
Silent Myocardial Ischemia: From Pathophysiology to Diagnosis and Treatment

 , , , ,
, , , ,
Abstract
:1. Introduction
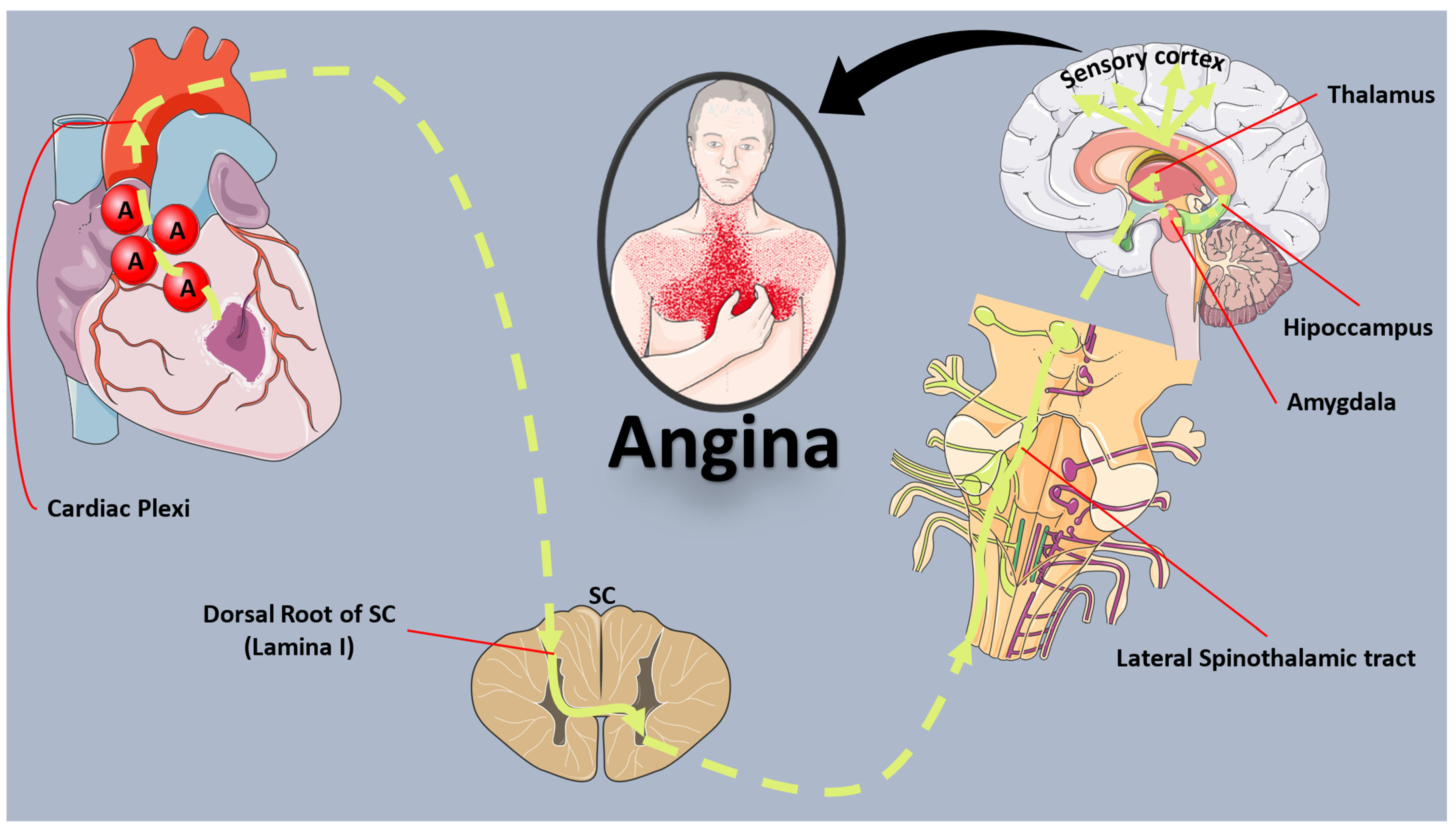
2. Mechanisms of Ischemic Cardiac Pain
3. Mechanisms of Silent Myocardial Ischemia
4. Epidemiology and Prognosis of Silent Myocardial Ischemia and Infarction
5. Screening and Diagnosis of Silent Ischemia
5.1. Exercise Treadmill Test
5.2. Echocardiography
5.3. Cardiac MRI
5.4. Single-Photon Emission Computed Tomography
5.5. Positron Emission Tomography
5.6. Silent Myocardial Ischemia Screening after Revascularization
6. Management of Silent Myocardial Ischemia
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Vaduganathan, M.; Mensah, G.A.; Turco, J.V.; Fuster, V.; Roth, G.A. The Global Burden of Cardiovascular Diseases and Risk: A Compass for Future Health. J. Am. Coll. Cardiol. 2022, 80, 2361–2371. [Google Scholar] [CrossRef] [PubMed]
- Theofilis, P.; Oikonomou, E.; Sagris, M.; Papageorgiou, N.; Tsioufis, K.; Tousoulis, D. Novel Concepts in the Management of Angina in Coronary Artery Disease. Curr. Pharm. Des. 2023, 29, 1825–1834. [Google Scholar] [CrossRef] [PubMed]
- Cohn, P.F.; Fox, K.M.; Daly, C. Silent myocardial ischemia. Circulation 2003, 108, 1263–1277. [Google Scholar] [CrossRef] [PubMed]
- Wink, J.; van Delft, R.; Notenboom, R.G.E.; Wouters, P.F.; DeRuiter, M.C.; Plevier, J.W.M.; Jongbloed, M.R.M. Human adult cardiac autonomic innervation: Controversies in anatomical knowledge and relevance for cardiac neuromodulation. Auton. Neurosci. 2020, 227, 102674. [Google Scholar] [CrossRef]
- Leach, A.; Fisher, M. Myocardial ischaemia and cardiac pain—A mysterious relationship. Br. J. Pain. 2013, 7, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Indolfi, C.; Polimeni, A.; Mongiardo, A.; De Rosa, S.; Spaccarotella, C. Old unsolved problems: When and how to treat silent ischaemia. Eur. Heart J. Suppl. 2020, 22, L82–L85. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.H.; Shankar, K.; Eftekhari, H.; Munir, M.; Robertson, J.; Brewer, A.; Stupin, I.V.; Casscells, S.W. Silent myocardial ischemia: Current perspectives and future directions. Exp. Clin. Cardiol. 2007, 12, 189–196. [Google Scholar]
- Cohn, P.F. Silent myocardial ischemia: Classification, prevalence, and prognosis. Am. J. Med. 1985, 79, 2–6. [Google Scholar] [CrossRef]
- Hamdan, M.; Kossaify, A. Silent Myocardial Ischemia Revisited, Another Silent Killer, Emphasis on the Diagnostic Value of Stress Echocardiography with Focused Update and Review. Adv. Biomed. Res. 2023, 12, 245. [Google Scholar] [CrossRef]
- Foreman, R.D.; Garrett, K.M.; Blair, R.W. Mechanisms of cardiac pain. Compr. Physiol. 2015, 5, 929–960. [Google Scholar] [CrossRef]
- Langer, A.; Freeman, M.R.; Josse, R.G.; Armstrong, P.W. Metaiodobenzylguanidine imaging in diabetes mellitus: Assessment of cardiac sympathetic denervation and its relation to autonomic dysfunction and silent myocardial ischemia. J. Am. Coll. Cardiol. 1995, 25, 610–618. [Google Scholar] [CrossRef]
- Faerman, I.; Faccio, E.; Milei, J.; Nunez, R.; Jadzinsky, M.; Fox, D.; Rapaport, M. Autonomic neuropathy and painless myocardial infarction in diabetic patients. Histologic evidence of their relationship. Diabetes 1977, 26, 1147–1158. [Google Scholar] [CrossRef]
- Valensi, P.; Lorgis, L.; Cottin, Y. Prevalence, incidence, predictive factors and prognosis of silent myocardial infarction: A review of the literature. Arch. Cardiovasc. Dis. 2011, 104, 178–188. [Google Scholar] [CrossRef]
- Krantz, D.S.; Kop, W.J.; Gabbay, F.H.; Rozanski, A.; Barnard, M.; Klein, J.; Pardo, Y.; Gottdiener, J.S. Circadian variation of ambulatory myocardial ischemia. Triggering by daily activities and evidence for an endogenous circadian component. Circulation 1996, 93, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Theofilis, P.; Vlachakis, P.K.; Mantzouranis, E.; Sakalidis, A.; Chrysohoou, C.; Leontsinis, I.; Lazaros, G.; Dimitriadis, K.; Drakopoulou, M.; Vordoni, A.; et al. Acute Coronary Syndromes in Women: A Narrative Review of Sex-Specific Characteristics. Angiology 2023, 33197231218331. [Google Scholar] [CrossRef] [PubMed]
- Mfeukeu-Kuate, L.; Meyanui, V.A.; Jingi, A.M.; Ndobo-Koe, V.; Mballa, F.; Ntep-Gweth, M.; Etoga, M.E.; Noubiap, J.J.; Sobngwi, E.; Menanga, A. Prevalence and determinants of silent myocardial ischemia in patients with type 2 diabetes in Cameroon: A cross-sectional study. Pan Afr. Med. J. 2022, 42, 41. [Google Scholar] [CrossRef]
- Prasad, D.S.; Kabir, Z.; Revathi Devi, K.; Peter, P.S.; Das, B.C. Prevalence and RIsk factors for Silent Myocardial ischemia (PRISM): A clinico observational study in patients of type 2 diabetes. Indian. Heart J. 2019, 71, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.M.; Rautaharju, P.M.; Prineas, R.J.; Rodriguez, C.J.; Loehr, L.; Rosamond, W.D.; Kitzman, D.; Couper, D.; Soliman, E.Z. Race and Sex Differences in the Incidence and Prognostic Significance of Silent Myocardial Infarction in the Atherosclerosis Risk in Communities (ARIC) Study. Circulation 2016, 133, 2141–2148. [Google Scholar] [CrossRef] [PubMed]
- Sato, C.; Wakabayashi, K.; Ikeda, N.; Honda, Y.; Sato, K.; Suzuki, T.; Shibata, K.; Tanno, K. Influence of sex on the incidence of potential coronary artery disease and long-term outcomes in asymptomatic patients with diabetes mellitus. Int. J. Cardiol. Heart Vasc. 2020, 27, 100504. [Google Scholar] [CrossRef] [PubMed]
- Kaze, A.D.; Fonarow, G.C.; Echouffo-Tcheugui, J.B. Cardiac Autonomic Dysfunction and Risk of Silent Myocardial Infarction Among Adults With Type 2 Diabetes. J. Am. Heart Assoc. 2023, 12, e029814. [Google Scholar] [CrossRef]
- Honda, Y.; Wakabayashi, K.; Sato, C.; Ikeda, N.; Sato, K.; Suzuki, T.; Shibata, K.; Shinke, T. Chronic kidney disease is a key predictive factor for potential myocardial ischaemia and poor prognosis in asymptomatic patients with diabetes mellitus. Sci. Rep. 2022, 12, 10268. [Google Scholar] [CrossRef] [PubMed]
- Devereaux, P.J.; Xavier, D.; Pogue, J.; Guyatt, G.; Sigamani, A.; Garutti, I.; Leslie, K.; Rao-Melacini, P.; Chrolavicius, S.; Yang, H.; et al. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: A cohort study. Ann. Intern. Med. 2011, 154, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Puelacher, C.; Lurati Buse, G.; Seeberger, D.; Sazgary, L.; Marbot, S.; Lampart, A.; Espinola, J.; Kindler, C.; Hammerer, A.; Seeberger, E.; et al. Perioperative Myocardial Injury After Noncardiac Surgery: Incidence, Mortality, and Characterization. Circulation 2018, 137, 1221–1232. [Google Scholar] [CrossRef] [PubMed]
- Vascular Events in Noncardiac Surgery Patients Cohort Evaluation (VISION) Study Investigators; Spence, J.; LeManach, Y.; Chan, M.T.V.; Wang, C.Y.; Sigamani, A.; Xavier, D.; Pearse, R.; Alonso-Coello, P.; Garutti, I.; et al. Association between complications and death within 30 days after noncardiac surgery. CMAJ 2019, 191, E830–E837. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, T.; Smilowitz, N.R.; Xia, Y.; Beckman, J.A.; Berger, J.S. Cardiovascular Risk Factors and Perioperative Myocardial Infarction After Noncardiac Surgery. Can. J. Cardiol. 2021, 37, 224–231. [Google Scholar] [CrossRef]
- Cheng, Y.J.; Jia, Y.H.; Yao, F.J.; Mei, W.Y.; Zhai, Y.S.; Zhang, M.; Wu, S.H. Association Between Silent Myocardial Infarction and Long-Term Risk of Sudden Cardiac Death. J. Am. Heart Assoc. 2021, 10, e017044. [Google Scholar] [CrossRef]
- Singleton, M.J.; German, C.A.; Soliman, E.Z.; Burke, G.L.; Yeboah, J. The utility of silent myocardial infarction on electrocardiogram as an ASCVD risk enhancer for primary prevention: The multi-ethnic study of atherosclerosis. J. Electrocardiol. 2021, 65, 105–109. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Laukkanen, J.A.; Kurl, S.; Lakka, T.A.; Tuomainen, T.P.; Rauramaa, R.; Salonen, R.; Eranen, J.; Salonen, J.T. Exercise-induced silent myocardial ischemia and coronary morbidity and mortality in middle-aged men. J. Am. Coll. Cardiol. 2001, 38, 72–79. [Google Scholar] [CrossRef]
- Albenque, G.; Rusinaru, D.; Bellaiche, M.; Di Lena, C.; Gabrion, P.; Delpierre, Q.; Malaquin, D.; Tribouilloy, C.; Bohbot, Y. Resting Left Ventricular Global Longitudinal Strain to Identify Silent Myocardial Ischemia in Asymptomatic Patients with Diabetes Mellitus. J. Am. Soc. Echocardiogr. 2022, 35, 258–266. [Google Scholar] [CrossRef]
- Sozzi, F.B.; Elhendy, A.; Rizzello, V.; Biagini, E.; van Domburg, R.T.; Schinkel, A.F.; Bax, J.J.; Vourvouri, E.; Danzi, G.B.; Poldermans, D. Prognostic significance of myocardial ischemia during dobutamine stress echocardiography in asymptomatic patients with diabetes mellitus and no prior history of coronary events. Am. J. Cardiol. 2007, 99, 1193–1195. [Google Scholar] [CrossRef] [PubMed]
- Fateh-Moghadam, S.; Reuter, T.; Htun, P.; Plockinger, U.; Dietz, R.; Bocksch, W. Stress echocardiography for risk stratification of asymptomatic patients with type 2 diabetes mellitus. Int. J. Cardiol. 2009, 131, 288–290. [Google Scholar] [CrossRef] [PubMed]
- Cortigiani, L.; Gherardi, S.; Faggioni, M.; Bovenzi, F.; Picano, E.; Petersen, C.; Molinaro, S.; Sicari, R. Dual-Imaging Stress Echocardiography for Prognostic Assessment of High-Risk Asymptomatic Patients with Diabetes Mellitus. J. Am. Soc. Echocardiogr. 2017, 30, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Stacey, R.B.; Vera, T.; Morgan, T.M.; Jordan, J.H.; Whitlock, M.C.; Hall, M.E.; Vasu, S.; Hamilton, C.; Kitzman, D.W.; Hundley, W.G. Asymptomatic myocardial ischemia forecasts adverse events in cardiovascular magnetic resonance dobutamine stress testing of high-risk middle-aged and elderly individuals. J. Cardiovasc. Magn. Reson. 2018, 20, 75. [Google Scholar] [CrossRef] [PubMed]
- Pezel, T.; Garot, P.; Kinnel, M.; Unterseeh, T.; Hovasse, T.; Champagne, S.; Toupin, S.; Sanguineti, F.; Garot, J. Prognostic value of stress cardiovascular magnetic resonance in asymptomatic patients without known coronary artery disease. Eur. Radiol. 2021, 31, 6172–6183. [Google Scholar] [CrossRef] [PubMed]
- Wackers, F.J.; Young, L.H.; Inzucchi, S.E.; Chyun, D.A.; Davey, J.A.; Barrett, E.J.; Taillefer, R.; Wittlin, S.D.; Heller, G.V.; Filipchuk, N.; et al. Detection of silent myocardial ischemia in asymptomatic diabetic subjects: The DIAD study. Diabetes Care 2004, 27, 1954–1961. [Google Scholar] [CrossRef] [PubMed]
- Lacourciere, Y.; Cote, C.; Lefebvre, J.; Dumont, M. Noninvasive detection of silent coronary artery disease in patients with essential hypertension, alone or associated with type 2 diabetes mellitus, using dipyridamole stress 99mtechnetium-sestamibi myocardial perfusion imaging. Can. J. Cardiol. 2006, 22 (Suppl. A), 16A–21A. [Google Scholar] [PubMed]
- Zellweger, M.J.; Hachamovitch, R.; Kang, X.; Hayes, S.W.; Friedman, J.D.; Germano, G.; Berman, D.S. Threshold, incidence, and predictors of prognostically high-risk silent ischemia in asymptomatic patients without prior diagnosis of coronary artery disease. J. Nucl. Cardiol. 2009, 16, 193–200. [Google Scholar] [CrossRef]
- Yamasaki, Y.; Nakajima, K.; Kusuoka, H.; Izumi, T.; Kashiwagi, A.; Kawamori, R.; Shimamoto, K.; Yamada, N.; Nishimura, T. Prognostic value of gated myocardial perfusion imaging for asymptomatic patients with type 2 diabetes: The J-ACCESS 2 investigation. Diabetes Care 2010, 33, 2320–2326. [Google Scholar] [CrossRef]
- Xiao-Rong, Z.; Hui-Rong, Z.; Mei, L.; Zhen, Z.; Wei, L.; Jing, L.; Guang-Ran, Y.; Jian-Bo, Z.; Jin-Kui, Y. Risk of silent myocardial ischemia detected by single photon emission computed tomography (SPECT) among asymptomatic Chinese patients with type 2 diabetes. Medicine 2019, 98, e15618. [Google Scholar] [CrossRef]
- Patel, K.K.; Singh, A.; Peri-Okonny, P.A.; Patel, F.S.; Kennedy, K.F.; Sperry, B.W.; Thompson, R.C.; McGhie, A.I.; Spertus, J.A.; Shaw, L.J.; et al. Prevalence and Prognostic Importance of Abnormal Positron Emission Tomography Among Asymptomatic Patients With Diabetes Mellitus. JACC Cardiovasc. Imaging 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Kadoglou, N.P.E.; Papadopoulos, C.H.; Papadopoulos, K.G.; Karagiannis, S.; Karabinos, I.; Loizos, S.; Theodosis-Georgilas, A.; Aggeli, K.; Keramida, K.; Klettas, D.; et al. Updated knowledge and practical implementations of stress echocardiography in ischemic and non-ischemic cardiac diseases: An expert consensus of the Working Group of Echocardiography of the Hellenic Society of Cardiology. Hellenic. J. Cardiol. 2022, 64, 30–57. [Google Scholar] [CrossRef]
- Biagini, E.; Schinkel, A.F.; Bax, J.J.; Rizzello, V.; van Domburg, R.T.; Krenning, B.J.; Bountioukos, M.; Pedone, C.; Vourvouri, E.C.; Rapezzi, C.; et al. Long term outcome in patients with silent versus symptomatic ischaemia during dobutamine stress echocardiography. Heart 2005, 91, 737–742. [Google Scholar] [CrossRef] [PubMed]
- Jacqueminet, S.; Barthelemy, O.; Rouzet, F.; Isnard, R.; Halbron, M.; Bouzamondo, A.; Le Guludec, D.; Grimaldi, A.; Metzger, J.P.; Le Feuvre, C. A randomized study comparing isotope and echocardiography stress testing in the screening of silent myocardial ischaemia in type 2 diabetic patients. Diabetes Metab. 2010, 36, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Paraskevaidis, I.A.; Tsougos, E.; Panou, F.; Dagres, N.; Karatzas, D.; Boutati, E.; Varounis, C.; Kremastinos, D.T. Diastolic stress echocardiography detects coronary artery disease in patients with asymptomatic type II diabetes. Coron. Artery Dis. 2010, 21, 104–112. [Google Scholar] [CrossRef]
- Scatteia, A.; Dellegrottaglie, S. Cardiac magnetic resonance in ischemic cardiomyopathy: Present role and future directions. Eur. Heart J. Suppl. 2023, 25, C58–C62. [Google Scholar] [CrossRef]
- Emrich, T.; Halfmann, M.; Schoepf, U.J.; Kreitner, K.F. CMR for myocardial characterization in ischemic heart disease: State-of-the-art and future developments. Eur. Radiol. Exp. 2021, 5, 14. [Google Scholar] [CrossRef]
- Oikonomou, E.; Theofilis, P.; Lampsas, S.; Katsarou, O.; Kalogeras, K.; Marinos, G.; Tsatsaragkou, A.; Anastasiou, A.; Lysandrou, A.; Gounaridi, M.I.; et al. Current Concepts and Future Applications of Non-Invasive Functional and Anatomical Evaluation of Coronary Artery Disease. Life 2022, 12, 1803. [Google Scholar] [CrossRef]
- Ammar, K.A.; Rodeheffer, R.J. Reassessing the clinical significance of electrocardiographically unrecognized myocardial infarctions: Radionuclide infarct size and its impact on long-term prognosis. Ann. Noninvasive Electrocardiol. 2023, 28, e13088. [Google Scholar] [CrossRef]
- Georgoulias, P.; Demakopoulos, N.; Tzavara, C.; Giannakou, S.; Valotassiou, V.; Tsougos, I.; Xaplanteris, P.; Fezoulidis, I. Long-term prognostic value of Tc-99m tetrofosmin myocardial gated-SPECT imaging in asymptomatic patients after percutaneous coronary intervention. Clin. Nucl. Med. 2008, 33, 743–747. [Google Scholar] [CrossRef]
- Harb, S.C.; Cook, T.; Jaber, W.A.; Marwick, T.H. Exercise testing in asymptomatic patients after revascularization: Are outcomes altered? Arch. Intern. Med. 2012, 172, 854–861. [Google Scholar] [CrossRef] [PubMed]
- Aldweib, N.; Negishi, K.; Hachamovitch, R.; Jaber, W.A.; Seicean, S.; Marwick, T.H. Impact of repeat myocardial revascularization on outcome in patients with silent ischemia after previous revascularization. J. Am. Coll. Cardiol. 2013, 61, 1616–1623. [Google Scholar] [CrossRef] [PubMed]
- Zellweger, M.J.; Fahrni, G.; Ritter, M.; Jeger, R.V.; Wild, D.; Buser, P.; Kaiser, C.; Osswald, S.; Pfisterer, M.E.; Investigators, B. Prognostic value of “routine” cardiac stress imaging 5 years after percutaneous coronary intervention: The prospective long-term observational BASKET (Basel Stent Kosteneffektivitats Trial) LATE IMAGING study. JACC Cardiovasc. Interv. 2014, 7, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Erne, P.; Schoenenberger, A.W.; Zuber, M.; Burckhardt, D.; Kiowski, W.; Dubach, P.; Resink, T.; Pfisterer, M. Effects of anti-ischaemic drug therapy in silent myocardial ischaemia type I: The Swiss Interventional Study on Silent Ischaemia type I (SWISSI I): A randomized, controlled pilot study. Eur. Heart J. 2007, 28, 2110–2117. [Google Scholar] [CrossRef] [PubMed]
- Wackers, F.J.; Chyun, D.A.; Young, L.H.; Heller, G.V.; Iskandrian, A.E.; Davey, J.A.; Barrett, E.J.; Taillefer, R.; Wittlin, S.D.; Filipchuk, N.; et al. Resolution of asymptomatic myocardial ischemia in patients with type 2 diabetes in the Detection of Ischemia in Asymptomatic Diabetics (DIAD) study. Diabetes Care 2007, 30, 2892–2898. [Google Scholar] [CrossRef] [PubMed]
- Gosselin, G.; Teo, K.K.; Tanguay, J.F.; Gokhale, R.; Hartigan, P.M.; Maron, D.J.; Gupta, V.; Mancini, G.B.; Bates, E.R.; Chaitman, B.R.; et al. Effectiveness of percutaneous coronary intervention in patients with silent myocardial ischemia (post hoc analysis of the COURAGE trial). Am. J. Cardiol. 2012, 109, 954–959. [Google Scholar] [CrossRef] [PubMed]
- Koshy, A.N.; Dinh, D.T.; Fulcher, J.; Brennan, A.L.; Murphy, A.C.; Duffy, S.J.; Reid, C.M.; Ajani, A.E.; Freeman, M.; Hiew, C.; et al. Long-term mortality in asymptomatic patients with stable ischemic heart disease undergoing percutaneous coronary intervention. Am. Heart J. 2022, 244, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.H.; Lee, J.M.; Park, I.; Kim, J.; Rhee, T.M.; Hwang, D.; Park, J.; Park, T.K.; Yang, J.H.; Song, Y.B.; et al. Comparison of long-term clinical outcomes between revascularization versus medical treatment in patients with silent myocardial ischemia. Int. J. Cardiol. 2019, 277, 47–53. [Google Scholar] [CrossRef]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e18–e114. [Google Scholar] [CrossRef]


{kind=link}
| Type | Definition |
|---|---|
| I | Occurring in patients with asymptomatic coronary artery disease without collateral anginal symptoms. |
| II | Manifesting in patients with a history of myocardial infarction. |
| III | Observed in patients with concurrent or collateral manifestations of chronic stable angina, unstable angina, and vasospastic angina. |
| Author | Year | Population (Number of Participants) | Method | Findings |
|---|---|---|---|---|
| Laukkanen et al. [29] | 2001 | Men with no prior CAD (1769) | ETT | Prevalence of SMI during exercise: 15.3% SMI during exercise → 1.7-fold risk of ACS and 3.5-fold risk of CAD mortality |
| Albenque et al. [30] | 2022 | Asymptomatic, with DM and high-risk features (273) | TTE | OR 1.39 (95% CI 1.14–1.70) per percentage LV GLS increase for predictive positive stress echocardiography OR 5.16 (95% CI 1.96–13.59) for LV GLS worse than −18% for predictive positive stress echocardiography |
| Sozzi et al. [31] | 2007 | Asymptomatic, with DM and no prior CAD (161) | DSE | Ischemia prevalence: 28% Adverse events were higher in the presence of an abnormal DSE (24% vs. 11% at 5 years) |
| Fateh-Moghadam et al. [32] | 2009 | Asymptomatic, with type 2 DM (211) | ESE or DSE | SMI: 28.9% Positive SE associated with a 13.5-fold risk of MACCE. |
| Cortigiani et al. [33] | 2017 | Asymptomatic, high-risk patients with DM (230) | SE + LAD-CFVR | Ischemia or abnormal LAD-CFVR in 23% and was predictive of incident MACE (HR 6.12, 95% CI 3.22–11.62) |
| Stacey et al. [34] | 2018 | Asymptomatic, high-risk patients (327) | DS-cardiac MRI | SMI was predictive of future cardiovascular events/survival (adjusted HR: 4.07, 95% CI 1.95–8.73, p < 0.001) |
| Pezel et al. [35] | 2021 | Asymptomatic, high-risk patients (903) | Dipyridamole cardiac MRI | SMI: 12.2% SMI was an independent predictor of incident MACE (HR 6.66, 95% CI 4.41–9.23) and cardiovascular mortality (HR: 6.21, 95% CI 3.89–9.48) |
| DIAD [36] | 2004 | Asymptomatic, with type 2 DM (522) | Adenosine Tc-99m sestamibi SPECT | SMI: 22% Moderate/Large defects: 6% |
| Lacourciere et al. [37] | 2006 | Asymptomatic, with essential hypertension (543) | Dipyridamole Tc-99m sestamibi SPECT | Abnormal SSS: 28% Greater prevalence and severity of SMI in coexisting DM |
| Zellweger et al. [38] | 2009 | Asymptomatic, with no prior CAD (3664) | Exercise Tc-99m sestamibi SPECT | SMI: 21% Patients with high-risk ischemia had higher event rates at follow-up compared to lesser SMI (3.1% vs. 0.4%, p = 0.0001) |
| Yamasaki et al. [39] | 2010 | Asymptomatic, with type 2 DM and high-risk features (485) | Stress/Rest Tc-99m tetrofosmin SPECT | SSS ≥ 9 was independently associated with a higher incidence of MACE (HR 3.39, 95% CI 1.78–6.43, p = 0.0002) |
| Xiao-Rong et al. [40] | 2019 | Asymptomatic, with type 2 DM (614) | Adenosine Tc-99m sestamibi SPECT | SMI: 21.3% Predictors of SMI: male sex, diabetic retinopathy, LDL-C |
| Patel et al. [41] | 2023 | DM without known CAD (2730) | Rb-82 Rest/Stress PET | SMI: 30.5% (significant in 12.5%) Reduced MBFR in 62% of asymptomatic patients CMD present in approximately 33% irrespective of symptoms Reduced MBFR and not SMI or symptoms were predictive of incident death |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theofilis, P.; Antonopoulos, A.S.; Sagris, M.; Papanikolaou, A.; Oikonomou, E.; Tsioufis, K.; Tousoulis, D. Silent Myocardial Ischemia: From Pathophysiology to Diagnosis and Treatment. Biomedicines 2024, 12, 259. https://doi.org/10.3390/biomedicines12020259
Theofilis P, Antonopoulos AS, Sagris M, Papanikolaou A, Oikonomou E, Tsioufis K, Tousoulis D. Silent Myocardial Ischemia: From Pathophysiology to Diagnosis and Treatment. Biomedicines. 2024; 12(2):259. https://doi.org/10.3390/biomedicines12020259
Chicago/Turabian StyleTheofilis, Panagiotis, Alexios S. Antonopoulos, Marios Sagris, Aggelos Papanikolaou, Evangelos Oikonomou, Konstantinos Tsioufis, and Dimitris Tousoulis. 2024. "Silent Myocardial Ischemia: From Pathophysiology to Diagnosis and Treatment" Biomedicines 12, no. 2: 259. https://doi.org/10.3390/biomedicines12020259