two weeks orally. | Gustatory sensory loss and cough recovery | The time it takes for patients to recover from gustatory sensory loss and cough is reduced by taking 5000 IU of vitamin D3 daily for two weeks. | [114] | |
| 65 hospitalized COVID-19 positive patients of age between 63–89 years. | Commodities, Type of respiratory involvement, laboratory parameters (vitamin, C-reactive protein, D, D-dimer), Pulmonary parameters (PaO2/FiO2, PaCO2, PaO2, and SO2) | Vitamin D insufficiency is linked to more serious respiratory involvement, a lengthier illness period, and a higher chance of mortality. | [112] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Afzal, M.; Kazmi, I.; Al-Abbasi, F.A.; Alshehri, S.; Ghoneim, M.M.; Imam, S.S.; Nadeem, M.S.; Al-Zahrani, M.H.; Alzarea, S.I.; Alquraini, A. Current Overview on Therapeutic Potential of Vitamin D in Inflammatory Lung Diseases. Biomedicines 2021, 9, 1843. https://doi.org/10.3390/biomedicines9121843
Afzal M, Kazmi I, Al-Abbasi FA, Alshehri S, Ghoneim MM, Imam SS, Nadeem MS, Al-Zahrani MH, Alzarea SI, Alquraini A. Current Overview on Therapeutic Potential of Vitamin D in Inflammatory Lung Diseases. Biomedicines. 2021; 9(12):1843. https://doi.org/10.3390/biomedicines9121843
Chicago/Turabian StyleAfzal, Muhammad, Imran Kazmi, Fahad A. Al-Abbasi, Sultan Alshehri, Mohammed M. Ghoneim, Syed Sarim Imam, Muhammad Shahid Nadeem, Maryam Hassan Al-Zahrani, Sami I. Alzarea, and Ali Alquraini. 2021. "Current Overview on Therapeutic Potential of Vitamin D in Inflammatory Lung Diseases" Biomedicines 9, no. 12: 1843. https://doi.org/10.3390/biomedicines9121843