
Macroscopic and Microscopic Cerebral Findings in Drug and Alcohol Abusers: The Point of View of the Forensic Pathologist

 , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
- Neuronal and axonal injury, which is due to an impaired axoplasmic transport [1] that causes an isolated neuropathy or polyneuropathy (cf. toxic neuropathy). Neuronal and axonal injury are typical alterations found in aluminum, acrylamide, colchicine, organophosphate or alcohol poisoning.
- Cerebral edema [2], represented by cytotoxic edema, resulting from injury of the membrane enzyme system and/or membrane damage, and vascular edema caused by alcohol. Two types of edemas may occur sequentially or simultaneously. Cytotoxic edema predominates in gray matter, and is characterized by astrocytic swelling and enlargement of perineuronal and perivascular spaces (indicative of the swelling of astrocytic foot processes around neurons, capillaries, and arterioles). The hallmarks of vasogenic edema include swelling of pericapillary astrocytic processes and of oligodendrocyte cytoplasm. In addition, it can also be present a spread of exudate in the extracellular space of white matter. Macroscopically, vasogenic edema induces a slight green discoloration of the white matter. Histologically, edema (particularly the vasogenic edema), features extensive cytoplasmic vacuolation in the white matter [3].
- Injury of the white matter, which is a structural alteration of cerebral white matter, in which myelin suffers the most damage (i.e., leukoencephalopathy). Toxic leukoencephalopathy may be caused by exposure to a wide variety of agents, including drugs, anti-neoplastic agents, antimicrobial agents and environmental toxins [7].
2. Methods
2.1. Database Search Terms and Timeline
2.2. Inclusion and Exclusion Criteria
2.3. Quality Assessment and Data Extrapolation
3. Neuropathological Investigations
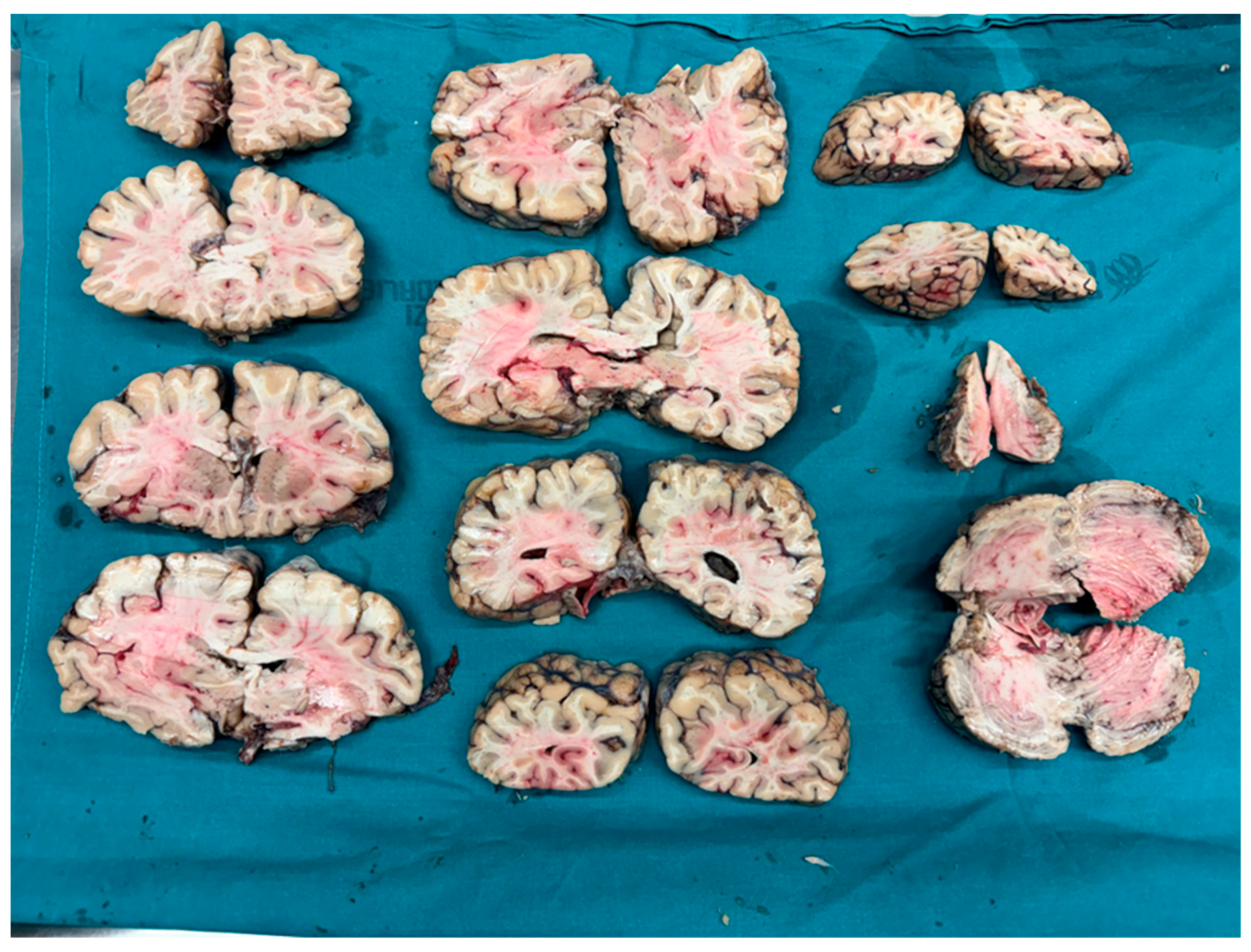
Brain Removal and Dissection
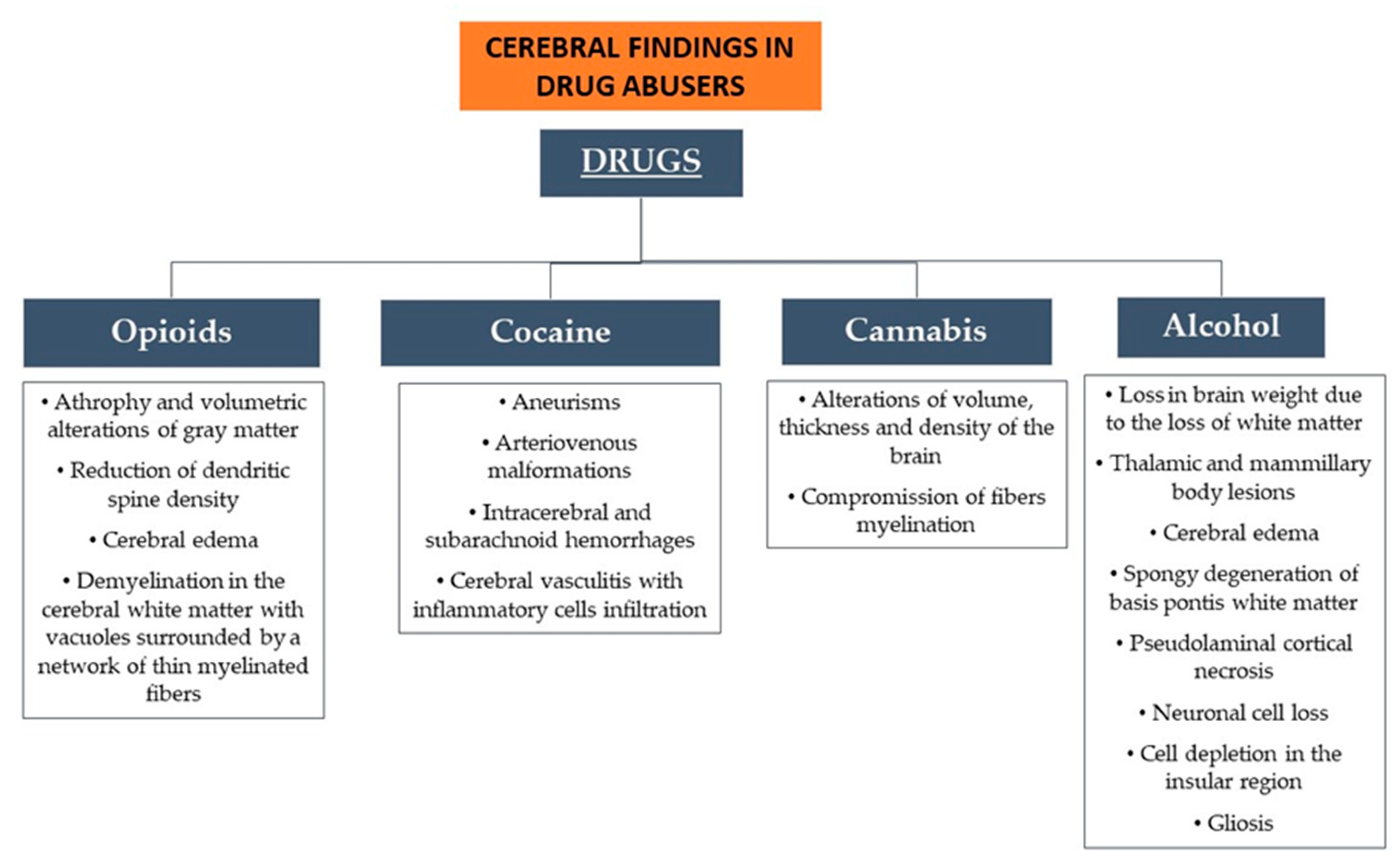
4. Neuropathological Findings in Drug Abusers
4.1. Polydrug
4.2. Opioids
4.3. Cocaine
4.4. Cannabis
4.5. Alcohol
4.6. New Psychoactive Substances
4.6.1. Synthetic Cannabinoids
4.6.2. Hallucinogenic NPS
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Medana, I.M.; Esiri, M.M. Axonal damage: A key predictor of outcome in human CNS diseases. Brain 2003, 126, 515–530. [Google Scholar] [CrossRef]
- Zogopoulos, P.; Theocharis, S. Drug Abuse and Perivascular Changes of the Brain. J. Clin. Exp. Pathol. 2016, 6, 281. [Google Scholar] [CrossRef]
- Connor, M.D.; Lammie, G.A.; Bell, J.E.; Warlow, C.P.; Simmonds, P.; Brettle, R.D. Cerebral infarction in adult AIDS patients: Observations from the Edinburgh HIV Autopsy Cohort. Stroke 2000, 31, 2117–2126. [Google Scholar] [CrossRef]
- Müller, U.J.; Truebner, K.; Schiltz, K.; Kuhn, J.; Mawrin, C.; Dobrowolny, H.; Bernstein, H.-G.; Bogerts, B.; Steiner, J. Postmortem volumetric analysis of the nucleus accumbens in male heroin addicts: Implications for deep brain stimulation. Eur. Arch. Psychiatry Clin. Neurosci. 2015, 265, 647–653. [Google Scholar] [CrossRef]
- Castilla-Ortega, E.; Serrano, A.; Blanco, E.; Araos, P.; Suárez, J.; Pavón, F.J.; de Fonseca, F.R.; Santín, L.J. A place for the hippocampus in the cocaine addiction circuit: Potential roles for adult hippocampal neurogenesis. Neurosci. Biobehav. Rev. 2016, 66, 15–32. [Google Scholar] [CrossRef]
- Baldelli, R.J.; Green, F.H.; Auer, R.N. Sulfide toxicity: Mechanical ventilation and hypotension determine survival rate and brain necrosis. J. Appl. Physiol. 1993, 75, 1348–1353. [Google Scholar] [CrossRef]
- Volkow, N.D.; Valentine, A.; Kulkarni, M. Radiological and neurological changes in the drug abuse patient: A study with MRI. J. Neuroradiol. 1988, 15, 288–293. [Google Scholar]
- Coller, J.K.; Hutchinson, M.R. Implications of central immune signaling caused by drugs of abuse: Mechanisms, mediators and new therapeutic approaches for prediction and treatment of drug dependence. Pharmacol. Ther. 2012, 134, 219–245. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Li, J.-X. Toll-Like Receptor 4 Signaling and Drug Addiction. Front. Pharmacol. 2020, 11, 603445. [Google Scholar] [CrossRef] [PubMed]
- Bernard, J.-P.; Khiabani, H.Z.; Hilberg, T.; Karinen, R.; Slørdal, L.; Waal, H.; Mørland, J. Characteristics of methadone-related fatalities in Norway. J. Forensic Leg. Med. 2015, 36, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Beswick, T.; Best, D.; Rees, S.; Coomber, R.; Gossop, M.; Strang, J. Multiple drug use: Patterns and practices of heroin and crack use in a population of opiate addicts in treatment. Drug Alcohol Rev. 2001, 20, 201–204. [Google Scholar] [CrossRef]
- Brådvik, L.; Berglund, M.; Frank, A.; Lindgren, A.; Löwenhielm, P. Number of addictive substances used related to increased risk of unnatural death: A combined medico-legal and case-record study. BMC Psychiatry 2009, 9, 48. [Google Scholar] [CrossRef]
- Calcaterra, S.; Glanz, J.; Binswanger, I.A. National trends in pharmaceutical opioid related overdose deaths compared to other substance related overdose deaths: 1999–2009. Drug Alcohol Depend. 2013, 131, 263–270. [Google Scholar] [CrossRef]
- Coffin, P.O.; Galea, S.; Ahern, J.; Leon, A.C.; Vlahov, D.; Tardiff, K. Opiates, cocaine and alcohol combinations in accidental drug overdose deaths in New York City, 1990–1998. Addiction 2003, 98, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Darke, S.; Lappin, J.; Kaye, S.; Duflou, J. Clinical Characteristics of Fatal Methamphetamine-related Stroke: A National Study. J. Forensic Sci. 2018, 63, 735–739. [Google Scholar] [CrossRef]
- Drummer, O.H. Fatalities Caused by Novel Opioids: A Review. Forensic Sci. Res. 2019, 4, 95–110. [Google Scholar] [CrossRef]
- Connor, J.P.; Gullo, M.J.; White, A.; Kelly, A.B. Polysubstance use: Diagnostic challenges, patterns of use and health. Curr. Opin. Psychiatry 2014, 27, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Bamsey, R. Polydrug Use: Prevalence, Predictors, Pharmacology and Psychopharmacology. Yale Rev. Undergrad. Res. Psychol. 2017, 7, 20–47. [Google Scholar]
- Büttner, A.; Weis, S. Neuropathological alterations in drug abusers. Forensic Sci. Med. Pathol. 2006, 2, 115–126. [Google Scholar] [CrossRef]
- Büttner, A.; Rohrmoser, K.; Mall, G.; Penning, R.; Weis, S. Widespread axonal damage in the brain of drug abusers as evidenced by accumulation of β-amyloid precursor protein (β-APP): An immunohistochemical investigation. Addiction 2006, 101, 1339–1346. [Google Scholar] [CrossRef] [PubMed]
- Kaag, A.M.; Schulte, M.H.J.; Jansen, J.M.; van Wingen, G.; Homberg, J.; van den Brink, W.; Wiers, R.; Schmaal, L.; Goudriaan, A.; Reneman, L. The relation between gray matter volume and the use of alcohol, tobacco, cocaine and cannabis in male polysubstance users. Drug Alcohol Depend. 2018, 187, 186–194. [Google Scholar] [CrossRef]
- Kaag, A.M.; van Wingen, G.A.; Caan, M.W.A.; Homberg, J.R.; van den Brink, W.; Reneman, L. White matter alterations in cocaine users are negatively related to the number of additionally (ab)used substances. Addict. Biol. 2017, 22, 1048–1056. [Google Scholar] [CrossRef] [PubMed]
- Noyan, C.O.; Kose, S.; Nurmedov, S.; Metin, B.; Darcin, A.E.; Dilbaz, N. Volumetric brain abnormalities in polysubstance use disorder patients. Neuropsychiatr. Dis. Treat. 2016, 12, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Bohnert, A.S.B.; Tracy, M.; Galea, S. Circumstances and witness characteristics associated with overdose fatality. Ann. Emerg. Med. 2009, 54, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Büttner, A.; Kroehling, C.; Mall, G.; Penning, R.; Weis, S. Alterations of the vascular basal lamina in the cerebral cortex in drug abuse: A combined morphometric and immunohistochemical investigation. Drug Alcohol Depend. 2005, 79, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Büttner, A.; Mehraein, P.; Weis, S. Vascular changes in the cerebral cortex in HIV-1 infection. II. An immunohistochemical and lectinhistochemical investigation. Acta Neuropathol. 1996, 92, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Valentino, R.J.; Volkow, N.D. Untangling the complexity of opioid receptor function. Neuropsychopharmacology 2018, 43, 2514–2520. [Google Scholar] [CrossRef]
- Makrigeorgi-Butera, M.; Hagel, C.; Laas, R.; Puschel, K.; Stavrou, D. Comparative brain pathology of HIV-seronegative and HIV-infected drug addicts. Clin. Neuropathol. 1996, 15, 324–329. [Google Scholar]
- Oehmichen, M.; Meissner, C.; Reiter, A.; Birkholz, M. Neuropathology in non-human immunodeficiency virus-infected drug addicts: Hypoxic brain damage after chronic intravenous drug abuse. Acta Neuropathol. 1996, 91, 642–646. [Google Scholar] [CrossRef]
- Andersen, S.N.; Skullerud, K. Hypoxic/ischaemic brain damage, especially pallidal lesions, in heroin addicts. Forensic Sci. Int. 1999, 102, 51–59. [Google Scholar] [CrossRef]
- Wollman, S.C.; Alhassoon, O.M.; Hall, M.G.; Stern, M.J.; Connors, E.J.; Kimmel, C.L.; Allen, K.E.; Stephan, R.A.; Radua, J. Gray matter abnormalities in opioid-dependent patients: A neuroimaging meta-analysis. Am. J. Drug Alcohol Abus. 2017, 43, 505–517. [Google Scholar] [CrossRef] [PubMed]
- Lyoo, I.K.; Pollack, M.H.; Silveri, M.M.; Ahn, K.H.; Diaz, C.I.; Hwang, J.; Kim, S.J.; Yurgelun-Todd, D.A.; Kaufman, M.J.; Renshaw, P.F. Prefrontal and temporal gray matter density decreases in opiate dependence. Psychopharmacology 2006, 184, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Reid, A.G.; Daglish, M.R.C.; Kempton, M.J.; Williams, T.M.; Watson, B.; Nutt, D.J.; Lingford-Hughes, A.R. Reduced thalamic grey matter volume in opioid dependence is influenced by degree of alcohol use: A voxel-based morphometry study. J. Psychopharmacol. 2008, 22, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.; Vogel, M.; Baumgartner, S.; Wiesbeck, G.A.; Lang, U.; Borgwardt, S.; Walter, M. Brain volume changes after long-term injectable opioid treatment: A longitudinal voxel-based morphometry study. Addict. Biol. 2021, 26, e12970. [Google Scholar] [CrossRef] [PubMed]
- Younger, J.W.; Chu, L.F.; D’Arcy, N.; Trott, K.; Jastrzab, L.E.; Mackey, S.C. Prescription opioid analgesics rapidly change the human brain. Pain 2011, 152, 1803–1810. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, J.; Maleki, N.; Potter, J.; Elman, I.; Rudrauf, D.; Knudsen, J.; Wallin, D.; Pendse, G.; McDonald, L.; Griffin, M.; et al. Alterations in brain structure and functional connectivity in prescription opioid-dependent patients. Brain 2010, 133, 2098–2114. [Google Scholar] [CrossRef] [PubMed]
- Merhar, S.L.; Kline, J.E.; Braimah, A.; Kline-Fath, B.M.; Tkach, J.A.; Altaye, M.; He, L.; Parikh, N.A. Prenatal opioid exposure is associated with smaller brain volumes in multiple regions. Pediatr. Res. 2021, 90, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Büttner, A.; Mall, G.; Penning, R.; Weis, S. The neuropathology of heroin abuse. Forensic Sci. Int. 2000, 113, 435–442. [Google Scholar] [CrossRef]
- Frisoni, P.; Bacchio, E.; Bilel, S.; Talarico, A.; Gaudio, R.M.; Barbieri, M.; Neri, M.; Marti, M. Novel Synthetic Opioids: The Pathologist’s Point of View. Brain Sci. 2018, 8, 170. [Google Scholar] [CrossRef]
- Kriegstein, A.R.; Armitage, B.A.; Kim, P.Y. Heroin inhalation and progressive spongiform leukoencephalopathy. N. Engl. J. Med. 1997, 336, 589–590. [Google Scholar] [CrossRef]
- Kashyap, S.; Majeed, G.; Bowen, I.; Beamer, Y.; Miulli, D. Toxic Leukoencephalopathy due to Inhalational Heroin Abuse. Ann. Indian Acad. Neurol. 2020, 23, 542–544. [Google Scholar] [CrossRef]
- Offiah, C.; Hall, E. Heroin-induced leukoencephalopathy: Characterization using MRI, diffusion-weighted imaging, and MR spectroscopy. Clin. Radiol. 2008, 63, 146–152. [Google Scholar] [CrossRef]
- Ropper, A.H.; Blair, R. Symmetric deep cerebellar lesions after smoking heroin. Arch. Neurol. 2003, 60, 1605–1606. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.; Molloy, F.M.; Farrell, M.A.; Hutchinson, M. Fatal toxic leukoencephalopathy: Clinical, radiological, and necropsy findings in two patients. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1014–1016. [Google Scholar] [CrossRef] [PubMed]
- Esse, K.; Fossati-Bellani, M.; Traylor, A.; Martin-Schild, S. Epidemic of illicit drug use, mechanisms of action/addiction and stroke as a health hazard. Brain Behav. 2011, 1, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Bora, E.; Yücel, M.; Fornito, A.; Pantelis, C.; Harrison, B.J.; Cocchi, L.; Pell, G.; Lubman, D.I. White matter microstructure in opiate addiction. Addict. Biol. 2012, 17, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Gottschalk, P.C.; Kosten, T.R. Cerebral perfusion defects in combined cocaine and alcohol dependence. Drug Alcohol Depend. 2002, 68, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Siniscalchi, A.; Bonci, A.; Mercuri, N.B.; De Siena, A.; De Sarro, G.; Malferrari, G.; Diana, M.; Gallelli, L. Cocaine dependence and stroke: Pathogenesis and management. Curr. Neurovascular Res. 2015, 12, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Treadwell, S.D.; Robinson, T.G. Cocaine use and stroke. Postgrad. Med. J. 2007, 83, 389–394. [Google Scholar] [CrossRef]
- Yao, H.; Kim, K.; Duan, M.; Hayashi, T.; Guo, M.; Morgello, S.; Prat, A.; Wang, J.; Su, T.-P.; Buch, S. Cocaine Hijacks σ1 Receptor to Initiate Induction of Activated Leukocyte Cell Adhesion Molecule: Implication for Increased Monocyte Adhesion and Migration in the CNS. J. Neurosci. 2011, 31, 5942–5955. [Google Scholar] [CrossRef]
- Martin-Schild, S.; Albright, K.C.; Hallevi, H.; Barreto, A.D.; Philip, M.; Misra, V.; Grotta, J.C.; Savitz, S.I. Intracerebral hemorrhage in cocaine users. Stroke 2010, 41, 680–684. [Google Scholar] [CrossRef]
- Nanda, A.; Vannemreddy, P.S.; Polin, R.S.; Willis, B.K. Intracranial aneurysms and cocaine abuse: Analysis of prognostic indicators. Neurosurgery 2000, 46, 1063–1067; discussion 1067–1069. [Google Scholar] [CrossRef]
- Sordo, L.; Indave, B.I.; Barrio, G.; Degenhardt, L.; de la Fuente, L.; Bravo, M.J. Cocaine use and risk of stroke: A systematic review. Drug Alcohol Depend. 2014, 142, 1–13. [Google Scholar] [CrossRef]
- Toossi, S.; Hess, C.P.; Hills, N.K.; Josephson, S.A. Neurovascular complications of cocaine use at a tertiary stroke center. J. Stroke Cerebrovasc. Dis. 2010, 19, 273–278. [Google Scholar] [CrossRef]
- Vannemreddy, P.; Caldito, G.; Willis, B.; Nanda, A. Influence of cocaine on ruptured intracranial aneurysms: A case control study of poor prognostic indicators. J. Neurosurg. 2008, 108, 470–476. [Google Scholar] [CrossRef]
- Jabbarli, R.; Dinger, T.F.; Darkwah Oppong, M.; Pierscianek, D.; Dammann, P.; Wrede, K.H.; Kaier, K.; Köhrmann, M.; Forsting, M.; Kleinschnitz, C.; et al. Risk Factors for and Clinical Consequences of Multiple Intracranial Aneurysms: A Systematic Review and Meta-Analysis. Stroke 2018, 49, 848–855. [Google Scholar] [CrossRef]
- Sato, H.; Kamide, T.; Kikkawa, Y.; Kimura, T.; Kuribara, S.; Yanagawa, T.; Suzuki, K.; Ikeda, T.; Kurita, H. Clinical Characteristics of Ruptured Intracranial Aneurysm in Patients with Multiple Intracranial Aneurysms. World Neurosurg. 2021, 149, e935–e941. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.E.; Tamargo, R.J. Cocaine use is an independent risk factor for cerebral vasospasm after aneurysmal subarachnoid hemorrhage. Stroke 2001, 32, 2338–2343. [Google Scholar] [CrossRef] [PubMed]
- Martin-Schild, S.; Albright, K.C.; Misra, V.; Philip, M.; Barreto, A.D.; Hallevi, H.; Grotta, J.C.; Savitz, S.I. Intravenous Tissue Plasminogen Activator in Patients with Cocaine-Associated Acute Ischemic Stroke. Stroke 2009, 40, 3635–3637. [Google Scholar] [CrossRef]
- Alaraj, A.; Wallace, A.; Mander, N.; Aletich, V.; Charbel, F.T.; Amin-Hanjani, S. Effect of acute cocaine use on vasospasm and outcome in aneurysmal subarachnoid hemorrhage. World Neurosurg. 2010, 73, 357–360. [Google Scholar] [CrossRef] [PubMed]
- Almaghrabi, T.S.; McDonald, M.M.; Cai, C.; Rahbar, M.H.; Choi, H.A.; Lee, K.; Naval, N.S.; Grotta, J.C.; Chang, T.R. Cocaine Use is Associated with More Rapid Clot Formation and Weaker Clot Strength in Acute Stroke Patients. Int. J. Cerebrovasc. Dis. Stroke 2019, 2, 110. [Google Scholar] [PubMed]
- Fessler, R.D.; Esshaki, C.M.; Stankewitz, R.C.; Johnson, R.R.; Diaz, F.G. The neurovascular complications of cocaine. Surg. Neurol. 1997, 47, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.K.; Fischer, D.K.; Narayan, R.K.; Cech, D.A.; Robertson, C.S. Intravenous cocaine abuse and subarachnoid haemorrhage: Effect on outcome. Br. J. Neurosurg. 1990, 4, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Howington, J.U.; Kutz, S.C.; Wilding, G.E.; Awasthi, D. Cocaine use as a predictor of outcome in aneurysmal subarachnoid hemorrhage. J. Neurosurg. 2003, 99, 271–275. [Google Scholar] [CrossRef]
- Boco, T.; Macdonald, R.L. Absence of acute cerebral vasoconstriction after cocaine-associated subarachnoid hemorrhage. Neurocritical Care 2004, 1, 449–454. [Google Scholar] [CrossRef]
- Bhattacharya, P.; Taraman, S.; Shankar, L.; Chaturvedi, S.; Madhavan, R. Clinical profiles, complications, and disability in cocaine-related ischemic stroke. J. Stroke Cerebrovasc. Dis. 2011, 20, 443–449. [Google Scholar] [CrossRef]
- Bajwa, A.A.; Silliman, S.; Cury, J.D.; Seeram, V.; Shujaat, A.; Usman, F.; Samuel, V. Characteristics and outcomes of cocaine-related spontaneous intracerebral hemorrhages. ISRN Neurol. 2013, 2013, 124390. [Google Scholar] [CrossRef]
- Chang, T.R.; Kowalski, R.G.; Caserta, F.; Carhuapoma, J.R.; Tamargo, R.J.; Naval, N.S. Impact of acute cocaine use on aneurysmal subarachnoid hemorrhage. Stroke 2013, 44, 1825–1829. [Google Scholar] [CrossRef]
- Moon, K.; Albuquerque, F.C.; Mitkov, M.; Ducruet, A.F.; Wilson, D.A.; Crowley, R.W.; Nakaji, P.; McDougall, C.G. Methamphetamine use is an independent predictor of poor outcome after aneurysmal subarachnoid hemorrhage. J. NeuroInterventional Surg. 2015, 7, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Aleksić, I.; Džambas, J.; Marinković, N.; Šegrt, Z.; Nikolić, M. Subarachnoid and intracerebral hemorrhage in cocaine abusers. Vojn. Pregl. 2021, 78, 1166–1172. [Google Scholar] [CrossRef]
- Kibayashi, K.; Mastri, A.R.; Hirsch, C.S. Cocaine induced intracerebral hemorrhage: Analysis of predisposing factors and mechanisms causing hemorrhagic strokes. Hum. Pathol. 1995, 26, 659–663. [Google Scholar] [CrossRef]
- Aggarwal, S.K.; Williams, V.; Levine, S.R.; Cassin, B.J.; Garcia, J.H. Cocaine-associated intracranial hemorrhage: Absence of vasculitis in 14 cases. Neurology 1996, 46, 1741–1743. [Google Scholar] [CrossRef]
- Nolte, K.B.; Brass, L.M.; Fletterick, C.F. Intracranial hemorrhage associated with cocaine abuse: A prospective autopsy study. Neurology 1996, 46, 1291–1296. [Google Scholar] [CrossRef]
- Fonseca, A.C.; Ferro, J.M. Drug abuse and stroke. Curr. Neurol. Neurosci. Rep. 2013, 13, 325. [Google Scholar] [CrossRef]
- Fredericks, R.K.; Lefkowitz, D.S.; Challa, V.R.; Troost, B.T. Cerebral vasculitis associated with cocaine abuse. Stroke 1991, 22, 1437–1439. [Google Scholar] [CrossRef]
- Diez-Tejedor, E.; Frank, A.; Gutierrez, M.; Barreiro, P. Encephalopathy and biopsy-proven cerebrovascular inflammatory changes in a cocaine abuser. Eur. J. Neurol. 1998, 5, 103–107. [Google Scholar] [CrossRef]
- Lee, Y.W.; Hennig, B.; Fiala, M.; Kim, K.S.; Toborek, M. Cocaine activates redox-regulated transcription factors and induces TNF-α expression in human brain endothelial cells. Brain Res. 2001, 920, 125–133. [Google Scholar] [CrossRef]
- Hall, W.; Degenhardt, L. Adverse health effects of non-medical cannabis use. Lancet 2009, 374, 1383–1391. [Google Scholar] [CrossRef]
- Mackie, K. Cannabinoid receptors: Where they are and what they do. J. Neuroendocri. 2008, 20 (Suppl. S1), 10–14. [Google Scholar] [CrossRef]
- Straiker, A.J.; Maguire, G.; Mackie, K.; Lindsey, J. Localization of cannabinoid CB1 receptors in the human anterior eye and retina. Investig. Ophthalmol. Vis. Sci. 1999, 40, 2442–2448. [Google Scholar]
- Herning, R.I.; Better, W.E.; Tate, K.; Cadet, J.L. Cerebrovascular perfusion in marijuana users during a month of monitored abstinence. Neurology 2005, 64, 488–493. [Google Scholar] [CrossRef]
- Thanvi, B.R.; Treadwell, S.D. Cannabis and stroke: Is there a link? Postgrad. Med. J. 2009, 85, 80–83. [Google Scholar] [CrossRef]
- Jacobus, J.; Tapert, S.F. Effects of cannabis on the adolescent brain. Curr. Pharm. Des. 2014, 20, 2186–2193. [Google Scholar] [CrossRef]
- van Hell, H.H.; Bossong, M.G.; Jager, G.; Kristo, G.; van Osch, M.J.P.; Zelaya, F.; Kahn, R.S.; Ramsey, N.F. Evidence for involvement of the insula in the psychotropic effects of THC in humans: A double-blind, randomized pharmacological MRI study. Int. J. Neuropsychopharmacol. 2011, 14, 1377–1388. [Google Scholar] [CrossRef]
- Cousijn, J.; Wiers, R.W.; Ridderinkhof, K.R.; van den Brink, W.; Veltman, D.J.; Goudriaan, A.E. Grey matter alterations associated with cannabis use: Results of a VBM study in heavy cannabis users and healthy controls. Neuroimage 2012, 59, 3845–3851. [Google Scholar] [CrossRef]
- Yücel, M.; Solowij, N.; Respondek, C.; Whittle, S.; Fornito, A.; Pantelis, C.; Lubman, D.I. Regional brain abnormalities associated with long-term heavy cannabis use. Arch. Gen. Psychiatry 2008, 65, 694–701. [Google Scholar] [CrossRef]
- Ashtari, M.; Avants, B.; Cyckowski, L.; Cervellione, K.L.; Roofeh, D.; Cook, P.; Gee, J.; Sevy, S.; Kumra, S. Medial temporal structures and memory functions in adolescents with heavy cannabis use. J. Psychiatr. Res. 2011, 45, 1055–1066. [Google Scholar] [CrossRef]
- Demirakca, T.; Sartorius, A.; Ende, G.; Meyer, N.; Welzel, H.; Skopp, G.; Mann, K.; Hermann, D. Diminished gray matter in the hippocampus of cannabis users: Possible protective effects of cannabidiol. Drug Alcohol Depend. 2011, 114, 242–245. [Google Scholar] [CrossRef]
- Matochik, J.A.; Eldreth, D.A.; Cadet, J.-L.; Bolla, K.I. Altered brain tissue composition in heavy marijuana users. Drug Alcohol Depend. 2005, 77, 23–30. [Google Scholar] [CrossRef]
- Medina, K.L.; McQueeny, T.; Nagel, B.J.; Hanson, K.L.; Yang, T.T.; Tapert, S.F. Prefrontal cortex morphometry in abstinent adolescent marijuana users: Subtle gender effects. Addict. Biol. 2009, 14, 457–468. [Google Scholar] [CrossRef]
- Solowij, N.; Walterfang, M.; Lubman, D.I.; Whittle, S.; Lorenzetti, V.; Styner, M.; Velakoulis, D.; Pantelis, C.; Yücel, M. Alteration to hippocampal shape in cannabis users with and without schizophrenia. Schizophr. Res. 2013, 143, 179–184. [Google Scholar] [CrossRef]
- Cohen, M.; Rasser, P.E.; Peck, G.; Carr, V.J.; Ward, P.B.; Thompson, P.M.; Johnston, P.; Baker, A.; Schall, U. Cerebellar grey-matter deficits, cannabis use and first-episode schizophrenia in adolescents and young adults. Int. J. Neuropsychopharmacol. 2012, 15, 297–307. [Google Scholar] [CrossRef]
- Zalesky, A.; Solowij, N.; Yücel, M.; Lubman, D.I.; Takagi, M.; Harding, I.H.; Lorenzetti, V.; Wang, R.; Searle, K.; Pantelis, C.; et al. Effect of long-term cannabis use on axonal fibre connectivity. Brain 2012, 135, 2245–2255. [Google Scholar] [CrossRef]
- Bolla, K.I.; Eldreth, D.A.; Matochik, J.A.; Cadet, J.L. Neural substrates of faulty decision-making in abstinent marijuana users. Neuroimage 2005, 26, 480–492. [Google Scholar] [CrossRef]
- Manza, P.; Yuan, K.; Shokri-Kojori, E.; Tomasi, D.; Volkow, N.D. Brain structural changes in cannabis dependence: Association with MAGL. Mol. Psychiatry 2020, 25, 3256–3266. [Google Scholar] [CrossRef]
- Gilman, J.M.; Kuster, J.K.; Lee, S.; Lee, M.J.; Kim, B.W.; Makris, N.; van der Kouwe, A.; Blood, A.J.; Breiter, H.C. Cannabis use is quantitatively associated with nucleus accumbens and amygdala abnormalities in young adult recreational users. J. Neurosci. 2014, 34, 5529–5538. [Google Scholar] [CrossRef]
- Orr, C.; Spechler, P.; Cao, Z.; Albaugh, M.; Chaarani, B.; Mackey, S.; D’Souza, D.; Allgaier, N.; Banaschewski, T.; Bokde, A.L.; et al. Grey Matter Volume Differences Associated with Extremely Low Levels of Cannabis Use in Adolescence. J. Neurosci. 2019, 39, 1817–1827. [Google Scholar] [CrossRef]
- Jacobus, J.; Squeglia, L.M.; Meruelo, A.D.; Castro, N.; Brumback, T.; Giedd, J.N.; Tapert, S.F. Cortical thickness in adolescent marijuana and alcohol users: A three-year prospective study from adolescence to young adulthood. Dev. Cogn. Neurosci. 2015, 16, 101–109. [Google Scholar] [CrossRef]
- Phillips, D.E.; Krueger, S.K.; Wall, K.A.; Smoyer-Dearing, L.H.; Sikora, A.K. The development of the blood-brain barrier in alcohol-exposed rats. Alcohol 1997, 14, 333–343. [Google Scholar] [CrossRef]
- Persson, L.; Rosengren, L. Increased blood-brain barrier permeability around cerebral stab wounds, aggravated by acute ethanol intoxication. Acta Neurol. Scand. 1977, 56, 7–16. [Google Scholar] [CrossRef]
- Harper, C. The neuropathology of alcohol-related brain damage. Alcohol Alcohol. 2009, 44, 136–140. [Google Scholar] [CrossRef]
- Harper, C.G.; Kril, J.J. Neuropathology of alcoholism. Alcohol Alcohol. 1990, 25, 207–216. [Google Scholar] [CrossRef]
- Laas, R.; Hagel, C. Neuropathology of chronic alcoholism. Clin. Neuropathol. 2000, 19, 252–253. [Google Scholar]
- Sullivan, E.V.; Pfefferbaum, A. Neurocircuitry in alcoholism: A substrate of disruption and repair. Psychopharmacol. 2005, 180, 583–594. [Google Scholar] [CrossRef]
- Alfonso-Loeches, S.; Pascual, M.; Gómez-Pinedo, U.; Pascual-Lucas, M.; Renau-Piqueras, J.; Guerri, C. Toll-like receptor 4 participates in the myelin disruptions associated with chronic alcohol abuse. Glia 2012, 60, 948–964. [Google Scholar] [CrossRef]
- Alfonso-Loeches, S.; Pascual-Lucas, M.; Blanco, A.M.; Sanchez-Vera, I.; Guerri, C. Pivotal role of TLR4 receptors in alcohol-induced neuroinflammation and brain damage. J. Neurosci. 2010, 30, 8285–8295. [Google Scholar] [CrossRef]
- Blanco, A.M.; Vallés, S.L.; Pascual, M.; Guerri, C. Involvement of TLR4/type I IL-1 receptor signaling in the induction of inflammatory mediators and cell death induced by ethanol in cultured astrocytes. J. Immunol. 2005, 175, 6893–6899. [Google Scholar] [CrossRef]
- Qin, L.; He, J.; Hanes, R.N.; Pluzarev, O.; Hong, J.-S.; Crews, F.T. Increased systemic and brain cytokine production and neuroinflammation by endotoxin following ethanol treatment. J. Neuroinflammation 2008, 5, 10. [Google Scholar] [CrossRef]
- de la Monte, S.M. Disproportionate atrophy of cerebral white matter in chronic alcoholics. Arch. Neurol. 1988, 45, 990–992. [Google Scholar] [CrossRef]
- Lewohl, J.M.; Wang, L.; Miles, M.F.; Zhang, L.; Dodd, P.R.; Harris, R.A. Gene expression in human alcoholism: Microarray analysis of frontal cortex. Alcohol Clin. Exp. Res. 2000, 24, 1873–1882. [Google Scholar] [CrossRef]
- Pfefferbaum, A.; Rosenbloom, M.; Rohlfing, T.; Sullivan, E.V. Degradation of Association and Projection White Matter Systems in Alcoholism Detected with Quantitative Fiber Tracking. Biol. Psychiatry 2009, 65, 680–690. [Google Scholar] [CrossRef]
- Kril, J.J.; Flowers, D.; Butterworth, R.F. Distinctive pattern of Bergmann glial pathology in human hepatic encephalopathy. Mol. Chem. Neuropathol. 1997, 31, 279–287. [Google Scholar] [CrossRef]
- Pfefferbaum, A.; Sullivan, E.V.; Mathalon, D.H.; Shear, P.K.; Rosenbloom, M.J.; Lim, K.O. Longitudinal changes in magnetic resonance imaging brain volumes in abstinent and relapsed alcoholics. Alcohol Clin. Exp. Res. 1995, 19, 1177–1191. [Google Scholar] [CrossRef]
- Pfefferbaum, A.; Rosenbloom, M.; Serventi, K.L.; Sullivan, E.V. Corpus callosum, pons, and cortical white matter in alcoholic women. Alcohol Clin. Exp. Res. 2002, 26, 400–406. [Google Scholar] [CrossRef]
- Denk, C.H.; Kunzmann, J.; Maieron, A.; Wöhrer, A.; Quinot, V.; Oberndorfer, S. Histopathological examination of characteristic brain MRI findings in acute hyperammonemic encephalopathy: A case report and review of the literature. Neuroradiol. J. 2023. [Google Scholar] [CrossRef]
- Butterworth, R.F. Neuronal cell death in hepatic encephalopathy. Metab. Brain Dis. 2007, 22, 309–320. [Google Scholar] [CrossRef]
- Torvik, A.; Lindboe, C.F.; Rogde, S. Brain lesions in alcoholics: A neuropathological study with clinical correlations. J. Neurol. Sci. 1982, 56, 233–248. [Google Scholar] [CrossRef]
- Karhunen, P.J.; Erkinjuntti, T.; Laippala, P. Moderate alcohol consumption and loss of cerebellar Purkinje cells. BMJ 1994, 308, 1663–1667. [Google Scholar] [CrossRef]
- Catalá, I.; Ferrer, I.; Galofré, E.; Fábregues, I. Decreased numbers of dendritic spines on cortical pyramidal neurons in dementia. A quantitative Golgi study on biopsy samples. Hum. Neurobiol. 1988, 6, 255–259. [Google Scholar]
- Kril, J.J.; Butterworth, R.F. Diencephalic and cerebellar pathology in alcoholic and nonalcoholic patients with end-stage liver disease. Hepatology 1997, 26, 837–841. [Google Scholar] [CrossRef]
- Okeda, R.; Taki, K.; Ikari, R.; Funata, N. Vascular changes in acute Wernicke’s encephalopathy. Acta Neuropathol. 1995, 89, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Thornberry, D.S.; Itabashi, H.H. Pontine spongy degeneration of white matter associated with hepatic encephalopathy. Arch. Pathol. Lab. Med. 1984, 108, 564–566. [Google Scholar] [PubMed]
- Wikström, M.; Thelander, G.; Nyström, I.; Kronstrand, R. Two fatal intoxications with the new designer drug methedrone (4-methoxymethcathinone). J. Anal. Toxicol. 2010, 34, 594–598. [Google Scholar] [CrossRef] [PubMed]
- Daziani, G.; Lo Faro, A.F.; Montana, V.; Goteri, G.; Pesaresi, M.; Bambagiotti, G.; Montana, A. Synthetic Cathinones and Neurotoxicity Risks: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 6230. [Google Scholar] [CrossRef]
- Angerer, V.; Jacobi, S.; Franz, F.; Auwärter, V.; Pietsch, J. Three fatalities associated with the synthetic cannabinoids 5F-ADB, 5F-PB-22, and AB-CHMINACA. Forensic Sci. Int. 2017, 281, e9–e15. [Google Scholar] [CrossRef]
- Chan, S.; Wu, J.; Lee, B. Fatalities related to new psychoactive substances in Singapore-A case series. Forensic Sci. Int. 2019, 304, 109892. [Google Scholar] [CrossRef]
- Yoshida, K.-I.; Saka, K.; Shintani-Ishida, K.; Maeda, H.; Nakajima, M.; Hara, S.; Ueno, M.; Sasaki, K.; Iwase, H.; Sakamoto, T. A case of fatal intoxication due to the new designer drug 25B-NBOMe. Forensic Toxicol. 2015, 33, 396–401. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug | Alterations | References |
|---|---|---|
| Opioids | Atrophy in the right insula, reductions in the superior temporal and orbitofrontal gyri decreased gray matter in the left cerebellar vermis and right Rolandic operculum, including the insula | [28] |
| Opioids | Decreased gray matter density in the bilateral medial frontal cortex, right superior and inferior frontal cortex, and left superior and middle frontal cortex. Decreased gray matter density in bilateral insula, bilateral superior temporal cortex, right uncus and left fusiform cortex | [29] |
| Opioids | Decreased gray matter volume in opioid dependent subjects compared with control subjects | [30] |
| Opioids | Increased volume of the right caudate nucleus and a decreasing trend of the volumes of the right amygdala, anterior cingulate cortex, and orbitofrontal cortex | [31] |
| Morphine | Increase in gray matter in the left pregenual anterior cingulate, right ventral posterior cingulate, inferior pons, the right hypothalamus, and left inferior frontal gyrus. Decreased gray matter in the amygdala and hypothalamus | [32] |
| Opioids | Increased dendritic spine density, bilateral volumetric loss in the amygdala and decreased fractional anisotropy of amygdala, nucleus accumbens, and insula | [33] |
| Opioids | Infants prenatally exposed to opioids showed a smaller overall deep gray matter of thalamus and insula. Increased volumes of white matter in the right cingulate gyrus and left occipital lobe | [34] |
| Heroin | Decreased brain tissue, cerebral edema, demyelination in the cerebral white matter. Decreased neuronal density in the globus pallidus | [35] |
| Opioids | Vacuolar degeneration of the deep white matter in the centrum semi-oval of the two hemispheres | [40] |
| Opioids | Decreased fractional anisotropy in corpus callosum, thalamic radiation, and inferior longitudinal fasciculus | [42] |
| Cocaine | Ischemic stroke | [43,44,45] |
| Cocaine | Intracerebral and subarachnoid hemorrhages | [47,48,49,50,51] |
| Cocaine | Cerebrovascular complications | [54,55,56,57] |
| Cocaine | Intracerebral and subarachnoid hemorrhages, ischemic stroke and aneurysmal subarachnoid hemorrhage | [47,48,50,55,56,58,59,60,61,62,63,64,65,66,67,68,69] |
| Cocaine | Cerebral vasculitis | [70,71,72] |
| Cannabis | Vasospasm, hypotension, arrhythmias and increased cerebrovascular resistance | [78,79] |
| Cannabis | Reduced cerebral blood flow in left, superior and middle temporal gyri, left insula, left and right medial frontal gyrus, and left supramarginal gyrus at the baseline | [80] |
| Cannabis | Increased blood perfusion in the anterior cingulate, frontal cortex, and insula, and reduced perfusion in posterior brain regions | [81] |
| Cannabis | Weekly utilization of cannabis is correlated with a decreased hippocampal and in amygdala volume. Instead, intense cannabis consumption correlates with increased grey matter volume in the cerebellum | [82,83,84,85] |
| Cannabis | Higher density in the left and right precentral gyrus, including portions of postcentral gyrus and thalamus | [86] |
| Cannabis | Female cannabis users have larger volumes in prefrontal cortex morphometry associated with impaired executive functioning | [87] |
| Cannabis | Alterations in shape of the tail, head, and midway down the body of the hippocampus | [88] |
| Cannabis | Axonal connectivity is impaired in the right fimbria of the hippocampus (fornix), splenium of the corpus callosum and commissural fibers | [90] |
| Cannabis | Increased activation in the left cerebellum and less activation in the right lateral orbitofrontal cortex and in the right dorsolateral prefrontal cortex | [91] |
| Cannabis | Decreased thickness and density of gray matter, particularly in the precuneus, especially in young adult cannabis users | [92] |
| Cannabis | In late adolescence, cannabis use might be linked to increased cortical thickness and volume in medial parietal cortex | [93,94,95] |
| Alcohol | Shrinkage of gray matter, enlargement of ventricles, myelin fiber disruption, and degeneration of the white matter | [96,97,98,99] |
| Alcohol | Loss in brain weight due to the loss of white matter | [104] |
| Alcohol | Edematous alterations with neuronal cell depletion in the insular region. Hypoxic ischemic encephalopathy of the frontal regions, with edema and neuronal cell in the occipital, frontal and temporal lobes. The cingulate gyrus only displayed mild gliosis. Diffuse subpial gliosis in both insular cortices | [107] |
| Alcohol | Pseudolaminar cortical necrosis and neuronal cell loss from basal ganglia, thalamus, and cerebellum | [108] |
| Alcohol | Wernicke’s encephalopathy with thalamic and mammillary body lesions | [110] |
| Alcohol | Spongy degeneration of white matter localized to the basis pontis | [111] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montana, A.; Alfieri, L.; Neri, M.; Piano, D.; Renier, E.; Marti, M.; Palpacelli, M.; Basile, G.; Tossetta, G.; Busardò, F.P. Macroscopic and Microscopic Cerebral Findings in Drug and Alcohol Abusers: The Point of View of the Forensic Pathologist. Biomedicines 2024, 12, 681. https://doi.org/10.3390/biomedicines12030681
Montana A, Alfieri L, Neri M, Piano D, Renier E, Marti M, Palpacelli M, Basile G, Tossetta G, Busardò FP. Macroscopic and Microscopic Cerebral Findings in Drug and Alcohol Abusers: The Point of View of the Forensic Pathologist. Biomedicines. 2024; 12(3):681. https://doi.org/10.3390/biomedicines12030681
Chicago/Turabian StyleMontana, Angelo, Letizia Alfieri, Margherita Neri, Denise Piano, Eva Renier, Matteo Marti, Marco Palpacelli, Giuseppe Basile, Giovanni Tossetta, and Francesco Paolo Busardò. 2024. "Macroscopic and Microscopic Cerebral Findings in Drug and Alcohol Abusers: The Point of View of the Forensic Pathologist" Biomedicines 12, no. 3: 681. https://doi.org/10.3390/biomedicines12030681