
The Impacts of Intervertebral Disc Degeneration of the Spine, Alcohol Consumption, Smoking Tobacco Products, and Glycemic Disorders on the Expression Profiles of Neurotrophins-3 and -4
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Study Group
2.3. Control Group
2.4. Securing the Collected Material for Molecular Testing
2.5. NT-3 and NT-4 mRNA Expression Profiles in the IVDs of the L/S Spine Obtained from the Study and Control Groups Using the Real-Time Polymerase Chain Reaction Technique Preceded by Reverse Transcription (RT-qPCR)
2.6. Assessment of the NT-3 and NT-4 Protein Concentration Profiles in the IVDs of the L/S Spine Obtained from the Study and Control Groups
2.7. Statistical Analysis
3. Results
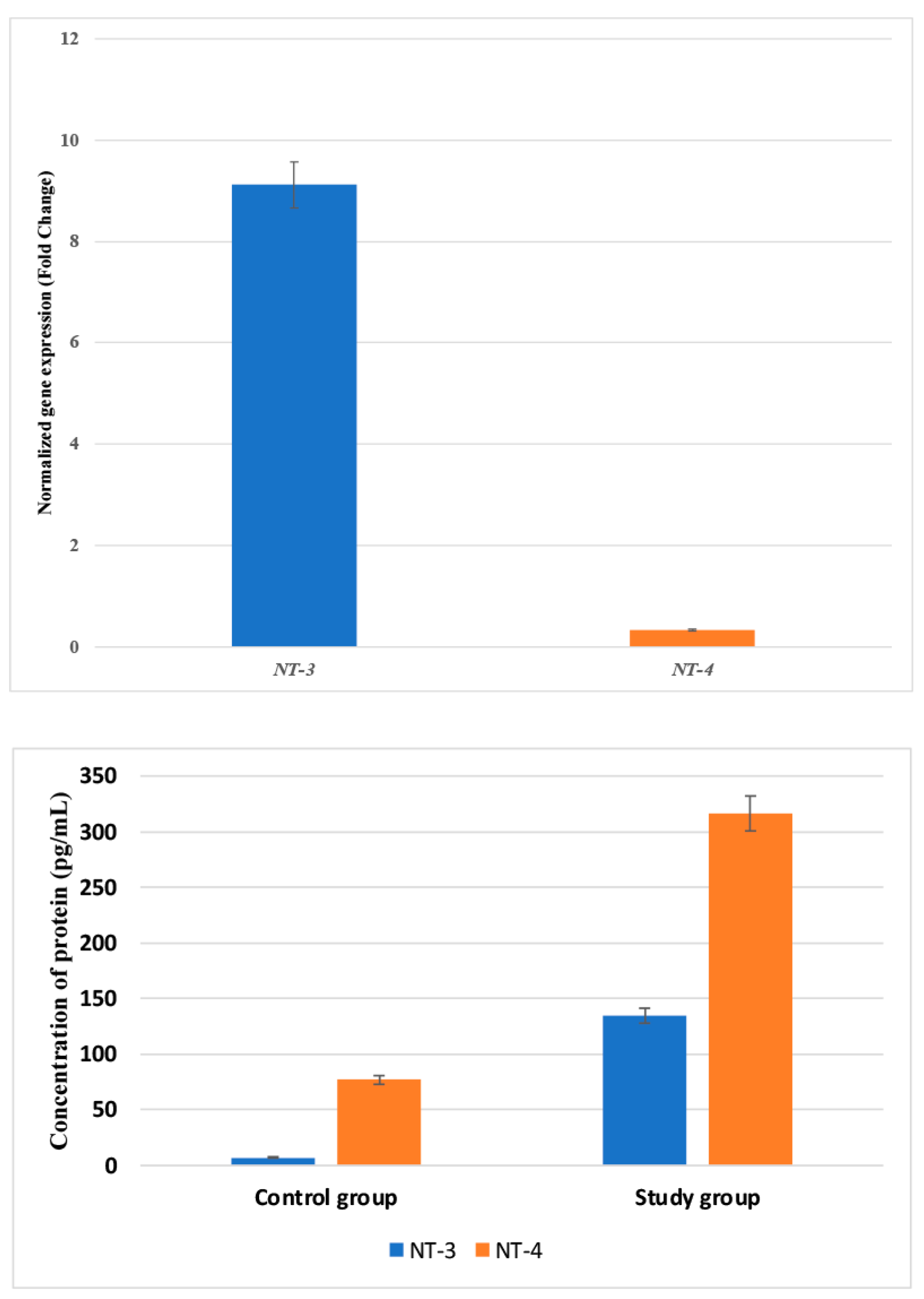
3.1. Expression Changes in the mRNA and Protein Levels of NT-3 and NT-4 in Control and Test Samples
3.2. Concentrations of mRNA and Protein of NT-3 and NT-4 in Control and Examined Samples, Considering the Stage of Radiological Degenerative Changes in IVDs according to the Pfirrmann Scale
3.3. The Concentrations of mRNA and Protein of NT-3 and NT-4 in the Tested Samples Depending on the Pain Degree Measured with the VAS
3.4. Variances in the Expression Profiles of NT-3 and NT-4 at the mRNA and Protein Levels in IVD Samples Obtained from the Study and Control Groups
3.5. Regression Analysis of Variables Potentially Associated with BDNF, GDNF, and GAP-43 Levels in IVDs and Serum Samples from the Study Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gilbert, H.T.J.; Hodson, N.; Baird, P.; Richardson, S.M.; Hoyland, J.A. Acidic pH Promotes Intervertebral Disc Degeneration: Acid-Sensing Ion Channel-3 as a Potential Therapeutic Target. Sci. Rep. 2016, 6, 37360. [Google Scholar] [CrossRef]
- Kirnaz, S.; Capadona, C.; Wong, T.; Goldberg, J.L.; Medary, B.; Sommer, F.; McGrath, L.B., Jr.; Härtl, R. Fundamentals of Intervertebral Disc Degeneration. World Neurosurg. 2022, 157, 264–273. [Google Scholar] [CrossRef]
- Oichi, T.; Taniguchi, Y.; Oshima, Y.; Tanaka, S.; Saito, T. Pathomechanism of Intervertebral Disc Degeneration. JOR Spine 2020, 3, e1076. [Google Scholar] [CrossRef]
- Morel, L.; Domingues, O.; Zimmer, J.; Michel, T. Revisiting the Role of Neurotrophic Factors in Inflammation. Cells 2020, 9, 865. [Google Scholar] [CrossRef]
- Skaper, S.D. Neurotrophic Factors: An Overview. In Neurotrophic Factors: Methods and Protocols; Skaper, S.D., Ed.; Methods in Molecular Biology; Springer: New York, NY, USA, 2018; pp. 1–17. ISBN 978-1-4939-7571-6. [Google Scholar]
- Skup, M. Neurotrophins: Evolution of Concepts on Rational Therapeutic Approaches. Postep. Biochem 2018, 64, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, F.F.; Xapelli, S. Intervention of Brain-Derived Neurotrophic Factor and Other Neurotrophins in Adult Neurogenesis. Adv. Exp. Med. Biol. 2021, 1331, 95–115. [Google Scholar] [CrossRef] [PubMed]
- Aragona, M.; Porcino, C.; Guerrera, M.C.; Montalbano, G.; Laurà, R.; Cometa, M.; Levanti, M.; Abbate, F.; Cobo, T.; Capitelli, G.; et al. The BDNF/TrkB Neurotrophin System in the Sensory Organs of Zebrafish. Int. J. Mol. Sci. 2022, 23, 2621. [Google Scholar] [CrossRef] [PubMed]
- Kojima, M.; Matsui, K.; Mizui, T. BDNF Pro-Peptide: Physiological Mechanisms and Implications for Depression. Cell Tissue Res. 2019, 377, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Zhao, X.; Shen, H.; Zhang, C. Molecular Mechanisms of Cell Death in Intervertebral Disc Degeneration (Review). Int. J. Mol. Med. 2016, 37, 1439–1448. [Google Scholar] [CrossRef] [PubMed]
- Meeker, R.B.; Williams, K.S. The P75 Neurotrophin Receptor: At the Crossroad of Neural Repair and Death. Neural Regen. Res. 2015, 10, 721. [Google Scholar] [CrossRef] [PubMed]
- Mitre, M.; Mariga, A.; Chao, M.V. Neurotrophin Signalling: Novel Insights into Mechanisms and Pathophysiology. Clin. Sci. 2016, 131, 13–23. [Google Scholar] [CrossRef]
- Staszkiewicz, R.; Sobański, D.; Bryś, K.; Och, W.; Garczarek, M.; Ulasavets, U.; Stasiowski, M.; Dammermann, W.; Strojny, D.; Grabarek, B.O. Effect of Glycemic Disorders and Habits on the Concentration of Selected Neurotrophic Factors in Patients with Lumbosacral Intervertebral Disc Degeneration. Curr. Pharm. Biotechnol. 2023, in press. [Google Scholar] [CrossRef]
- Jackson, A.R.; Dhawale, A.A.; Brown, M.D. Association between Intervertebral Disc Degeneration and Cigarette Smoking: Clinical and Experimental Findings. JBJS Rev. 2015, 3, e2. [Google Scholar] [CrossRef]
- Elmasry, S.; Asfour, S.; de Rivero Vaccari, J.P.; Travascio, F. Effects of Tobacco Smoking on the Degeneration of the Intervertebral Disc: A Finite Element Study. PLoS ONE 2015, 10, e0136137. [Google Scholar] [CrossRef]
- Chen, Z.; Li, X.; Pan, F.; Wu, D.; Li, H. A Retrospective Study: Does Cigarette Smoking Induce Cervical Disc Degeneration? Int. J. Surg. 2018, 53, 269–273. [Google Scholar] [CrossRef]
- Kiraz, M.; Demir, E. Relationship of Lumbar Disc Degeneration with Hemoglobin Value and Smoking. Neurochirurgie 2020, 66, 373–377. [Google Scholar] [CrossRef]
- Sampara, P.; Banala, R.R.; Vemuri, S.K.; Av, G.R.; Gpv, S. Understanding the Molecular Biology of Intervertebral Disc Degeneration and Potential Gene Therapy Strategies for Regeneration: A Review. Gene Ther. 2018, 25, 67–82. [Google Scholar] [CrossRef]
- Boissoneault, J.; Lewis, B.; Nixon, S.J. Characterizing Chronic Pain and Alcohol Use Trajectory among Treatment-Seeking Alcoholics. Alcohol 2019, 75, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Karimi, R.; Mallah, N.; Nedjat, S.; Beasley, M.J.; Takkouche, B. Association between Alcohol Consumption and Chronic Pain: A Systematic Review and Meta-Analysis. Br. J. Anaesth. 2022, 129, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Kapetanakis, S.; Gkantsinikoudis, N.; Chaniotakis, C.; Charitoudis, G.; Givissis, P. Percutaneous Transforaminal Endoscopic Discectomy for the Treatment of Lumbar Disc Herniation in Obese Patients: Health-Related Quality of Life Assessment in a 2-Year Follow-Up. World Neurosurg. 2018, 113, e638–e649. [Google Scholar] [CrossRef] [PubMed]
- Zingg, R.W.; Kendall, R. Obesity, Vascular Disease, and Lumbar Disk Degeneration: Associations of Comorbidities in Low Back Pain. PMR 2017, 9, 398–402. [Google Scholar] [CrossRef]
- Özcan-Ekşi, E.E.; Kara, M.; Berikol, G.; Orhun, Ö.; Turgut, V.U.; Ekşi, M.Ş. A New Radiological Index for the Assessment of Higher Body Fat Status and Lumbar Spine Degeneration. Skelet. Radiol. 2022, 51, 1261–1271. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kim, W.; Lee, S.-U.; Choi, K.H. Relationship between Obesity and Lumbar Spine Degeneration: A Cross-Sectional Study from the Fifth Korean National Health and Nutrition Examination Survey, 2010–2012. Metab. Syndr. Relat. Disord. 2019, 17, 60–66. [Google Scholar] [CrossRef]
- Jakoi, A.M.; Pannu, G.; D’oro, A.; Buser, Z.; Pham, M.H.; Patel, N.N.; Hsieh, P.C.; Liu, J.C.; Acosta, F.L.; Hah, R. The Clinical Correlations between Diabetes, Cigarette Smoking and Obesity on Intervertebral Degenerative Disc Disease of the Lumbar Spine. Asian Spine J. 2017, 11, 337. [Google Scholar] [CrossRef]
- Russo, F.; Ambrosio, L.; Ngo, K.; Vadalà, G.; Denaro, V.; Fan, Y.; Sowa, G.; Kang, J.D.; Vo, N. The Role of Type I Diabetes in Intervertebral Disc Degeneration. Spine 2019, 44, 1177–1185. [Google Scholar] [CrossRef]
- Mahmoud, M.; Kokozidou, M.; Auffarth, A.; Schulze-Tanzil, G. The Relationship between Diabetes Mellitus Type II and Intervertebral Disc Degeneration in Diabetic Rodent Models: A Systematic and Comprehensive Review. Cells 2020, 9, 2208. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Ballantyne, C.M. Metabolic Inflammation and Insulin Resistance in Obesity. Circ. Res. 2020, 126, 1549–1564. [Google Scholar] [CrossRef] [PubMed]
- Wondmkun, Y.T. Obesity, Insulin Resistance, and Type 2 Diabetes: Associations and Therapeutic Implications. Diabetes Metab. Syndr. Obes. 2020, 13, 3611–3616. [Google Scholar] [CrossRef] [PubMed]
- Staszkiewicz, R.; Gralewski, M.; Gładysz, D.; Bryś, K.; Garczarek, M.; Gadzieliński, M.; Marcol, W.; Sobański, D.; Grabarek, B.O. Evaluation of the Concentration of Growth Associated Protein-43 and Glial Cell-Derived Neurotrophic Factor in Degenerated Intervertebral Discs of the Lumbosacral Region of the Spine. Mol. Pain 2023, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Staszkiewicz, R.; Gładysz, D.; Gralewski, M.; Bryś, K.; Garczarek, M.; Gadzieliński, M.; Marcol, W.; Sobański, D.; Grabarek, B.O. Usefulness of Detecting Brain-Derived Neurotrophic Factor in Intervertebral Disc Degeneration of the Lumbosacral Spine. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2023, 29, e938663-1–e938663-13. [Google Scholar] [CrossRef]
- Ustawa z Dnia 1 Lipca 2005 r. o Pobieraniu, Przechowywaniu i Przeszczepianiu Komórek, Tkanek i Narządów. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=wdu20051691411 (accessed on 9 February 2024).
- Pfirrmann, C.W.; Metzdorf, A.; Zanetti, M.; Hodler, J.; Boos, N. Magnetic Resonance Classification of Lumbar Intervertebral Disc Degeneration. Spine 2001, 26, 1873–1878. [Google Scholar] [CrossRef]
- Staszkiewicz, R.; Ulasavets, U.; Dobosz, P.; Drewniak, S.; Niewiadomska, E.; Grabarek, B.O. Assessment of Quality of Life, Pain Level and Disability Outcomes after Lumbar Discectomy. Sci. Rep. 2023, 13, 6009. [Google Scholar] [CrossRef]
- Baumgartner, L.; Wuertz-Kozak, K.; Le Maitre, C.L.; Wignall, F.; Richardson, S.M.; Hoyland, J.; Ruiz Wills, C.; González Ballester, M.A.; Neidlin, M.; Alexopoulos, L.G.; et al. Multiscale Regulation of the Intervertebral Disc: Achievements in Experimental, In Silico, and Regenerative Research. Int. J. Mol. Sci. 2021, 22, 703. [Google Scholar] [CrossRef]
- Li, H.; Liu, H.; Zhang, N.; Zhu, Z. Involvement of the G-Protein-Coupled Receptor 4 in the Increased Expression of RANK/RANKL/OPG System and Neurotrophins by Nucleus Pulposus Cells under the Degenerated Intervertebral Disc-Like Acidic Microenvironment. BioMed Res. Int. 2020, 2020, e1328436. [Google Scholar] [CrossRef]
- Moghanlou, A.E.; Yazdanian, M.; Roshani, S.; Demirli, A.; Seydyousefi, M.; Metz, G.A.S.; Faghfoori, Z. Neuroprotective Effects of Pre-Ischemic Exercise Are Linked to Expression of NT-3/NT-4 and TrkB/TrkC in Rats. Brain Res. Bull. 2023, 194, 54–63. [Google Scholar] [CrossRef]
- de Miranda, A.S.; de Barros, J.L.V.M.; Teixeira, A.L. Is Neurotrophin-3 (NT-3): A Potential Therapeutic Target for Depression and Anxiety? Expert Opin. Ther. Targets 2020, 24, 1225–1238. [Google Scholar] [CrossRef] [PubMed]
- Galvez-Sánchez, C.M.; Montoro, C.I.; Duschek, S.; Reyes del Paso, G.A. Depression and Trait-Anxiety Mediate the Influence of Clinical Pain on Health-Related Quality of Life in Fibromyalgia. J. Affect. Disord. 2020, 265, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Michaelides, A.; Zis, P. Depression, Anxiety and Acute Pain: Links and Management Challenges. Postgrad. Med. 2019, 131, 438–444. [Google Scholar] [CrossRef] [PubMed]
- The Evolution of Nerve Growth Factor Inhibition in Clinical Medicine. Nature Reviews Rheumatology. Available online: https://www.nature.com/articles/s41584-020-00528-4 (accessed on 17 June 2023).
- Carvalho, C.R.; Oliveira, J.M.; Reis, R.L. Modern Trends for Peripheral Nerve Repair and Regeneration: Beyond the Hollow Nerve Guidance Conduit. Front. Bioeng. Biotechnol. 2019, 7, 337. [Google Scholar] [CrossRef] [PubMed]
- Sahenk, Z.; Galloway, G.; Clark, K.R.; Malik, V.; Rodino-Klapac, L.R.; Kaspar, B.K.; Chen, L.; Braganza, C.; Montgomery, C.; Mendell, J.R. AAV1.NT-3 Gene Therapy for Charcot–Marie–Tooth Neuropathy. Mol. Ther. 2014, 22, 511–521. [Google Scholar] [CrossRef] [PubMed]
- Omura, T.; Sano, M.; Omura, K.; Hasegawa, T.; Doi, M.; Sawada, T.; Nagano, A. Different Expressions of BDNF, NT3, and NT4 in Muscle and Nerve after Various Types of Peripheral Nerve Injuries. J. Peripher. Nerv. Syst. 2005, 10, 293–300. [Google Scholar] [CrossRef]
- Wang, T.; Zhang, J.; Li, P.; Ding, Y.; Tang, J.; Chen, G.; Zhang, J.H. NT-4 Attenuates Neuroinflammation via TrkB/PI3K/FoxO1 Pathway after Germinal Matrix Hemorrhage in Neonatal Rats. J. Neuroinflamm. 2020, 17, 158. [Google Scholar] [CrossRef]
- Omar, N.A.; Kumar, J.; Teoh, S.L. Neurotrophin-3 and Neurotrophin-4: The Unsung Heroes That Lies behind the Meninges. Neuropeptides 2022, 92, 102226. [Google Scholar] [CrossRef]
- Lambert, S.A.; Jolma, A.; Campitelli, L.F.; Das, P.K.; Yin, Y.; Albu, M.; Chen, X.; Taipale, J.; Hughes, T.R.; Weirauch, M.T. The Human Transcription Factors. Cell 2018, 172, 650–665. [Google Scholar] [CrossRef]
- Cramer, P. Organization and Regulation of Gene Transcription. Nature 2019, 573, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Yang, F.; Jin, H.; Wang, X. The Regulation of Protein Translation and Its Implications for Cancer. Signal Transduct. Target. Ther. 2021, 6, 68. [Google Scholar] [CrossRef] [PubMed]
- Riba, A.; Di Nanni, N.; Mittal, N.; Arhné, E.; Schmidt, A.; Zavolan, M. Protein Synthesis Rates and Ribosome Occupancies Reveal Determinants of Translation Elongation Rates. Proc. Natl. Acad. Sci. USA 2019, 116, 15023–15032. [Google Scholar] [CrossRef] [PubMed]
- Michlewski, G.; Cáceres, J.F. Post-Transcriptional Control of miRNA Biogenesis. RNA 2019, 25, 1–16. [Google Scholar] [CrossRef]
- Jens, M.; Rajewsky, N. Competition between Target Sites of Regulators Shapes Post-Transcriptional Gene Regulation. Nat. Rev. Genet. 2015, 16, 113–126. [Google Scholar] [CrossRef]
- Wang, C.; Han, B.; Zhou, R.; Zhuang, X. Real-Time Imaging of Translation on Single mRNA Transcripts in Live Cells. Cell 2016, 165, 990–1001. [Google Scholar] [CrossRef]
- Ye, J.; Xu, M.; Tian, X.; Cai, S.; Zeng, S. Research Advances in the Detection of miRNA. J. Pharm. Anal. 2019, 9, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Zhao, Y.; Yang, S.; Zhang, H.; Chen, F. Integrative Analysis of miRNA-mRNA and miRNA-miRNA Interactions. BioMed Res. Int. 2014, 2014, e907420. [Google Scholar] [CrossRef] [PubMed]
- Ihara, C.; Shimatsu, A.; Mizuta, H.; Murabe, H.; Nakamura, Y.; Nakao, K. Decreased Neurotrophin-3 Expression in Skeletal Muscles of Streptozotocin-Induced Diabetic Rats. Neuropeptides 1996, 30, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xia, B.; Li, R.; Yin, D.; Wang, Y.; Liang, W. Expression of Brain-Derived Neurotrophic Factors, Neurotrophin-3, and Neurotrophin-4 in the Nucleus Accumbens during Heroin Dependency and Withdrawal. Neuroreport 2017, 28, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Chimbar, L.; Moleta, Y. Naloxone Effectiveness: A Systematic Review. J. Addict. Nurs. 2018, 29, 167–171. [Google Scholar] [CrossRef]
- Miller, M.W.; Mooney, S.M. Chronic Exposure to Ethanol Alters Neurotrophin Content in the Basal Forebrain-Cortex System in the Mature Rat: Effects on Autocrine-Paracrine Mechanisms. J. Neurobiol. 2004, 60, 490–498. [Google Scholar] [CrossRef]
- Requena-Ocaña, N.; Araos, P.; Flores, M.; García-Marchena, N.; Silva-Peña, D.; Aranda, J.; Rivera, P.; Ruiz, J.J.; Serrano, A.; Pavón, F.J.; et al. Evaluation of Neurotrophic Factors and Education Level as Predictors of Cognitive Decline in Alcohol Use Disorder. Sci. Rep. 2021, 11, 15583. [Google Scholar] [CrossRef]
- Silva-Peña, D.; García-Marchena, N.; Alén, F.; Araos, P.; Rivera, P.; Vargas, A.; García-Fernández, M.I.; Martín-Velasco, A.I.; Villanúa, M.Á.; Castilla-Ortega, E.; et al. Alcohol-Induced Cognitive Deficits Are Associated with Decreased Circulating Levels of the Neurotrophin BDNF in Humans and Rats. Addict. Biol. 2019, 24, 1019–1033. [Google Scholar] [CrossRef]
- Yang, J.-T.; Chang, C.-N.; Wu, J.H.; Chung, C.-Y.; Weng, H.-H.; Cheng, W.-C.; Lee, T.-H. Cigarette Smoking Decreases Neurotrophin-3 Expression in Rat Hippocampus after Transient Forebrain Ischemia. Neurosci. Res. 2008, 60, 431–438. [Google Scholar] [CrossRef]
- Kimata, H. Passive Smoking Elevates Neurotrophin Levels in Tears. Hum. Exp. Toxicol. 2004, 23, 215–217. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Aged > 18 years old | Aged < 18 years old |
| Lumbosacral spine-isolated IVD degeneration of a prolapse/extrusion character determined using magnetic resonance imaging | IVD degeneration in the lumbosacral spine of a protrusion or sequestration character determined using magnetic resonance imaging |
| Discogenic pain and/or symptomatic sciatica without improvement after non-surgical treatment for at least 6 weeks | Previous surgical procedures due to IVD degeneration in the lumbosacral spine |
| No other coexisting pathologies of the spine | Inflammatory and autoimmune diseases |
| Condition after spine injury | |
| Dementia/mental disorders | |
| Polyneuropathy | |
| Pregnancy | |
| Coexisting diseases, including metabolic diseases | |
| Neoplasms: metastatic tumors in the spine; lymphoma; leukemia; spinal cord tumors; retroperitoneal tumors; and primary shaft tumors | |
| Inflammatory diseases: inflammation of the bone elements of the spine | |
| Osteoporosis | |
| Disease duration of no longer than 12 weeks | Disease duration exceeding 12 weeks or of less than 6 weeks |
| Inflammatory disease history |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Up to 45 years of age | Over 45 years of age |
| No signs of degeneration in the collected material during microscopic examination | Features of degeneration in the collected material during microscopic examination (hematoxylin and eosin staining) |
| No neoplastic disease history | Neoplastic disease history |
| No inflammatory diseases: inflammation of the bone elements of the spine (osteomyelitis); IVD inflammation; epidural empyema; shingles; arthritis; inflammatory infiltrates of the rectum; Scheuermann’s disease; and Paget’s disease | Spinal disease history |
| mRNA | Oligonucleotide Sequence |
|---|---|
| NT-3 | Forward: 5′-CGTGGTGGCGAACAGAACAT-3′ Reverse 5′-GGCCGATGACTTGTCGGTC-3′ |
| NT-4 | Forward: 5′-CTGTGTGCGATGCAGTCAGT-3′ Reverse 5′-GCAGCGGGTTTCAAAGAAGT-3′ |
| GAPDH | Forward: 5′-GGTGAAGGTCGGAGTCAACGGA-3′ Reverse 5′-GAGGGATCTCGCTCCTGGAAGA-3′ |
| Neurotrophin | The Advancement of Changes | Fold Change (mRNA) | Protein Concentration (pg/mL) |
|---|---|---|---|
| NT-3 | Pfirrmann 2 | 7.21 ± 1.98 a | 45.98 ± 7.18 a |
| Pfirrmann 3 | 11/12 ± 1/17 | 245.98 ± 9.87 | |
| Pfirrmann 4 | 10.9 ± 1.76 b,c,d,e | 202.98 ± 13.12 b,c,d,e | |
| Pfirrmann 5 | 7.26 ± 2.87 | 43.91 ± 4.87 | |
| NT-4 | Pfirrmann 2 | 0.26 ± 0.03 | 187.98 ± 13.23 |
| Pfirrmann 3 | 0.43 ± 0.08 | 456.99 ± 13.41 | |
| Pfirrmann 4 | 0.42 ± 0.11 | 498.18 ± 10.87 | |
| Pfirrmann 5 | 0.22 ± 0.04 | 123.91 ± 8.76 |
| Neurotrophin | Pain Intensity on the VAS | Fold Change (mRNA) | Protein Concentration (pg/mL) | ANOVA (p) b |
|---|---|---|---|---|
| NT-3 | 2 | 3/11 | <corner detection | 0.114 a 0.654 b |
| 3 | 2.98 | <corner detection | ||
| 4 | 14.76 | 134.98 ± 4.65 | ||
| 5 | 16.78 | 201.12 ± 5.67 | ||
| 6 | 7/98 | 31.87 ± 5.67 | ||
| 7 | 8.76 | 8.98 ± 2.34 | ||
| 8 | 8/98 | 8.91 ± 2.91 | ||
| 9 | 9.65 | 14.98 ± 3.45 | ||
| 10 | 9/12 | 23.19 ± 6.78 | ||
| NT-4 | 2 | 0.41 | <corner detection | 0.118 a 0.787 b |
| 3 | 0.23 | <corner detection | ||
| 4 | 0.21 | <corner detection | ||
| 5 | 0.62 | 419.98 ± 21.54 | ||
| 6 | 0.61 | 408.17 ± 18.17 | ||
| 7 | 0.25 | 210.87 ± 6.76 | ||
| 8 | 0.27 | 187.98 ± 12.87 | ||
| 9 | 0.26 | 203.13 ± 10.98 | ||
| 10 | 0.15 | 89.09 ± 13.87 |
| Protein | Comparison | mRNA | Student’s t-Test 1 or ANOVA2 (Study Group) | Protein | Student’s t-Test 1 or ANOVA2 (Control Group) | |
|---|---|---|---|---|---|---|
| NT-3 | Gender | Female (n = 43) | 9/19 ± 1/12 | 0.761 1 | 0.36 ± 0.04 | 0.981 1 |
| Male (n = 38) | 9/04 ± 0.97 | 0.39 ± 0.05 | ||||
| BMI (kg/m2) | Normal (n = 54) | 7.29 ±1.54 | 0.009 2 | 0.12 ± 0.05 | <0.0001 2 | |
| Overweight (n = 42) | 8/08 ±1/23 | 0.40 ± 0.09 | ||||
| Obesity (n = 17) | 12.00 ± 1.54 | 0.47 ± 0.09 | ||||
| Diabetes | No (n = 91) | 5.78 ± 1.01 | <0.0001 1 | 0.23 ± 0.10 | 0.023 1 | |
| Yes (n = 22) | 12.45 ± 2.02 | 0.43 ± 0.08 | ||||
| Smoking | No (n = 77) | 8/11 ± 2/12 | <0.008 1 | 0.42 ± 0.11 | 0.004 1 | |
| Yes (n =36) | 10.12 ± 2.34 | 0.23 ± 0.07 | ||||
| Drinking alcohol | No (n = 8) | 11.77 ± 1.77 | 0.876 1 | 0.52 ± 0.12 | <0.0001 1 | |
| Yes (n = 105) | 6.89 ± 1.21 | 0.13 ± 0.06 | ||||
| NT-4 | Gender | Female (n = 43) | 135.65 ± 5.17 | 0.765 1 | 320.87 ± 11.09 | 0.376 1 |
| Male (n = 38) | 133.76 ± 5.34 | 312.67 ± 8.12 | ||||
| BMI (kg/m2) | Normal (n = 54) | 116.06 ± 5.08 | <0.0001 2 | 288.22 ± 9.31 | 0.009 2 | |
| Overweight (n = 42) | 139.97 ± 7.12 | 319.17 ± 10.19 | ||||
| Obesity (n = 17) | 148.11 ± 3.19 | 342.91 ± 6.87 | ||||
| Diabetes | No (n = 91) | 118.60 ± 2.01 | <0.0001 1 | 288.01 ± 4.13 | <0.0001 1 | |
| Yes (n = 22) | 150.84 ± 1.76 | 345.53 ± 5.28 | ||||
| Smoking | No (n = 77) | 120.19 ± 2.76 | <0.0001 1 | 281.75 ± 0.43 | <0.0001 1 | |
| Yes (n =36) | 149.22 ± 4.54 | 351.79 ± 0.65 | ||||
| Drinking alcohol | No (n = 8) | 135.32 ± 3.87 | 0.049 1 | 281.16 ± 8.41 | <0.0001 1 | |
| Yes (n = 105) | 134.11 ± 2.19 | 352.37 ± 9.18 | ||||
| Neurotrophin | Characteristic | Expression Level | Linear Regression | Multiple Regression | |||
|---|---|---|---|---|---|---|---|
| r | R2 | p-Value | Coefficient | p-Value | |||
| NT-3 | Sex | mRNA | 0.31 | 0.07 | 0.231 | ||
| Protein | 0.29 | 0.09 | 0.276 | ||||
| BMI (kg/m2) | mRNA | 0.79 | 0.61 | <0.0001 | 0.3411 | <0.0001 | |
| Protein | 0.80 | 0.65 | <0.0001 | 0.408 | <0.0001 | ||
| Diabetes | mRNA | 0.71 | 0.76 | <0.0001 | 0.321 | 0.015 | |
| Protein | 0.76 | 0.74 | <0.0001 | 0.308 | 0.021 | ||
| Smoking | mRNA | 0.87 | 0.45 | 0.001 | 0.476 | 0.024 | |
| Protein | 0.89 | 0.41 | 0.003 | 0.487 | 0.021 | ||
| Drinking alcohol | mRNA | 0.56 | 0.39 | 0.024 | 0.234 | 0.028 | |
| Protein | 0.54 | 0.42 | 0.023 | 0.265 | 0.029 | ||
| NT-4 | Sex | mRNA | 0.21 | 0.02 | 0.421 | ||
| Protein | 0.18 | 0.02 | 0.476 | ||||
| BMI (kg/m2) | mRNA | 0.81 | 0.87 | <0.0001 | 0.410 | 0.018 | |
| Protein | 0.78 | 0.81 | <0.0001 | 0.421 | 0.021 | ||
| Diabetes | mRNA | 0.56 | 0.39 | <0.0001 | 0.318 | 0.017 | |
| Protein | 0.56 | 0.38 | <0.0001 | 0.321 | 0.021 | ||
| Smoking | mRNA | 0.80 | 0.45 | 0.009 | 0.309 | 0.024 | |
| Protein | 0.81 | 0.54 | 0.003 | 0.319 | 0.029 | ||
| Drinking alcohol | mRNA | 0.54 | 0.21 | 0.031 | 0.151 | 0.017 | |
| Protein | 0.41 | 0.23 | 0.029 | 0.168 | 0.020 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Staszkiewicz, R.; Gładysz, D.; Sobański, D.; Bolechała, F.; Golec, E.; Dammermann, W.; Grabarek, B.O. The Impacts of Intervertebral Disc Degeneration of the Spine, Alcohol Consumption, Smoking Tobacco Products, and Glycemic Disorders on the Expression Profiles of Neurotrophins-3 and -4. Biomedicines 2024, 12, 427. https://doi.org/10.3390/biomedicines12020427
Staszkiewicz R, Gładysz D, Sobański D, Bolechała F, Golec E, Dammermann W, Grabarek BO. The Impacts of Intervertebral Disc Degeneration of the Spine, Alcohol Consumption, Smoking Tobacco Products, and Glycemic Disorders on the Expression Profiles of Neurotrophins-3 and -4. Biomedicines. 2024; 12(2):427. https://doi.org/10.3390/biomedicines12020427
Chicago/Turabian StyleStaszkiewicz, Rafał, Dorian Gładysz, Dawid Sobański, Filip Bolechała, Edward Golec, Werner Dammermann, and Beniamin Oskar Grabarek. 2024. "The Impacts of Intervertebral Disc Degeneration of the Spine, Alcohol Consumption, Smoking Tobacco Products, and Glycemic Disorders on the Expression Profiles of Neurotrophins-3 and -4" Biomedicines 12, no. 2: 427. https://doi.org/10.3390/biomedicines12020427