Differential Role of Circulating microRNAs to Track Progression and Pre-Symptomatic Stage of Chronic Heart Failure: A Pilot Study

 , , , , , , ,
, , , , , , , 
Abstract
:1. Introduction
2. Experimental Section
2.1. Patients
2.2. Natriuretic Peptide
2.3. Total RNA Purification
2.4. MicroRNA Screening
2.5. Single miRNA Assays
2.6. Statistical Analysis
3. Results
3.1. Study Population Characteristics
3.2. Correlation between NYHA Class, LVEDV, and NT-proBNP Levels
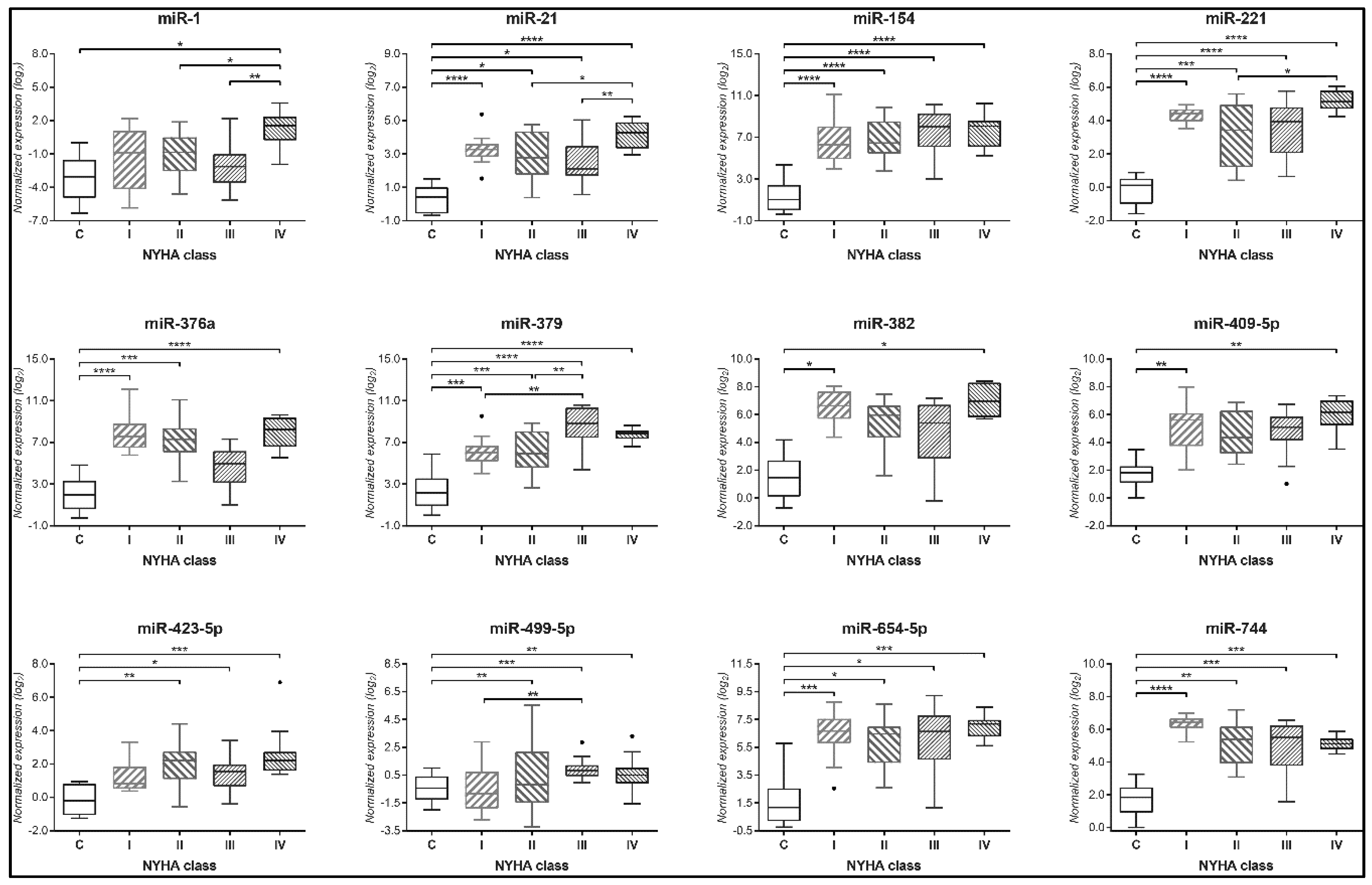
3.3. Circulating miRNAs Expression and in Relation with NYHA Class
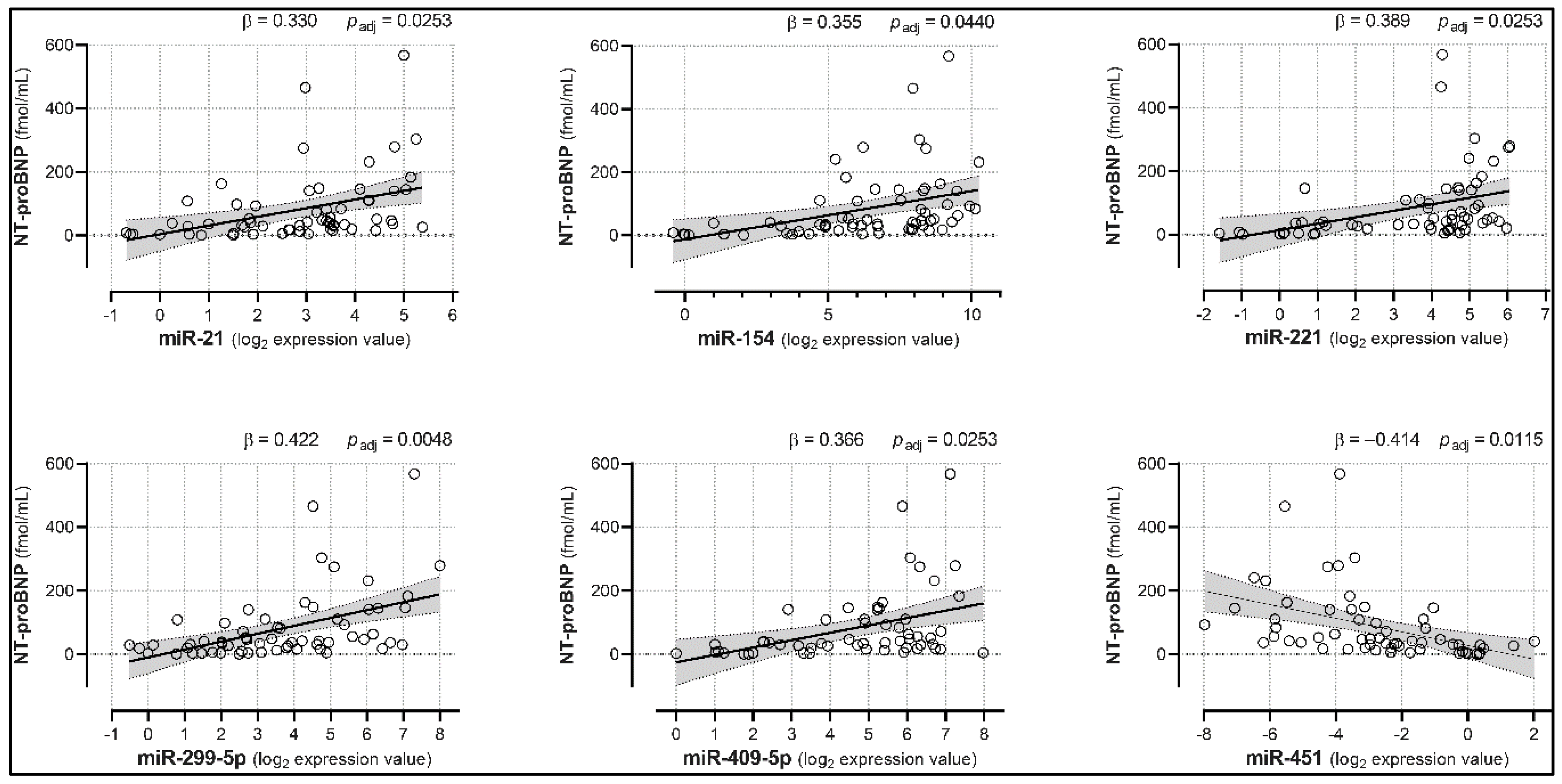
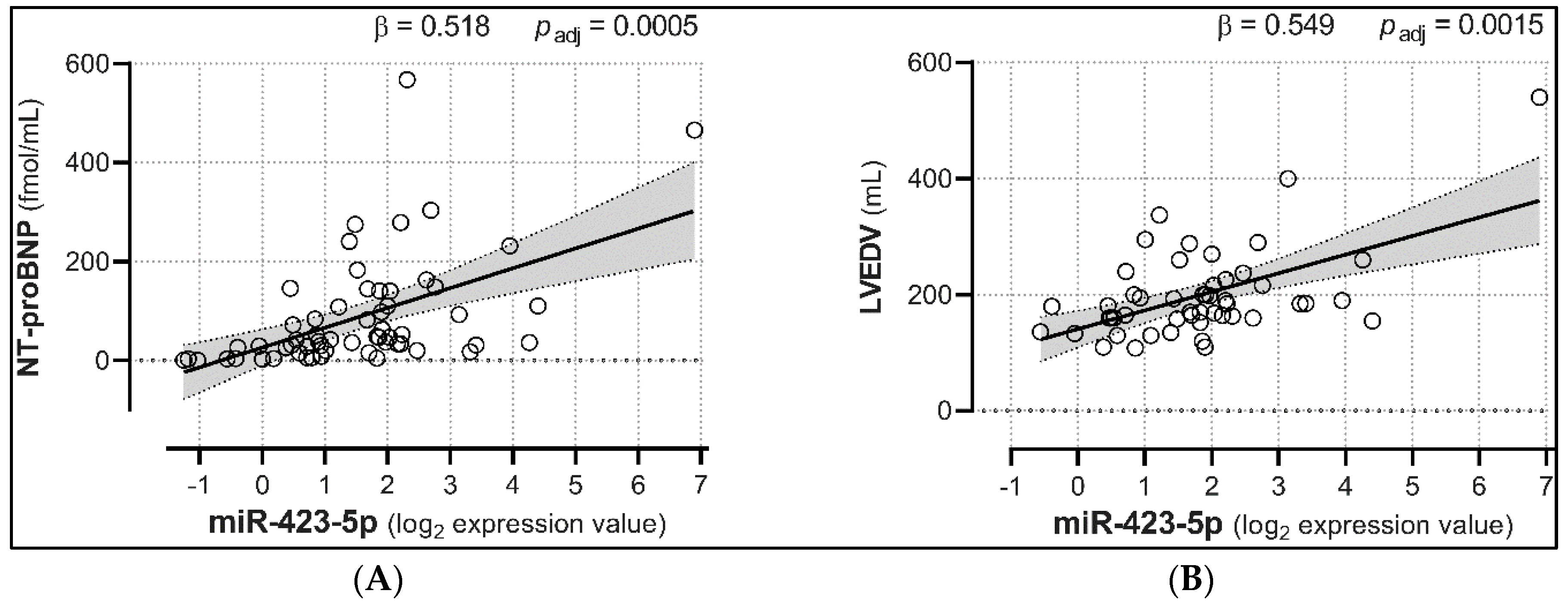
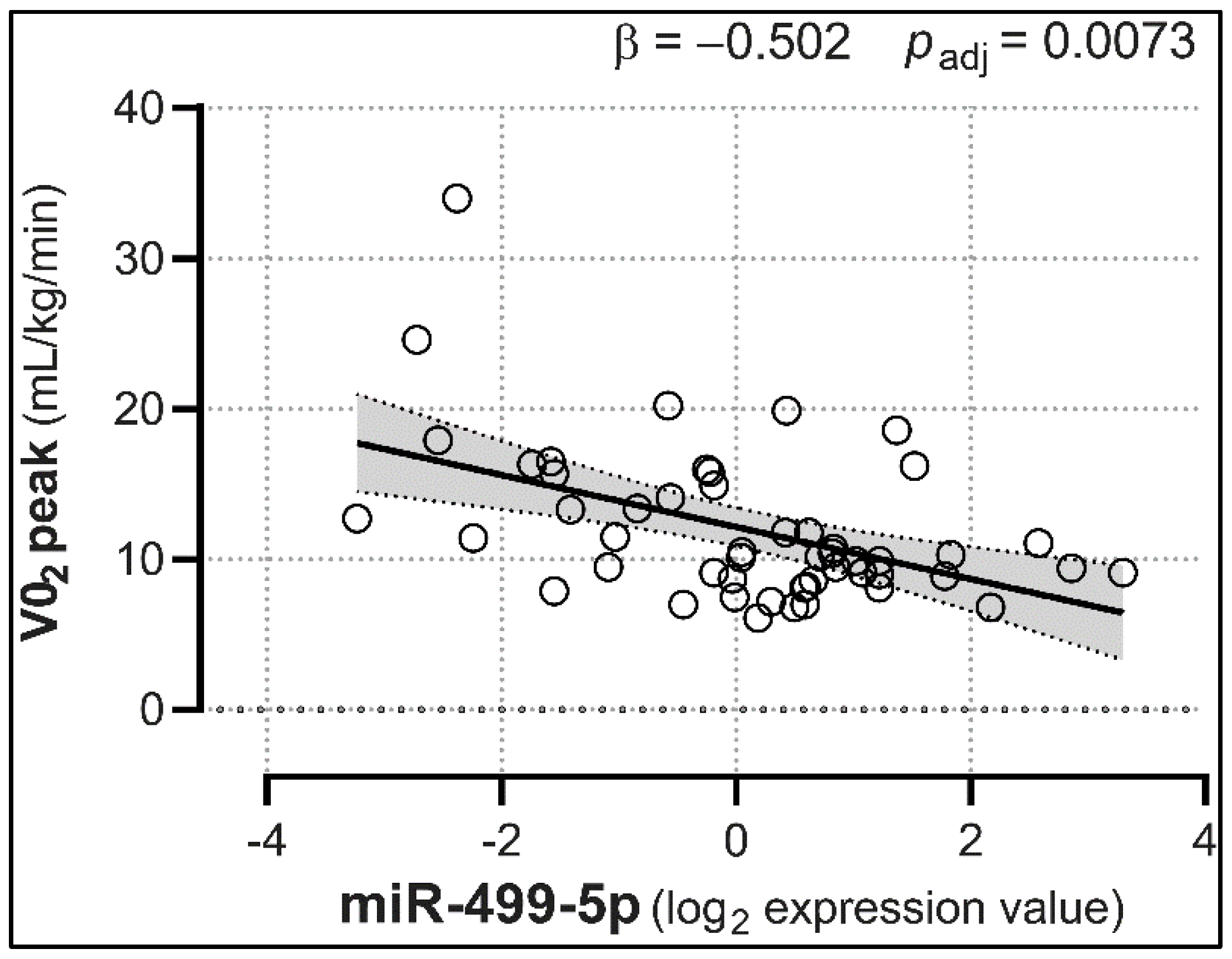
3.4. Correlation between Plasma miRNA Levels and NT-proBNP, LVEDV, and VO2 Peak
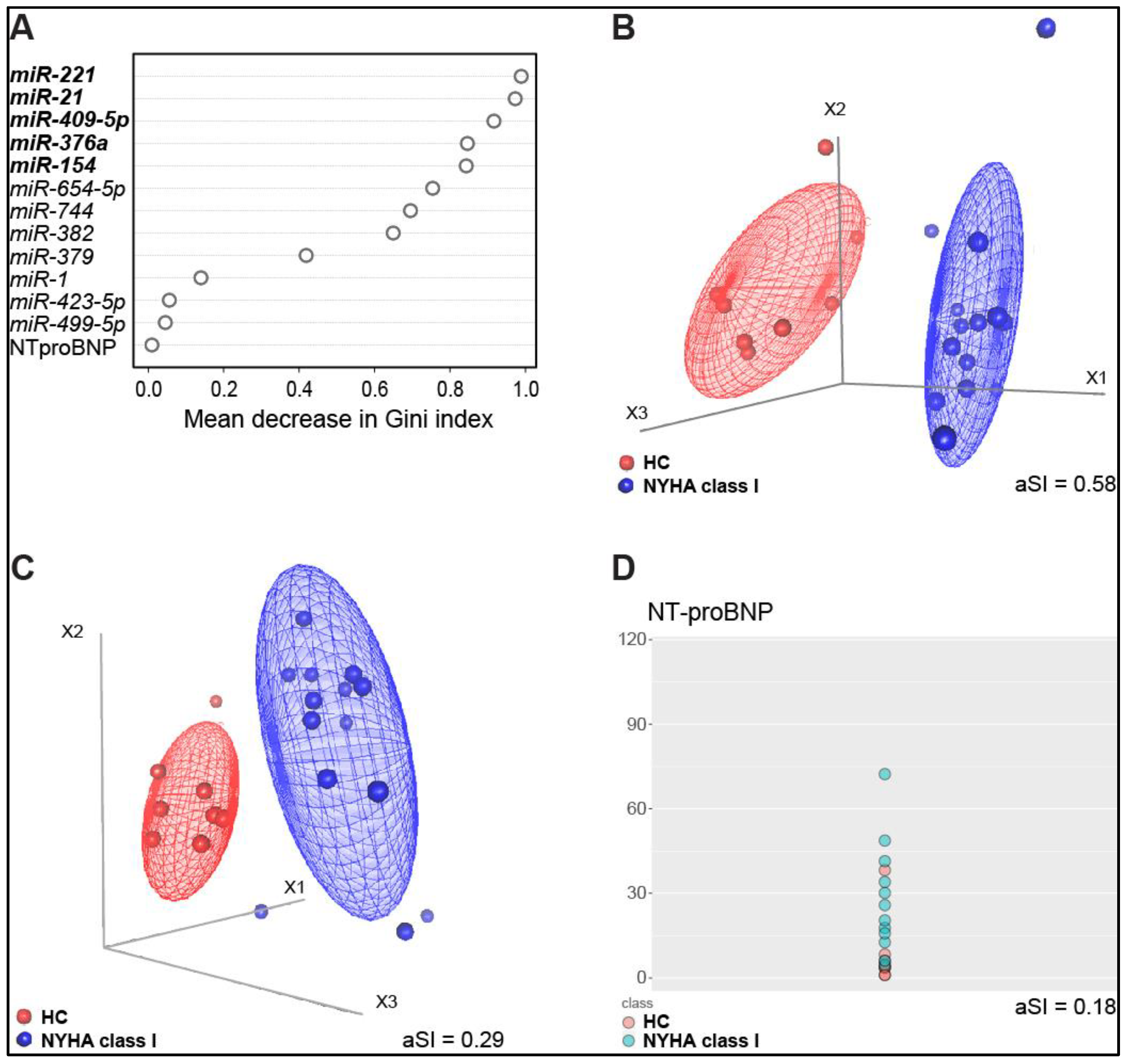
3.5. Identification of a miRNA Signature of Early-Stage CHF
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Maalouf, R.; Bailey, S. A review on B-type natriuretic peptide monitoring: Assays and biosensors. Heart Fail. Rev. 2016, 21, 567–578. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failureThe Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Brunner-La Rocca, H.-P.; Sanders-van Wijk, S. Natriuretic Peptides in Chronic Heart Failure. Card. Fail. Rev. 2019, 5, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Maisel, A.; Mueller, C.; Adams, K.; Anker, S.D.; Aspromonte, N.; Cleland, J.G.F.; Cohen-Solal, A.; Dahlstrom, U.; DeMaria, A.; Di Somma, S.; et al. State of the art: Using natriuretic peptide levels in clinical practice. Eur. J. Heart Fail. 2008, 10, 824–839. [Google Scholar] [CrossRef] [PubMed]
- Gaggin, H.K.; Januzzi, J.L. Biomarkers and diagnostics in heart failure. Biochim. Biophys. Acta 2013, 1832, 2442–2450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, W.L.; Jaffe, A.S. Biomarkers in heart failure: The importance of inconvenient details. ESC Heart Fail. 2016, 3, 3–10. [Google Scholar] [CrossRef] [PubMed]
- D’Elia, E.; Vaduganathan, M.; Gori, M.; Gavazzi, A.; Butler, J.; Senni, M. Role of biomarkers in cardiac structure phenotyping in heart failure with preserved ejection fraction: Critical appraisal and practical use. Eur. J. Heart Fail. 2015, 17, 1231–1239. [Google Scholar] [CrossRef]
- Correale, M.; Monaco, I.; Brunetti, N.D.; Di Biase, M.; Metra, M.; Nodari, S.; Butler, J.; Gheorghiade, M. Master Program Students on Drug Development for Heart Failure Redefining biomarkers in heart failure. Heart Fail. Rev. 2018, 23, 237–253. [Google Scholar] [CrossRef]
- Cortez, M.A.; Bueso-Ramos, C.; Ferdin, J.; Lopez-Berestein, G.; Sood, A.K.; Calin, G.A. MicroRNAs in body fluids--the mix of hormones and biomarkers. Nat. Rev. Clin. Oncol. 2011, 8, 467–477. [Google Scholar] [CrossRef] [Green Version]
- Iguchi, H.; Kosaka, N.; Ochiya, T. Secretory microRNAs as a versatile communication tool. Commun. Integr. Biol. 2010, 3, 478–481. [Google Scholar] [CrossRef]
- Wang, J.; Chen, J.; Sen, S. MicroRNA as Biomarkers and Diagnostics. J. Cell. Physiol. 2016, 231, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Fichtlscherer, S.; Zeiher, A.M.; Dimmeler, S. Circulating microRNAs: Biomarkers or mediators of cardiovascular diseases? Arterioscler. Thromb. Vasc. Biol. 2011, 31, 2383–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Alessandra, Y.; Devanna, P.; Limana, F.; Straino, S.; Di Carlo, A.; Brambilla, P.G.; Rubino, M.; Carena, M.C.; Spazzafumo, L.; De Simone, M.; et al. Circulating microRNAs are new and sensitive biomarkers of myocardial infarction. Eur. Heart J. 2010, 31, 2765–2773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sommariva, E.; D’Alessandra, Y.; Farina, F.M.; Casella, M.; Cattaneo, F.; Catto, V.; Chiesa, M.; Stadiotti, I.; Brambilla, S.; Dello Russo, A.; et al. MiR-320a as a Potential Novel Circulating Biomarker of Arrhythmogenic CardioMyopathy. Sci. Rep. 2017, 7, 4802. [Google Scholar] [CrossRef] [PubMed]
- Stadiotti, I.; Pompilio, G.; Maione, A.S.; Pilato, C.A.; D’Alessandra, Y.; Sommariva, E. Arrhythmogenic cardiomyopathy: What blood can reveal? Heart Rhythm. 2019, 16, 470–477. [Google Scholar] [CrossRef] [Green Version]
- Tijsen, A.J.; Pinto, Y.M.; Creemers, E.E. Circulating microRNAs as diagnostic biomarkers for cardiovascular diseases. Am. J. Physiol. Heart Circ. Physiol. 2012, 303, H1085–H1095. [Google Scholar] [CrossRef] [Green Version]
- McManus, D.D.; Lin, H.; Tanriverdi, K.; Quercio, M.; Yin, X.; Larson, M.G.; Ellinor, P.T.; Levy, D.; Freedman, J.E.; Benjamin, E.J. Relations between circulating microRNAs and atrial fibrillation: Data from the Framingham Offspring Study. Heart Rhythm. 2014, 11, 663–669. [Google Scholar] [CrossRef] [Green Version]
- Olivieri, F.; Antonicelli, R.; Lorenzi, M.; D’Alessandra, Y.; Lazzarini, R.; Santini, G.; Spazzafumo, L.; Lisa, R.; La Sala, L.; Galeazzi, R.; et al. Diagnostic potential of circulating miR-499-5p in elderly patients with acute non ST-elevation myocardial infarction. Int. J. Cardiol. 2013, 167, 531–536. [Google Scholar] [CrossRef]
- Tijsen, A.J.; Creemers, E.E.; Moerland, P.D.; de Windt, L.J.; van der Wal, A.C.; Kok, W.E.; Pinto, Y.M. MiR423-5p as a circulating biomarker for heart failure. Circ. Res. 2010, 106, 1035–1039. [Google Scholar] [CrossRef]
- Masson, S.; Batkai, S.; Beermann, J.; Bär, C.; Pfanne, A.; Thum, S.; Magnoli, M.; Balconi, G.; Nicolosi, G.L.; Tavazzi, L.; et al. Circulating microRNA-132 levels improve risk prediction for heart failure hospitalization in patients with chronic heart failure. Eur. J. Heart Fail. 2018, 20, 78–85. [Google Scholar] [CrossRef]
- Yan, H.; Ma, F.; Zhang, Y.; Wang, C.; Qiu, D.; Zhou, K.; Hua, Y.; Li, Y. miRNAs as biomarkers for diagnosis of heart failure: A systematic review and meta-analysis. Medicine (Baltimore) 2017, 96, e6825. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandra, Y.; Carena, M.C.; Spazzafumo, L.; Martinelli, F.; Bassetti, B.; Devanna, P.; Rubino, M.; Marenzi, G.; Colombo, G.I.; Achilli, F.; et al. Diagnostic potential of plasmatic MicroRNA signatures in stable and unstable angina. PLoS ONE 2013, 8, e80345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rousseeuw, P.J. Silhouettes: A graphical aid to the interpretation and validation of cluster analysis. J. Comput. Appl. Math. 1987, 20, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Triposkiadis, F.; Butler, J.; Abboud, F.M.; Armstrong, P.W.; Adamopoulos, S.; Atherton, J.J.; Backs, J.; Bauersachs, J.; Burkhoff, D.; Bonow, R.O.; et al. The continuous heart failure spectrum: Moving beyond an ejection fraction classification. Eur. Heart J. 2019, 40, 2155–2163. [Google Scholar] [CrossRef] [PubMed]
- Carè, A.; Catalucci, D.; Felicetti, F.; Bonci, D.; Addario, A.; Gallo, P.; Bang, M.-L.; Segnalini, P.; Gu, Y.; Dalton, N.D.; et al. MicroRNA-133 controls cardiac hypertrophy. Nat. Med. 2007, 13, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Lafferty-Whyte, K.; Cairney, C.J.; Jamieson, N.B.; Oien, K.A.; Keith, W.N. Pathway analysis of senescence-associated miRNA targets reveals common processes to different senescence induction mechanisms. Biochim. Biophys. Acta 2009, 1792, 341–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goren, Y.; Kushnir, M.; Zafrir, B.; Tabak, S.; Lewis, B.S.; Amir, O. Serum levels of microRNAs in patients with heart failure. Eur. J. Heart Fail. 2012, 14, 147–154. [Google Scholar] [CrossRef]
- Goldraich, L.A.; Martinelli, N.C.; Matte, U.; Cohen, C.; Andrades, M.; Pimentel, M.; Biolo, A.; Clausell, N.; Rohde, L.E. Transcoronary gradient of plasma microRNA 423-5p in heart failure: Evidence of altered myocardial expression. Biomarkers 2014, 19, 135–141. [Google Scholar] [CrossRef]
- Luo, P.; Zhang, W. MicroRNA-423-5p mediates H2O2-induced apoptosis in cardiomyocytes through O-GlcNAc transferase. Mol. Med. Rep. 2016, 14, 857–864. [Google Scholar] [CrossRef]
- Verjans, R.; Peters, T.; Beaumont, F.J.; van Leeuwen, R.; van Herwaarden, T.; Verhesen, W.; Munts, C.; Bijnen, M.; Henkens, M.; Diez, J.; et al. MicroRNA-221/222 Family Counteracts Myocardial Fibrosis in Pressure Overload-Induced Heart Failure. Hypertension 2018, 71, 280–288. [Google Scholar] [CrossRef]
- Liang, H.; Zhang, C.; Ban, T.; Liu, Y.; Mei, L.; Piao, X.; Zhao, D.; Lu, Y.; Chu, W.; Yang, B. A novel reciprocal loop between microRNA-21 and TGFβRIII is involved in cardiac fibrosis. Int. J. Biochem. Cell Biol. 2012, 44, 2152–2160. [Google Scholar] [CrossRef] [PubMed]
- Villar, A.V.; García, R.; Merino, D.; Llano, M.; Cobo, M.; Montalvo, C.; Martín-Durán, R.; Hurlé, M.A.; Nistal, J.F. Myocardial and circulating levels of microRNA-21 reflect left ventricular fibrosis in aortic stenosis patients. Int. J. Cardiol. 2013, 167, 2875–2881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, Q.; Li, L.; Zhao, J.; Sun, Y.; Yang, H. MiRNA Expression Profile of the Myocardial Tissue of Pigs with Coronary Microembolization. Cell. Physiol. Biochem. 2017, 43, 1012–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, L.-Y.; Bie, Z.-D.; Zhang, C.-H.; Li, H.; Li, L.-D.; Yang, J. MiR-154 directly suppresses DKK2 to activate Wnt signaling pathway and enhance activation of cardiac fibroblasts. Cell Biol. Int. 2016, 40, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Josson, S.; Gururajan, M.; Sung, S.Y.; Hu, P.; Shao, C.; Zhau, H.E.; Liu, C.; Lichterman, J.; Duan, P.; Li, Q.; et al. Stromal fibroblast-derived miR-409 promotes epithelial-to-mesenchymal transition and prostate tumorigenesis. Oncogene 2015, 34, 2690–2699. [Google Scholar] [CrossRef]
- Marfella, R.; Di Filippo, C.; Potenza, N.; Sardu, C.; Rizzo, M.R.; Siniscalchi, M.; Musacchio, E.; Barbieri, M.; Mauro, C.; Mosca, N.; et al. Circulating microRNA changes in heart failure patients treated with cardiac resynchronization therapy: Responders vs. non-responders. Eur. J. Heart Fail. 2013, 15, 1277–1288. [Google Scholar] [CrossRef] [Green Version]
- Sardu, C.; Barbieri, M.; Rizzo, M.R.; Paolisso, P.; Paolisso, G.; Marfella, R. Cardiac Resynchronization Therapy Outcomes in Type 2 Diabetic Patients: Role of MicroRNA Changes. J. Diabetes Res. 2016, 7292564. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | NYHA I (n = 14) | NYHA II (n = 17) | NYHA III (n = 16) | NYHA IV (n = 14) | p-Value | HC (n = 10) | p-Value |
|---|---|---|---|---|---|---|---|
| Age, years | 64 ± 6.4 | 70.8 ± 10.4 | 69.2 ± 10.4 | 68.4 ± 8.6 | 0.23 | 62.7 ± 2.3 | 0.08 |
| Male sex, n (%) | 11 (79%) | 10 (59%) | 11 (69%) | 9 (64%) | 0.71 | 9 (90%) | 0.47 |
| NT-proBNP, fmol/mL | 27.5 ± 19.5 | 66.2 ± 51.4 | 60.3 ± 41 | 221.6 ± 153.3 | <0.001 | 18.3 ± 35.9 | <0.001 |
| Current smoker, n (%) | 8 (57%) | 8 (47%) | 11 (69%) | 8 (57%) | 0.72 | 0 (0%) | |
| CAD familiarity, n (%) | 6 (43%) | 9 (53%) | 8 (50%) | 5 (36%) | 0.8 | 0 (0%) | |
| Ischemic aetiology, n (%) | 10 (71%) | 10 (63%) | 12 (75%) | 9 (64%) | 0.9 | 0 (0%) | |
| Hypertension, n (%) | 7 (50%) | 10 (59%) | 12 (75%) | 5 (36%) | 0.18 | 0 (0%) | |
| Hypercholesterolemia, n (%) | 11 (79%) | 12 (71%) | 11 (69%) | 5 (36%) | 0.1 | 0 (0%) | |
| Diabetes, n (%) | 4 (29%) | 4 (24%) | 5 (31%) | 8 (57%) | 0.26 | 0 (0%) | |
| LVEDV, mL | 163.2 ± 45.2 | 174.9 ± 58.7 | 189.9 ± 65.9 | 242.9 ± 99.4 | 0.02 | NA | |
| LVEDD, mm | 59.3 ± 5.3 | 61.9 ± 8.8 | 62.3 ± 9.2 | 64.8 ± 8.8 | 0.4 | NA | |
| LVEF, % | 38.2 ± 4.4 | 35.6 ± 8.6 | 32.1 ± 7.4 | 24.4 ± 7.3 | <0.001 | NA | |
| PAP, mmHg | 31.2 ± 5.8 | 35.9 ± 15.6 | 32.4 ± 5.7 | 42.1 ± 13.2 | 0.23 | NA | |
| VO2 peak, mL/kg/min | 16.4 ± 6.9 | 15.2 ± 3.3 | 9.9 ± 0.9 | 7.9 ± 1 | <0.001 | NA | |
| ACEIs, n (%) | 11 (79%) | 12 (71%) | 12 (75%) | 7 (50%) | 0.37 | 0 (0%) | |
| ARAs, n (%) | 3 (25%) | 6 (50%) | 4 (25%) | 8 (57%) | 0.2 | 0 (0%) | |
| ARBs, n (%) | 9 (%) | 12 (53%) | 12 (69%) | 7 (43%) | 0.54 | 0 (0%) | |
| Beta blockers, n (%) | 13 (93%) | 16 (94%) | 13 (81%) | 13 (93%) | 0.67 | 0 (0%) | |
| Calcium antagonists, n (%) | 3 (21%) | 1 (6%) | 1 (6%) | 0 (0%) | 0.25 | 0 (0%) | |
| Digitalis, n (%) | 2 (14%) | 4 (24%) | 7 (44%) | 5 (36%) | 0.32 | 0 (0%) | |
| Diuretics, n (%) | 9 (64%) | 15 (88%) | 14 (88%) | 14 (100%) | 0.06 | 0 (0%) | |
| Nitrates, n (%) | 2 (14%) | 3 (17%) | 6 (38%) | 2 (14%) | 0.39 | 0 (0%) | |
| PUFAs, n (%) | 9 (64%) | 7 (41%) | 7 (44%) | 5 (36%) | 0.48 | 0 (0%) | |
| Statins, n (%) | 8 (57%) | 9 (53%) | 11 (69%) | 6 (43%) | 0.59 | 0 (0%) |
| microRNA | B | SE | 95% CI for B | β | 95% CI for β | p-Value | padj |
|---|---|---|---|---|---|---|---|
| Mir-1 | 11.810 | 5.35 | 1.089, 22.53 | 0.264 | 0.024, 0.504 | 0.03149 | 0.05353 |
| Mir-124a | −3.040 | 5.22 | −13.508, 7.44 | −0.073 | −0.325, 0.179 | 0.56355 | 0.59635 |
| Mir-154 | 14.120 | 5.80 | 2.504, 25.74 | 0.355 | 0.063, 0.646 | 0.01813 | 0.04403 |
| Mir-21 | 22.630 | 8.31 | 5.96, 39.29 | 0.330 | 0.087, 0.572 | 0.00874 | 0.02533 |
| Mir-221 | 20.732 | 7.54 | 5.61, 35.85 | 0.389 | 0.105, 0.672 | 0.00815 | 0.02533 |
| Mir-299-5p | 21.906 | 5.97 | 9.934, 33.88 | 0.422 | 0.191, 0.652 | 0.00056 | 0.00476 |
| Mir-331-5p | −5.860 | 11.00 | −27.949, 16.23 | −0.080 | −0.381, 0.221 | 0.59635 | 0.59635 |
| Mir-375 | −17.890 | 8.04 | −34.003, −1.77 | −0.261 | −0.496, −0.026 | 0.03025 | 0.05353 |
| Mir-376a | 10.810 | 4.78 | 1.216, 20.4 | 0.284 | 0.032, 0.536 | 0.02796 | 0.05353 |
| Mir-379 | 12.700 | 6.09 | 0.49, 24.91 | 0.295 | 0.011, 0.578 | 0.04178 | 0.05464 |
| Mir-382 | 11.750 | 5.45 | 0.757, 22.74 | 0.387 | 0.025, 0.748 | 0.03676 | 0.05464 |
| Mir-409-5p | 20.970 | 7.70 | 5.492, 36.44 | 0.366 | 0.096, 0.636 | 0.00894 | 0.02533 |
| Mir-423-5p | 40.190 | 8.69 | 22.74, 57.63 | 0.518 | 0.293, 0.743 | 0.00003 | 0.00051 |
| Mir-451 | −20.150 | 6.20 | −32.59, −7.71 | −0.414 | −0.669, −0.158 | 0.00203 | 0.01150 |
| Mir-499-5p | 5.520 | 9.62 | −13.788, 24.82 | 0.070 | −0.176, 0.316 | 0.56890 | 0.59635 |
| Mir-654-5p | 15.130 | 7.17 | 0.759, 29.5 | 0.318 | 0.016, 0.621 | 0.03945 | 0.05464 |
| Mir-744 | 6.140 | 7.25 | −8.504, 20.78 | 0.148 | −0.205, 0.501 | 0.40244 | 0.48868 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Alessandra, Y.; Chiesa, M.; Carena, M.C.; Beltrami, A.P.; Rizzo, P.; Buzzetti, M.; Ricci, V.; Ferrari, R.; Fucili, A.; Livi, U.; et al. Differential Role of Circulating microRNAs to Track Progression and Pre-Symptomatic Stage of Chronic Heart Failure: A Pilot Study. Biomedicines 2020, 8, 597. https://doi.org/10.3390/biomedicines8120597
D’Alessandra Y, Chiesa M, Carena MC, Beltrami AP, Rizzo P, Buzzetti M, Ricci V, Ferrari R, Fucili A, Livi U, et al. Differential Role of Circulating microRNAs to Track Progression and Pre-Symptomatic Stage of Chronic Heart Failure: A Pilot Study. Biomedicines. 2020; 8(12):597. https://doi.org/10.3390/biomedicines8120597
Chicago/Turabian StyleD’Alessandra, Yuri, Mattia Chiesa, Maria Cristina Carena, Antonio Paolo Beltrami, Paola Rizzo, Marta Buzzetti, Veronica Ricci, Roberto Ferrari, Alessandro Fucili, Ugolino Livi, and et al. 2020. "Differential Role of Circulating microRNAs to Track Progression and Pre-Symptomatic Stage of Chronic Heart Failure: A Pilot Study" Biomedicines 8, no. 12: 597. https://doi.org/10.3390/biomedicines8120597