
Mechanisms and Clinical Implications of Human Gut Microbiota-Drug Interactions in the Precision Medicine Era

Abstract
:1. Introduction
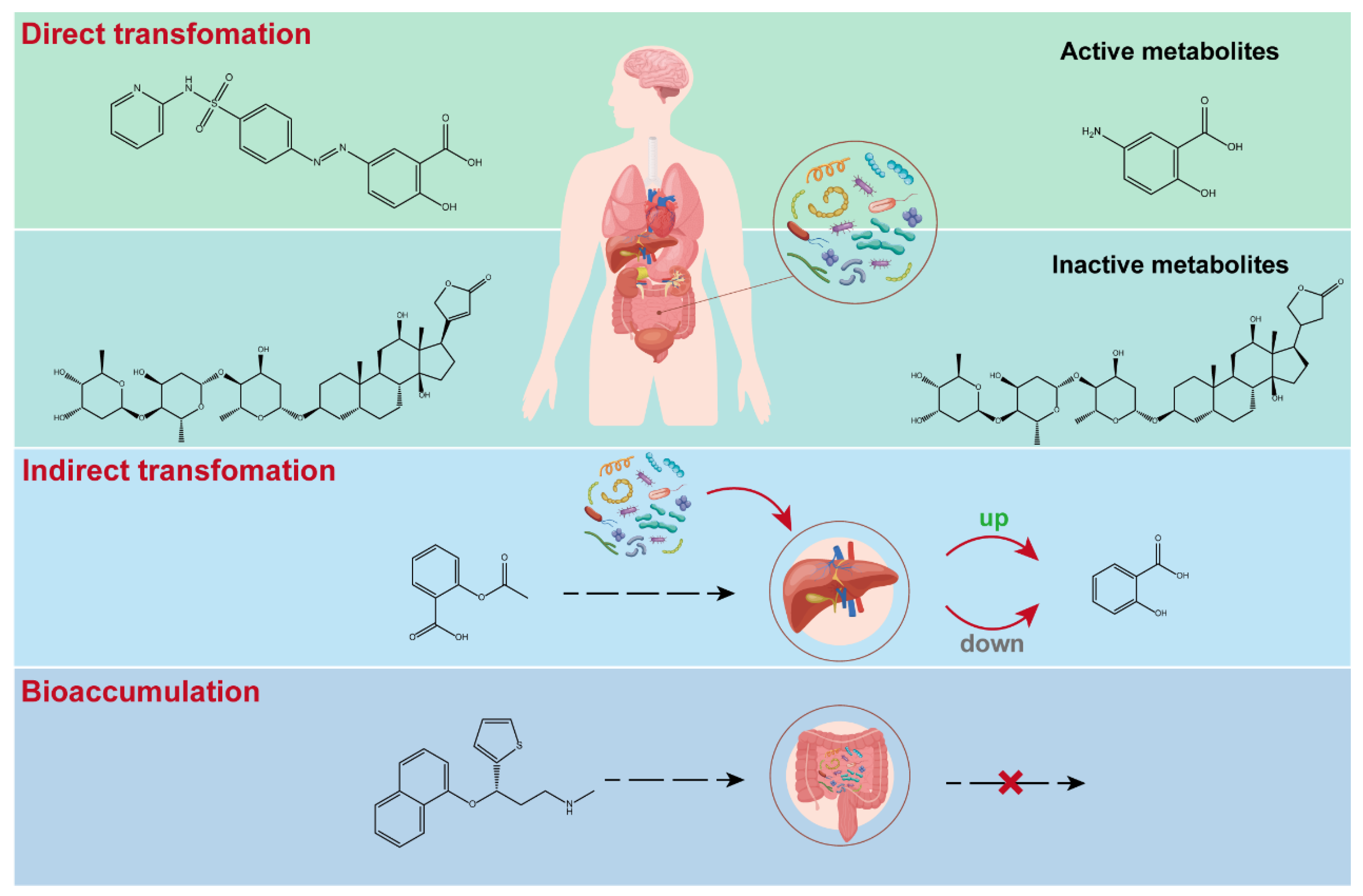
2. Molecular Mechanisms of Microbiota-Drug Interactions
2.1. Direct Metabolic Transformation of Drugs by Microbiota
2.2. Indirect Impact of Microbiota on Drug Metabolism
2.3. Bioaccumulation of Drugs in Microbiota
3. Impact of MDI on Drug Responses
3.1. Efficacy
3.2. Toxicity
3.3. Immune Modulation
3.4. Impact on COVID-19
3.5. Interindividual Variability
4. Clinical Implications of MDI
4.1. Modulation of Microbiota by Probiotics and Prebiotics
4.2. Pharmacomicrobiomics
4.3. Insights for Rational Drug Discovery
5. Challenges and Future Directions
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pant, A.; Maiti, T.K.; Mahajan, D.; Das, B. Human Gut Microbiota and Drug Metabolism. Microb. Ecol. 2023, 86, 97–111. [Google Scholar] [CrossRef]
- Wu, J.; Wang, K.; Wang, X.; Pang, Y.; Jiang, C. The role of the gut microbiome and its metabolites in metabolic diseases. Protein Cell 2021, 12, 360–373. [Google Scholar] [CrossRef]
- Chen, H.Q.; Gong, J.Y.; Xing, K.; Liu, M.Z.; Ren, H.; Luo, J.Q. Pharmacomicrobiomics: Exploiting the Drug-Microbiota Interactions in Antihypertensive Treatment. Front. Med. 2021, 8, 742394. [Google Scholar] [CrossRef]
- Weersma, R.K.; Zhernakova, A.; Fu, J. Interaction between drugs and the gut microbiome. Gut 2020, 69, 1510–1519. [Google Scholar] [CrossRef]
- Tsunoda, S.M.; Gonzales, C.; Jarmusch, A.K.; Momper, J.D.; Ma, J.D. Contribution of the Gut Microbiome to Drug Disposition, Pharmacokinetic and Pharmacodynamic Variability. Clin. Pharmacokinet. 2021, 60, 971–984. [Google Scholar] [CrossRef] [PubMed]
- Clayton, T.A.; Baker, D.; Lindon, J.C.; Everett, J.R.; Nicholson, J.K. Pharmacometabonomic identification of a significant host-microbiome metabolic interaction affecting human drug metabolism. Proc. Natl. Acad. Sci. USA 2009, 106, 14728–14733. [Google Scholar] [CrossRef] [PubMed]
- Wilson, I.D.; Nicholson, J.K. Gut microbiome interactions with drug metabolism, efficacy, and toxicity. Transl. Res. 2017, 179, 204–222. [Google Scholar] [CrossRef] [PubMed]
- Enright, E.F.; Gahan, C.G.; Joyce, S.A.; Griffin, B.T. Focus: Microbiome: The impact of the gut microbiota on drug metabolism and clinical outcome. Yale J. Biol. Med. 2016, 89, 375. [Google Scholar]
- Seekatz, A.M.; Safdar, N.; Khanna, S. The role of the gut microbiome in colonization resistance and recurrent Clostridioides difficile infection. Ther. Adv. Gastroenterol. 2022, 15, 17562848221134396. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.W.; Lawley, T.D. Therapeutic modulation of intestinal dysbiosis. Pharmacol. Res. 2013, 69, 75–86. [Google Scholar] [CrossRef]
- Nagata, N.; Nishijima, S.; Miyoshi-Akiyama, T.; Kojima, Y.; Kimura, M.; Aoki, R.; Ohsugi, M.; Ueki, K.; Miki, K.; Iwata, E.; et al. Population-level Metagenomics Uncovers Distinct Effects of Multiple Medications on the Human Gut Microbiome. Gastroenterology 2022, 163, 1038–1052. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Chen, Y.; Huang, W.; Zhou, H.; Zhang, W. Drug-microbiota interactions: An emerging priority for precision medicine. Signal Transduct. Target. Ther. 2023, 8, 386. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, L.; Kelly, L. Bringing microbiome-drug interaction research into the clinic. EBioMedicine 2019, 44, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Heinken, A.; Hertel, J.; Acharya, G.; Ravcheev, D.A.; Nyga, M.; Okpala, O.E.; Hogan, M.; Magnusdottir, S.; Martinelli, F.; Nap, B.; et al. Genome-scale metabolic reconstruction of 7,302 human microorganisms for personalized medicine. Nat. Biotechnol. 2023, 41, 1320–1331. [Google Scholar] [CrossRef] [PubMed]
- Bilotta, A.J.; Cong, Y. Gut microbiota metabolite regulation of host defenses at mucosal surfaces: Implication in precision medicine. Precis. Clin. Med. 2019, 2, 110–119. [Google Scholar] [CrossRef]
- Sayers, E.; MacGregor, A.; Carding, S.R. Drug-microbiota interactions and treatment response: Relevance to rheumatoid arthritis. AIMS Microbiol. 2018, 4, 642–654. [Google Scholar] [CrossRef]
- Savage, N. The complex relationship between drugs and the microbiome. Nature 2020, 577, S10–S11. [Google Scholar] [CrossRef] [PubMed]
- Le Bastard, Q.; Al-Ghalith, G.A.; Gregoire, M.; Chapelet, G.; Javaudin, F.; Dailly, E.; Batard, E.; Knights, D.; Montassier, E. Systematic review: Human gut dysbiosis induced by non-antibiotic prescription medications. Aliment. Pharmacol. Ther. 2018, 47, 332–345. [Google Scholar] [CrossRef]
- Fishbein, S.R.S.; Mahmud, B.; Dantas, G. Antibiotic perturbations to the gut microbiome. Nat. Rev. Microbiol. 2023, 21, 772–788. [Google Scholar] [CrossRef]
- Namasivayam, S.; Maiga, M.; Yuan, W.; Thovarai, V.; Costa, D.L.; Mittereder, L.R.; Wipperman, M.F.; Glickman, M.S.; Dzutsev, A.; Trinchieri, G.; et al. Longitudinal profiling reveals a persistent intestinal dysbiosis triggered by conventional anti-tuberculosis therapy. Microbiome 2017, 5, 71. [Google Scholar] [CrossRef]
- Mruk-Mazurkiewicz, H.; Kulaszynska, M.; Jakubczyk, K.; Janda-Milczarek, K.; Czarnecka, W.; Rebacz-Maron, E.; Zacha, S.; Sienko, J.; Zeair, S.; Dalewski, B.; et al. Clinical Relevance of Gut Microbiota Alterations under the Influence of Selected Drugs-Updated Review. Biomedicines 2023, 11, 952. [Google Scholar] [CrossRef] [PubMed]
- Crouwel, F.; Buiter, H.J.C.; de Boer, N.K. Gut microbiota-driven drug metabolism in inflammatory bowel disease. J. Crohns Colitis 2020, 15, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Gulnaz, A.; Chang, J.-E.; Maeng, H.-J.; Shin, K.-H.; Lee, K.-R.; Chae, Y.-J. A mechanism-based understanding of altered drug pharmacokinetics by gut microbiota. J. Pharm. Investig. 2023, 53, 73–92. [Google Scholar] [CrossRef]
- Dingsdag, S.A.; Hunter, N. Metronidazole: An update on metabolism, structure-cytotoxicity and resistance mechanisms. J. Antimicrob. Chemother. 2018, 73, 265–279. [Google Scholar] [CrossRef]
- Li, H.; He, J.; Jia, W. The influence of gut microbiota on drug metabolism and toxicity. Expert. Opin. Drug Metab. Toxicol. 2016, 12, 31–40. [Google Scholar] [CrossRef]
- Quosdorf, S.; Schuetz, A.; Kolodziej, H. Different Inhibitory Potencies of Oseltamivir Carboxylate, Zanamivir, and Several Tannins on Bacterial and Viral Neuraminidases as Assessed in a Cell-Free Fluorescence-Based Enzyme Inhibition Assay. Molecules 2017, 22, 1989. [Google Scholar] [CrossRef]
- Zhang, X.; Fang, Z.; Zhang, C.; Xia, H.; Jie, Z.; Han, X.; Chen, Y.; Ji, L. Effects of Acarbose on the Gut Microbiota of Prediabetic Patients: A Randomized, Double-blind, Controlled Crossover Trial. Diabetes Ther. 2017, 8, 293–307. [Google Scholar] [CrossRef]
- Yang, G.; Ge, S.; Singh, R.; Basu, S.; Shatzer, K.; Zen, M.; Liu, J.; Tu, Y.; Zhang, C.; Wei, J.; et al. Glucuronidation: Driving factors and their impact on glucuronide disposition. Drug Metab. Rev. 2017, 49, 105–138. [Google Scholar] [CrossRef]
- Klaassen, C.D.; Cui, J.Y. Review: Mechanisms of How the Intestinal Microbiota Alters the Effects of Drugs and Bile Acids. Drug Metab. Dispos. 2015, 43, 1505–1521. [Google Scholar] [CrossRef]
- Zhang, L.; Meng, J.; Ban, Y.; Jalodia, R.; Chupikova, I.; Fernandez, I.; Brito, N.; Sharma, U.; Abreu, M.T.; Ramakrishnan, S.; et al. Morphine tolerance is attenuated in germfree mice and reversed by probiotics, implicating the role of gut microbiome. Proc. Natl. Acad. Sci. USA 2019, 116, 13523–13532. [Google Scholar] [CrossRef]
- Fuhrman, B.J.; Feigelson, H.S.; Flores, R.; Gail, M.H.; Xu, X.; Ravel, J.; Goedert, J.J. Associations of the fecal microbiome with urinary estrogens and estrogen metabolites in postmenopausal women. J. Clin. Endocrinol. Metab. 2014, 99, 4632–4640. [Google Scholar] [CrossRef] [PubMed]
- Lazarevic, S.; Danic, M.; Al-Salami, H.; Mooranian, A.; Mikov, M. Gut Microbiota Metabolism of Azathioprine: A New Hallmark for Personalized Drug-Targeted Therapy of Chronic Inflammatory Bowel Disease. Front. Pharmacol. 2022, 13, 879170. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhong, X.; Yan, J.; Sun, C.; Zhao, X.; Wang, X. Potential roles of gut microbes in biotransformation of natural products: An overview. Front. Microbiol. 2022, 13, 956378. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhang, B.; Hu, Y.; Zhao, Y. New Insights Into Gut-Bacteria-Derived Indole and Its Derivatives in Intestinal and Liver Diseases. Front. Pharmacol. 2021, 12, 769501. [Google Scholar] [CrossRef] [PubMed]
- Swanson, H.I. Drug Metabolism by the Host and Gut Microbiota: A Partnership or Rivalry? Drug Metab. Dispos. 2015, 43, 1499–1504. [Google Scholar] [CrossRef] [PubMed]
- Klunemann, M.; Andrejev, S.; Blasche, S.; Mateus, A.; Phapale, P.; Devendran, S.; Vappiani, J.; Simon, B.; Scott, T.A.; Kafkia, E.; et al. Bioaccumulation of therapeutic drugs by human gut bacteria. Nature 2021, 597, 533–538. [Google Scholar] [CrossRef]
- Zimmermann, M.; Zimmermann-Kogadeeva, M.; Wegmann, R.; Goodman, A.L. Mapping human microbiome drug metabolism by gut bacteria and their genes. Nature 2019, 570, 462–467. [Google Scholar] [CrossRef]
- Kamath, S.; Stringer, A.M.; Prestidge, C.A.; Joyce, P. Targeting the gut microbiome to control drug pharmacomicrobiomics: The next frontier in oral drug delivery. Expert. Opin. Drug Deliv. 2023, 20, 1315–1331. [Google Scholar] [CrossRef]
- Zhao, W.; Hong, H.; Yin, J.; Wu, B.; Zhao, F.; Zhang, X.X. Recovery of gut microbiota in mice exposed to tetracycline hydrochloride and their correlation with host metabolism. Ecotoxicology 2021, 30, 1620–1631. [Google Scholar] [CrossRef]
- Wan, Y.; Zuo, T. Interplays between drugs and the gut microbiome. Gastroenterol. Rep. 2022, 10, goac009. [Google Scholar] [CrossRef]
- Zhao, L.Y.; Mei, J.X.; Yu, G.; Lei, L.; Zhang, W.H.; Liu, K.; Chen, X.L.; Kolat, D.; Yang, K.; Hu, J.K. Role of the gut microbiota in anticancer therapy: From molecular mechanisms to clinical applications. Signal Transduct. Target. Ther. 2023, 8, 201. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Lau, R.I.; Liu, Q.; Su, Q.; Chan, F.K.L.; Ng, S.C. Gut microbiota in COVID-19: Key microbial changes, potential mechanisms and clinical applications. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 323–337. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, J.; Wang, R. Gut microbiota modulates drug pharmacokinetics. Drug Metab. Rev. 2018, 50, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Haiser, H.J.; Gootenberg, D.B.; Chatman, K.; Sirasani, G.; Balskus, E.P.; Turnbaugh, P.J. Predicting and manipulating cardiac drug inactivation by the human gut bacterium Eggerthella lenta. Science 2013, 341, 295–298. [Google Scholar] [CrossRef] [PubMed]
- Cui, C.; Qu, Y.; Sia, J.E.V.; Zhu, Z.; Wang, Y.; Ling, J.; Li, H.; Jiang, Y.; Pan, J.; Liu, D. Assessment of Aging-Related Function Variations of P-gp Transporter in Old-Elderly Chinese CHF Patients Based on Modeling and Simulation. Clin. Pharmacokinet. 2022, 61, 1789–1800. [Google Scholar] [CrossRef] [PubMed]
- Foley, S.E.; Tuohy, C.; Dunford, M.; Grey, M.J.; De Luca, H.; Cawley, C.; Szabady, R.L.; Maldonado-Contreras, A.; Houghton, J.M.; Ward, D.V.; et al. Gut microbiota regulation of P-glycoprotein in the intestinal epithelium in maintenance of homeostasis. Microbiome 2021, 9, 183. [Google Scholar] [CrossRef] [PubMed]
- Feng, W.; Liu, J.; Ao, H.; Yue, S.; Peng, C. Targeting gut microbiota for precision medicine: Focusing on the efficacy and toxicity of drugs. Theranostics 2020, 10, 11278–11301. [Google Scholar] [CrossRef]
- Lilja, E.E.; Johnson, D.R. Metabolite toxicity determines the pace of molecular evolution within microbial populations. BMC Evol. Biol. 2017, 17, 52. [Google Scholar] [CrossRef]
- Dehhaghi, M.; Kazemi Shariat Panahi, H.; Heng, B.; Guillemin, G.J. The Gut Microbiota, Kynurenine Pathway, and Immune System Interaction in the Development of Brain Cancer. Front. Cell Dev. Biol. 2020, 8, 562812. [Google Scholar] [CrossRef]
- Lazar, V.; Ditu, L.M.; Pircalabioru, G.G.; Gheorghe, I.; Curutiu, C.; Holban, A.M.; Picu, A.; Petcu, L.; Chifiriuc, M.C. Aspects of Gut Microbiota and Immune System Interactions in Infectious Diseases, Immunopathology, and Cancer. Front. Immunol. 2018, 9, 1830. [Google Scholar] [CrossRef]
- Lu, Y.; Yuan, X.; Wang, M.; He, Z.; Li, H.; Wang, J.; Li, Q. Gut microbiota influence immunotherapy responses: Mechanisms and therapeutic strategies. J. Hematol. Oncol. 2022, 15, 47. [Google Scholar] [CrossRef] [PubMed]
- Ciabattini, A.; Olivieri, R.; Lazzeri, E.; Medaglini, D. Role of the Microbiota in the Modulation of Vaccine Immune Responses. Front. Microbiol. 2019, 10, 1305. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Wu, X.; Mou, M.; Wang, C.; Wang, L.; Li, F.; Guo, M.; Yin, J.; Xie, W.; Wang, X.; et al. GIMICA: Host genetic and immune factors shaping human microbiota. Nucleic Acids Res. 2021, 49, D715–D722. [Google Scholar] [CrossRef]
- Hou, X.; Zheng, Z.; Wei, J.; Zhao, L. Effects of gut microbiota on immune responses and immunotherapy in colorectal cancer. Front. Immunol. 2022, 13, 1030745. [Google Scholar] [CrossRef]
- Jardou, M.; Provost, Q.; Brossier, C.; Pinault, E.; Sauvage, F.L.; Lawson, R. Alteration of the gut microbiome in mycophenolate-induced enteropathy: Impacts on the profile of short-chain fatty acids in a mouse model. BMC Pharmacol. Toxicol. 2021, 22, 66. [Google Scholar] [CrossRef]
- Manes, A.; Di Renzo, T.; Dodani, L.; Reale, A.; Gautiero, C.; Di Lauro, M.; Nasti, G.; Manco, F.; Muscariello, E.; Guida, B.; et al. Pharmacomicrobiomics of Classical Immunosuppressant Drugs: A Systematic Review. Biomedicines 2023, 11, 2562. [Google Scholar] [CrossRef]
- Saqr, A.; Carlson, B.; Staley, C.; Rashidi, A.; Al-Kofahi, M.; Kaiser, T.; Holtan, S.; MacMillan, M.; Young, J.A.; Jurdi, N.E.; et al. Reduced Enterohepatic Recirculation of Mycophenolate and Lower Blood Concentrations Are Associated with the Stool Bacterial Microbiome after Hematopoietic Cell Transplantation. Transpl. Cell. Ther. 2022, 28, 372.e1–372.e9. [Google Scholar] [CrossRef]
- Gabarre, P.; Loens, C.; Tamzali, Y.; Barrou, B.; Jaisser, F.; Tourret, J. Immunosuppressive therapy after solid organ transplantation and the gut microbiota: Bidirectional interactions with clinical consequences. Am. J. Transpl. 2022, 22, 1014–1030. [Google Scholar] [CrossRef]
- Muratore, E.; Leardini, D.; Baccelli, F.; Venturelli, F.; Prete, A.; Masetti, R. Nutritional modulation of the gut microbiome in allogeneic hematopoietic stem cell transplantation recipients. Front. Nutr. 2022, 9, 993668. [Google Scholar] [CrossRef]
- Xu, H.M.; Huang, H.L.; Zhou, Y.L.; Zhao, H.L.; Xu, J.; Shou, D.W.; Liu, Y.D.; Zhou, Y.J.; Nie, Y.Q. Fecal Microbiota Transplantation: A New Therapeutic Attempt from the Gut to the Brain. Gastroenterol. Res. Pr. 2021, 2021, 6699268. [Google Scholar] [CrossRef]
- Lynn, D.J.; Benson, S.C.; Lynn, M.A.; Pulendran, B. Modulation of immune responses to vaccination by the microbiota: Implications and potential mechanisms. Nat. Rev. Immunol. 2022, 22, 33–46. [Google Scholar] [CrossRef]
- Huang, B.; Wang, J.; Li, L. Recent five-year progress in the impact of gut microbiota on vaccination and possible mechanisms. Gut Pathog. 2023, 15, 27. [Google Scholar] [CrossRef]
- Lamers, M.M.; Beumer, J.; van der Vaart, J.; Knoops, K.; Puschhof, J.; Breugem, T.I.; Ravelli, R.B.G.; Paul van Schayck, J.; Mykytyn, A.Z.; Duimel, H.Q.; et al. SARS-CoV-2 productively infects human gut enterocytes. Science 2020, 369, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, Y.K.; Zuo, T.; Lui, G.C.; Zhang, F.; Liu, Q.; Li, A.Y.; Chung, A.C.; Cheung, C.P.; Tso, E.Y.; Fung, K.S.; et al. Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. Gut 2021, 70, 698–706. [Google Scholar] [CrossRef]
- Dhar, D.; Mohanty, A. Gut microbiota and COVID-19—Possible link and implications. Virus Res. 2020, 285, 198018. [Google Scholar] [CrossRef] [PubMed]
- Bernard-Raichon, L.; Venzon, M.; Klein, J.; Axelrad, J.E.; Zhang, C.; Sullivan, A.P.; Hussey, G.A.; Casanovas-Massana, A.; Noval, M.G.; Valero-Jimenez, A.M.; et al. Gut microbiome dysbiosis in antibiotic-treated COVID-19 patients is associated with microbial translocation and bacteremia. Nat. Commun. 2022, 13, 5926. [Google Scholar] [CrossRef] [PubMed]
- Farsi, Y.; Tahvildari, A.; Arbabi, M.; Vazife, F.; Sechi, L.A.; Shahidi Bonjar, A.H.; Jamshidi, P.; Nasiri, M.J.; Mirsaeidi, M. Diagnostic, Prognostic, and Therapeutic Roles of Gut Microbiota in COVID-19: A Comprehensive Systematic Review. Front. Cell. Infect. Microbiol. 2022, 12, 804644. [Google Scholar] [CrossRef]
- Torjesen, I. Covid-19: Norway investigates 23 deaths in frail elderly patients after vaccination. BMJ 2021, 372, n149. [Google Scholar] [CrossRef]
- Ng, S.C.; Peng, Y.; Zhang, L.; Mok, C.K.; Zhao, S.; Li, A.; Ching, J.Y.; Liu, Y.; Yan, S.; Chan, D.L.S.; et al. Gut microbiota composition is associated with SARS-CoV-2 vaccine immunogenicity and adverse events. Gut 2022, 71, 1106–1116. [Google Scholar] [CrossRef]
- Patel, P.; Roper, J. Gut Microbiome Composition Is Associated with COVID-19 Disease Severity. Gastroenterology 2021, 161, 722–724. [Google Scholar] [CrossRef]
- Wissel, E.F.; Smith, L.K. Inter-individual variation shapes the human microbiome. Behav. Brain Sci. 2019, 42. [Google Scholar] [CrossRef]
- Gerard, C.; Vidal, H. Impact of Gut Microbiota on Host Glycemic Control. Front. Endocrinol. 2019, 10, 29. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Chen, Y.; Tang, G.; Li, Z.; Yang, X.; Shang, X.; Huang, T.; Huang, G.; Wang, L.; Han, Y.; et al. Gut microbiota composition reflects disease progression, severity and outcome, and dysfunctional immune responses in patients with hypertensive intracerebral hemorrhage. Front. Immunol. 2022, 13, 869846. [Google Scholar] [CrossRef] [PubMed]
- Musso, G.; Gambino, R.; Cassader, M. Interactions between gut microbiota and host metabolism predisposing to obesity and diabetes. Annu. Rev. Med. 2011, 62, 361–380. [Google Scholar] [CrossRef] [PubMed]
- Healey, G.R.; Murphy, R.; Brough, L.; Butts, C.A.; Coad, J. Interindividual variability in gut microbiota and host response to dietary interventions. Nutr. Rev. 2017, 75, 1059–1080. [Google Scholar] [CrossRef] [PubMed]
- Ting, N.L.; Lau, H.C.; Yu, J. Cancer pharmacomicrobiomics: Targeting microbiota to optimise cancer therapy outcomes. Gut 2022, 71, 1412–1425. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Jiang, T.; He, D. Advances in the implications of the gut microbiota on the treatment efficacy of disease-modifying anti-rheumatic drugs in rheumatoid arthritis. Front. Immunol. 2023, 14, 1189036. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.I.; Tsay, F.W.; Graham, D.Y.; Tsai, T.J.; Tsai, K.W.; Kao, J.Y.; Peng, N.J.; Kuo, C.H.; Kao, S.S.; Wang, H.M.; et al. Equivalent Efficacies of Reverse Hybrid and Bismuth Quadruple Therapies in Eradication of Helicobacter pylori Infection in a Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2018, 16, 1427–1433. [Google Scholar] [CrossRef]
- Wimmers, F.; Donato, M.; Kuo, A.; Ashuach, T.; Gupta, S.; Li, C.; Dvorak, M.; Foecke, M.H.; Chang, S.E.; Hagan, T.; et al. The single-cell epigenomic and transcriptional landscape of immunity to influenza vaccination. Cell 2021, 184, 3915–3935.e3921. [Google Scholar] [CrossRef]
- Amdur, R.L.; Paul, R.; Barrows, E.D.; Kincaid, D.; Muralidharan, J.; Nobakht, E.; Centron-Vinales, P.; Siddiqi, M.; Patel, S.S.; Raj, D.S. The potassium regulator patiromer affects serum and stool electrolytes in patients receiving hemodialysis. Kidney Int. 2020, 98, 1331–1340. [Google Scholar] [CrossRef]
- Ali, A.H.; Damman, J.; Shah, S.B.; Davies, Y.; Hurwitz, M.; Stephen, M.; Lemos, L.M.; Carey, E.J.; Lindor, K.D.; Buness, C.W.; et al. Open-label prospective therapeutic clinical trials: Oral vancomycin in children and adults with primary sclerosing cholangitis. Scand. J. Gastroenterol. 2020, 55, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Aroniadis, O.C.; Brandt, L.J.; Oneto, C.; Feuerstadt, P.; Sherman, A.; Wolkoff, A.W.; Kassam, Z.; Sadovsky, R.G.; Elliott, R.J.; Budree, S.; et al. Faecal microbiota transplantation for diarrhoea-predominant irritable bowel syndrome: A double-blind, randomised, placebo-controlled trial. Lancet Gastroenterol. Hepatol. 2019, 4, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Raj, D.S.; Sohn, M.B.; Charytan, D.M.; Himmelfarb, J.; Ikizler, T.A.; Mehrotra, R.; Ramezani, A.; Regunathan-Shenk, R.; Hsu, J.Y.; Landis, J.R.; et al. The Microbiome and p-Inulin in Hemodialysis: A Feasibility Study. Kidney360 2021, 2, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Lu, Y.; Tian, Q.Y.; Zhang, Y.; Guo, F.J.; Liu, G.Y.; Syed, N.M.; Lai, Y.; Lin, E.A.; Kong, L.; et al. The growth factor progranulin binds to TNF receptors and is therapeutic against inflammatory arthritis in mice. Science 2011, 332, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Scher, J.U.; Sczesnak, A.; Longman, R.S.; Segata, N.; Ubeda, C.; Bielski, C.; Rostron, T.; Cerundolo, V.; Pamer, E.G.; Abramson, S.B.; et al. Expansion of intestinal Prevotella copri correlates with enhanced susceptibility to arthritis. Elife 2013, 2, e01202. [Google Scholar] [CrossRef] [PubMed]
- Kwak, S.; Choi, J.; Hink, T.; Reske, K.A.; Blount, K.; Jones, C.; Bost, M.H.; Sun, X.; Burnham, C.D.; Dubberke, E.R.; et al. Impact of investigational microbiota therapeutic RBX2660 on the gut microbiome and resistome revealed by a placebo-controlled clinical trial. Microbiome 2020, 8, 125. [Google Scholar] [CrossRef] [PubMed]
- Dubberke, E.R.; Lee, C.H.; Orenstein, R.; Khanna, S.; Hecht, G.; Gerding, D.N. Results From a Randomized, Placebo-Controlled Clinical Trial of a RBX2660-A Microbiota-Based Drug for the Prevention of Recurrent Clostridium difficile Infection. Clin. Infect. Dis. 2018, 67, 1198–1204. [Google Scholar] [CrossRef]
- Meyer-Myklestad, M.H.; Medhus, A.W.; Stiksrud, B.; Lorvik, K.B.; Seljeflot, I.; Hansen, S.H.; Holm, K.; Hov, J.R.; Kvale, D.; Dyrhol-Riise, A.M.; et al. Probiotics to HIV-Infected Immunological Nonresponders: Altered Mucosal Immunity and Microbial Diversity Restricted to Ileum. J. Acquir. Immune Defic. Syndr. 2022, 89, 77–86. [Google Scholar] [CrossRef]
- Orenstein, R.; Dubberke, E.R.; Khanna, S.; Lee, C.H.; Yoho, D.; Johnson, S.; Hecht, G.; DuPont, H.L.; Gerding, D.N.; Blount, K.F.; et al. Durable reduction of Clostridioides difficile infection recurrence and microbiome restoration after treatment with RBX2660: Results from an open-label phase 2 clinical trial. BMC Infect. Dis. 2022, 22, 245. [Google Scholar] [CrossRef]
- Li, Z.; Henning, S.M.; Lee, R.P.; Lu, Q.Y.; Summanen, P.H.; Thames, G.; Corbett, K.; Downes, J.; Tseng, C.H.; Finegold, S.M.; et al. Pomegranate extract induces ellagitannin metabolite formation and changes stool microbiota in healthy volunteers. Food Funct. 2015, 6, 2487–2495. [Google Scholar] [CrossRef]
- Ding, L.; He, C.; Li, X.; Huang, X.; Lei, Y.; Ke, H.; Chen, H.; Yang, Q.; Cai, Y.; Liao, Y.; et al. Efficacy and Safety of Faecal Microbiota Transplantation for Acute Pancreatitis: A Randomised, Controlled Study. Front. Med. 2021, 8, 772454. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.K.; Seo, J.; Pravodelov, V.; Frazier, S.; Guy, M.; Concilio, K.; Lau-Ng, R.; Brandeis, G.; Watson, J.; van der Velde, J.; et al. Pilot study of autologous fecal microbiota transplants in nursing home residents: Feasibility and safety. Contemp. Clin. Trials Commun. 2022, 27, 100906. [Google Scholar] [CrossRef] [PubMed]
- Lemos, L.N.; Fulthorpe, R.R.; Triplett, E.W.; Roesch, L.F. Rethinking microbial diversity analysis in the high throughput sequencing era. J. Microbiol. Methods 2011, 86, 42–51. [Google Scholar] [CrossRef]
- Drekonja, D.M.; Shaukat, A.; Zhang, J.H.; Reinink, A.R.; Nugent, S.; Dominitz, J.A.; Davis-Karim, A.; Gerding, D.N.; Kyriakides, T.C. Microbiota or placebo after antimicrobial therapy for recurrent Clostridioides difficile at home: A clinical trial with novel home-based enrollment. Clin. Trials 2021, 18, 622–629. [Google Scholar] [CrossRef]
- Scorletti, E.; Afolabi, P.R.; Miles, E.A.; Smith, D.E.; Almehmadi, A.; Alshathry, A.; Moyses, H.E.; Clough, G.F.; Wright, M.; Patel, J.; et al. Design and rationale of the INSYTE study: A randomised, placebo controlled study to test the efficacy of a synbiotic on liver fat, disease biomarkers and intestinal microbiota in non-alcoholic fatty liver disease. Contemp. Clin. Trials 2018, 71, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Scorletti, E.; Afolabi, P.R.; Miles, E.A.; Smith, D.E.; Almehmadi, A.; Alshathry, A.; Childs, C.E.; Del Fabbro, S.; Bilson, J.; Moyses, H.E.; et al. Synbiotics Alter Fecal Microbiomes, But Not Liver Fat or Fibrosis, in a Randomized Trial of Patients with Nonalcoholic Fatty Liver Disease. Gastroenterology 2020, 158, 1597–1610.e1597. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, J.; Wu, C. Modulation of Gut Microbiota and Immune System by Probiotics, Pre-biotics, and Post-biotics. Front. Nutr. 2021, 8, 634897. [Google Scholar] [CrossRef]
- Hernandez-Calderon, P.; Wiedemann, L.; Benitez-Paez, A. The microbiota composition drives personalized nutrition: Gut microbes as predictive biomarkers for the success of weight loss diets. Front. Nutr. 2022, 9, 1006747. [Google Scholar] [CrossRef]
- Hughes, R.L. A Review of the Role of the Gut Microbiome in Personalized Sports Nutrition. Front. Nutr. 2019, 6, 191. [Google Scholar] [CrossRef]
- Wang, Z.; Li, L.; Wang, S.; Wei, J.; Qu, L.; Pan, L.; Xu, K. The role of the gut microbiota and probiotics associated with microbial metabolisms in cancer prevention and therapy. Front. Pharmacol. 2022, 13, 1025860. [Google Scholar] [CrossRef]
- Zhang, X.F.; Guan, X.X.; Tang, Y.J.; Sun, J.F.; Wang, X.K.; Wang, W.D.; Fan, J.M. Clinical effects and gut microbiota changes of using probiotics, prebiotics or synbiotics in inflammatory bowel disease: A systematic review and meta-analysis. Eur. J. Nutr. 2021, 60, 2855–2875. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Verde, L.; Auriemma, R.S.; Vetrani, C.; Cataldi, M.; Frias-Toral, E.; Pugliese, G.; Camajani, E.; Savastano, S.; Colao, A.; et al. Probiotics and Prebiotics: Any Role in Menopause-Related Diseases? Curr. Nutr. Rep. 2023, 12, 83–97. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Qin, S.; Hu, S.; Liu, Z.; Song, Y.; Li, L. Restoration of cefixime-induced gut microbiota changes by a prebiotic blend in a mouse model. Appl. Microbiol. Biotechnol. 2022, 106, 5197–5209. [Google Scholar] [CrossRef] [PubMed]
- Afifirad, R.; Darb Emamie, A.; Golmoradi Zadeh, R.; Asadollahi, P.; Ghanavati, R.; Darbandi, A. Effects of Pro/Prebiotics Alone over Pro/Prebiotics Combined with Conventional Antibiotic Therapy to Treat Bacterial Vaginosis: A Systematic Review. Int. J. Clin. Pract. 2022, 2022, 4774783. [Google Scholar] [CrossRef] [PubMed]
- Williams, N.T. Probiotics. Am. J. Health Syst. Pharm. 2010, 67, 449–458. [Google Scholar] [CrossRef]
- Karpa, K.D. Probiotics for Clostridium difficile diarrhea: Putting it into perspective. Ann. Pharmacother. 2007, 41, 1284–1287. [Google Scholar] [CrossRef]
- Doestzada, M.; Vila, A.V.; Zhernakova, A.; Koonen, D.P.Y.; Weersma, R.K.; Touw, D.J.; Kuipers, F.; Wijmenga, C.; Fu, J. Pharmacomicrobiomics: A novel route towards personalized medicine? Protein Cell 2018, 9, 432–445. [Google Scholar] [CrossRef]
- Aziz, R.K.; Saad, R.; Rizkallah, M.R. PharmacoMicrobiomics or how bugs modulate drugs: An educational initiative to explore the effects of human microbiome on drugs. BMC Bioinform. 2011, 12, A10. [Google Scholar] [CrossRef]
- Zeng, X.; Yang, X.; Fan, J.; Tan, Y.; Ju, L.; Shen, W.; Wang, Y.; Wang, X.; Chen, W.; Ju, D.; et al. MASI: Microbiota-active substance interactions database. Nucleic Acids Res. 2021, 49, D776–D782. [Google Scholar] [CrossRef]
- Javdan, B.; Lopez, J.G.; Chankhamjon, P.; Lee, Y.J.; Hull, R.; Wu, Q.; Wang, X.; Chatterjee, S.; Donia, M.S. Personalized Mapping of Drug Metabolism by the Human Gut Microbiome. Cell 2020, 181, 1661–1679.e1622. [Google Scholar] [CrossRef]
- Petrosino, J.F. The microbiome in precision medicine: The way forward. Genome Med. 2018, 10, 12. [Google Scholar] [CrossRef]
- Chen, D.; Wu, J.; Jin, D.; Wang, B.; Cao, H. Fecal microbiota transplantation in cancer management: Current status and perspectives. Int. J. Cancer 2019, 145, 2021–2031. [Google Scholar] [CrossRef]
- Khoruts, A.; Sadowsky, M.J. Understanding the mechanisms of faecal microbiota transplantation. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 508–516. [Google Scholar] [CrossRef]
- Haiser, H.J.; Turnbaugh, P.J. Is it time for a metagenomic basis of therapeutics? Science 2012, 336, 1253–1255. [Google Scholar] [CrossRef] [PubMed]
- Koppel, N.; Maini Rekdal, V.; Balskus, E.P. Chemical transformation of xenobiotics by the human gut microbiota. Science 2017, 356, eaag2770. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.K.; Holmes, E.; Kinross, J.; Burcelin, R.; Gibson, G.; Jia, W.; Pettersson, S. Host-gut microbiota metabolic interactions. Science 2012, 336, 1262–1267. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Han, Y.; Huang, W.; Jin, M.; Gao, Z. The influence of the gut microbiota on the bioavailability of oral drugs. Acta Pharm. Sin. B 2021, 11, 1789–1812. [Google Scholar] [CrossRef] [PubMed]
- Najjar, A.; Najjar, A.; Karaman, R. Newly Developed Prodrugs and Prodrugs in Development; an Insight of the Recent Years. Molecules 2020, 25, 884. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Guan, J.; Wan, J.; Li, Z. Disulfide based prodrugs for cancer therapy. RSC Adv. 2020, 10, 24397–24409. [Google Scholar] [CrossRef] [PubMed]
- Rautio, J.; Meanwell, N.A.; Di, L.; Hageman, M.J. The expanding role of prodrugs in contemporary drug design and development. Nat. Rev. Drug Discov. 2018, 17, 559–587. [Google Scholar] [CrossRef]
- Fouts, J.R.; Kamm, J.J.; Brodie, B.B. Enzymatic reduction of prontosil and other azo dyes. J. Pharmacol. Exp. Ther. 1957, 120, 291–300. [Google Scholar]
- Gingell, R.; Bridges, J.W.; Williams, R.T. The role of the gut flora in the metabolism of prontosil and neoprontosil in the rat. Xenobiotica 1971, 1, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Hayllar, J.; Bjarnason, I. Sulphasalazine in ulcerative colitis: In memoriam? Gut 1991, 32, 462–463. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.P.; Pope, D.J.; Gilbert, A.P.; Sacra, P.J.; Baron, J.H.; Lennard-Jones, J.E. Studies of two novel sulfasalazine analogs, ipsalazide and balsalazide. Dig. Dis. Sci. 1983, 28, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Wadworth, A.N.; Fitton, A. Olsalazine. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic potential in inflammatory bowel disease. Drugs 1991, 41, 647–664. [Google Scholar] [CrossRef] [PubMed]
- Matthies, A.; Clavel, T.; Gutschow, M.; Engst, W.; Haller, D.; Blaut, M.; Braune, A. Conversion of daidzein and genistein by an anaerobic bacterium newly isolated from the mouse intestine. Appl. Env. Microbiol. 2008, 74, 4847–4852. [Google Scholar] [CrossRef]
- Feng, R.; Shou, J.W.; Zhao, Z.X.; He, C.Y.; Ma, C.; Huang, M.; Fu, J.; Tan, X.S.; Li, X.Y.; Wen, B.Y.; et al. Transforming berberine into its intestine-absorbable form by the gut microbiota. Sci. Rep. 2015, 5, 12155. [Google Scholar] [CrossRef]
- Shu, Y.Z.; Kingston, D.G.; Van Tassell, R.L.; Wilkins, T.D. Metabolism of levamisole, an anti-colon cancer drug, by human intestinal bacteria. Xenobiotica 1991, 21, 737–750. [Google Scholar] [CrossRef]
- Harris, B.E.; Manning, B.W.; Federle, T.W.; Diasio, R.B. Conversion of 5-fluorocytosine to 5-fluorouracil by human intestinal microflora. Antimicrob. Agents Chemother. 1986, 29, 44–48. [Google Scholar] [CrossRef]
- Basit, A.W.; Newton, J.M.; Lacey, L.F. Susceptibility of the H2-receptor antagonists cimetidine, famotidine and nizatidine, to metabolism by the gastrointestinal microflora. Int. J. Pharm. 2002, 237, 23–33. [Google Scholar] [CrossRef]
- Carmody, R.N.; Turnbaugh, P.J. Host-microbial interactions in the metabolism of therapeutic and diet-derived xenobiotics. J. Clin. Investig. 2014, 124, 4173–4181. [Google Scholar] [CrossRef] [PubMed]
- Sousa, T.; Paterson, R.; Moore, V.; Carlsson, A.; Abrahamsson, B.; Basit, A.W. The gastrointestinal microbiota as a site for the biotransformation of drugs. Int. J. Pharm. 2008, 363, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Hyun, S.H.; Shim, S.B.; Kobashi, K. The role of intestinal bacteria in the transformation of sodium picosulfate. Jpn. J. Pharmacol. 1992, 59, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Trinh, H.T.; Joh, E.H.; Kwak, H.Y.; Baek, N.I.; Kim, D.H. Anti-pruritic effect of baicalin and its metabolites, baicalein and oroxylin A, in mice. Acta Pharmacol. Sin. 2010, 31, 718–724. [Google Scholar] [CrossRef]
- Takakura, A.; Kurita, A.; Asahara, T.; Yokoba, M.; Yamamoto, M.; Ryuge, S.; Igawa, S.; Yasuzawa, Y.; Sasaki, J.; Kobayashi, H.; et al. Rapid deconjugation of SN-38 glucuronide and adsorption of released free SN-38 by intestinal microorganisms in rat. Oncol. Lett. 2012, 3, 520–524. [Google Scholar] [CrossRef] [PubMed]
- Vanderhoof, J. Early changes in the human Microbiome alter immune function and immunologically mediated disorders. J. Anim. Sci. 2017, 95, 69. [Google Scholar] [CrossRef]
- Yadav, M.; Chauhan, N.S. Microbiome therapeutics: Exploring the present scenario and challenges. Gastroenterol. Rep. 2022, 10, goab046. [Google Scholar] [CrossRef]
- De Vos, W.M.; de Vos, E.A. Role of the intestinal microbiome in health and disease: From correlation to causation. Nutr. Rev. 2012, 70 (Suppl. S1), S45–S56. [Google Scholar] [CrossRef]
- Al-Bakri, A.G.; Akour, A.A.; Al-Delaimy, W.K. Knowledge, attitudes, ethical and social perspectives towards fecal microbiota transplantation (FMT) among Jordanian healthcare providers. BMC Med. Ethics 2021, 22, 19. [Google Scholar] [CrossRef]
- Rhodes, R. Ethical issues in microbiome research and medicine. BMC Med. 2016, 14, 156. [Google Scholar] [CrossRef]
- Shi, D.; Turroni, S.; Gong, L.; Wu, W.; Yim, H.C.H. Editorial: Manipulation of gut microbiota as a key target to intervene on the onset and progression of digestive system diseases. Front. Med. 2022, 9, 999005. [Google Scholar] [CrossRef]
- Mishima, Y.; Sartor, R.B. Manipulating resident microbiota to enhance regulatory immune function to treat inflammatory bowel diseases. J. Gastroenterol. 2020, 55, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Vargason, A.M.; Anselmo, A.C. Clinical translation of microbe-based therapies: Current clinical landscape and preclinical outlook. Bioeng. Transl. Med. 2018, 3, 124–137. [Google Scholar] [CrossRef] [PubMed]
- Narayana, J.K.; Mac Aogain, M.; Goh, W.W.B.; Xia, K.; Tsaneva-Atanasova, K.; Chotirmall, S.H. Mathematical-based microbiome analytics for clinical translation. Comput. Struct. Biotechnol. J. 2021, 19, 6272–6281. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| MDI Categories | Trial Number | Conditions | Interventions | Descriptions of the Microbiota Involvement |
|---|---|---|---|---|
| Drugs/substances alter gut microbiota composition | NCT02086110 | Autism | Synbiotic | Prebiotic and synbiotic treatments altered the stool microbiota composition of children with autism, increasing Bifidobacterium and reducing Prevotella enterotype. |
| NCT02547038 | Helicobacter pylori Infection | Pantoprazole+bismuth+tetra+metro | Reverse hybrid therapy achieved a higher eradication rate of Helicobacter pylori than bismuth quadruple therapy, with fewer adverse events and better compliance [78]. | |
| NCT03018925 | Ulcerative Colitis (UC) | Golimumab | Golimumab induced shifts in the abundance of bacterial markers in patients with UC, increasing Akkermansia municiphila and Faecalibacterium prausnitzii and decreasing Escherichia coli. | |
| NCT02330653 | Inflammatory Bowel Diseases (IBD), Crohn Disease (CD), UC | Fecal Microbiota Transplant (FMT) | Universal donor FMT was safe and well-tolerated for pediatric patients with active UC or CD, and resulted in a significant improvement in stool microbiota composition and diversity. | |
| NCT02154061 | Influenza | IIV flu vaccine, Metronidazole, Neomycin | IIV flu vaccine induced similar immune responses in both groups, but antibiotic treatment prior to vaccination significantly altered the gut microbiome composition and diversity, reducing Bacteroidetes and increasing Firmicutes [79]. | |
| NCT02765256 | CD | Fluconazole, Vancomycin, Neomycin, Ciprofloxacin, Prilosec, FMT | The intervention of bowel lavage and antibiotics with or without fluconazole was effective in reducing CD activity and modifying the gut microbiota. | |
| NCT03326583 | Hyperkalemia, End Stage Renal Disease (ESRD) | Patiromer | Patiromer reduced serum potassium levels in ESRD patients with hyperkalemia, and altered gut microbiome composition, increasing Bacteroides and decreasing Prevotella [80]. | |
| NCT01322386 | Primary Sclerosing Cholangitis, Biliary Atresia | Vancomycin | Vancomycin therapy improved the liver function tests of some patients with biliary atresia or primary sclerosing cholangitis and altered the composition and diversity of their gut microbiota [81]. | |
| NCT02328547 | Irritable Bowel Syndrome (IBS) | FMT | FMT using oral capsules was safe, feasible, and tolerable for patients with diarrhea-predominant IBS, and resulted in improvement of IBS symptoms and quality of life, as well as changes in the intestinal microbiome composition and diversity of the patients [82]. | |
| NCT02572882 | End-Stage Renal Disease, Gut Microbiome Dysbiosis | Dietary Supplement: P-inulin | P-Inulin improved gut microbiome diversity and reduced inflammation in hemodialysis patients with hyperkalemia, and had no serious adverse effects [83]. | |
| NCT01198509 | Rheumatoid Arthritis, Psoriatic Arthritis, Periodontal Disease | Doxycycline, Vancomycin | Doxycycline and vancomycin had different effects on the oral and intestinal microbiota of rheumatoid arthritis patients, and that changes in the microbiota were associated with changes in disease activity and inflammatory markers [84,85]. | |
| NCT03476317 | CD | Vancomycin, Neomycin, Ciprofloxacin, FMT | The intervention of bowel lavage and antibiotics with or without fluconazole was effective in reducing CD activity and modifying the gut microbiota. | |
| NCT01619176 | Rheumatoid Arthritis | Methotrexate, NSAID, Leflunomide Biological: Etanercept injection | Acupuncture plus conventional treatment improved the clinical symptoms and inflammatory markers of rheumatoid arthritis patients, and altered the gut microbiota composition and diversity. | |
| NCT02299570 | Recurrent Clostridium difficile infection | Biological: RBX2660 | RBX2660 was superior to placebo in achieving treatment success, defined as the absence of recurrent CDI or death within 8 weeks of treatment [86,87]. | |
| NCT02646332 | Helicobacter pylori Infection | Dexlan+amox+clar+metr, Dexlan+clarith+amox+metro | Concomitant therapy was non-inferior to reverse hybrid therapy in achieving Helicobacter pylori eradication. Both therapies had similar adverse event rates and patient compliance. | |
| NCT03181828 | Urea Cycle Disorder | Acetohydroxamic acid oral tablet | Acetohydroxamic acid reduced the hydrolysis of urea by gut bacteria and increased the excretion of 13C-urea in healthy subjects and subjects with urea cycle disorders. | |
| NCT01839734 | HIV Infection | Lubiprostone | Lubiprostone did not affect gut microbiota composition or function in HIV-infected patients with incomplete CD4+ T-cell recovery on antiretroviral therapy. | |
| NCT01355575 | Non-Alcoholic Fatty Liver Disease (NAFLD) | Rifaximin | Rifaximin altered the gut microbiome composition, reduced hepatic lipid content and improved insulin sensitivity in patients with NAFLD. | |
| Gut microbiota influences drug metabolism/disease treatment | NCT02640625 | Human Immunodeficiency Virus | Probiotic compound | Probiotics were safe and well-tolerated for cART-treated INR patients with chronic HIV infection, and had a modest effect on reducing blood CD4 count and increasing blood HIV viral load [88]. |
| NCT02711800 | Anxiety, Abdominal Pain | Lactobacillus rhamnosus | Probiotics reduced anxiety symptoms and abdominal pain in children with IBS, and had no serious adverse effects. | |
| NCT02589847 | Clostridium difficile Infection (CDI) | Biological: RBX2660 | Fecal microbiota transplantation with RBX2660 was safe and effective in preventing recurrent Clostridium difficile infection in patients with a history of CDI [89]. | |
| NCT02108821 | IBD, CD, UC | FMT | FMT was safe and well-tolerated, and resulted in a significant decrease in fecal calprotectin and a trend towards improvement in disease activity in pediatric patients with IBD. | |
| NCT02370641 | Urolith | Dietary Supplement: PomX | Pomegranate extract consumption resulted in three distinct groups of urolith producers, which were associated with different gut microbiota profiles [90]. | |
| NCT02318134 | Acute Pancreatitis, Intestinal Bacteria Flora Disturbance, Intestinal Dysfunction | FMT, Normal saline | FMT improved the intestinal barrier function and reduced the systemic inflammatory response of patients with severe acute pancreatitis, and also changed the intestinal microbiome composition and diversity of the patients [91]. | |
| NCT04322500 | Chalazion | Probiotics | Probiotics improved chalaziosis resolution time and reduced recurrence rate in children compared to conservative treatment. | |
| NCT03061097 | Antibiotic resistance | Autologous FMT | FMT was safe and feasible, and significantly reduced the prevalence and abundance of antibiotic resistant bacteria in the fecal microbiota of patients who had an infectious episode requiring antibiotics [92]. | |
| NCT03795233 | CDI | FMT, Vancomycin | FMT for primary CDI restored microbiome diversity compared to patients who did not receive FMT, and had a high rate of clinical cure and patient satisfaction. | |
| NCT02706717 | HIV Infection | Visbiome | Visbiome reduced inflammation in HIV-infected men and women compared to placebo, and had no serious adverse effects [93]. | |
| NCT03005379 | CDI | FMT | FMT was not superior to placebo in preventing recurrent CDI in patients with a history of recurrent or severe CDI [94]. | |
| NCT03106844 | IBD, CDI | FMT | FMT was safe and effective for patients with IBD and CDI, and resulted in a significant improvement in gut microbiota composition and function. | |
| NCT01680640 | NAFLD | Dietary Supplement: Synbiotic, Maltodextrin | Synbiotic treatment improved liver function, insulin resistance, and gut microbiota diversity in patients with NAFLD [95,96]. | |
| NCT03621657 | CDI | FMT | FMT increased the gut microbiota diversity and richness, and reduced the recurrence of Clostridium difficile infection in patients with a history of CDI. |
| Parent Compound | Metabolic Types | Active Compound | Involved Microbiota Species | Pharmacological Activity | Reference |
|---|---|---|---|---|---|
 | Azo reduction |  | Escherichia coli; Enterococcus faecalis; Clostridium perfringens; Bacteroides fragilis | Anti-bacterial | [121] |
 | Azo reduction |  | Escherichia coli; Enterococcus faecalis; Clostridium perfringens; Bacteroides fragilis | Anti-bacterial | [122] |
 | Azo reduction |  | Escherichia coli; Bacteroides fragilis; Clostridium perfringens | Anti-bacterial | [123] |
 | Azo reduction |  | Escherichia coli; Bacteroides fragilis; Clostridium perfringens | Anti-bacterial | [124] |
 | Azo reduction |  | Escherichia coli; Bacteroides fragilis; Clostridium perfringens | Anti-bacterial | [125] |
 | Reduction |  | Slackia isoflavoniconvertens; Lactococcus garvieae; Adlercreutzia equolifaciens; Eggerthella lenta | Estrogenic | [126] |
 | Reduction |  | Escherichia coli; Enterococcus faecalis; Veillonella sp. | Anti-inflammation | [127] |
 | Oxidation |  | Escherichia coli; Clostridium perfringens; Lactobacillus sp. | Anti-neoplastic | [128] |
 | Oxidation |  | Escherichia coli; Enterococcus sp.; Streptococcus sp. | Anti-neoplastic | [129] |
 | Cleavage of N-oxide bond |  | Escherichia coli; Enterococcus sp. | Anti-laxative | [130] |
 | Decarboxylation |  | Enterococcus sp.; Lactobacillus sp.; Streptococcus sp. | Anti-parkinsonian | [131] |
 | Hydrolysis |  | Escherichia coli; Enterococcus sp.; Bacteroides sp. | Anti-bacterial | [132] |
 | Hydrolysis |  | Clostridium sp.; Eubacterium sp.; Lactobacillus sp. | Cholesterol-lowering | [25] |
 | Hydrolysis |  | Escherichia coli; Bacteroides fragilis; Clostridium perfringens | Laxative | [133] |
 | Hydrolysis |  | Escherichia coli; Bifidobacterium longum; Enterococcus faecalis | Anti-neoplastic | [7] |
 | Deconjugation |  | Escherichia coli; Eubacterium limosum; Ruminococcus sp. | Estrogenic | [31] |
 | Deconjugation |  | Escherichia coli; Bacteroides fragilis; Eubacterium ramulus; Firmicutes sp. | Anti-inflammatory | [134] |
 | Deconjugation |  | Escherichia coli; Clostridium sp.; Ruminococcus sp.; Bifidobacterium sp. | Anti-neoplastic | [135] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, S.; Ju, D.; Zeng, X. Mechanisms and Clinical Implications of Human Gut Microbiota-Drug Interactions in the Precision Medicine Era. Biomedicines 2024, 12, 194. https://doi.org/10.3390/biomedicines12010194
Wang S, Ju D, Zeng X. Mechanisms and Clinical Implications of Human Gut Microbiota-Drug Interactions in the Precision Medicine Era. Biomedicines. 2024; 12(1):194. https://doi.org/10.3390/biomedicines12010194
Chicago/Turabian StyleWang, Shuaiqi, Dianwen Ju, and Xian Zeng. 2024. "Mechanisms and Clinical Implications of Human Gut Microbiota-Drug Interactions in the Precision Medicine Era" Biomedicines 12, no. 1: 194. https://doi.org/10.3390/biomedicines12010194