
Microbiome Modulation as a Therapeutic Approach in Chronic Skin Diseases

 ,
,
Abstract
:1. Introduction
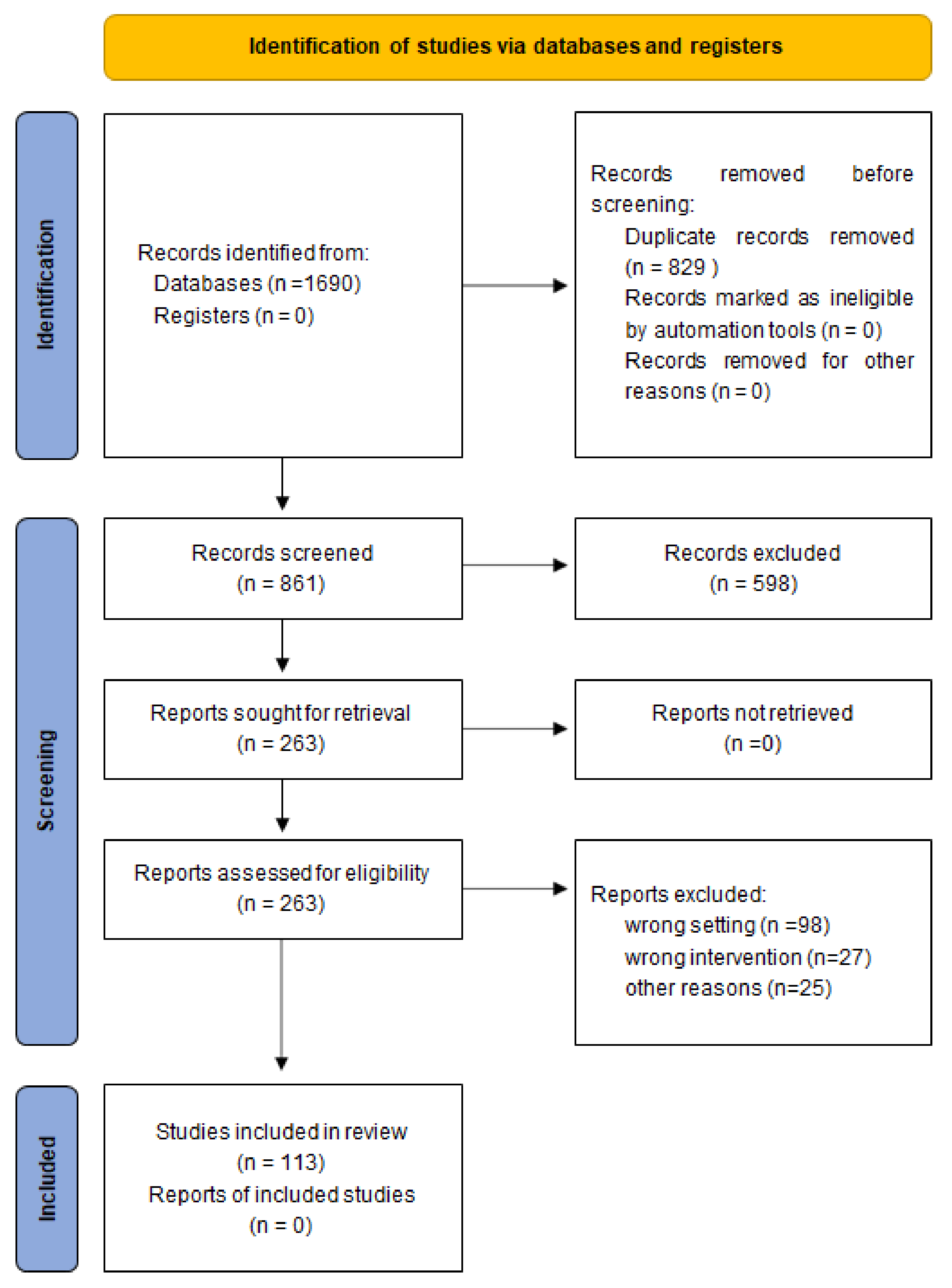
2. Materials and Methods
3. Results
4. Discussion
4.1. Atopic Dermatitis
4.2. Psoriasis
4.3. Chronic Ulcers
4.4. Seborrheic Dermatitis
4.5. Burns
4.6. Acne
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Pillsbury, D.M.; Shelley, W.B. Dermatology. Annu. Rev. Med. 1954, 5, 363–388. [Google Scholar] [CrossRef]
- Hooper, L.V.; Gordon, J.I. Commensal host-bacterial relationships in the gut. Science 2001, 292, 1115–1118. [Google Scholar] [CrossRef]
- Patra, V.; Byrne, S.N.; Wolf, P. The Skin Microbiome: Is It Affected by UV-induced Immune Suppression? Front. Microbiol. 2016, 7, 1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrd, A.L.; Belkaid, Y.; Segre, J.A. The human skin microbiome. Nat. Rev. Microbiol. 2018, 16, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Skowron, K.; Bauza-Kaszewska, J.; Kraszewska, Z.; Wiktorczyk-Kapischke, N.; Grudlewska-Buda, K.; Kwiecinska-Pirog, J.; Walecka-Zacharska, E.; Radtke, L.; Gospodarek-Komkowska, E. Human Skin Microbiome: Impact of Intrinsic and Extrinsic Factors on Skin Microbiota. Microorganisms 2021, 9, 543. [Google Scholar] [CrossRef]
- Mueller, N.T.; Bakacs, E.; Combellick, J.; Grigoryan, Z.; Dominguez-Bello, M.G. The infant microbiome development: Mom matters. Trends Mol. Med. 2015, 21, 109–117. [Google Scholar] [CrossRef] [Green Version]
- Dominguez-Bello, M.G.; Costello, E.K.; Contreras, M.; Magris, M.; Hidalgo, G.; Fierer, N.; Knight, R. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc. Natl. Acad. Sci. USA 2010, 107, 11971–11975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grice, E.A.; Kong, H.H.; Conlan, S.; Deming, C.B.; Davis, J.; Young, A.C.; Program, N.C.S.; Bouffard, G.G.; Blakesley, R.W.; Murray, P.R.; et al. Topographical and temporal diversity of the human skin microbiome. Science 2009, 324, 1190–1192. [Google Scholar] [CrossRef] [Green Version]
- Oh, J.; Byrd, A.L.; Park, M.; Program, N.C.S.; Kong, H.H.; Segre, J.A. Temporal Stability of the Human Skin Microbiome. Cell 2016, 165, 854–866. [Google Scholar] [CrossRef] [Green Version]
- Buerger, S. The Skin and Oral Microbiome: An Examination of Overlap and Potential Interactions between Microbiome Communities. In Skin Microbiome Handbook: From Basic Research to Product Development; Scrivener Publishing LLC: Beverly, MA, USA, 2020. [Google Scholar]
- Findley, K.; Oh, J.; Yang, J.; Conlan, S.; Deming, C.; Meyer, J.A.; Schoenfeld, D.; Nomicos, E.; Park, M.; NIH Intramural Sequencing Center Comparative Sequencing Program; et al. Topographic diversity of fungal and bacterial communities in human skin. Nature 2013, 498, 367–370. [Google Scholar] [CrossRef]
- Verbanic, S.; Kim, C.Y.; Deacon, J.M.; Chen, I.A. Improved single-swab sample preparation for recovering bacterial and phage DNA from human skin and wound microbiomes. BMC Microbiol. 2019, 19, 214. [Google Scholar] [CrossRef] [Green Version]
- Weyrich, L.S.; Dixit, S.; Farrer, A.G.; Cooper, A.J.; Cooper, A.J. The skin microbiome: Associations between altered microbial communities and disease. Australas. J. Dermatol. 2015, 56, 268–274. [Google Scholar] [CrossRef]
- Polak, K.; Bergler-Czop, B.; Szczepanek, M.; Wojciechowska, K.; Fratczak, A.; Kiss, N. Psoriasis and Gut Microbiome-Current State of Art. Int. J. Mol. Sci. 2021, 22, 4529. [Google Scholar] [CrossRef]
- Arumugam, M.; Raes, J.; Pelletier, E.; Le Paslier, D.; Yamada, T.; Mende, D.R.; Fernandes, G.R.; Tap, J.; Bruls, T.; Batto, J.M.; et al. Enterotypes of the human gut microbiome. Nature 2011, 473, 174–180. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, J.G.; Milani, C.; de Giori, G.S.; Sesma, F.; van Sinderen, D.; Ventura, M. Bacteria as vitamin suppliers to their host: A gut microbiota perspective. Curr. Opin. Biotechnol. 2013, 24, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Bosman, E.S.; Albert, A.Y.; Lui, H.; Dutz, J.P.; Vallance, B.A. Skin Exposure to Narrow Band Ultraviolet (UVB) Light Modulates the Human Intestinal Microbiome. Front. Microbiol. 2019, 10, 2410. [Google Scholar] [CrossRef]
- Zhao, Y.; Zeng, Y.; Zeng, D.; Wang, H.; Zhou, M.; Sun, N.; Xin, J.; Khalique, A.; Rajput, D.S.; Pan, K.; et al. Probiotics and MicroRNA: Their Roles in the Host-Microbe Interactions. Front. Microbiol. 2020, 11, 604462. [Google Scholar] [CrossRef] [PubMed]
- Mu, C.; Zhu, W. Antibiotic effects on gut microbiota, metabolism, and beyond. Appl. Microbiol. Biotechnol. 2019, 103, 9277–9285. [Google Scholar] [CrossRef]
- O’Sullivan, J.N.; Rea, M.C.; Hill, C.; Ross, R.P. Protecting the outside: Biological tools to manipulate the skin microbiota. FEMS Microbiol. Ecol. 2020, 96. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, C.F.A.; Silveira, G.; Candido, E.S.; Cardoso, M.H.; Espinola Carvalho, C.M.; Franco, O.L. Effects of Antibiotic Treatment on Gut Microbiota and How to Overcome Its Negative Impacts on Human Health. ACS Infect. Dis. 2020, 6, 2544–2559. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.J.; Langdon, A.E.; Dantas, G. Understanding the impact of antibiotic perturbation on the human microbiome. Genome Med. 2020, 12, 82. [Google Scholar] [CrossRef] [PubMed]
- Frei, R.; Akdis, M.; O’Mahony, L. Prebiotics, probiotics, synbiotics, and the immune system: Experimental data and clinical evidence. Curr. Opin. Gastroenterol. 2015, 31, 153–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapat, L.; Chemin, K.; Dubois, B.; Bourdet-Sicard, R.; Kaiserlian, D. Lactobacillus casei reduces CD8+ T cell-mediated skin inflammation. Eur. J. Immunol. 2004, 34, 2520–2528. [Google Scholar] [CrossRef]
- Kalliomaki, M.; Salminen, S.; Poussa, T.; Isolauri, E. Probiotics during the first 7 years of life: A cumulative risk reduction of eczema in a randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 2007, 119, 1019–1021. [Google Scholar] [CrossRef] [PubMed]
- Rautava, S.; Arvilommi, H.; Isolauri, E. Specific probiotics in enhancing maturation of IgA responses in formula-fed infants. Pediatr. Res. 2006, 60, 221–224. [Google Scholar] [CrossRef]
- Abrahamsson, T.R.; Jakobsson, T.; Bottcher, M.F.; Fredrikson, M.; Jenmalm, M.C.; Bjorksten, B.; Oldaeus, G. Probiotics in prevention of IgE-associated eczema: A double-blind, randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 2007, 119, 1174–1180. [Google Scholar] [CrossRef]
- Taylor, A.L.; Dunstan, J.A.; Prescott, S.L. Probiotic supplementation for the first 6 months of life fails to reduce the risk of atopic dermatitis and increases the risk of allergen sensitization in high-risk children: A randomized controlled trial. J. Allergy Clin. Immunol. 2007, 119, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Wickens, K.; Black, P.N.; Stanley, T.V.; Mitchell, E.; Fitzharris, P.; Tannock, G.W.; Purdie, G.; Crane, J.; Probiotic Study, G. A differential effect of 2 probiotics in the prevention of eczema and atopy: A double-blind, randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 2008, 122, 788–794. [Google Scholar] [CrossRef]
- Huurre, A.; Laitinen, K.; Rautava, S.; Korkeamaki, M.; Isolauri, E. Impact of maternal atopy and probiotic supplementation during pregnancy on infant sensitization: A double-blind placebo-controlled study. Clin. Exp. Allergy 2008, 38, 1342–1348. [Google Scholar] [CrossRef]
- Kopp, M.V.; Hennemuth, I.; Heinzmann, A.; Urbanek, R. Randomized, double-blind, placebo-controlled trial of probiotics for primary prevention: No clinical effects of Lactobacillus GG supplementation. Pediatrics 2008, 121, e850–e856. [Google Scholar] [CrossRef]
- West, C.E.; Hammarstrom, M.L.; Hernell, O. Probiotics during weaning reduce the incidence of eczema. Pediatr. Allergy Immunol. 2009, 20, 430–437. [Google Scholar] [CrossRef]
- Niers, L.; Martin, R.; Rijkers, G.; Sengers, F.; Timmerman, H.; van Uden, N.; Smidt, H.; Kimpen, J.; Hoekstra, M. The effects of selected probiotic strains on the development of eczema (the PandA study). Allergy 2009, 64, 1349–1358. [Google Scholar] [CrossRef] [PubMed]
- Soh, S.E.; Aw, M.; Gerez, I.; Chong, Y.S.; Rauff, M.; Ng, Y.P.; Wong, H.B.; Pai, N.; Lee, B.W.; Shek, L.P. Probiotic supplementation in the first 6 months of life in at risk Asian infants--effects on eczema and atopic sensitization at the age of 1 year. Clin. Exp. Allergy 2009, 39, 571–578. [Google Scholar] [CrossRef]
- Kim, J.; Ko, Y.; Park, Y.K.; Kim, N.I.; Ha, W.K.; Cho, Y. Dietary effect of lactoferrin-enriched fermented milk on skin surface lipid and clinical improvement of acne vulgaris. Nutrition 2010, 26, 902–909. [Google Scholar] [CrossRef] [PubMed]
- Dotterud, C.K.; Storro, O.; Johnsen, R.; Oien, T. Probiotics in pregnant women to prevent allergic disease: A randomized, double-blind trial. Br. J. Dermatol. 2010, 163, 616–623. [Google Scholar] [CrossRef]
- Boyle, R.J.; Ismail, I.H.; Kivivuori, S.; Licciardi, P.V.; Robins-Browne, R.M.; Mah, L.J.; Axelrad, C.; Moore, S.; Donath, S.; Carlin, J.B.; et al. Lactobacillus GG treatment during pregnancy for the prevention of eczema: A randomized controlled trial. Allergy 2011, 66, 509–516. [Google Scholar] [CrossRef]
- Rautava, S.; Kainonen, E.; Salminen, S.; Isolauri, E. Maternal probiotic supplementation during pregnancy and breast-feeding reduces the risk of eczema in the infant. J. Allergy Clin. Immunol. 2012, 130, 1355–1360. [Google Scholar] [CrossRef]
- Ou, C.Y.; Kuo, H.C.; Wang, L.; Hsu, T.Y.; Chuang, H.; Liu, C.A.; Chang, J.C.; Yu, H.R.; Yang, K.D. Prenatal and postnatal probiotics reduces maternal but not childhood allergic diseases: A randomized, double-blind, placebo-controlled trial. Clin. Exp. Allergy 2012, 42, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.; Gerhold, K.; Zimmermann, K.; Ockeloen, C.W.; Rossberg, S.; Wagner, P.; Sulser, C.; Bunikowski, R.; Witt, I.; Wauer, J.; et al. Oral application of bacterial lysate in infancy decreases the risk of atopic dermatitis in children with 1 atopic parent in a randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 2012, 129, 1040–1047. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.J.; Jordan, S.; Storey, M.; Thornton, C.A.; Gravenor, M.B.; Garaiova, I.; Plummer, S.F.; Wang, D.; Morgan, G. Probiotics in the prevention of eczema: A randomised controlled trial. Arch. Dis. Child. 2014, 99, 1014–1019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabana, M.D.; McKean, M.; Caughey, A.B.; Fong, L.; Lynch, S.; Wong, A.; Leong, R.; Boushey, H.A.; Hilton, J.F. Early Probiotic Supplementation for Eczema and Asthma Prevention: A Randomized Controlled Trial. Pediatrics 2017, 140. [Google Scholar] [CrossRef] [Green Version]
- Wickens, K.; Barthow, C.; Mitchell, E.A.; Kang, J.; van Zyl, N.; Purdie, G.; Stanley, T.; Fitzharris, P.; Murphy, R.; Crane, J. Effects of Lactobacillus rhamnosus HN001 in early life on the cumulative prevalence of allergic disease to 11 years. Pediatr. Allergy Immunol. 2018, 29, 808–814. [Google Scholar] [CrossRef] [PubMed]
- Plummer, E.L.; Chebar Lozinsky, A.; Tobin, J.M.; Uebergang, J.B.; Axelrad, C.; Garland, S.M.; Jacobs, S.E.; Tang, M.L.K. Postnatal probiotics and allergic disease in very preterm infants: Sub-study to the ProPrems randomized trial. Allergy 2020, 75, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.M.; Pilmann Laursen, R.; Bruun, S.; Larnkjaer, A.; Molgaard, C.; Michaelsen, K.F.; Host, A. Probiotics in late infancy reduce the incidence of eczema: A randomized controlled trial. Pediatr. Allergy Immunol. 2019, 30, 335–340. [Google Scholar] [CrossRef]
- Moro, G.; Arslanoglu, S.; Stahl, B.; Jelinek, J.; Wahn, U.; Boehm, G. A mixture of prebiotic oligosaccharides reduces the incidence of atopic dermatitis during the first six months of age. Arch. Dis. Child. 2006, 91, 814–819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziegler, E.; Vanderhoof, J.A.; Petschow, B.; Mitmesser, S.H.; Stolz, S.I.; Harris, C.L.; Berseth, C.L. Term infants fed formula supplemented with selected blends of prebiotics grow normally and have soft stools similar to those reported for breast-fed infants. J. Pediatr. Gastroenterol. Nutr. 2007, 44, 359–364. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Moro, G.E.; Schmitt, J.; Tandoi, L.; Rizzardi, S.; Boehm, G. Early dietary intervention with a mixture of prebiotic oligosaccharides reduces the incidence of allergic manifestations and infections during the first two years of life. J. Nutr. 2008, 138, 1091–1095. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Moro, G.E.; Boehm, G.; Wienz, F.; Stahl, B.; Bertino, E. Early neutral prebiotic oligosaccharide supplementation reduces the incidence of some allergic manifestations in the first 5 years of life. J. Biol. Regul. Homeost. Agents 2012, 26, 49–59. [Google Scholar] [PubMed]
- Grüber, C.; van Stuijvenberg, M.; Mosca, F.; Moro, G.; Chirico, G.; Braegger, C.P.; Riedler, J.; Boehm, G.; Wahn, U. Reduced occurrence of early atopic dermatitis because of immunoactive prebiotics among low-atopy-risk infants. J. Allergy Clin. Immunol. 2010, 126, 791–797. [Google Scholar] [CrossRef]
- Grüber, C.; van Stuivenberg, M.; Mosca, F.; Moro, G.; Chirico, G.; Braegger, C.P.; Riedler, J.; Yavuz, Y.; Boehm, G.; Wahn, U. Immunoactive prebiotics transiently prevent occurrence of early atopic dermatitis among low-atopy-risk infants. J. Allergy Clin. Immunol. 2015, 136, 1696–1698.e1691. [Google Scholar] [CrossRef] [PubMed]
- Niele, N.; van Zwol, A.; Westerbeek, E.A.; Lafeber, H.N.; van Elburg, R.M. Effect of non-human neutral and acidic oligosaccharides on allergic and infectious diseases in preterm infants. Eur. J. Pediatr. 2013, 172, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Pontes, M.V.; Ribeiro, T.C.; Ribeiro, H.; de Mattos, A.P.; Almeida, I.R.; Leal, V.M.; Cabral, G.N.; Stolz, S.; Zhuang, W.; Scalabrin, D.M. Cow’s milk-based beverage consumption in 1- to 4-year-olds and allergic manifestations: An RCT. Nutr. J. 2016, 15, 19. [Google Scholar] [CrossRef] [Green Version]
- Boyle, R.J.; Tang, M.L.; Chiang, W.C.; Chua, M.C.; Ismail, I.; Nauta, A.; Hourihane, J.O.B.; Smith, P.; Gold, M.; Ziegler, J.; et al. Prebiotic-supplemented partially hydrolysed cow’s milk formula for the prevention of eczema in high-risk infants: A randomized controlled trial. Allergy 2016, 71, 701–710. [Google Scholar] [CrossRef] [Green Version]
- Ranucci, G.; Buccigrossi, V.; Borgia, E.; Piacentini, D.; Visentin, F.; Cantarutti, L.; Baiardi, P.; Felisi, M.; Spagnuolo, M.I.; Zanconato, S.; et al. Galacto-Oligosaccharide/Polidextrose Enriched Formula Protects against Respiratory Infections in Infants at High Risk of Atopy: A Randomized Clinical Trial. Nutrients 2018, 10, 286. [Google Scholar] [CrossRef] [Green Version]
- Wopereis, H.; Sim, K.; Shaw, A.; Warner, J.O.; Knol, J.; Kroll, J.S. Intestinal microbiota in infants at high risk for allergy: Effects of prebiotics and role in eczema development. J. Allergy Clin. Immunol. 2018, 141, 1334–1342.e1335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majamaa, H.; Isolauri, E. Probiotics: A novel approach in the management of food allergy. J. Allergy Clin. Immunol. 1997, 99, 179–185. [Google Scholar] [CrossRef]
- Isolauri, E.; Arvola, T.; Sütas, Y.; Moilanen, E.; Salminen, S. Probiotics in the management of atopic eczema. Clin. Exp. Allergy 2000, 30, 1604–1610. [Google Scholar] [CrossRef] [Green Version]
- Kirjavainen, P.V.; Salminen, S.J.; Isolauri, E. Probiotic bacteria in the management of atopic disease: Underscoring the importance of viability. J. Pediatr. Gastroenterol. Nutr. 2003, 36, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Viljanen, M.; Savilahti, E.; Haahtela, T.; Juntunen-Backman, K.; Korpela, R.; Poussa, T.; Tuure, T.; Kuitunen, M. Probiotics in the treatment of atopic eczema/dermatitis syndrome in infants: A double-blind placebo-controlled trial. Allergy 2005, 60, 494–500. [Google Scholar] [CrossRef]
- Weston, S.; Halbert, A.; Richmond, P.; Prescott, S.L. Effects of probiotics on atopic dermatitis: A randomised controlled trial. Arch. Dis. Child. 2005, 90, 892–897. [Google Scholar] [CrossRef]
- Taniuchi, S.; Hattori, K.; Yamamoto, A.; Sasai, M.; Hatano, Y.; Kojima, T.; Kobayashi, Y.; Iwamoto, H.; Yaeshima, T. Administration of Bifidobacterium to Infants with Atopic Dermatitis: Changes in Fecal Microflora and Clinical Symptoms. J. Appl. Res. 2005, 5, 2. [Google Scholar]
- Fölster-Holst, R.; Müller, F.; Schnopp, N.; Abeck, D.; Kreiselmaier, I.; Lenz, T.; von Rüden, U.; Schrezenmeir, J.; Christophers, E.; Weichenthal, M. Prospective, randomized controlled trial on Lactobacillus rhamnosus in infants with moderate to severe atopic dermatitis. Br. J. Dermatol. 2006, 155, 1256–1261. [Google Scholar] [CrossRef]
- Brouwer, M.L.; Wolt-Plompen, S.A.; Dubois, A.E.; van der Heide, S.; Jansen, D.F.; Hoijer, M.A.; Kauffman, H.F.; Duiverman, E.J. No effects of probiotics on atopic dermatitis in infancy: A randomized placebo-controlled trial. Clin. Exp. Allergy 2006, 36, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Grüber, C.; Wendt, M.; Sulser, C.; Lau, S.; Kulig, M.; Wahn, U.; Werfel, T.; Niggemann, B. Randomized, placebo-controlled trial of Lactobacillus rhamnosus GG as treatment of atopic dermatitis in infancy. Allergy 2007, 62, 1270–1276. [Google Scholar] [CrossRef]
- Flinterman, A.E.; Knol, E.F.; van Ieperen-van Dijk, A.G.; Timmerman, H.M.; Knulst, A.C.; Bruijnzeel-Koomen, C.A.; Pasmans, S.G.; van Hoffen, E. Probiotics have a different immunomodulatory potential in vitro versus ex vivo upon oral administration in children with food allergy. Int. Arch. Allergy Immunol. 2007, 143, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Van der Aa, L.B.; Heymans, H.S.; van Aalderen, W.M.; Sillevis Smitt, J.H.; Knol, J.; Ben Amor, K.; Goossens, D.A.; Sprikkelman, A.B. Effect of a new synbiotic mixture on atopic dermatitis in infants: A randomized-controlled trial. Clin. Exp. Allergy 2010, 40, 795–804. [Google Scholar] [CrossRef]
- Gøbel, R.; Larsen, N.; Mølgaard, C.; Jakobsen, M.; Michaelsen, K. Probiotics to young children with atopic dermatitis: A randomized placebo-controlled trial. Int. J. Probiotics Prebiotics 2010, 5, 53–59. [Google Scholar]
- Nermes, M.; Kantele, J.M.; Atosuo, T.J.; Salminen, S.; Isolauri, E. Interaction of orally administered Lactobacillus rhamnosus GG with skin and gut microbiota and humoral immunity in infants with atopic dermatitis. Clin. Exp. Allergy 2011, 41, 370–377. [Google Scholar] [CrossRef]
- Farid, R.; Ahanchian, H.; Jabbari, F.; Moghiman, T. Effect of a new synbiotic mixture on atopic dermatitis in children: A randomized-controlled trial. Iran. J. Pediatr. 2011, 21, 225–230. [Google Scholar]
- Gore, C.; Custovic, A.; Tannock, G.W.; Munro, K.; Kerry, G.; Johnson, K.; Peterson, C.; Morris, J.; Chaloner, C.; Murray, C.S.; et al. Treatment and secondary prevention effects of the probiotics Lactobacillus paracasei or Bifidobacterium lactis on early infant eczema: Randomized controlled trial with follow-up until age 3 years. Clin. Exp. Allergy 2012, 42, 112–122. [Google Scholar] [CrossRef]
- Shafiei, A.; Moin, M.; Pourpak, Z.; Gharagozlou, M.; Aghamohammadi, A.; Sajedi, V.; Sotoodeh, S.; Movahedi, M. Synbiotics could not reduce the scoring of childhood atopic dermatitis (SCORAD): A randomized double blind placebo-controlled trial. Iran. J. Allergy Asthma Immunol. 2011, 10, 21–28. [Google Scholar] [PubMed]
- Ivakhnenko, O.; Niankovskyy, S. Clinical effectiveness of probiotics in complex treatment of infants with cow’s milk allergy. Georgian Med. News 2013, 216, 39–45. [Google Scholar]
- Lin, R.J.; Qiu, L.H.; Guan, R.Z.; Hu, S.J.; Liu, Y.Y.; Wang, G.J. Protective effect of probiotics in the treatment of infantile eczema. Exp. Ther Med. 2015, 9, 1593–1596. [Google Scholar] [CrossRef]
- Yan-hu, G. Clinical effect of microecologics as an adjuvant therapy on infants’ eczema. J. Dalian Med Univ. 2015, 6, 571–573. [Google Scholar]
- Wu, Y.J.; Wu, W.F.; Hung, C.W.; Ku, M.S.; Liao, P.F.; Sun, H.L.; Lu, K.H.; Sheu, J.N.; Lue, K.H. Evaluation of efficacy and safety of Lactobacillus rhamnosus in children aged 4-48 months with atopic dermatitis: An 8-week, double-blind, randomized, placebo-controlled study. J. Microbiol. Immunol. Infect. 2017, 50, 684–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenfeldt, V.; Benfeldt, E.; Nielsen, S.D.; Michaelsen, K.F.; Jeppesen, D.L.; Valerius, N.H.; Paerregaard, A. Effect of probiotic Lactobacillus strains in children with atopic dermatitis. J. Allergy Clin. Immunol. 2003, 111, 389–395. [Google Scholar] [CrossRef]
- Sistek, D.; Kelly, R.; Wickens, K.; Stanley, T.; Fitzharris, P.; Crane, J. Is the effect of probiotics on atopic dermatitis confined to food sensitized children? Clin. Exp. Allergy 2006, 36, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Passeron, T.; Lacour, J.P.; Fontas, E.; Ortonne, J.P. Prebiotics and synbiotics: Two promising approaches for the treatment of atopic dermatitis in children above 2 years. Allergy 2006, 61, 431–437. [Google Scholar] [CrossRef]
- Gerasimov, S.V.; Vasjuta, V.V.; Myhovych, O.O.; Bondarchuk, L.I. Probiotic supplement reduces atopic dermatitis in preschool children: A randomized, double-blind, placebo-controlled, clinical trial. Am. J. Clin. Dermatol. 2010, 11, 351–361. [Google Scholar] [CrossRef]
- Woo, S.I.; Kim, J.Y.; Lee, Y.J.; Kim, N.S.; Hahn, Y.S. Effect of Lactobacillus sakei supplementation in children with atopic eczema-dermatitis syndrome. Ann. Allergy Asthma Immunol. 2010, 104, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Kim, B.; Ban, J.; Lee, J.; Kim, B.J.; Choi, B.S.; Hwang, S.; Ahn, K.; Kim, J. A randomized trial of Lactobacillus plantarum CJLP133 for the treatment of atopic dermatitis. Pediatr. Allergy Immunol. 2012, 23, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.G.; Li, T.H.; Peng, H.J. Lactobacillus salivarius plus fructo-oligosaccharide is superior to fructo-oligosaccharide alone for treating children with moderate to severe atopic dermatitis: A double-blind, randomized, clinical trial of efficacy and safety. Br. J. Dermatol. 2012, 166, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Yeşilova, Y.; Çalka, Ö.; Akdeniz, N.; Berktaş, M. Effect of probiotics on the treatment of children with atopic dermatitis. Ann. Dermatol. 2012, 24, 189–193. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.J.; Min, T.K.; Lee, H.W.; Pyun, B.Y. Efficacy of Probiotic Therapy on Atopic Dermatitis in Children: A Randomized, Double-blind, Placebo-controlled Trial. Allergy Asthma Immunol. Res. 2014, 6, 208–215. [Google Scholar] [CrossRef] [Green Version]
- Wang, I.J.; Wang, J.Y. Children with atopic dermatitis show clinical improvement after Lactobacillus exposure. Clin. Exp. Allergy 2015, 45, 779–787. [Google Scholar] [CrossRef]
- Roessler, A.; Friedrich, U.; Vogelsang, H.; Bauer, A.; Kaatz, M.; Hipler, U.C.; Schmidt, I.; Jahreis, G. The immune system in healthy adults and patients with atopic dermatitis seems to be affected differently by a probiotic intervention. Clin. Exp. Allergy 2008, 38, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Seki, T.; Matsunaka, H.; Watanabe, T.; Shindo, M.; Yamada, N.; Yamamoto, O. Clinical Effects of Probiotic Bifidobacterium breve Supplementation in Adult Patients with Atopic Dermatitis. Yonago Acta Medica 2010, 53, 37–45. [Google Scholar]
- Drago, L.; Toscano, M.; De Vecchi, E.; Piconi, S.; Iemoli, E. Changing of fecal flora and clinical effect of L. salivarius LS01 in adults with atopic dermatitis. J. Clin. Gastroenterol. 2012, 46, S56–S63. [Google Scholar] [CrossRef]
- Iemoli, E.; Trabattoni, D.; Parisotto, S.; Borgonovo, L.; Toscano, M.; Rizzardini, G.; Clerici, M.; Ricci, E.; Fusi, A.; De Vecchi, E.; et al. Probiotics reduce gut microbial translocation and improve adult atopic dermatitis. J. Clin. Gastroenterol. 2012, 46, S33–S40. [Google Scholar] [CrossRef]
- Matsumoto, M.; Ebata, T.; Hirooka, J.; Hosoya, R.; Inoue, N.; Itami, S.; Tsuji, K.; Yaginuma, T.; Muramatsu, K.; Nakamura, A.; et al. Antipruritic effects of the probiotic strain LKM512 in adults with atopic dermatitis. Ann. Allergy Asthma Immunol. 2014, 113, 209–216.e207. [Google Scholar] [CrossRef]
- Drago, L.; De Vecchi, E.; Toscano, M.; Vassena, C.; Altomare, G.; Pigatto, P. Treatment of atopic dermatitis eczema with a high concentration of Lactobacillus salivarius LS01 associated with an innovative gelling complex: A pilot study on adults. J. Clin. Gastroenterol. 2014, 48 (Suppl. 1), S47–S51. [Google Scholar] [CrossRef]
- Nakatsuji, T.; Hata, T.R.; Tong, Y.; Cheng, J.Y.; Shafiq, F.; Butcher, A.M.; Salem, S.S.; Brinton, S.L.; Rudman Spergel, A.K.; Johnson, K.; et al. Development of a human skin commensal microbe for bacteriotherapy of atopic dermatitis and use in a phase 1 randomized clinical trial. Nat. Med. 2021, 27, 700–709. [Google Scholar] [CrossRef]
- Vijayashankar, M.; Raghunath, N. Pustular Psoriasis Responding to Probiotics—A New Insight. Our Dermatol. Online 2012, 3, 326–329. [Google Scholar] [CrossRef]
- Groeger, D.; O’Mahony, L.; Murphy, E.F.; Bourke, J.F.; Dinan, T.G.; Kiely, B.; Shanahan, F.; Quigley, E.M. Bifidobacterium infantis 35624 modulates host inflammatory processes beyond the gut. Gut Microbes 2013, 4, 325–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro-López, V.; Martínez-Andrés, A.; Ramírez-Boscá, A.; Ruzafa-Costas, B.; Núñez-Delegido, E.; Carrión-Gutiérrez, M.A.; Prieto-Merino, D.; Codoñer-Cortés, F.; Ramón-Vidal, D.; Genovés-Martínez, S.; et al. Efficacy and Safety of Oral Administration of a Mixture of Probiotic Strains in Patients with Psoriasis: A Randomized Controlled Clinical Trial. Acta Derm.-Venereol. 2019, 99, 1078–1084. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.H.; Wu, C.S.; Chao, Y.H.; Lin, C.C.; Tsai, H.Y.; Li, Y.R.; Chen, Y.Z.; Tsai, W.H.; Chen, Y.K. Lactobacillus pentosus GMNL-77 inhibits skin lesions in imiquimod-induced psoriasis-like mice. J. Food Drug Anal. 2017, 25, 559–566. [Google Scholar] [CrossRef] [Green Version]
- Rather, I.A.; Bajpai, V.K.; Huh, Y.S.; Han, Y.-K.; Bhat, E.A.; Lim, J.; Paek, W.K.; Park, Y.-H. Probiotic Lactobacillus sakei proBio-65 Extract Ameliorates the Severity of Imiquimod Induced Psoriasis-Like Skin Inflammation in a Mouse Model. Front. Microbiol. 2018, 9, 1021. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Deng, Y.; Fang, Z.; Zhai, Q.; Cui, S.; Zhao, J.; Chen, W.; Zhang, H. Potential Role of Probiotics in Ameliorating Psoriasis by Modulating Gut Microbiota in Imiquimod-Induced Psoriasis-Like Mice. Nutrients 2021, 13, 2010. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, C.; Inoue, R.; Yonejima, Y.; Hisa, K.; Yamamoto, Y.; Suzuki, T. Supplemental Leuconostoc mesenteroides strain NTM048 attenuates imiquimod-induced psoriasis in mice. J. Appl. Microbiol. 2021. ahead of print. [Google Scholar] [CrossRef]
- Peral, M.C.; Rachid, M.M.; Gobbato, N.M.; Huaman Martinez, M.A.; Valdez, J.C. Interleukin-8 production by polymorphonuclear leukocytes from patients with chronic infected leg ulcers treated with Lactobacillus plantarum. Clin. Microbiol. Infect. 2010, 16, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Mohseni, S.; Bayani, M.; Bahmani, F.; Tajabadi-Ebrahimi, M.; Bayani, M.A.; Jafari, P.; Asemi, Z. The beneficial effects of probiotic administration on wound healing and metabolic status in patients with diabetic foot ulcer: A randomized, double-blind, placebo-controlled trial. Diabetes Metab Res. Rev. 2018, 34. [Google Scholar] [CrossRef]
- Venosi, S.; Ceccarelli, G.; de Angelis, M.; Laghi, L.; Bianchi, L.; Martinelli, O.; Maruca, D.; Cavallari, E.N.; Toscanella, F.; Vassalini, P.; et al. Infected chronic ischemic wound topically treated with a multi-strain probiotic formulation: A novel tailored treatment strategy. J. Transl. Med. 2019, 17, 364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, M.; Ganopolsky, J.G.; Labbé, A.; Gilardino, M.; Wahl, C.; Martoni, C.; Prakash, S. Novel nitric oxide producing probiotic wound healing patch: Preparation and in vivo analysis in a New Zealand white rabbit model of ischaemic and infected wounds. Int. Wound J. 2012, 9, 330–343. [Google Scholar] [CrossRef] [PubMed]
- Stefia, L.V.; Lee, J.; Patel, J.; de Sousa, S.R.; Legrand, J.; Rodero, M.; Burman, S.; Linedale, R.; Morrison, M.; Khosrotehrani, K. Secretome Components from Faecalibacterium prausnitzii Strains A2-165 and AHMP21 Modulate Cutaneous Wound Inflammation. J. Investig. Dermatol. 2020, 140, 2312–2315.e2316. [Google Scholar] [CrossRef] [PubMed]
- Kusumaningsih, T.; Irmawati, A.; Ernawati, D.S.; Prahasanti, C.; Aljunaid, M.; Amelia, S. The differences in the number of fibroblasts and blood vessels after the topical and systemic administration of Lactobacillus casei Shirota probiotics for the treatment of traumatic ulcers in Wistar rats (Rattus norvegicus). Vet. World 2021, 14, 1279–1283. [Google Scholar] [CrossRef]
- Vågesjö, E.; Öhnstedt, E.; Mortier, A.; Lofton, H.; Huss, F.; Proost, P.; Roos, S.; Phillipson, M. Accelerated wound healing in mice by on-site production and delivery of CXCL12 by transformed lactic acid bacteria. Proc. Natl. Acad. Sci. USA 2018, 115, 1895–1900. [Google Scholar] [CrossRef] [Green Version]
- Coman, M.M.; Mazzotti, L.; Silvi, S.; Scalise, A.; Orpianesi, C.; Cresci, A.; Verdenelli, M.C. Antimicrobial activity of SYNBIO(®) probiotic formulation in pathogens isolated from chronic ulcerative lesions: In vitro studies. J. Appl. Microbiol. 2020, 128, 584–597. [Google Scholar] [CrossRef]
- Guéniche, A.; Cathelineau, A.C.; Bastien, P.; Esdaile, J.; Martin, R.; Queille Roussel, C.; Breton, L. Vitreoscilla filiformis biomass improves seborrheic dermatitis. J. Eur. Acad Dermatol. Venereol. 2008, 22, 1014–1015. [Google Scholar] [CrossRef] [PubMed]
- Reygagne, P.; Bastien, P.; Couavoux, M.P.; Philippe, D.; Renouf, M.; Castiel-Higounenc, I.; Gueniche, A. The positive benefit of Lactobacillus paracasei NCC2461 ST11 in healthy volunteers with moderate to severe dandruff. Benef Microbes 2017, 8, 671–680. [Google Scholar] [CrossRef]
- Peral, M.C.; Martinez, M.A.; Valdez, J.C. Bacteriotherapy with Lactobacillus plantarum in burns. Int. Wound J. 2009, 6, 73–81. [Google Scholar] [CrossRef]
- Stefanatou, E.; Kompoti, M.; Paridou, A.; Koutsodimitropoulos, I.; Giannopoulou, P.; Markou, N.; Kalofonou, M.; Trikka-Graphakos, E.; Tsidemiadou, F. Probiotic sepsis due to Saccharomyces fungaemia in a critically ill burn patient. Mycoses 2011, 54, e643–e646. [Google Scholar] [CrossRef]
- Thomson, C.H.; Hassan, I.; Dunn, K. Yakult: A role in combating multi-drug resistant Pseudomonas aeruginosa? J. Wound Care 2012, 21, 568–569. [Google Scholar] [CrossRef] [PubMed]
- Mayes, T.; Gottschlich, M.M.; James, L.E.; Allgeier, C.; Weitz, J.; Kagan, R.J. Clinical safety and efficacy of probiotic administration following burn injury. J. Burn Care Res. 2015, 36, 92–99. [Google Scholar] [CrossRef] [PubMed]
- El-Ghazely, M.H.; Mahmoud, W.H.; Atia, M.A.; Eldip, E.M. Effect of probiotic administration in the therapy of pediatric thermal burn. Ann. Burn. Fire Disasters 2016, 29, 268–272. [Google Scholar]
- Perdanakusuma, D.S.; Hariani, L.; Nasser, N.F.; Datusanantyo, R.A. The effect of a single-strain probiotic administration in the treatment of thermal burns patients. Iran. J. Microbiol. 2019, 11, 541. [Google Scholar] [CrossRef]
- Fleming, D.; Jiang, Y.; Opoku, K.; Alhaj Saleh, A.; Larumbe-Zabala, E.; Kesey, J.E.; Griswold, J.A.; Dissanaike, S. Prophylactic Probiotics in Burn Patients: Risk versus Reward. J. Burn Care Res. 2019, 40, 953–960. [Google Scholar] [CrossRef]
- Herek, O.; Kara, I.G.; Kaleli, I. Effects of antibiotics and Saccharomyces boulardii on bacterial translocation in burn injury. Surg Today 2004, 34, 256–260. [Google Scholar] [CrossRef]
- Gong, Z.Y.; Yuan, Z.Q.; Dong, Z.W.; Peng, Y.Z. Glutamine with probiotics attenuates intestinal inflammation and oxidative stress in a rat burn injury model through altered iNOS gene aberrant methylation. Am. J. Transl Res. 2017, 9, 2535–2547. [Google Scholar]
- Valdéz, J.C.; Peral, M.C.; Rachid, M.; Santana, M.; Perdigón, G. Interference of Lactobacillus plantarum with Pseudomonas aeruginosa in vitro and in infected burns: The potential use of probiotics in wound treatment. Clin. Microbiol. Infect. 2005, 11, 472–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brachkova, M.I.; Duarte, A.; Pinto, J.F. Alginate films containing viable Lactobacillus plantarum: Preparation and in vitro evaluation. AAPS PharmSciTech 2012, 13, 357–363. [Google Scholar] [CrossRef] [Green Version]
- Argenta, A.; Satish, L.; Gallo, P.; Liu, F.; Kathju, S. Local Application of Probiotic Bacteria Prophylaxes against Sepsis and Death Resulting from Burn Wound Infection. PLoS ONE 2016, 11, e0165294. [Google Scholar] [CrossRef] [Green Version]
- Satish, L.; Gallo, P.H.; Johnson, S.; Yates, C.C.; Kathju, S. Local Probiotic Therapy with Lactobacillus plantarum Mitigates Scar Formation in Rabbits after Burn Injury and Infection. Surg Infect. 2017, 18, 119–127. [Google Scholar] [CrossRef] [Green Version]
- Sürmeli, M.; Maçin, S.; Akyön, Y.; Kayikçioğlu, A.U. The protective effect of Lactobacillus plantarum against meticillin-resistant Staphylococcus aureus infections: An experimental animal model. J. Wound Care 2019, 28, s29–s34. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Hussain, Z.; Ali, S.; Qamar, Z.; Imran, M.; Hafeez, F.Y. Fabrication of Electrospun Probiotic Functionalized Nanocomposite Scaffolds for Infection Control and Dermal Burn Healing in a Mice Model. ACS Biomater. Sci. Eng. 2019, 5, 6109–6116. [Google Scholar] [CrossRef]
- Olguin, F.; Araya, M.; Hirsch, S.; Brunser, O.; Ayala, V.; Rivera, R.; Gotteland, M. Prebiotic ingestion does not improve gastrointestinal barrier function in burn patients. Burns 2005, 31, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Fabbrocini, G.; Bertona, M.; Picazo, Ó.; Pareja-Galeano, H.; Monfrecola, G.; Emanuele, E. Supplementation with Lactobacillus rhamnosus SP1 normalises skin expression of genes implicated in insulin signalling and improves adult acne. Benef. Microbes 2016, 7, 625–630. [Google Scholar] [CrossRef] [Green Version]
- Dall’Oglio, F.; Milani, M.; Micali, G. Effects of oral supplementation with FOS and GOS prebiotics in women with adult acne: The “S.O. Sweet” study: A proof-of-concept pilot trial. Clin. Cosmet Investig. Dermatol. 2018, 11, 445–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahmayani, T.; Putra, I.B.; Jusuf, N.K. The Effect of Oral Probiotic on the Interleukin-10 Serum Levels of Acne Vulgaris. Open Access Maced J. Med. Sci. 2019, 7, 3249–3252. [Google Scholar] [CrossRef] [Green Version]
- Kang, B.S.; Seo, J.G.; Lee, G.S.; Kim, J.H.; Kim, S.Y.; Han, Y.W.; Kang, H.; Kim, H.O.; Rhee, J.H.; Chung, M.J.; et al. Antimicrobial activity of enterocins from Enterococcus faecalis SL-5 against Propionibacterium acnes, the causative agent in acne vulgaris, and its therapeutic effect. J. Microbiol. 2009, 47, 101–109. [Google Scholar] [CrossRef] [PubMed]
- AOBiome. Therapeutics Reports Positive Efficacy Results from Phase 2b Clinical Trial of Ammonia Oxidizing Bacteria (AOB) for the Treatment of Acne Vulgaris; Therapeutics: San Diego, CA, USA, 2017. [Google Scholar]
- Tayupanta, T.d.l.A.M.; Ocana, V. In vivo Evaluation of the Antagonistic Effect of Lactobacillus acidophilus against Propionobacterium acnes in the Treatment of Acne. J. Pure Appl. Microbiol. 2019, 13, 1317–1324. [Google Scholar] [CrossRef] [Green Version]
- Al-Ghazzewi, F.H.; Tester, R.F. Effect of konjac glucomannan hydrolysates and probiotics on the growth of the skin bacterium Propionibacterium acnes in vitro. Int. J. Cosmet Sci 2010, 32, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.S.; Oh, J.S.; Lee, S.W.; Lim, H.S.; Choi, N.K.; Kim, S.M. Effect of Lactobacillus reuteri on the proliferation of Propionibacterium acnes and Staphylococcus epidermidis. J. Microbiol. 2012, 50, 137–142. [Google Scholar] [CrossRef]
- Lee, D.K.; Kim, M.J.; Ham, J.W.; An, H.M.; Cha, M.K.; Lee, S.W.; Park, C.I.; Shin, S.H.; Lee, K.O.; Kim, K.J.; et al. In vitro evaluation of antibacterial activities and anti-inflammatory effects of Bifidobacterium spp. addressing acne vulgaris. Arch Pharm Res 2012, 35, 1065–1071. [Google Scholar] [CrossRef] [PubMed]
- Khalfallah, G.; Gartzen, R.; Möller, M.; Heine, E.; Lütticken, R. A New Approach to Harness Probiotics Against Common Bacterial Skin Pathogens: Towards Living Antimicrobials. Probiotics Antimicrob. Proteins 2021, 1–15. [Google Scholar] [CrossRef]
- Kunz, B.; Oranje, A.P.; Labreze, L.; Stalder, J.F.; Ring, J.; Taieb, A. Clinical validation and guidelines for the SCORAD index: Consensus report of the European Task Force on Atopic Dermatitis. Dermatology 1997, 195, 10–19. [Google Scholar] [CrossRef]
- Nutten, S. Atopic dermatitis: Global epidemiology and risk factors. Ann. Nutr. Metab 2015, 66 (Suppl. 1), 8–16. [Google Scholar] [CrossRef]
- Bjorksten, B.; Sepp, E.; Julge, K.; Voor, T.; Mikelsaar, M. Allergy development and the intestinal microflora during the first year of life. J. Allergy Clin. Immunol. 2001, 108, 516–520. [Google Scholar] [CrossRef]
- Kong, H.H.; Oh, J.; Deming, C.; Conlan, S.; Grice, E.A.; Beatson, M.A.; Nomicos, E.; Polley, E.C.; Komarow, H.D.; Program, N.C.S.; et al. Temporal shifts in the skin microbiome associated with disease flares and treatment in children with atopic dermatitis. Genome Res. 2012, 22, 850–859. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.Y.; Kwon, J.H.; Ahn, S.H.; Lee, S.I.; Han, Y.S.; Choi, Y.O.; Lee, S.Y.; Ahn, K.M.; Ji, G.E. Effect of probiotic mix (Bifidobacterium bifidum, Bifidobacterium lactis, Lactobacillus acidophilus) in the primary prevention of eczema: A double-blind, randomized, placebo-controlled trial. Pediatr. Allergy Immunol. 2010, 21, e386–e393. [Google Scholar] [CrossRef]
- Parisi, R.; Symmons, D.P.; Griffiths, C.E.; Ashcroft, D.M. Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J. Investig. Dermatol. 2013, 133, 377–385. [Google Scholar] [CrossRef] [Green Version]
- Langley, R.G.; Krueger, G.G.; Griffiths, C.E. Psoriasis: Epidemiology, clinical features, and quality of life. Ann. Rheum. Dis. 2005, 64 (Suppl. 2), ii18–ii23. [Google Scholar] [CrossRef] [Green Version]
- Polkowska-Pruszynska, B.; Gerkowicz, A.; Krasowska, D. The gut microbiome alterations in allergic and inflammatory skin diseases—An update. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Sonal Sekhar, M.; Unnikrishnan, M.K.; Vijayanarayana, K.; Rodrigues, G.S.; Mukhopadhyay, C. Topical application/formulation of probiotics: Will it be a novel treatment approach for diabetic foot ulcer? Med. Hypotheses 2014, 82, 86–88. [Google Scholar] [CrossRef]
- Vijaya Chandra, S.H.; Srinivas, R.; Dawson, T.L., Jr.; Common, J.E. Cutaneous Malassezia: Commensal, Pathogen, or Protector? Front. Cell. Infect. Microbiol. 2021, 10, 614446. [Google Scholar] [CrossRef] [PubMed]
- White, T.C.; Findley, K.; Dawson, T.L., Jr.; Scheynius, A.; Boekhout, T.; Cuomo, C.A.; Xu, J.; Saunders, C.W. Fungi on the skin: Dermatophytes and Malassezia. Cold Spring Harb. Perspect. Med. 2014, 4, a019802. [Google Scholar] [CrossRef] [Green Version]
- Kistowska, M.; Fenini, G.; Jankovic, D.; Feldmeyer, L.; Kerl, K.; Bosshard, P.; Contassot, E.; French, L.E. Malassezia yeasts activate the NLRP3 inflammasome in antigen-presenting cells via Syk-kinase signalling. Exp. Dermatol. 2014, 23, 884–889. [Google Scholar] [CrossRef] [PubMed]
- Perkins, M.A.; Cardin, C.W.; Osterhues, M.A.; Robinson, M.K. A non-invasive tape absorption method for recovery of inflammatory mediators to differentiate normal from compromised scalp conditions. Skin Res. Technol. 2002, 8, 187–193. [Google Scholar] [CrossRef]
- Vlachos, C.; Schulte, B.M.; Magiatis, P.; Adema, G.J.; Gaitanis, G. Malassezia-derived indoles activate the aryl hydrocarbon receptor and inhibit Toll-like receptor-induced maturation in monocyte-derived dendritic cells. Br. J. Dermatol. 2012, 167, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo, B.; Luca, S.; Antonio, M.; Alberto, D.M.; Cesare, F.; Omar, C. Effects of Probiotics in the Management of Infected Chronic Wounds: From Cell Culture to Human Studies. Curr. Clin. Pharmacol. 2020, 15, 193–206. [Google Scholar] [CrossRef]
- De Pessemier, B.; Grine, L.; Debaere, M.; Maes, A.; Paetzold, B.; Callewaert, C. Gut-Skin Axis: Current Knowledge of the Interrelationship between Microbial Dysbiosis and Skin Conditions. Microorganisms 2021, 9, 353. [Google Scholar] [CrossRef]
- Mottin, V.H.M.; Suyenaga, E.S. An approach on the potential use of probiotics in the treatment of skin conditions: Acne and atopic dermatitis. Int. J. Dermatol. 2018, 57, 1425–1432. [Google Scholar] [CrossRef]
- Fitz-Gibbon, S.; Tomida, S.; Chiu, B.H.; Nguyen, L.; Du, C.; Liu, M.; Elashoff, D.; Erfe, M.C.; Loncaric, A.; Kim, J.; et al. Propionibacterium acnes strain populations in the human skin microbiome associated with acne. J. Investig. Dermatol. 2013, 133, 2152–2160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruggemann, H.; Salar-Vidal, L.; Gollnick, H.P.M.; Lood, R. A Janus-Faced Bacterium: Host-Beneficial and -Detrimental Roles of Cutibacterium acnes. Front. Microbiol. 2021, 12, 673845. [Google Scholar] [CrossRef]
- Deng, Y.; Wang, H.; Zhou, J.; Mou, Y.; Wang, G.; Xiong, X. Patients with Acne Vulgaris Have a Distinct Gut Microbiota in Comparison with Healthy Controls. Acta Derm. Venereol. 2018, 98, 783–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebello, D.; Wang, E.; Yen, E.; Lio, P.A.; Kelly, C.R. Hair Growth in Two Alopecia Patients after Fecal Microbiota Transplant. ACG Case Rep. J. 2017, 4, e107. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Number (No.) of Study | Author | Patient Population (Number) | Type of Study | Intervention | Results |
|---|---|---|---|---|---|
| 1 | Kalliomaki et al.—2007 [25] | Pregnant women (n = 159) with a family histors of AD, continuing after delivery and their children (n = 132) | Double-blind, randomised placebo-controlled trial | Participants received two capsules of placebo (n = 95) or LGG (n = 64) daily for 2–4 weeks before expected delivery | The frequency of AD was significantly reduced |
| 2 | Rautava et al.—2006 [26] | Infants with 6 months of exclusive breast-feeding (n = 38) | Double-blind placebo-controlled study | Infant formula supplemented with either LGG and Bb-12 (n = 38) or placebo (microcrystalline cellulose) (n = 43) daily until the age of 12 months | Supplementation of probiotics increased protective cow’s milk-specific IgA responses. 13% of the infants receiving probiotics and 20% of those receiving placebo manifested with AD, cow’s milk allergy was confirmed in none of the infants receiving probiotics and in 8% of the infants receiving placebo |
| 3 | Abrahamsson et al.—2007 [27] | Pregnant women with a family history of at least 1 allergic disease (n = 188) and then their infants (n = 188) | Prospective, double-blind, placebo-controlled, multicenter trial | The mothers were taking L. reuteri (n = 95) or placebo (n = 93) 4 weeks before term and continued daily until delivery, after birth, the baby continued with the same product up to 12 months of age | The cumulative incidence of AD was similar in the probiotic and the placebo groups (36% vs. 34%) |
| 4 | Taylor et al.—2007 [28] | Infants with atopic mother (n = 178) | Randomized, double-blind, placebo-controlled | Newborns of women with allergy received either L. acidophilus (n = 89) or placebo (n = 89) daily for the first 6 months of life | Not reduction in the risk of AD and increased allergen sensitization |
| 5 | Wickens et al.—2008 [29] | Pregnant women (n = 474) and their infants (n = 474) | Double-blind randomized placebo-controlled trial | Daily supplementation with either HN001 (n = 157) or HN019 (n = 158) or placebo (n = 159) from 35 weeks gestation until birth, continuing to 6 months after birth in mothers if breastfeeding, and from birth till 2 years in all infants | Prevention of the development of AD |
| 6 | Huurre et al.—2008 [30] | Pregnant women (n = 140) and infants (n = 138) | Placebo-controlled prospective intervention study | Oral administration of LGG and Bb-12 each day (n = 72/70), or placebo (microcrystalline cellulose and dextrose anhydrate) (n = 68). Atopic sensitization was at the age of 6 and 12 months and in mothers at third trimester of pregnancy | There was no difference between infant sensitization in the probiotic and the placebo group |
| 7 | Kopp et al.—2008 [31] | Pregnant women (n = 105) with a family history of at least one allergic disease and their children (n = 96) | Double-blind, placebo-controlled prospective trial | Administration of either the probiotic LGG (n = 54) twice daily or placebo (n = 51) 4–6 weeks before expected delivery, followed by a postnatal period of 6 months | After a 2 year follow-up, administration of probiotic did not reduce the incidence nor altered the severity of AD |
| 8 | West et al.—2009 [32] | Healthy infants with birth weight >2500 g who were vaginally delivered (n = 89) | Double-blind, placebo-controlled randomized intervention trial | Daily intake of cereals supplemented with LF19 (n = 89) or identical cereals without LF19 supplementation (n = 90) from 4 to 13 months of age | Decreased cumulative incidence of AD |
| 9 | Niers et al.—2009 [33] | Pregnant women (156) and then their infants with a positive family history of allergic disease (n = 156) | Double-blind, randomized, placebo-controlled trial | Probiotic bacteria were prenatally administered to pregnant mothers (n = 78) during the last 6 weeks of pregnancy and postnatally for 12 months to their infants (n = 78); the intervention group received once daily B. bifidum W23, B. lactis W52, and L. lactis W58) in a freeze dried powder | Decreased incidence of AD |
| 10 | Soh et al.—2009 [34] | Infants with a positive family history of allergic disease (n = 253) | Double-blind, placebo-controlled randomized clinical trial | Infants (n = 127) received commercially available cow’s milk formula with probiotic supplementation of BL999 and L. rhamnosus daily for the first 6 months. Infants in the control group (n = 126) received milk without probiotics | No effect on the prevention of AD or allergen sensitization |
| 11 | Kim et al.—2010 [35] | Pregnant women with a family history of allergic diseases (n = 112), continuing after delivery and their infants (n = 68) | Double-blind, randomized, placebo-controlled trial | Pregnant woman received supplement of B. bifidum BGN4, B. lactis AD011 and L. acidophilus AD03 (n = 33) or placebo (n = 35), starting at 4–8 weeks before delivery and continuing until 6 months after delivery. Infants were exclusively breastfed during the first 3 months, and were fed with breastmilk or cow’s milk formula from 4 to 6 months of age | The prevalence of AD in the first year of life was significantly lower in the probiotic group. |
| 12 | Dotterud et al.—2010 [36] | Pregnant women (n = 415) and their infants (n = 278) | Randomized, double-blind trial | Pregnant women received probiotic milk (n = 138) or placebo (n = 140) from 36 weeks of gestation to 3 months postnatally during breastfeeding | Decreased cumulative incidenceof AD. |
| 13 | Boyle et al.—2011 [37] | Pregnant women (n = 250), their partner or a previous child was affected by allergic disease including asthma, eczema, food allergy or allergic rhinitis | Randomized controlled trial | Participants were allocated to take probiotic treatment with LGG (n = 125) or maltodextrin placebo (n = 125) each morning from 36 weeks gestation until delivery. Infants were assessed during their first year for eczema or allergic sensitization | Prenatal treatment was not associated with reduced risk of eczema or IgE-associated eczema but decreased breast milk soluble CD14 and IgA levels |
| 14 | Rautava et al.—2012 [38] | Pregnant women with atopic sensitization (n = 241) and their infants (n = 205) | Double-blind, randomized, placebo-controlled trial | Pregnant women received a dietary food supplement with the combination of LPR and BL999 (n = 81) or the combination of ST11 and BL999 (n = 82) or placebo (78) | Administration of specific probiotics is a safe and effective way in reducing the risk of AD |
| 15 | Ou et al.—2012 [39] | Pregnant women with atopic diseases determined by history, total immunoglobulin (Ig)E > 100 kU/L, and/or positive specific IgE (n = 191) | Prospective, double-blind, placebo-controlled clinical trial | Pregnant woman receive either LGG ATCC 53103 (n = 95) or placebo (n = 96) from the second trimester of pregnancy | Reduced severity of maternal allergic disease |
| 16 | Lau et al.—2012 [40] | Infants with at least single heredity for atopy (n = 606) | Randomized, placebo-controlled trial | From week 5 until the end of month 7, infants were treated orally with bacterial lysate containing heat-killed gram-negative E. coli and gram-positive E. faecalis (n = 303) or placebo (n = 303) | Prevention of the development of AD |
| 17 | Allen et al.—2014 [41] | Pregnant women (n = 454) and then their infants with a positive family history of allergic disease (n = 454) | Randomised, double-blind, placebo-controlled, parallel group trial | Women from 36 weeks gestation and their infants to age 6 months received daily either the probiotic (L. salivarius CUL61, L. paracasei CUL08, B. animalis subsp. lactis CUL34 and B. bifidum CUL20) (n = 220) or placebo (n = 234) | Cumulative frequency of AD at 2 years of age was similar between the two groups |
| 18 | Cabana et al.—2017 [42] | Infants (n = 184) | Randomized, double-blind controlled trial | The intervention group received a daily capsule of LGG and inulin for the first 6 months of life (n = 92); the control group received inulin (n = 92) | At 5 years of age, the cumulative incidence of asthma was significantly higher in the control group (17.4%) than in the intervetion group (9.7%) |
| 19 | Wickens et al.—2018 [43] | Pregnant women, continuing after giving birth. The patient or her partner had a history of atopic disease (n = 473) | 2-centre, parallel double-blind, randomized placebo-controlled trial | HN001 (n = 157), HN019 (n = 158) or placebo (n = 159) was taken daily by mothers from 14-16 weeks of gestation until 6 months post-partum. Their infants were also given the the same capsule daily from birth until the age of 2 years | Prevention of the development of AD and atopic sensitization |
| 20 | Plummer et al.—2019 [44] | Preterm infants, born <32 gestational week and weighing <1500 g (n = 281) | Multi-center, double-blind, placebo-controlled randomized trial | Infants in the inetrvention group (n = 127) received a probiotic combination B. infantis, Str. thermophilus, and B. lactis once daily (in a maltodextrin base powder) and the placebo group (n = 154) received maltodextrin | No effect on the incidence of allergic diseases or atopic sensitization |
| 21 | Schmidt et al.—2019 [45] | Infants with birthweight >2500 g, gestational age >36 weeks (n = 144) | Double-blind, placebo-controlled intervention trial | The intervention group (n = 144) received sachets of maltodextrin supplemented with LGG and Bb-12, and the placebo group (146) received maltodextrin only | A significantly lower incidence of AD in the probiotic group |
| No. of Study | Author | Patient Population (Number) | Type of Study | Intervention | Results |
|---|---|---|---|---|---|
| 1 | Moro et al.—2006 [46] | Infants at risk for atopy (n = 259) | Prospective, double-blind, randomised, placebo controlled trial | Participants received either hydrolysed cows’ milk with GOS/FOS in the prebiotic group (n = 102) or maltodexitrin in the control group (n = 104) | Development of AD was significantly more frequent in the control group |
| 2 | Ziegler et al.—2007 [47] | Healthy infants (n = 226) | Double-blind, randomized, controlled, parallel-group, prospective trial | Participants were divided into 3 different formula groups: control group-PDX (n = 76), PG4 group- PDX+GOS (n = 74), PDL8 group-PDX, GOS, LOS (76). Formula was fed for 120 days | No differences among the groups in growth rate |
| 3 | Arslanoglu et al.—2008, 2012 [48,49] | Healthy infants with a parental history of atopy (n = 134) | Prospective, double-blind, randomised, placebo controlled trial | Participants received either GOS/FOS prebiotic supplement in the intervention group (n = 66) or maltodexitrin supplementation in the controll group (n = 68) | Cumulative incidences for AD, recurrent wheezing, and allergic urticaria were higher in the placebo group after 2 years |
| 4 | Grüber et al.—2010, 2016 [50,51] | Healthy infants with low risk of atopy (n = 1130) | Double-blind, controlled, randomized, prospective intervention study | Participants were divided into thre groups: prebiotic group (n = 414) -mixture of GOS, FOS, pAOS, breastfed group (n = 300), control group (n = 416) | After 1 year, AD occurred in significantly fewer infants from the prebiotic group |
| 5 | Niele et al.—2012 [52] | Preterm infants (n = 94) | Prospective, double-blind, randomised, placebo controlled trial | Volunteers received either enteral GOS, FOS and pAOS supplementation (n = 48) or placebo (n = 46) during first month of life | No decrease in the incidence of allergic and infectious diseases during first year of life |
| 6 | Pontes et al.—2016 [53] | Healthy children (1–4 years of age) (n = 256) | Double-blind, randomized, controlled trial | The intervention group (n = 125) received cow’s milk-based beverage containing DHA, PDX, GOS, β-glucan and the control group (n = 131) were fed cow’s milk three servings/day up to 28 weeks | Participants in the intervention group were associated with fewer episodes of allergic manifestations |
| 7 | Boyle et al.—2016 [54] | Infants with an atopic parent (n = 1047) | Parallel-group, multicentre, randomized double-blind controlled trial | Three groups: prebiotic group (n = 432) -mixture of GOS, FOS, pAOS, breastfed group (n = 184), control group (n = 431) | Prebiotics did not prevent AD in the first year of life |
| 8 | Ranucci et al.—2018 [55] | Infants (n = 400) with an atopic parent | Randomised, double-blind, placebo-controlled trial | Participants received either prebiotic formula containing GOS/PDX (n = 201) or standard formula (n = 199) in the first 48 weeks of life | No significant differences in the cumulative incidence of AD and its intensity and duration between groups |
| 9 | Wopereis et al.—2018 [56] | Healthy infants (n = 138) | Double-blind, randomized, controlled parallel-group nutritional intervention trial | Participants were divided into thre groups: prebiotic group (n = 51) -mixture of GOS, FOS, pAOS, breastfed group (n = 30), control group (n = 57) | Metabolites and pH of infants receiving GOS/FOS/pAOS was closer to breastfed infants than to infants receiving standard cow’s milk formula. After 18 months, AD occurred in significantly fewer infants in the prebiotic group |
| No. of Study | Author | Patient Population (Number) | Type of Study | Intervention | Results |
|---|---|---|---|---|---|
| 1 | Majamaa et al.—1997 [57] | Infants aged 2.5 to 15.7 months with AD (n = 27), nursing mothers of infants with AD (n = 10) | Randomized controlled trial | Infants with AD and cow’s milk allergy received cow’s milk without (n = 14) and with (n = 13) the addition of LGG; the second part of the study involved 10 breast-fed infants who had AD and cow’s milk allergy. In this group LGG was given to nursing mothers | Probiotic bacteria downregulated hypersensitivity reactions and intestinal inflammation |
| 2 | Isolauri et al.—2000 [58] | Infants with AD, mean age of 4.6 months (n = 27) | Randomized double-blind placebo-controlled study | Probiotic-supplemented, Bb-12 (n = 9) or LGG ATCC 53103 (n = 9), extensively hydrolysed whey formulas or to the same formula without probiotics (n = 9) | First clinical demonstration of specific probiotic strains modifying AD |
| 3 | Kirjavainen et al.—2003 [59] | Infants with AD, mean age was 5.5 months (n = 43) | Randomized double-blind manner | Infants were randomly assigned into placebo (n = 10), viable LGG (n = 17), or heat-inactivated LGG groups (n = 16) and extensively hydrolyzed whey formula or the same formula supplemented with viable or heat-inactivated LGG | Supplementation of infant formulas with viable but not heat-inactivated probiotic was effective for the management of AD and cow’s milk allergy |
| 4 | Viljanen et al.—2005 [60] | Infants with AD under the age of 12 months (n = 230) | Randomized double-blinded study | First group (n = 80) received capsules containing LGG ATCC 53103; the second group (n = 76) a mixture of probiotics: LGG, L. rhamnosus LC705, B. breve Bbi99, and Propionibacterium JS; and there was a placebo group (n = 74) | Treatment with L. rhamnosus alleviated AD symptoms in IgE-sensitized infants |
| 5 | Weston et al.—2005 [61] | Children aged 6-18 months with moderate or severe AD (n = 56) | Randomised double blind placebo controlled trial | The children were given a L. fermentum VRI-033 PCC (n = 28) or placebo (n = 28), twice daily for 8 weeks | Supplementation with probiotic bacteria is beneficial in improving the extent and severity of the symptoms |
| 6 | Taniuchi et al.—2005 [62] | Infants with cow milk hypersensitivity and AD (n = 10) | Randomised placebo controlled trial | Orally given lyophilized bifidobacteria B. breve M-16V (n = 10) strain or placebo (n = 7) | Significantly increased proportion of bifidobacteria in the fecal microflora |
| 7 | Folster-Holst et al.—2006 [63] | Infants (n = 54) aged 1-55 months with moderate-to-severe AD | Randomized, double-blind, placebo-controlled study | LGG (n = 26) or placebo (n = 27) was received during an 8-week period | No significant differences between the groups in the clinical symptoms |
| 8 | Brouwer et al.—2006 [64] | Infants less than 5 months old with AD (n = 50) | Randomized, double-blind, placebo-controlled study | Participants received a hydrolysed whey-based formula as placebo (n = 17), or supplemented with either L. rhamnosus (n = 17) or LGG (n = 16) for 3 months | No clinical or immunological effect of L. rhamnosus |
| 9 | Grüber et al.—2007 [65] | Infants with AD aged 3–12 months (n = 54) | Randomized trial | LGG (54) or placebo (48) as a food supplement for 12 weeks | No therapeutic effect of probiotic against mild to moderate AD |
| 10 | Flintermann et al.—2007 [66] | Children aged 0.5–2.8 years with AD (n = 13) | Randomized trial | Probiotics (n = 7) or placebo (n = 6) was randomly assigned to the patients. The probiotics contained a mixture of L. acidophilus W55, L. casei W56, L. salivarius W57, L. lactis W58, B. infantis W52, B. lactis W18 and B. longum W51 | Probiotics enhanced the production of Th1 and regulatory cytokines in vitro |
| 11 | van der Aa LB et al.—2010 [67] | Infants with AD SCORAD > or =15, aged < 7 months and exclusively formula fed (n = 90) | Double-blind, placebo-controlled multi-centre trial | Extensively hydrolysed formula with B. breve M-16V and a galacto-/fructo-oligosaccharide mixture (n = 46) or the same formula without synbiotics (n = 44) for 12 weeks | Synbiotic mixture does not have a beneficial effect on the severity of AD, but it modulates the intestinal microbiota |
| 12 | Gøbel et al.—2010 [68] | Children from 7 to 24 months of age with AD (n = 50) | Randomised double-blind placebo-controlled trial | First group: L. acidophilus NCFM and other supplements in a capsule given (n = 17), Second group: B. lactis Bi-07 and supplements in a capsule given (n = 17). Third group received placebo (n = 16). Treatment was given daily for 8 weeks | No overall beneficial effects on the degree of SCORAD index. |
| 13 | Nermes et al.—2011 [69] | Infants with AD (n = 39) | Double-blind study | Extensively hydrolysed casein formula supplemented with (n = 19) or without (n = 20) LGG (ATCC 53103) was given to the two differenct groups for three months | Probiotics may enhance gut barrier function |
| 14 | Farid et al.—2011 [70] | Infants and children aged 3 months to 6 years with AD (n = 40) | Randomized, double-blind, placebo-controlled study | Patients in the probiotic group (n = 19) received synbiotic containing a mixture of L. casei, L. rhamnosus, Str. thermophilus, B. breve, L. acidophilus, B. infantis, Lactobacillus bulgaricus and FOS twice daily for 8 weeks | Mixture of probiotics and FOS improved the severity of symptoms |
| 15 | Gore et al.—2012 [71] | Infants with AD (n = 208) | Randomized-controlled trial | Infants were randomized to daily supplements containing L. paracasei or B. lactis (n = 137) or placebo (n = 71) for a 3-month period, while receiving extensively hydrolysed whey-formula (dairy-free diet) | No benefit in the treatment of eczema and no effect on the progression of allergic disease |
| 16 | Shafiei et al.—2011 [72] | Infants aged 1-36 months with moderate-to-severe AD (n = 41) | Randomized double blind-placebo controlled trial | Mixture of seven strain probiotics plus FOS (n = 20) or placebo (n = 21), administered daily as a powder for two months | No improvement of AD |
| 17 | Ivakhnenko et al.—2013 [73] | Infants aged of 3-12 months with the diagnosis of AD and allergy to cow’s milk protein (n = 60) | Open randomized prospective clinical study | Bb-12 and Str. thermophilus TH-4 intake for half of volunteers (n = 30). The other half of the volunteers (n = 30) received placebo for 4 weeks | Improved clinical symptoms |
| 18 | Lin et al.—2015 [74] | Infants with AD (n = 40) | Randomized controled study | The intervention group (n = 20) received B. bifidum triple viable capsules for 4 weeks with a dosage of one capsule three times a day. The control group (n = 20) were not given a placebo drug | Positive effect on the prevention and treatment |
| 19 | Guo et al.—2015 [75] | Adult AD patients (n = 180) | Randomized trial | Participants were divided into two groups. Participants received routine symptomatic treatment and combination of probiotics (microecologics) (n = 90) or symptomatic treatment (n = 90) orally twice a day for one month | Application of microecologics as an adjuvant therapy was effective |
| 20 | Wu et al.—2017 [76] | Children aged 4-48 months with AD and with SCORAD ≥ 15 at enrollment. (n = 66) | Two-center, double-blinded, randomized and placebo-controlled study | Treatment group (n = 33)—one capsule containing L. rhamnosus a day, control group (n = 33)—one capsule of placebo a day for 8 weeks | Probiotic was effective in decreasing AD symptoms |
| No. of Study | Author | Patient Population (Number) | Type of Study | Intervention | Results |
|---|---|---|---|---|---|
| 1 | Rosenfeldt et al.—2003 [77] | Children aged 1 to 13 years with AD (n = 43) | Double-blind, placebo-controlled, crossover study | The patients were randomized in two groups to receive either placebo followed by active treatment or active treatment followed by placebo. 2 probiotic lyophilized L. rhamnosus 19070-2 and L. reuteri DSM 122460 were given in combination for 6 weeks | Combination of probiotics was significantly effective in the management of AD |
| 2 | Sistek et al.—2006 [78] | Children aged between 1 and 10 years with AD (n = 59) | Randomized controlled trial | L. rhamnosus and B. lactis (n = 29) or placebo (n = 30) were given daily as a powder for 12 weeks | Combination of probiotic bacteria improved AD only in food sensitized children |
| 3 | Passeron et al.—2006 [79] | Children aged at least 2 years with AD (n = 48) | Double-blind prospective randomized study | L. rhamnosus Lcr35 plus prebiotic preparation (n = 24) or prebiotic preparation alone (n = 24) was given three times a day for 3 months | Both synbiotics and prebiotics used alone seem able to significantly improve the manifestations of AD |
| 4 | Gerasimov et al.—2010 [80] | Children aged 1–3 years with moderate-to-severe AD (n = 90) | Randomized, double-blind, placebo-controlled, prospective trial | Infants were randomly assigned into placebo (n = 47), and intervention group (n = 43). Mixture of L. acidophilus DDS-1, B. lactis UABLA-12 with fructo-oligosaccharide or placebo twice daily for 8 weeks | Significant clinical improvement |
| 5 | Woo et al. —2010 [81] | Children aged 2 to 10 years with AD (n = 45) | Double-blind, placebo-controlled trial | Volunteers received either L. sakei KCTC 10755BP (n = 45) or placebo (n = 33) daily for 12 weeks | Substantial clinical improvement and a significant decrease in chemokine levels |
| 6 | Han et al.—2012 [82] | Children aged 1–13 years presenting with AD (n = 83) | Randomized, double-blind, placebo-controlled study | L. plantarum CJLP133(n = 44) or placebo (n = 39) was given to children twice a day for 12 weeks. SCORAD scores, eosinophil counts, serum total IgE, IFN-γ and IL-4 were evaluated | SCORAD score at week 14 was significantly lower in the probiotic group |
| 7 | Wu et al.—2012 [83] | Children aged 2-14 years with moderate-to-severe AD (n = 54) | Double-blind, randomized, clinical trial | One capsule twice daily for 8 weeks containing either L. salivarius and FOS (n = 27) or FOS only (n = 27) | Synbiotic combination was superior to the prebiotic alone |
| 8 | Yesilova et al.—2012 [84] | Children suffering from a moderate-to-severe AD, 1-13 years of age (n = 40) | Double-blind, randomized, placebo-controlled study | The probiotic group (n = 20) was administered with a probiotic complex containing B. bifidum, L. acidophilus, L. casei, and L. salivarius for 8 weeks. The placebo group (n = 20) was administered skim milk powder and dextrose | Probiotics to be effective in reducing SCORAD index, serum IL-5, IL-6, IFN-γ, and total serum IgE levels but not effective in reducing serum IL-2, IL-4, IL-10, ECP, or TNF-α levels |
| 9 | Yang et al.— 2014 [85] | Children aged 2-9 years with AD (n = 100) | Randomized, double-blind, placebo-controlled, parallel trial | Randomly allocated to the probiotics (L. casei, L. rhamnosus, L. plantarum, B. lactis) (n = 50) or placebo (n = 50) groups for 6 weeks | Probiotics successfully colonized in the intestine; but additional effects were not found |
| 10 | Wang et al.—2015 [86] | Children aged 1-18 years with moderate-to-severe AD (n = 210) | Double-blind, prospective, randomized placebo-controlled study | The groups received L. paracasei (n = 55) or L. fermentum (n = 55) or L. paracasei and L. fermentum mixture (n = 55) or placebo (n = 55) for 3 months | Supplementation of a probiotic mixture was associated with clinical improvement |
| No. of Study | Author | Patient Population (Number) | Type of Study | Intervention | Results |
|---|---|---|---|---|---|
| 1 | Roessler et al.—2008 [87] | Adults with AD (n = 15) and healthy adults (n = 15) | Double-blind, placebo-controlled, randomized cross-over study | Probiotic containing a combination of probiotics L. paracasei Lpc-37, L. acidophilus 74-2 and B. lactis DGCC 420 in healthy volunteers (n = 15) and in patients with AD (n = 15) given over 8 weeks | Probiotic bacteria transiently colonized the intestines |
| 2 | Yoshida et al.—2010 [88] | Adults with AD (n = 24) | Randomized, placebo-controlled study | Intervention group (n = 16) were given either B. breve strain YY or patients received placebo (n = 8) for 8 weeks | Probiotic was beneficial for the treatment of AD |
| 3 | Drago et al.—2012 [89] | Adult patients between 18 and 46 years with moderate-to-severe AD (n = 38) | Parallel-group double-blind placebo-controlled randomised trial | Clinical efficacy of the intake of L. salivarius LS01 (n = 19) in the treatment of adult patients with AD | Positively modified clinical and immunologic status and life quality |
| 4 | Iemoli et al.—2012 [90] | Adult AD patients (n = 48) | Randomized double-blinded active treatment versus placebo study | Intake of a combination of two probiotics: L. salivarius LS01 and B. breve BR03 for 12 weeks in the probiotic group (n = 16) | Beneficial effects for clinical and immunologic alterations |
| 5 | Matsumoto et al. [91] | Adult patients with AD (n = 44) | Randnomized controlled trial | Patients were randomly assigned to receive LKM512 (n = 22) or a placebo (n = 22) | LKM512 exerted antipruritic effects by increasing kynurenic acid production |
| 6 | Drago et al.—2014 [92] | Adult patients with AD (n = 25) | Prospective, controlled pilot trial | L. salivarius, Str. thermophilus ST10 and tara gum intake for half of participants (n = 13). The other half of the participants (n = 12) received placebo for 1 month | The combination of tara gum and probiotics increases the efficacy of other probiotic strains |
| 7 | Nakatsuji et al.—2021 [93] | Adult patients with AD (n = 54) | Double-blinded, randomized trial | 1-week trial of topical Staphylococcus hominis A9 (ShA9) or vehicle on the forearm skin of 54 adults with S. aureus-positive AD | Participants receiving ShA9 had fewer adverse events associated with AD; eczema severity was not significantly different when evaluated in all participants treated with ShA9 but a significant decrease in S. aureus and increased ShA9 DNA were seen |
| No. of Study | Author | Patient Population (Number) | Type of Study | Intervention | Results |
|---|---|---|---|---|---|
| HUMAN MODEL—PROBIOTICS ADMINISTERED ORALLY | |||||
| 1 | Vijayashankar, Raghunath.—2012 [94] | A patient with generalised pustular psoriasis (n = 1) | Case report | L. sporogene, one sachet thrice daily | In 15 days, the fever subsided, lesions started involuting and no new lesions appeared |
| 2 | Groeger et al.—2013 [95] | Patients with psoriasis (n = 26), patients with ulcerative colitis and chronic fatigue syndrome (n = 70), healthy volunteers (n = 35) | Randomized, double-blind, placebo-controlled | Sachets containing B. infantis 35264 (n = 63) or placebo containing maltodextran (n = 55) daily for 8 weeks | Significant decrease in CRP and TNF-α levels |
| 3 | Navarro-Lopez et al.— 2019 [96] | 18–70 year old adults withplaque psoriasis (n = 90) | Randomized, double-blind, placebo-controlled | Participant were randomized into probiotic (n = 45) and placebo (n = 45) groups. In the probiotic group capsule containing a mixture of 3 probiotic strains in 1:1:1 ratio (B. longum CECT 7347, B. lactis CECT 8145 and L. rhamnosus CECT 8361) was given for 12 weeks | Lower risk of relapse following the administration of probiotic bacteria, which reduced PASI75 in 66.7% of the patients. In the placebo group, 41.9% of patients showed reduction. In PGA index 48.9% of the probiotic group reached a score of 0 or 1 compared to 30.2% in the placebo group |
| ANIMAL MODEL—PROBIOTICS ADMINISTERED TOPICALLY AND ORALLY | |||||
| 4 | Chen et al.—2017 [97] | Male BALB/c; imiquimod-induced epidermal hyperplasia and psoriasis-like skin inflammation (n = 24) | Animal study | In the intervetion group mice were fed orally with differentdoses of L. pentosus GMNL-77 or with the vehicle control (distilled water) for 7 consecutive days | Improvement of skin symptoms, decreased TNF-α, IL-6, IL-23, IL-17A/F, and IL-22 levels in the skin, and reduced number of IL-17- and IL-22-producing CD4+ T cells |
| 5 | Rather et al.—2018 [98] | Mice with imiquimod-induced psoriasis-like skin inflammation (n = 30) | Animal study | Mice divided into five different groups, 6 mice each: control group, imiquimod group, imiquimod+vaseline group, imiquimod+clobetasol group, and imiquimod+ ethanolic extract of L. sakei Probio65 | Significant inhibition of imiquimod-induced skin inflammation |
| 6 | Lu et al.— 2021 [99] | Female BALB/c mice (n = 60) | Animal study | Mice were separated into 10 groups (6 included in each group): control group, imiquimod group, methotrexate positive control group and probiotic groups (seven groups); CCFM667 B. adolescentis, CCFM1078 B. breve, CCFM1148 B. animalis, CCFM1147 and CCFM1074 L. paracasei, CCFM1032 and CCFM1040 L. reuteri | Four probiotic bacteria groups ameliorated psoriasis-like pathological characteristics and suppressed the release of IL-23/T helper cell 17 axis-related inflammatory cytokines |
| 7 | Ogawa C. et al.—2021 [100] | Mice with imiquimod-induced psoriasis | Animal study | Mice were administered L. mesenteroides for 21 days alongside the topical application of imiquimod on the dorsal skin for 6 consecutive days | Suppressed erythema, scaling, upregulated IL-17 production, increased levels of plasma deoxycholic acid, altered the faecal microbiota composition |
| No. of Study | Author | Patients (Number) | Type of Study | Intervention | Results |
|---|---|---|---|---|---|
| HUMAN MODEL—PROBIOTIC SUPPLEMENTATION | |||||
| 1 | Peral et al.—2010 [101] | Patients aged 40–70 years of age; patients suffered from type 2 diabetes mellitus (n = 14); non-diabetic (n = 20); inclusion criteria: venous ulcer; infection and no signs of healing in the past 3 months, despite conventional medical treatment | Interventional study | Wounds were treated with topical applications of a whole culture of L. plantarum ATCC; the culture was applied once-daily over a period of 10 days | After 30 days of treatment, a reduction of more than 90% of the wound area was observed in 43% and 50% of the diabetic and non-diabetic patients, respectively |
| 2 | Mohseni et al.—2018 [102] | Patients aged 40-85 years old with grade 3 diabetic foot ulcer (n = 60) | Randomized, double-blind, placebo-controlled trial | Participants were randomly divided into two groups (n = 30/group) to receive either probiotic or placebo daily for 12 weeks. The probiotic mix consisted of L. acidophilus, L. casei, L. fermentum, B. bifidum | Beneficial effects on ulcer size, glycaemic control, total cholesterol, CRP, plasma nitric oxide, total antioxidant capacity and malondialdehyde levels |
| 3 | Venosi et al.—2019 [103] | 83-year-old woman with a critical limb ischemia and an infected difficult-to-treat ulcerated cutaneous lesion of the right leg | Case report | Mixture of probiotic bacteria (lyophilized powder sachets, containing Lactobacillus plantarum, Lactobacillus acidophilus and Str. thermophilus) against different bacteria species K. pneumonia, P. mirabilis and E. faecalis | Treatment was effective against the three bacteria species |
| ANIMAL MODEL—PROBIOTICS SUPPLEMENTATION AND TOPICAL APPLICATION | |||||
| 4 | Jones et al.—2012 [104] | New Zealand white rabbit (n = 4) | Animal study | The wounds were treated with control or gNO-producing patches designed to produce gNO levels. Wounds are not infected (1. and 2. rabbit) or infected (3. and 4. rabbit). Wounds are treated with placebo (1. and 3. rabbit) or with gNO producing patches (2. and 4. rabbit) | Histological analysis showed improved wound healing in gNO-producing patch-treated rabbits |
| 5 | Stefia et al.—2020 [105] | C57BL/6 wild type wounded mice (n = 30) | Randomized controlled trial in mice | Mice were wounded and divided into 3 groups (n = 10/group); receiving topical applications Pluronic gel containing either vehicle alone or the supernatant fractions prepared from F. prausnitzii strains A2-165 or AHMP21 | Probiotic can regulate wound inflammation and accelerate wound closure |
| 6 | Kusumaningsih et al.—2021 [106] | Male Wistar rats (n = 36) | Animal study | Rats were wounded and divided intor 6 groups (n = 6/group); (1) a control group over 3 days, (2) a group that used distilled water over 7 days, (3) a group that underwent topical treatment over 3 days, (4) a group that used probiotic (L. casei) administered topically over 7 days, (5) a group that underwent systemic treatment over 3 days (6) a group that took oral probiotics for the traumatic ulcers over 7 days | Significant differences were observed in the number of fibroblasts and blood vessels |
| IN VITRO STUDIES—PROBIOTICS APPLICATION | |||||
| 7 | Vågesjö et al.—2018 [107] | Human skin wound model/mice | In vitro model of wound reepithelialization | Wounds were treated daily with saline solution, control Lactobacillus reuteri or CXCL12-expressing L. reuteri or L. lacti | Promising therapeutic approach for non-healing wounds |
| 8 | Coman et al.—2020 [108] | Pathogenic bacteria were isolated from chronic ulcerative lesions | In vitro study | To evaluate probiotic efficacy of SYNBIO (1:1 combination of L. rhamnosus IMC 501 and L paracasei IMC 502) in wound infections | Good antimicrobial capacity and adhesion percentage to human keratinocyte cells and fibroblasts |
| No. of Study | Author | Patient Population (Number) | Type of Study | Intervention | Results |
|---|---|---|---|---|---|
| 1 | Guéniche et al.—2008 [109] | Volunteers aged 6 to 70 years suffering from SD (n = 60) | Prospective, double-blind, placebo-controlled | A cream containing a 5% lysate of the nonpathogenic bacteria V. filiformis (n = 30) or a vehicle cream applied once daily for 4 weeks (n = 30) | Significant improvement of SD |
| 2 | Reygagne et al.—2017 [110] | Male volunteers aged 18 to 60 years with moderate-to-severe dandruff (n = 60) | Randomized, placebo-controlled study | A sachet containing ST11 (n = 30) or a placebo (n = 30) administered orally for 56 days | Significantly reduced severity of dandruff |
| No. of Study | Author | Patient Population (Number) | Type of Study | Intervention | Results |
|---|---|---|---|---|---|
| HUMAN MODEL—PROBIOTICS ADMINISTERED ORALLY OR TOPICALLY | |||||
| 1 | Peral et al.—2009 [111] | Patients with second and third-degree burns (n = 80) | Case-control study | Patients were separated into 2 groups: in the topical probiotic group patients (n = 38) received L. plantarum ATCC 10241.In the control group patients (n = 42) received 1% SD-Ag cream for 10 days | Topical probiotic treatment of 2nd degree burn patients was as effective as SD-Ag decreasing pathogen load |
| 2 | Stefanatou et al.—[112] | 34-year-old woman suffering from extensive deep-partial and full thickness thermal burns | Case report | S. boulardii administered for nearly 2 months | Probiotic sepsis due to fungaemia in a critically ill burn patient which resulted in death |
| 3 | Thomson et al.—2012 [113] | 47-year-old lady with 54% deep-dermal and full-thickness flame burns to her neck, chest, upper abdomen and upper limbs | Case report | Oral administration of L. casei shirota for 2 weeks after infection which occurred 5 months after burn | Pathogen of the wound changed from multidrug resistant to multidrug sensitive strain |
| 4 | Mayes T et al.—2015 [114] | Less than 22 years old acutely burned patients, and were admitted/consented within 10 days of burn injury (n = 20) | Randomized, double-blind, placebo-controlled | The treatment group received LGG (n = 10). The control group received placebo (n = 10). Investigational products were administered via nasoduodenal feeding tube twice daily | Improved gastrointestinal outcomes and reduced time to wound healing |
| 5 | El-Ghazely et al. —2016 [115] | Thermally-injured pediatric patients with total body surface burns between 20-50% and depth between 5-10% (n = 40) | Randomized, double-blinded, controlled trial | Participants were separated into 2 groups; probiotic group (n = 20) received probiotic preparations of L. fermentum and L. delbrueckii and placebo control group (n = 20) | Decreased infection incidence in the probiotic group |
| 6 | Perdanakusuma et al.—2019 [116] | Burn patients (n = 16) | Randomized, placebo-controlled trial | Patients were randomized into three treatment groups. Oral administration of either a placebo, a L. reuteri probiotic, or a B. infantis 35624 probiotic for 14 consecutive days | B. infantis 35624 single-strain probiotic was not significantly superior to L. reuteri protectis in altering intestinal immunity after burns |
| 7 | Fleming et al.—2019 [117] | Burn patients aged 18 to 89, who were hospitalized for at least 2 weeks, no formal protocol of antibiotics use was estabilished (n = 108) | Retrospective study | Oral administration of >1 million colony-forming units per day of L. acidophilus and L. rhamnosus | No improvements in patient outcomes but increased incidence of diarrhea |
| ANIMAL MODEL—PROBIOTICS ADMINISTERED ORALLY | |||||
| 8 | Herek et al.—2004 [118] | Male albino rats (n = 23) | Animal study | The rats were divided into sham burn group (n = 7), burn + Ampicillin-sulbactam group (n = 8), burn + Ampicillin-sulbactam + probiotic (S. boulardii) group (n = 8) administered twice daily for 5 days | Decreased incidence of antibiotic-induced bacterial translocation |
| 9 | Gong et al.—2017 [119] | Healthy male Wistar rats (n = 60) | Animal study | The rats were divided into groups: burn model group (n = 15)—normal saline; glutamine treatment group (n = 15)—glutamine + normal saline; probiotics treatment group (n = 15)—probiotic + normal saline; glutamine and probiotics combined treatment group (n = 15)—glutamine + normal saline. All were administered once daily for 7 days | Glutamine and probiotics together significantly inhibited nitric oxide (NO) content and reduced levels of the inflammatory factors |
| ANIMAL MODEL—PROBIOTICS ADMINISTERED TOPICALLY OR LOCALLY | |||||
| 10 | Valdez et al.—2005 [120] | Adult inbred BALB/c mice | Animal study | L. plantarum ATCC 10241 injection into burned area on 3, 4, 5, 7 and 9 days | Samples from skin, liver and spleen taken after 5, 10 and 15 days demonstrated inhibition of P. aeruginosa colonisation |
| 11 | Brachkova et al.—2011 [121] | Male Wistar rats (n = 25) | Animal study | Rats were randomly allocated into groups: non-burned control rats (n = 2); burned control rats (n = 6); burned skin covered with films containing L. plantarum (n = 3); burned skin on to with a suspension of P. aeruginosa (n = 7); burned skin, contaminated with P. aeruginosa, and covered with films containing L. plantarum ATCC 8014(7) | Reduction of pathogen load |
| 12 | Argenta et al. —2016 [122] | Female C57 BL/b mice (n = 38) | Animal study | The mice were divided into groups. Injured sites were treated with vehicle (burn wound control), probiotics (L. plantarum ATCC 1024) only, pathogenic bacteria (P. aeruginosa) only, or probiotics + pathogen (Lactobacillus and P. aeruginosa) for five days | Lower mortality rate and inhibition of pathogenic bacteria |
| 13 | Satish et al.—2017 [123] | Male Dutch Belted rabbits | Animal study | Each rabbit had four burn wounds created on its dorsum-the four burn wound conditions therefore were: (1) Burn wound only; (2) L. plantarum ATCC 10241 only; (3) P. aeruginosa only; (4) L. plantarum + P. aeruginosa | Curtailed severity and length of infection, reduced scarring |
| 14 | Sürmeli et al.—2019 [124] | Rats (n = 35) | Animal study | Rats were divided into groups (n = 7/group): control group; L. plantarum applied immediately after the burn and then MRSA inoculated; MRSA applied immediately after the burn and then L. plantarum inoculated; control of L. plantarum; control of MRSA | Probiotic showed protective role in non-infected burn wounds |
| 15 | Khan et al.—2019 [125] | Male BALB/c mice (n = 30) | Animal study | The mice were randomized into negative (untreated), positive (silver sulfadiazine cream), vehicle (biodispersion and nanoscaffold), and experimental bioscaffold groups (n = 6/group). Treatments were applied locally on 2, 6, 10, and 14 days postburn–application of probiotic (E. mundtii QAUEM2808) | Accelerated epithelialization, collagen deposition, and hair follicle formation and inhibit pathogens |
| HUMAN MODEL–PREBIOTICS OR PREBIOTICS and PROBIOTICS ADMINISTERED ORALLY | |||||
| 16 | Olguin et al.—2005 [126] | Burn patients (n = 21) | Randomized, double-blind, placebo-controlled | 6 g of oligofructose (study group) or sucrose as placebo (control group) during 15 days | No effect on gastrointestinal permeability |
| No. of Study | Author | Patient Population (Number) | Type of Study | Intervention | Results |
|---|---|---|---|---|---|
| HUMAN MODEL–PROBIOTICS OR PREBIOTICS ORAL SUPPLEMENTATION | |||||
| 1 | Kim et al.—2010 [35] | Patients with acne (n = 36) | Randomized, double-blind, placebo-controlled study | Fermented milk with lactoferrin daily (n = 18) or fermented milk only (n = 18) for 12 weeks supplemented orally | Improvement of acne with a selective decrease of triacylglycerols in skin surface lipids |
| 2 | Fabroccini et al.—2016 [127] | Patients with acne (n = 20) | Placebo–controlled trial | Over a 12-week period, the probiotic group (n = 10) consumed a liquid supplement containing LSP1, placebo group (n = 10) | Normalised skin expression of genes involved in insulin signalling and improvement of acne |
| 3 | Dall’Oglio et al.—2018 [128] | Female patients with mild to moderate acne (n = 12) | Proof of concept pilot trial | Prebiotic oral supplementation with food supplement containing FOS and GOS for 3 months | Positive effects on glycemic and lipid metabolic parameters |
| 4 | Rahmayani et al.—2019 [129] | Patients with acne aged between 17 and 25 years old (n = 33) | Pre-experimental clinical study with a pretest-posttest design | Oral mix of probiotics was given to individuals for 30 days-B. lactis W51, B. lactis W52, L. acidophilus W55, L. casei W56, L. W57, L. lactis W58 | Elevated serum IL-10 levels |
| HUMAN MODEL–PREBIOBIOTICS OR PREBIOTICS TOPICAL APPLICATION | |||||
| 5 | Kang et al.—2009 [130] | 12 years of age or older patients with acne (n = 70) | Double-blind, randomized, placebo-controlled trial | E. faecalis SL-5 lotion (n = 35) or placebo lotion (n = 35) to apply twice a day for 8 weeks | Reduced number of inflammatory lesions |
| 6 | AOBiome LLC.—2019 [131] | Adult patients with mild to moderate acne (n = 358) | Double-blind, randomized, placebo-controlled trial | Probiotic (N. eutropha) or placebo spray to saturate the entire face in the morning and at night for 12 weeks | 2-point reduction in IGA of acne severity compared to vehicle control |
| 7 | De Los Angeles Mosquera Tayupanta et al.—2019 [132] | Patients from 15 to 20 years old, with previous diagnosis of type II acne (n = 20) | Interventional study | First the evaluation of the in vitro antagonistic effect of L. acidophilus against C. acnes was performed, then topical application | Decrease in the population of C. acnes |
| IN VITRO STUDIES | |||||
| 8 | Al-Ghazzewi et al.—2010 [133] | - | In vitro study | The synbiotic ability of probiotic bacteria and konjac glucomannan hydrolysates to inhibit acne-inducing bacterium, C. acnes growth was studied in vitro | Inhibition of the growth of C. acnes, which was significantly enhanced by the presence of prebiotic |
| 9 | Kang et al.—2012 [134] | - | In vitro study | Study examined the effects of L. reuteri strains (KCTC 3594, KCTC 3678, KCTC 3679) on the proliferation of C. acnes and S. epidermidis | Control of the growth of bacteria involved in acne inflammation and prevent acne |
| 10 | Lee et al.—2012 [135] | - | In vitro study | Activity of Bifidobacterium spp. against C. acnes KCTC3320 using the co-culture method was investigated | Bifidobacterium spp. could be used as an effective treatment and reduced the risk of acne development |
| 11 | Khalfallah et al.—2021 [136] | - | In vitro study | Two type of Str. salivarius strains and one L. plantarum were tested for production of antimicrobials-target organisms used were C. acnes, S. aureus, and P. aeruginosa | Probiotic containing could be topically applied without the need for a regular antibiotic treatment or as an adjunctive therapy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polak, K.; Jobbágy, A.; Muszyński, T.; Wojciechowska, K.; Frątczak, A.; Bánvölgyi, A.; Bergler-Czop, B.; Kiss, N. Microbiome Modulation as a Therapeutic Approach in Chronic Skin Diseases. Biomedicines 2021, 9, 1436. https://doi.org/10.3390/biomedicines9101436
Polak K, Jobbágy A, Muszyński T, Wojciechowska K, Frątczak A, Bánvölgyi A, Bergler-Czop B, Kiss N. Microbiome Modulation as a Therapeutic Approach in Chronic Skin Diseases. Biomedicines. 2021; 9(10):1436. https://doi.org/10.3390/biomedicines9101436
Chicago/Turabian StylePolak, Karina, Antal Jobbágy, Tomasz Muszyński, Kamila Wojciechowska, Aleksandra Frątczak, András Bánvölgyi, Beata Bergler-Czop, and Norbert Kiss. 2021. "Microbiome Modulation as a Therapeutic Approach in Chronic Skin Diseases" Biomedicines 9, no. 10: 1436. https://doi.org/10.3390/biomedicines9101436