
Novel Noninvasive Paraclinical Study Method for Investigation of Liver Diseases
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Bioimpedance Spectral Measurement
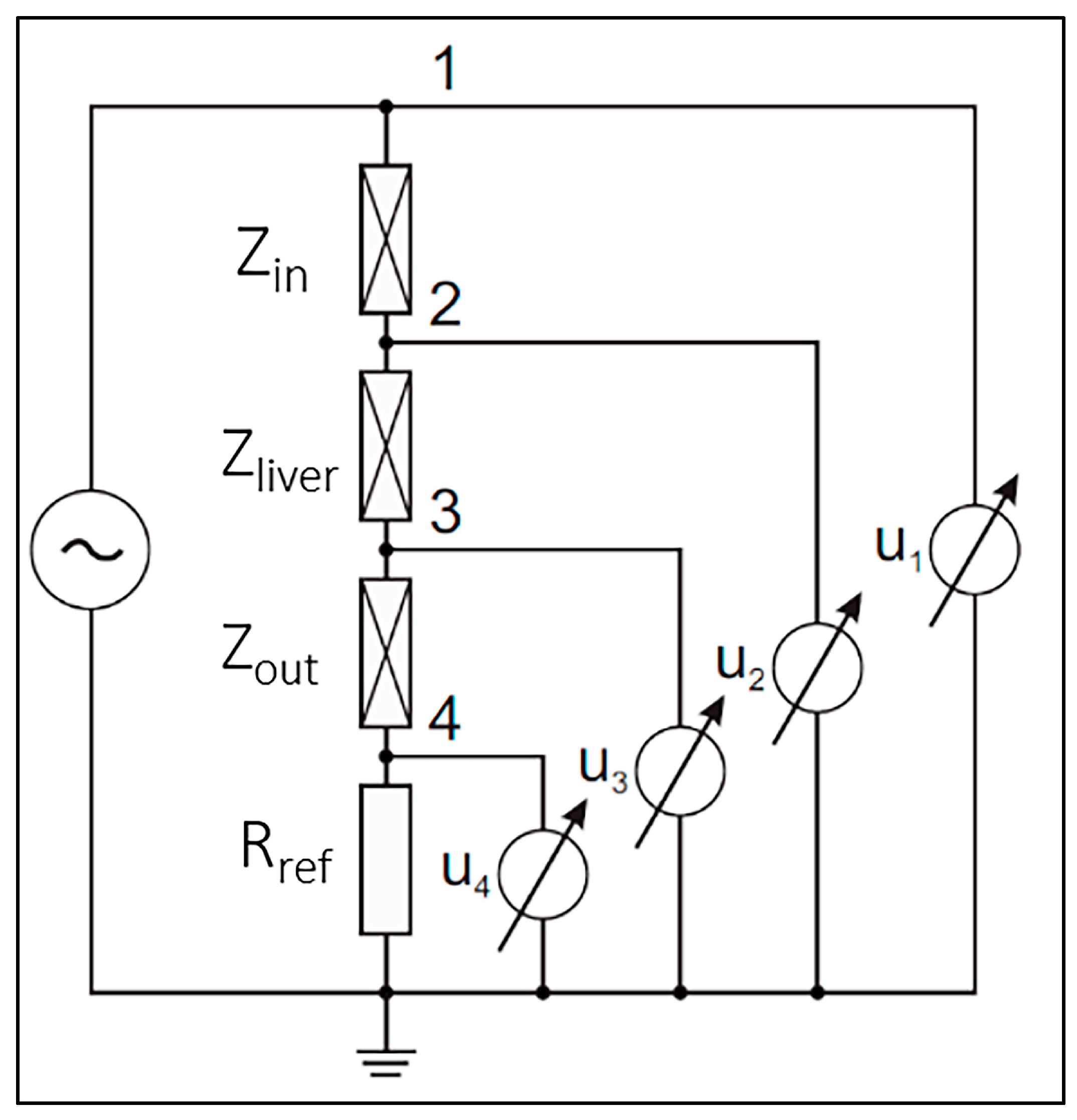
2.1.1. BIS Measurement Principal
2.1.2. Small Laboratory Animal Model BIS Measurements
- Generator signal: monochrome sine;
- Voltage generator amplitude: 1 mV–1 V (peak to peak);
- Frequency range: 1 Hz–100 kHz;
- Number of measuring channels: 4;
- Stored measurement result: Transfer function (absolute value and phase);
- Dynamic range: 140 dB;
- Measurement accuracy: <1 ppm magnitude and <±0.001° phase;
- Resolution of measurement result: double precision (fixed point arithmetic);
- Input AD conversion, generator DA conversion: 24 bits;
- Measurement function: bioimpedance spectrum measurement;
- Power supply: Battery operated.
2.1.3. Clinical BIS Measurements
2.2. Animal Experiment
2.2.1. Animals
2.2.2. Diet
2.2.3. Supplementary Examinations
2.3. Clinical Study
2.3.1. Patients
2.3.2. Statistical Data
2.3.3. Histological Examination of the Liver Sample
2.4. BIS Data Evaluation
3. Results
3.1. Animal Experiment
3.1.1. BIS Measurements
3.1.2. Statistical Data
3.1.3. Micro-CT Scan
3.1.4. Blood Test
3.1.5. Histological Analysis
3.2. Clinical Study
3.2.1. BIS Measurement
3.2.2. Statistical Data
3.2.3. Histological Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kechagias, S.; Ekstedt, M.; Simonsson, C.; Nasr, P. Non-invasive diagnosis and staging of non-alcoholic fatty liver disease. Hormones 2022, 21, 349–368. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.N. Non-alcoholic fatty liver disease—A global public health perspective. J. Hepatol. 2019, 70, 531–544. [Google Scholar] [CrossRef]
- Friedman, S.L.; Neuschwander-Tetri, B.A.; Rinella, M.; Sanyal, A.J. Mechanisms of NAFLD development and therapeutic strategies. Nat. Med. 2018, 24, 908–922. [Google Scholar] [CrossRef] [PubMed]
- Petzold, G. Role of Ultrasound Methods for the Assessment of NAFLD. J. Clin. Med. 2022, 11, 4581. [Google Scholar] [CrossRef] [PubMed]
- Riazi, K.; Azhari, H.; Charlette, J.H.; Underwood, F.E.; King, J.A.; Afshar, E.E.; Swain, M.G.; Congly, S.E.; Kaplan, G.G.; Shaheen, A.-A. The prevalence and incidence of NAFLD worldwide: A systematic review and meta-analysis. Gastroenterol. Hepatol. 2022, 7, 851–861. [Google Scholar]
- Alqahtani, S.A.; Schattenberg, J.M. NAFLD in the Elderly. Clin. Interv. Aging 2021, 16, 1633–1649. [Google Scholar] [CrossRef]
- Dowman, J.K.; Tomlinson, J.W.; Newsome, P.N. Pathogenesis of non-alcoholic fatty liver disease. QJM Int. J. Med. 2010, 103, 71–83. [Google Scholar] [CrossRef]
- Ballestri, S.; Nascimbeni, F.; Baldelli, E.; Marrazzo, A.; Romagnoli, D.; Lonardo, A. NAFLD as a Sexual Dimorphic Disease: Role of Gender and Reproductive Status in the Development and Progression of Nonalcoholic Fatty Liver Disease and Inherent Cardiovascular Risk. Adv. Ther. 2017, 34, 1291–1326. [Google Scholar] [CrossRef]
- Jonas, W.; Schürmann, A. Genetic and epigenetic factors determining NAFLD risk. Mol. Metab. 2021, 50, 101111. [Google Scholar] [CrossRef]
- Kang, D.; Zhao, D.; Ryu, S.; Guallar, E.; Cho, J.; Lazo, M.; Shin, H.; Chang, Y.; Sung, E. Perceived stress and non-alcoholic fatty liver disease in apparently healthy men and women. Sci. Rep. 2020, 10, 38. [Google Scholar] [CrossRef]
- Zhang, S.; Ma, C.; Wang, X.; Wang, Q.; Song, W.; Li, C.; Zhai, C.; Qi, Y.; Fan, S.; Cheng, F. Impact of chronic psychological stress on nonalcoholic fatty liver disease. Int. J. Clin. Exp. Med. 2019, 12, 7991–7998. [Google Scholar]
- Basu, R.; Noureddin, M.; Clark, J.M. Nonalcoholic Fatty Liver Disease: Review of Management for Primary Care Providers. Mayo Clin. Proc. 2022, 97, 1700–1716. [Google Scholar] [CrossRef] [PubMed]
- Panera, N.; Barbaro, B.; Della Corte, C.; Mosca, A.; Nobili, V.; Alisi, A. A review of the pathogenic and therapeutic role of nutrition in pediatric nonalcoholic fatty liver disease. Nutr. Res. 2018, 58, 1–16. [Google Scholar] [CrossRef]
- Zhu, B.; Chan, S.L.; Li, J.; Li, K.; Wu, H.; Cui, K.; Chen, H. Non-alcoholic Steatohepatitis Pathogenesis, Diagnosis, and Treatment. Front. Cardiovasc. Med. 2021, 8, 742382. [Google Scholar] [CrossRef] [PubMed]
- Tannapfel, A.; Denk, H.; Dienes, H.P.; Langner, C.; Schirmacher, P.; Trauner, M.; Flott-Rahmel, B. Histopathological diagnosis of non-alcoholic and alcoholic fatty liver disease. Virchows Arch. 2011, 458, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Lăpădat, A.M.; Jianu, I.R.; Ungureanu, B.S.; Florescu, L.M.; Gheonea, D.I.; Sovaila, S.; Gheonea, I.A. Non-invasive imaging techniques in assessing non-alcoholic fatty liver disease: A current status of available methods. J. Med. Life 2017, 10, 19–26. [Google Scholar] [CrossRef]
- Li, Q.; Dhyani, M.; Grajo, J.R.; Sirlin, C.; Samir, A.E. Current status of imaging in nonalcoholic fatty liver disease. World J. Hepatol. 2018, 10, 530–542. [Google Scholar] [CrossRef]
- Jang, W.; Song, J.S. Non-Invasive Imaging Methods to Evaluate Non-Alcoholic Fatty Liver Disease with Fat Quantification: A Review. Diagnostics 2023, 13, 1852. [Google Scholar] [CrossRef]
- Wentworth, B.J.; Caldwell, S.H. Pearls and pitfalls in nonalcoholic fatty liver disease: Tricky results are common. Metab. Target. Organ. Damage. 2021, 1, 2. [Google Scholar]
- Shrestha, R.; Kc, S.; Thapa, P.; Pokharel, A.; Karki, N.; Jaishi, B. Estimation of Liver Fat by FibroScan in Patients with Nonalcoholic Fatty Liver Disease. Cureus 2021, 13, e16414. [Google Scholar] [CrossRef]
- Yang, A.; Nguyen, M.; Ju, I.; Brancatisano, A.; Ryan, B.; van der Poorten, D. Utility of Fibroscan XL to assess the severity of non-alcoholic fatty liver disease in patients undergoing bariatric surgery. Sci. Rep. 2021, 11, 14006. [Google Scholar] [CrossRef] [PubMed]
- Parramon, D.; Erill, I.; Guimerà, A.; Ivorra, A.; Muñoz, A.; Sola, A.; Fondevila, C.; García-Valdecasas, J.C.; Villa, R. In vivo detection of liver steatosis in rats based on impedance spectroscopy. Physiol. Meas. 2007, 28, 813–828. [Google Scholar] [CrossRef] [PubMed]
- Showkat, I.; Khanday, F.A.; Beigh, M.R. A review of bio-impedance devices. Med. Biol. Eng. Comput. 2023, 61, 927–950. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, A.C.; Bartok, C.; Schoeller, D.A. The Validity of Bioelectrical Impedance Models in Clinical Populations. Nutr. Clin. Pract. 2004, 19, 433–446. [Google Scholar] [CrossRef]
- Jaffrin, M.Y.; Morel, H. Body fluid volumes measurements by impedance: A review of bioimpedance spectroscopy (BIS) and bioimpedance analysis (BIA) methods. Med. Eng. Phys. 2008, 30, 1257–1269. [Google Scholar] [CrossRef]
- Yamada, Y.; Watanabe, Y.; Ikenaga, M.; Yokoyama, K.; Yoshida, T.; Morimoto, T.; Kimura, M. Comparison of single- or multifrequency bioelectrical impedance analysis and spectroscopy for assessment of appendicular skeletal muscle in the elderly. J. Appl. Physiol. 2013, 115, 812–818. [Google Scholar] [CrossRef]
- Schwenger, K.J.P.; Kiu, A.; Ali, M.; Alhanaee, A.; Fischer, S.E.; Allard, J.P. Comparison of bioelectrical impedance analysis, mass index, and waist circumference in assessing risk for non-alcoholic steatohepatitis. Nutrition 2022, 93, 111491. [Google Scholar] [CrossRef]
- Choi, J.W.; Yoo, J.-J.; Kim, S.G.; Kim, Y.S. Bioelectrical Impedance Analysis Can Be an Effective Tool for Screening Fatty Liver in Patients with Suspected Liver Disease. Healthcare 2022, 10, 2268. [Google Scholar] [CrossRef]
- Chen, G.; Lv, Y.; Ni, W.; Shi, Q.; Xiang, X.; Li, S.; Song, C.; Xiao, M.; Jin, S. Associations between Phase Angle Values Obtained by Bioelectrical Impedance Analysis and Nonalcoholic Fatty Liver Disease in an Overweight Population. Can. J. Gastroenterol. Hepatol. 2020, 2020, 8888405. [Google Scholar] [CrossRef]
- Campa, F.; Toselli, S.; Mazzilli, M.; Gobbo, L.A.; Coratella, G. Assessment of Body Composition in Athletes: A Narrative Review of Available Methods with Special Reference to Quantitative and Qualitative Bioimpedance Analysis. Nutrients 2021, 13, 1620. [Google Scholar] [CrossRef]
- Verney, J.; Mezt, L.; Chaplais, E.; Cardenoux, C.; Pereira, B.; Thivel, D. Bioelectrical impedance is an accurate methon to asses body composition in obese but not severely obese adolescents. Nutr. Res. 2016, 30, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Orkin, S.; Yodoshi, T.; Romantic, E.; Hitchcock, K.; Arce-Clachar, A.C.; Bramlage, K.; Sun, Q.; Fei, L.; Xanthakos, S.A.; Trout, A.T.; et al. Body compo-sition measured by bioelectrical impedance analysis is a viable alternative to magnetic resonance imaging in children with nonalcoholic fatty liver disease. J. Parenter. Enter. Nutr. 2022, 46, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Abe, Y.; Tonouchi, R.; Hara, M.; Okada, T.; Jego, E.H.; Taniguchi, T.; Koshinaga, T.; Morioka, I. Visceral Fat Area Measured by Abdominal Bioelectrical Impedance Analysis in School-Aged Japanese Children. J. Clin. Med. 2022, 11, 4148. [Google Scholar] [CrossRef]
- Wu, T.C.; Chen, L.K.; Tsai, S.H.; Liaw, Y.H.; Hwang, B. Hepatic steatosis: An experimental model for quantification. Arch. Gerontol. Geriatr. 2011, 52, 164–166. [Google Scholar] [CrossRef]
- Davis, K.; Kowdley, K.V.; Unalp, A.; Kanwal, F.; Brunt, M.E.; Schwimmer, J.B. Quality of life in adults with nonalcoholic fatty liver disease: Baseline data from the nonalcoholic steatohepatitis clinical research network. Hepatology 2009, 49, 1904–1912. [Google Scholar]
- Hessheimer, A.J.; Parramón, D.; Guimerà, A.; Erill, I.; Rimola, A.; García-Valdecasas, J.C.; Villa, R.; Fondevila, C. A rapid and reliable means of assessing hepatic steatosis in vivo via electrical bioimpedance. Transplantation 2009, 88, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Gyorfi, N.; Nadasdi, L.; Toth, A.; Klincsik, M.; Sari, Z.; Kuljic, B.; Odry, A.; Odry, P.; Vizvari, Z. A Modified Cole-Cole Model Used in the Evaluation of Low-Frequency Electrical Impedance Spectroscopy Measurements. Int. J. Syst. Appl.—Eng. Dev. 2019, 13, 195–199. [Google Scholar]
- Vizvari, Z.; Gyorfi, N.; Odry, A.; Sari, Z.; Klincsik, M.; Gergics, M.; Kovacs, L.; Kovacs, A.; Pal, J.; Karadi, Z.; et al. Physical Validation of a Residual Impedance Rejection Method during Ultra-Low Frequency Bio-Impedance Spectral Measurements. Sensors 2020, 20, 4686. [Google Scholar] [CrossRef]
- Gyorfi, N.; Odry, A.; Karadi, Z.; Odry, P.; Szakall, T.; Kuljic, B.; Toth, A.; Vizvari, Z. Development of Bioimpedance-based Measuring Systems for Diagnosis of Non-alcoholic Fatty Liver Disease. In Proceedings of the 2021 IEEE 15th International Symposium on Applied Computational Intelligence and Informatics (SACI), Timisoara, Romania, 19–21 May 2021; pp. 135–140. [Google Scholar]
- Győrfi, N.; Vereczkei, A.; Karadi, Z.; Kalmár Nagy, K.; Vizvari, Z.; Sari, Z.; Odry, P.; Gál, A.R.; Tóth, A. The next milestone in clinical trial of a measurement system developed to diagnose NAFLD. In Proceedings of the 21th IEEE International Symposium on Computational Intelligence and Informatics (CINTI 2021), Budapest, Hungary, 18–20 November 2021; pp. 199–204. [Google Scholar]
- Santhekadur, P.K.; Kumar, D.P.; Sanyal, A.J. Preclinical models of non-alcoholic fatty liver disease. J. Hepatol. 2018, 68, 230–237. [Google Scholar] [CrossRef]
- Carreres, L.; Jílková, Z.M.; Vial, G.; Marche, P.N.; Decaens, T.; Lerat, H. Modeling Diet-Induced NAFLD and NASH in Rats: A Comprehensive Review. Biomedicines 2021, 9, 378. [Google Scholar] [CrossRef]
- Clark, J.M.; Bracanti, F.L.; Diehl, A.M. Nonalcoholic fatty liver disease. Gastroenterology 2002, 122, 1649–1657. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | Interpretation |
|---|---|
| S0 | No steatosis (<5%) |
| S1 | Mild steatosis (5–33%) |
| S2 | Moderate steatosis (34–66%) |
| S3 | Marked steatosis (>67%) |
| All Animals | SAF 0+0+0 | SAF 1+0+0 | SAF 2+0+0 | |
|---|---|---|---|---|
| n (%) | 60 | 23 (38%) | 26 (43%) | 11 (19%) |
| Day 1 body weight (g) (mean ± SD) | 305.3 ± 50.4 | 308.4 ± 30.4 | 302.6 ± 49.6 | 304.9 ± 32.6 |
| Day 90 body weight (g) (mean ± SD) | 491.5 ± 79.8 | 391.8 ± 32.4 | 508.7 ± 72.9 | 534.7 ± 69.4 |
| Liver weight (g) (mean ± SD) | 14.4 ± 3.1 | 10.2 ± 0.9 | 14.7 ± 1.7 | 17.3 ± 3.2 |
| Abdominal circumference (cm) (mean ± SD) | 18.8 ± 2.3 | 16.9 ± 0.8 | 18.9 ± 2.1 | 20.2 ± 2.7 |
| Animal Number | AST/GOT (U/L) | ALT/GPT (U/L) | GGT/γGT (U/L) | Chol (mmol/L) | Trigl. (mmol/L) | HDL (mmol/L) | LDL (mmol/L) | Glucose (mmol/L) | Uric Acid (µmol/L) |
|---|---|---|---|---|---|---|---|---|---|
| 20 (SAF score: 0) | 377 | 79 | 0 | 1.73 | 1.27 | 1.05 | 0.32 | 6.68 | 64 |
| 4 (SAF score: 1) | 503 | 66 | 0 | 1.97 | 0.97 | 1.2 | 0.48 | 5.7 | 86 |
| 10 (SAF score: 2) | 199 | 47 | 0 | 2.11 | 2.82 | 1.03 | 0.62 | 9.79 | 49 |
| Characteristic/Group | All Patients | SAF 0+0+0 (n = 4) | SAF 1+0+0 (n = 15) | SAF 2+0+0 (n = 7) |
|---|---|---|---|---|
| Female (n (%)) | 21 (80%) | 3 (75%) | 11 (73%) | 7 (100%) |
| Male (n (%)) | 5 (20%) | 1 (25%) | 4 (27%) | 0 (0%) |
| Age (mean ± SD) years | 51 ± 13.6 | 52 ± 12.1 | 50 ± 13.2 | 53 ± 16.9 |
| Weight (mean ± SD) kg | 84.6 ± 19.4 | 64.0 ± 7.1 | 88.0 ± 16.0 | 88.3 ± 25.5 |
| Waist circumference (mean ± SD) cm | 98.3 ± 13.6 | 87.0 ± 8.1 | 98.6 ± 13.4 | 104.3 ± 13.9 |
| BMI (mean ± SD) kg/m2 | 29.9 ± 7.1 | 24 ± 2.6 | 30 ± 4.9 | 34 ± 9.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gyorfi, N.; Gal, A.R.; Fincsur, A.; Kalmar-Nagy, K.; Mintal, K.; Hormay, E.; Miseta, A.; Tornoczky, T.; Nemeth, A.K.; Bogner, P.; et al. Novel Noninvasive Paraclinical Study Method for Investigation of Liver Diseases. Biomedicines 2023, 11, 2449. https://doi.org/10.3390/biomedicines11092449
Gyorfi N, Gal AR, Fincsur A, Kalmar-Nagy K, Mintal K, Hormay E, Miseta A, Tornoczky T, Nemeth AK, Bogner P, et al. Novel Noninvasive Paraclinical Study Method for Investigation of Liver Diseases. Biomedicines. 2023; 11(9):2449. https://doi.org/10.3390/biomedicines11092449
Chicago/Turabian StyleGyorfi, Nina, Adrian Robert Gal, Andras Fincsur, Karoly Kalmar-Nagy, Kitti Mintal, Edina Hormay, Attila Miseta, Tamas Tornoczky, Anita Katalin Nemeth, Peter Bogner, and et al. 2023. "Novel Noninvasive Paraclinical Study Method for Investigation of Liver Diseases" Biomedicines 11, no. 9: 2449. https://doi.org/10.3390/biomedicines11092449