

Washed Microbiota Transplantation Improves Patients with Overweight by the Gut Microbiota and Sphingolipid Metabolism
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
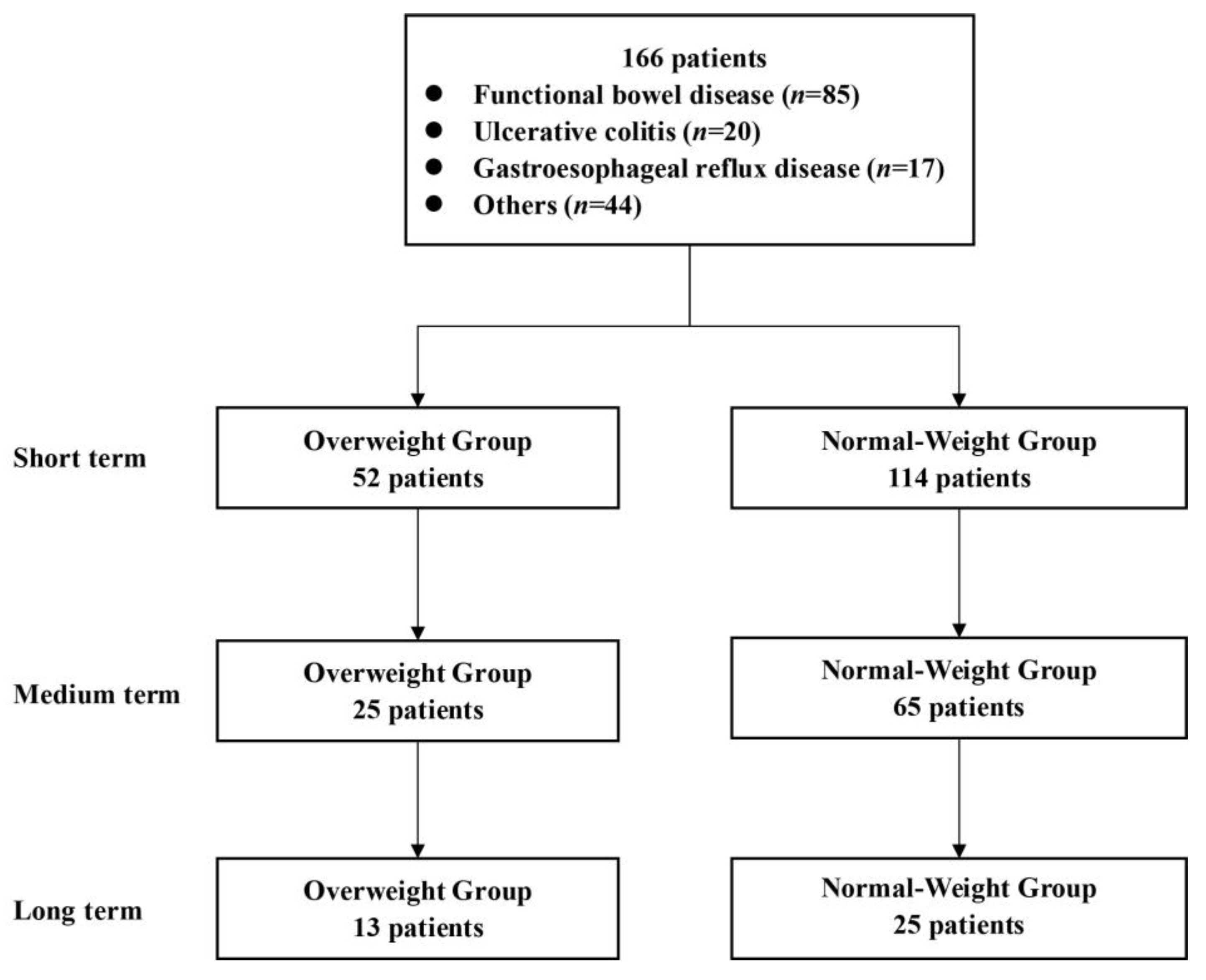
2.1. Patients and Experimental Design
2.2. Preparation of Washed Microbiota and WMT Process
2.3. Clinical Data Collection
2.4. DNA Extraction and Sequencing
2.5. Amplicon Data Processing and Analysis
2.6. Extraction and Data Analysis of Lipidomics and Sphingolipomics
2.7. Data Analysis
3. Results
3.1. Clinical Features of Patients Receiving WMT
3.2. Comprehensive Clinical Efficacy Evaluation of WMT for Overweight Patients
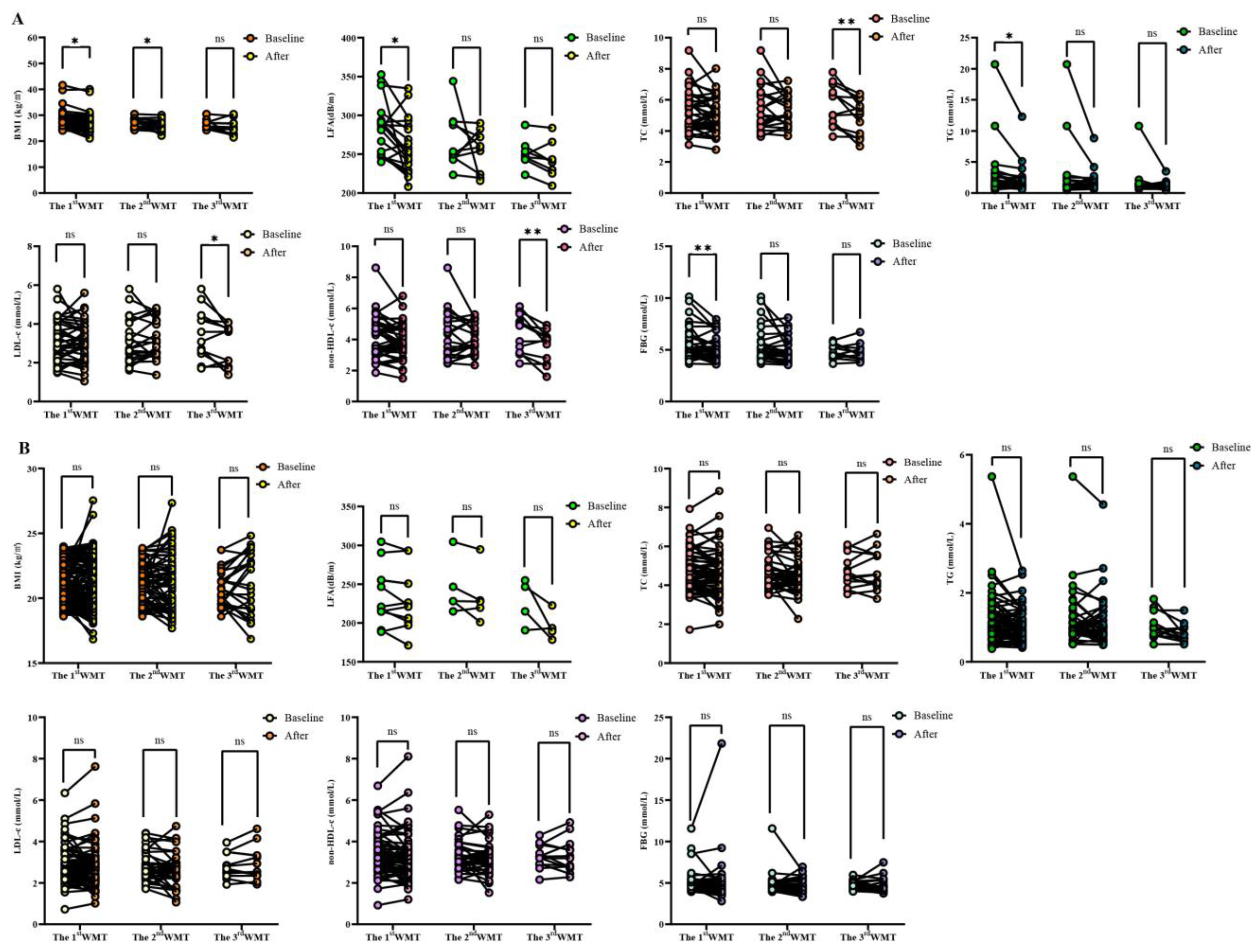
3.3. Comparative Analysis of Each Index after WMT Treatment and Baseline
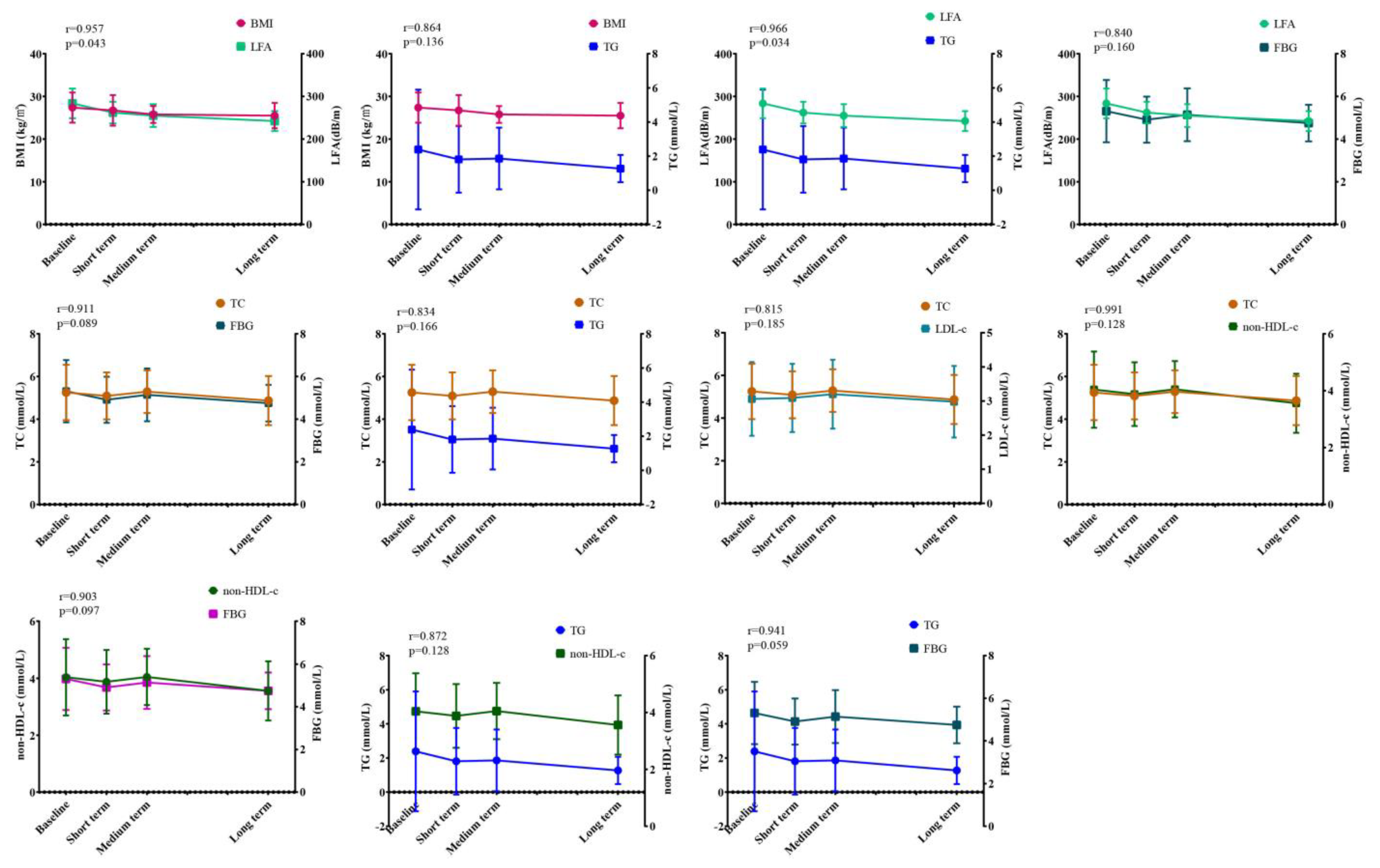
3.4. Correlation Analysis of WMT on Overweight Index
3.5. Prevalence of Adverse Events (AEs) in Patients Undergoing WMT
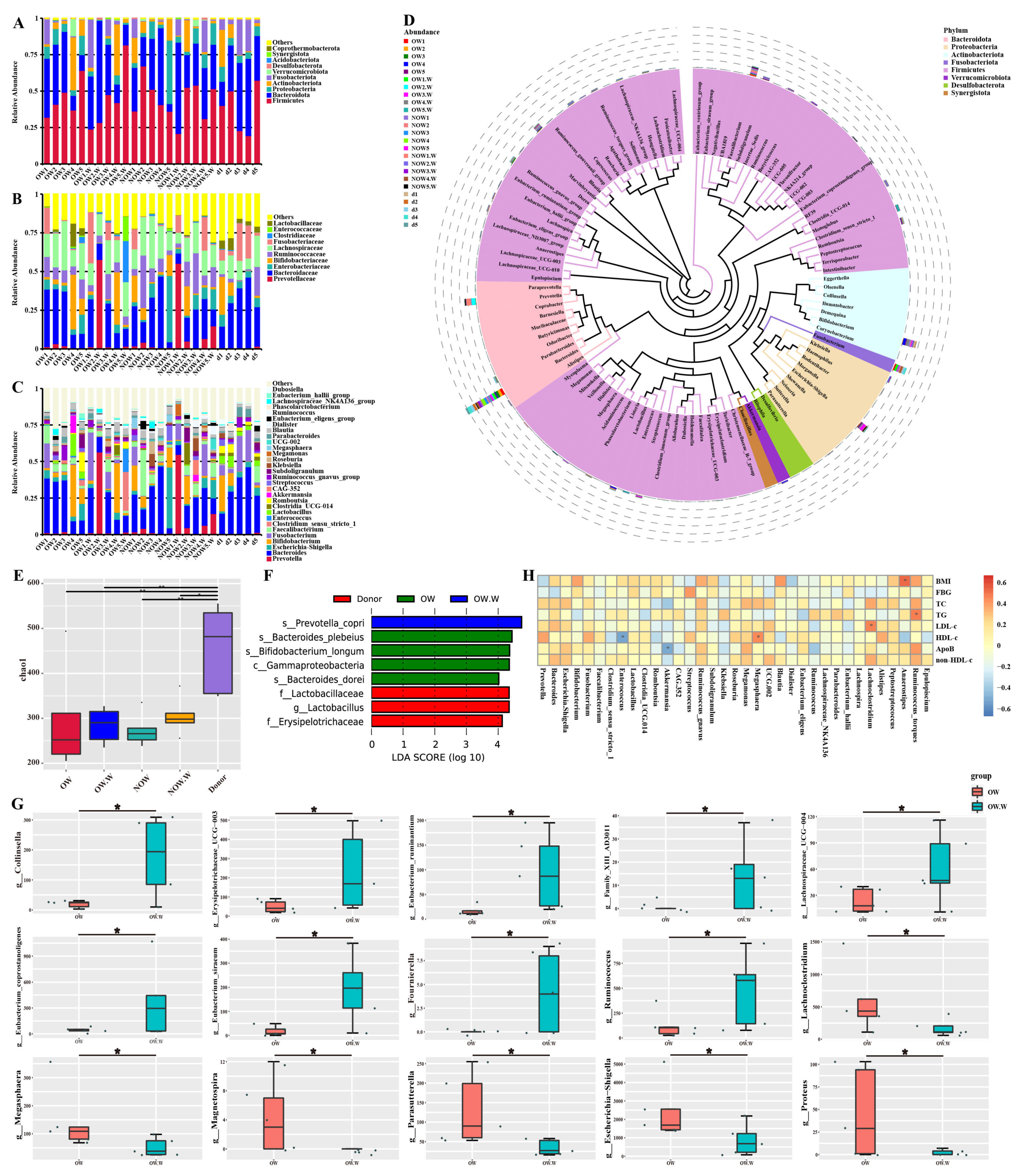
3.6. Analysis of Gut Microbiota Composition before and after WMT
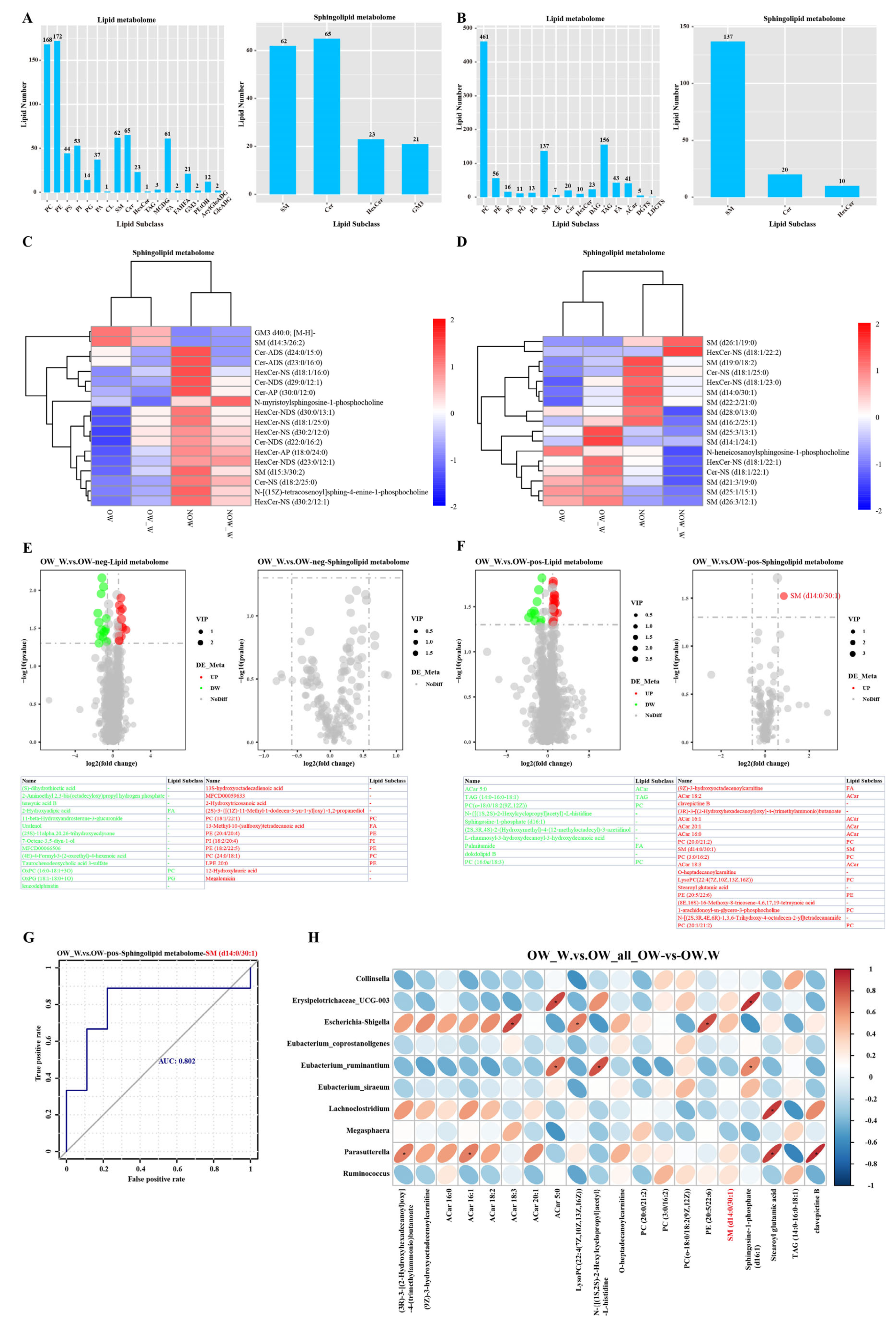
3.7. Analysis of Sphingolipid Metabolism before and after WMT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Bovolini, A.; Garcia, J.; Andrade, M.A.; Duarte, J.A. Metabolic Syndrome Pathophysiology and Predisposing Factors. Int. J. Sports Med. 2021, 42, 199–214. [Google Scholar] [CrossRef] [PubMed]
- Albi, E.; Alessenko, A.; Grösch, S. Sphingolipids in Inflammation. Mediat. Inflamm. 2018, 2018, 7464702. [Google Scholar] [CrossRef] [PubMed]
- Chaurasia, B.; Summers, S.A. Ceramides—Lipotoxic Inducers of Metabolic Disorders. Trends Endocrinol. Metab. 2015, 26, 538–550. [Google Scholar] [CrossRef]
- Mousa, A.; Naderpoor, N.; Mellett, N.; Wilson, K.; Plebanski, M.; Meikle, P.J.; de Courten, B. Lipidomic profiling reveals early-stage metabolic dysfunction in overweight or obese humans. Biochim. Biophys. Acta (BBA) Mol. Cell Biol. Lipids 2019, 1864, 335–343. [Google Scholar] [CrossRef]
- Yaribeygi, H.; Bo, S.; Ruscica, M.; Sahebkar, A. Ceramides and diabetes mellitus: An update on the potential molecular relationships. Diabet. Med. 2020, 37, 11–19. [Google Scholar] [CrossRef]
- Sokolowska, E.; Blachnio-Zabielska, A. The Role of Ceramides in Insulin Resistance. Front. Endocrinol. 2019, 10, 577. [Google Scholar] [CrossRef]
- Turnbaugh, P.J.; Ley, R.E.; Mahowald, M.A.; Magrini, V.; Mardis, E.R.; Gordon, J.I. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 2006, 444, 1027–1031. [Google Scholar] [CrossRef]
- Le Chatelier, E.; Nielsen, T.; Qin, J.; Prifti, E.; Hildebrand, F.; Falony, G.; Almeida, M.; Arumugam, M.; Batto, J.-M.; Kennedy, S.; et al. Richness of human gut microbiome correlates with metabolic markers. Nature 2013, 500, 541–546. [Google Scholar] [CrossRef]
- Bafeta, A.; Yavchitz, A.; Riveros, C.; Batista, R.; Ravaud, P. Methods and Reporting Studies Assessing Fecal Microbiota Transplantation: A Systematic Review. Ann. Intern. Med. 2017, 167, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Varier, R.U.; Biltaji, E.; Smith, K.J.; Roberts, M.S.; Jensen, M.K.; LaFleur, J.; Nelson, R.E. Cost-effectiveness analysis of fecal microbiota transplantation for recurrent Clostridium difficile infection. Infect. Control Hosp. Epidemiol. 2015, 36, 438–444. [Google Scholar] [CrossRef] [PubMed]
- De Groot, P.; Scheithauer, T.; Bakker, G.J.; Prodan, A.; Levin, E.; Khan, M.T.; Herrema, H.; Ackermans, M.; Serlie, M.J.M.; de Brauw, M.; et al. Donor metabolic characteristics drive effects of faecal microbiota transplantation on recipient insulin sensitivity, energy expenditure and intestinal transit time. Gut 2020, 69, 502–512. [Google Scholar] [CrossRef] [PubMed]
- Moayyedi, P.; Surette, M.G.; Kim, P.T.; Libertucci, J.; Wolfe, M.; Onischi, C.; Armstrong, D.; Marshall, J.K.; Kassam, Z.; Reinisch, W.; et al. Fecal Microbiota Transplantation Induces Remission in Patients with Active Ulcerative Colitis in a Randomized Controlled Trial. Gastroenterology 2015, 149, 102–109.e6. [Google Scholar] [CrossRef]
- Paramsothy, S.; Kamm, M.A.; Kaakoush, N.O.; Walsh, A.J.; van den Bogaerde, J.; Samuel, D.; Leong, R.W.L.; Connor, S.; Ng, W.; Paramsothy, R.; et al. Multidonor intensive faecal microbiota transplantation for active ulcerative colitis: A randomised placebo-controlled trial. Lancet 2017, 389, 1218–1228. [Google Scholar] [CrossRef]
- Pamer, E.G. Fecal microbiota transplantation: Effectiveness, complexities, and lingering concerns. Mucosal Immunol. 2014, 7, 210–214. [Google Scholar] [CrossRef]
- Zhang, T.; Lu, G.; Zhao, Z.; Liu, Y.; Shen, Q.; Li, P.; Chen, Y.; Yin, H.; Wang, H.; Marcella, C.; et al. Washed microbiota transplantation vs. manual fecal microbiota transplantation: Clinical findings, animal studies and in vitro screening. Protein Cell 2020, 11, 251–266. [Google Scholar] [CrossRef]
- Endocrinology Branch of Chinese Medical Association. Endocrinology: Multidisciplinary clinical consensus on diagnosis and treatment of obesity (2021 edition). Chin. J. Obes. Metab. Dis. 2021, 7, 211–226. [Google Scholar] [CrossRef]
- Zhu, D. Chinese Diabetes: Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin. J. Pract. Intern. Med. 2021, 41, 668–695. [Google Scholar] [CrossRef]
- Fecal Microbiota Transplantation-standardization Study Group. Nanjing consensus on methodology of washed microbiota transplantation. Chin. Med. J. 2020, 133, 2330–2332. [Google Scholar] [CrossRef]
- Qin, J.; Li, Y.; Cai, Z.; Li, S.; Zhu, J.; Zhang, F.; Liang, S.; Zhang, W.; Guan, Y.; Shen, D.; et al. A metagenome-wide association study of gut microbiota in type 2 diabetes. Nature 2012, 490, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Magoč, T.; Salzberg, S.L. FLASH: Fast length adjustment of short reads to improve genome assemblies. Bioinformatics 2011, 27, 2957–2963. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Zhou, Y.; Chen, Y.; Gu, J. fastp: An ultra-fast all-in-one FASTQ preprocessor. Bioinformatics 2018, 34, i884–i890. [Google Scholar] [CrossRef] [PubMed]
- Haas, B.J.; Gevers, D.; Earl, A.M.; Feldgarden, M.; Ward, D.V.; Giannoukos, G.; Ciulla, D.; Tabbaa, D.; Highlander, S.K.; Sodergren, E.; et al. Chimeric 16S rRNA sequence formation and detection in Sanger and 454-pyrosequenced PCR amplicons. Genome Res. 2011, 21, 494–504. [Google Scholar] [CrossRef]
- Matyash, V.; Liebisch, G.; Kurzchalia, T.V.; Shevchenko, A.; Schwudke, D. Lipid extraction by methyl-tert-butyl ether for high-throughput lipidomics. J. Lipid Res. 2008, 49, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- Turnbaugh, P.J.; Gordon, J.I. The core gut microbiome, energy balance and obesity. J. Physiol. 2009, 587 Pt 17, 4153–4158. [Google Scholar] [CrossRef]
- Ridaura, V.K.; Faith, J.J.; Rey, F.E.; Cheng, J.; Duncan, A.E.; Kau, A.L.; Griffin, N.W.; Lombard, V.; Henrissat, B.; Bain, J.R.; et al. Gut microbiota from twins discordant for obesity modulate metabolism in mice. Science 2013, 341, 1241214. [Google Scholar] [CrossRef]
- Lai, Z.-L.; Tseng, C.-H.; Ho, H.J.; Cheung, C.K.Y.; Lin, J.-Y.; Chen, Y.-J.; Cheng, F.-C.; Hsu, Y.-C.; Lin, J.-T.; El-Omar, E.M.; et al. Fecal microbiota transplantation confers beneficial metabolic effects of diet and exercise on diet-induced obese mice. Sci. Rep. 2018, 8, 15625. [Google Scholar] [CrossRef]
- Louis, S.; Tappu, R.-M.; Damms-Machado, A.; Huson, D.H.; Bischoff, S.C. Characterization of the Gut Microbial Community of Obese Patients Following a Weight-Loss Intervention Using Whole Metagenome Shotgun Sequencing. PLoS ONE 2016, 11, e0149564. [Google Scholar] [CrossRef]
- Furet, J.-P.; Kong, L.-C.; Tap, J.; Poitou, C.; Basdevant, A.; Bouillot, J.-L.; Mariat, D.; Corthier, G.; Doré, J.; Henegar, C.; et al. Differential adaptation of human gut microbiota to bariatric surgery–induced weight loss: Links with metabolic and low-grade inflammation markers. Diabetes 2010, 59, 3049–3057. [Google Scholar] [CrossRef]
- Li, S.S.; Zhu, A.; Benes, V.; Costea, P.I.; Hercog, R.; Hildebrand, F.; Huerta-Cepas, J.; Nieuwdorp, M.; Salojärvi, J.; Voigt, A.Y.; et al. Durable coexistence of donor and recipient strains after fecal microbiota transplantation. Science 2016, 352, 586–589. [Google Scholar] [CrossRef]
- Azad, M.B.; Vehling, L.; Chan, D.; Klopp, A.; Nickel, N.C.; McGavock, J.M.; Becker, A.B.; Mandhane, P.J.; Turvey, S.E.; Moraes, T.J.; et al. Infant Feeding and Weight Gain: Separating Breast Milk from Breastfeeding and Formula from Food. Pediatrics 2018, 142, e20181092. [Google Scholar] [CrossRef]
- Smits, L.P.; Kootte, R.S.; Levin, E.; Prodan, A.; Fuentes, S.; Zoetendal, E.G.; Wang, Z.; Levison, B.S.; Cleophas, M.C.P.; Kemper, E.M.; et al. Effect of Vegan Fecal Microbiota Transplantation on Carnitine- and Choline-Derived Trimethylamine-N-Oxide Production and Vascular Inflammation in Patients with Metabolic Syndrome. J. Am. Heart Assoc. 2018, 7, e008342. [Google Scholar] [CrossRef]
- Sung, M.M.; Kim, T.T.; Denou, E.; Soltys, C.-L.M.; Hamza, S.M.; Byrne, N.J.; Masson, G.; Park, H.; Wishart, D.S.; Madsen, K.L.; et al. Improved Glucose Homeostasis in Obese Mice Treated with Resveratrol Is Associated with Alterations in the Gut Microbiome. Diabetes 2017, 66, 418–425. [Google Scholar] [CrossRef]
- Mestdagh, R.; Dumas, M.-E.; Rezzi, S.; Kochhar, S.; Holmes, E.; Claus, S.P.; Nicholson, J.K. Gut microbiota modulate the metabolism of brown adipose tissue in mice. J. Proteome Res. 2012, 11, 620–630. [Google Scholar] [CrossRef]
- Velagapudi, V.R.; Hezaveh, R.; Reigstad, C.S.; Gopalacharyulu, P.; Yetukuri, L.; Islam, S.; Felin, J.; Perkins, R.; Borén, J.; Orešič, M.; et al. The gut microbiota modulates host energy and lipid metabolism in mice. J. Lipid Res. 2010, 51, 1101–1112. [Google Scholar] [CrossRef]
- Haimovitz-Friedman, A.; Kolesnick, R.N.; Fuks, Z. Ceramide signaling in apoptosis. Br. Med. Bull. 1997, 53, 539–553. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Li, M.-Q.; Xie, Y.-T.; Zhang, Q.; Lu, X.-J.; Liu, T.; Lin, W.-Y.; Xu, J.-T.; Wu, Q.-P.; He, X.-X. Washed microbiota transplantation improves patients with high blood glucose in South China. Front. Endocrinol. 2022, 13, 985636. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Lu, X.-J.; Lin, D.-J.; Chen, W.-J.; Xue, X.-Y.; Liu, T.; Xu, J.-T.; Xie, Y.-T.; Li, M.-Q.; Lin, W.-Y.; et al. Washed microbiota transplantation improves patients with metabolic syndrome in South China. Front. Cell. Infect. Microbiol. 2022, 12, 1044957. [Google Scholar] [CrossRef]
- Wu, L.; Xie, X.; Zhang, J.; Ding, Y.; Wu, Q. Bacterial Diversity and Community in Regional Water Microbiota between Different Towns in World’s Longevity Township Jiaoling, China. Diversity 2021, 13, 361. [Google Scholar] [CrossRef]
- Wu, L.; Xie, X.; Li, Y.; Liang, T.; Zhong, H.; Ma, J.; Yang, L.; Yang, J.; Li, L.; Xi, Y.; et al. Metagenomics-Based Analysis of the Age-Related Cumulative Effect of Antibiotic Resistance Genes in Gut Microbiota. Antibiotics 2021, 10, 1006. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Xie, X.; Li, Y.; Liang, T.; Zhong, H.; Yang, L.; Xi, Y.; Zhang, J.; Ding, Y.; Wu, Q. Gut microbiota as an antioxidant system in centenarians associated with high antioxidant activities of gut-resident Lactobacillus. NPJ Biofilms Microbiomes 2022, 8, 102. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Xie, X.; Liang, T.; Ma, J.; Yang, L.; Yang, J.; Li, L.; Xi, Y.; Li, H.; Zhang, J.; et al. Integrated Multi-Omics for Novel Aging Biomarkers and Antiaging Targets. Biomolecules 2022, 12, 39. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary Cause for WMT | Number (n) | Percentage (%) |
|---|---|---|
| Functional bowel disease | 85 | 51.20% |
| Ulcerative colitis | 20 | 12.05% |
| Gastroesophageal reflux disease | 17 | 10.24% |
| Non-alcoholic fatty liver disease | 8 | 4.82% |
| Atopic dermatitis | 6 | 3.61% |
| Chemotherapy-associated diarrhea | 6 | 3.61% |
| Gouty arthritis | 5 | 3.01% |
| Posthepatitic cirrhosis | 3 | 1.81% |
| Crohn’s Disease | 3 | 1.81% |
| Radiation enteritis | 3 | 1.81% |
| Psoriasis vulgaris | 1 | 0.60% |
| Hyperuricemia | 1 | 0.60% |
| Depression | 1 | 0.60% |
| Senile tremor | 1 | 0.60% |
| Chronic urticaria | 1 | 0.60% |
| Functional dyspepsia | 1 | 0.60% |
| Bipolar disorder | 1 | 0.60% |
| Perianal eczema | 1 | 0.60% |
| Pustular psoriasis | 1 | 0.60% |
| Neuromyelitis optica | 1 | 0.60% |
| Total | 166 | 100.00% |
| Overweight Group (n = 52) | Normal-Weight Group (n = 114) | p Value | |
|---|---|---|---|
| Age (year) | 54.77 ± 16.74 (n = 52) | 50.61 ± 15.31 (n = 114) | 0.117 |
| Drinking history n (%) | 5 (9.62) | 4 (3.51) | 0.214 |
| History of smoking n (%) | 12 (23.08) | 14 (12.28) | 0.076 |
| Male n (%) | 34 (65.38) | 49 (42.98) | 0.007 |
| BMI (kg/m2) | 27.38 ± 3.54 (n = 52) | 21.17 ± 1.65 (n = 114) | <0.001 |
| LFA (dB/m) | 272.45 ± 34.65 (n = 29) | 221.22 ± 31.29 (n = 48) | <0.001 |
| LSM (kPa) | 7.81 ± 2.67 (n = 29) | 6.59 ± 2.74 (n = 48) | 0.060 |
| TC (mmol/L) | 5.20 ± 1.19 (n = 49) | 4.64 ± 0.99 (n = 102) | 0.003 |
| TG (mmol/L) | 2.18 ± 3.15 (n = 49) | 1.07 ± 0.62 (n = 102) | 0.018 |
| LDL-c (mmol/L) | 3.09 ± 1.03 (n = 49) | 2.84 ± 0.87 (n = 102) | 0.145 |
| HDL-c (mmol/L) | 1.20 ± 0.31 (n = 49) | 1.33 ± 0.33 (n = 102) | 0.026 |
| ApoB (g/L) | 1.02 ± 0.21 (n = 49) | 0.89 ± 0.22 (n = 102) | 0.001 |
| non-HDL-c (mmol/L) | 4.00 ± 1.23 (n = 49) | 3.32 ± 0.92 (n = 102) | 0.001 |
| LIP (mmol/L) | 146.31 ± 144.60 (n = 17) | 144.80 ± 158.40 (n = 31) | 0.974 |
| FBG (mmol/L) | 5.27 ± 1.40 (n = 52) | 4.72 ± 1.01 (n = 112) | 0.012 |
| HbA1c (%) | 6.44 ± 0.97 (n = 14) | 5.76 ± 0.84 (n = 9) | 0.099 |
| FI (μU/mL) | 12.84 ± 7.37 (n = 32) | 6.80 ± 3.33 (n = 64) | <0.001 |
| HOMA-IR | 3.19 ± 2.21 (n = 32) | 1.45 ± 0.80 (n = 62) | <0.001 |
| SBP (mmHg) | 126.87 ± 13.01 (n = 52) | 120.89 ± 12.93 (n = 114) | 0.006 |
| DBP (mmHg) | 78.94 ± 9.49 (n = 52) | 76.13 ± 9.40 (n = 114) | 0.077 |
| Data Periods | Before Therapy (n) | Therapeutic Effect Base on Overweight | |||
|---|---|---|---|---|---|
| Unchanged Group (n) | Changed Group (n, %) | X2 | p Value | ||
| OW Group | |||||
| Short term | 52 | 44 | 8 (15.4%) | 6.635 | 0.010 |
| Medium term | 20 | 16 | 4 (20.0%) | 2.500 | 0.114 |
| Long term | 10 | 7 | 3 (30.0%) | 1.569 | 0.210 |
| Items | Baseline | Short Term | p Value | Baseline | Medium Term | p Value | Baseline | Long Term | p Value |
|---|---|---|---|---|---|---|---|---|---|
| OW Group | |||||||||
| BMI (kg/m2) | 27.38 ± 3.54 (n = 52) | 26.73 ± 3.57 (n = 52) | 0.004 | 26.76 ± 1.71 (n = 20) | 25.78 ± 1.97 (n = 20) | 0.012 | 26.50 ± 1.93 (n = 10) | 25.50 ± 2.99 (n = 10) | 0.253 |
| LFA (dB/m) | 283.64 ± 34.72 (n = 18) | 262.14 ± 35.40 (n = 18) | 0.025 | 267.69 ± 35.60 (n = 10) | 254.99 ± 26.69 (n = 10) | 0.402 | 251.14 ± 18.16 (n = 8) | 242.20 ± 23.32 (n = 8) | 0.073 |
| LSM (kPa) | 8.21 ± 2.76 (n = 18) | 7.22 ± 2.96 (n = 18) | 0.277 | 7.26 ± 2.16 (n = 10) | 6.93 ± 1.75 (n = 10) | 0.747 | 7.69 ± 2.38 (n = 8) | 8.03 ± 2.35 (n = 8) | 0.728 |
| TC (mmol/L) | 5.25 ± 1.30 (n = 38) | 5.09 ± 1.10 (n = 38) | 0.279 | 5.47 ± 1.46 (n = 21) | 5.29 ± 1.00 (n = 21) | 0.402 | 5.66 ± 1.35 (n = 12) | 4.87 ± 1.15 (n = 12) | 0.007 |
| TG (mmol/L) | 2.39 ± 3.51 (n = 38) | 1.81 ± 1.95 (n = 38) | 0.036 | 2.66 ± 4.67 (n = 21) | 1.86 ± 1.81 (n = 21) | 0.235 | 2.01 ± 2.79 (n = 12) | 1.27 ± 0.80 (n = 12) | 0.254 |
| LDL-c (mmol/L) | 3.06 ± 1.08 (n = 38) | 3.09 ± 1.00 (n = 38) | 0.843 | 3.14 ± 1.18 (n = 21) | 3.20 ± 1.01 (n = 21) | 0.666 | 3.49 ± 1.31 (n = 12) | 2.98 ± 1.05 (n = 12) | 0.040 |
| HDL-c (mmol/L) | 1.2 ± 0.32 (n = 38) | 1.21 ± 0.3 (n = 38) | 0.749 | 1.28 ± 0.36 (n = 21) | 1.23 ± 0.30 (n = 21) | 0.227 | 1.34 ± 0.27 (n = 12) | 1.32 ± 0.28 (n = 12) | 0.562 |
| ApoB (g/L) | 1.04 ± 0.21 (n = 38) | 1.04 ± 0.24 (n = 38) | 0.832 | 1.02 ± 0.19 (n = 21) | 1.09 ± 0.20 (n = 21) | 0.044 | 1.09 ± 0.21 (n = 12) | 1.05 ± 0.20 (n = 12) | 0.375 |
| non-HDL-c (mmol/L) | 4.04 ± 1.34 (n = 38) | 3.88 ± 1.12 (n = 38) | 0.229 | 4.19 ± 1.57 (n = 21) | 4.05 ± 0.99 (n = 21) | 0.543 | 4.32 ± 1.26 (n = 12) | 3.56 ± 1.04 (n = 12) | 0.006 |
| LIP (mmol/L) | 147.96 ± 151.03 (n = 14) | 166.56 ± 168.51 (n = 14) | 0.034 | 258.35 ± 71.77 (n = 2) | 267.35 ± 23.26 (n = 2) | 0.837 | / | / | / |
| FBG (mmol/L) | 5.31 ± 1.46 (n = 46) | 4.91 ± 1.08 (n = 46) | 0.005 | 5.62 ± 1.81 (n = 24) | 5.14 ± 1.24 (n = 24) | 0.091 | 4.82 ± 0.70 (n = 11) | 4.75 ± 0.86 (n = 11) | 0.726 |
| HbA1c (%) | 6.53 ± 0.57 (n = 3) | 6.63 ± 0.81 (n = 3) | 0.622 | 7.75 ± 0.50 (n = 2) | 7.70 ± 0.28 (n = 2) | 0.942 | / | / | / |
| FI (μU/mL) | 12.27 ± 6.83 (n = 22) | 12.57 ± 5.16 (n = 22) | 0.835 | 10.38 ± 5.11 (n = 12) | 10.15 ± 5.01 (n = 12) | 0.809 | 11.82 ± 5.43 (n = 8) | 12.45 ± 5.44 (n = 8) | 0.628 |
| HOMA-IR | 3.02 ± 2.24 (n = 22) | 2.89 ± 1.61 (n = 22) | 0.813 | 2.47 ± 1.40 (n = 12) | 2.32 ± 1.19 (n = 12) | 0.533 | 2.55 ± 1.47 (n = 7) | 2.59 ± 1.35 (n = 7) | 0.902 |
| SBP (mmHg) | 126.87 ± 13.01 (n = 52) | 125.06 ± 10.65 (n = 52) | 0.321 | 125.48 ± 13.82 (n = 25) | 123.12 ± 11.66 (n = 25) | 0.451 | 121.38 ± 10.09 (n = 13) | 119.69 ± 10.70 (n = 13) | 0.713 |
| DBP (mmHg) | 78.94 ± 9.49 (n = 52) | 78.4 ± 8.86 (n = 52) | 0.759 | 78.64 ± 10.46 (n = 25) | 76.12 ± 8.21 (n = 25) | 0.252 | 75.85 ± 9.60 (n = 13) | 80.08 ± 7.78 (n = 13) | 0.223 |
| NOW Group | |||||||||
| BMI (kg/m2) | 21.15 ± 1.65 (n = 113) | 21.22 ± 2.00 (n = 113) | 0.609 | 21.22 ± 1.56 (n = 64) | 21.16 ± 2.13 (n = 64) | 0.760 | 20.79 ± 1.42 (n = 24) | 21.07 ± 2.35 (n = 24) | 0.399 |
| LFA (dB/m) | 236.34 ± 37.79 (n = 11) | 230.38 ± 38.60 (n = 11) | 0.101 | 244.56 ± 35.42 (n = 5) | 234.43 ± 35.47 (n = 5) | 0.149 | 226.85 ± 29.56 (n = 4) | 195.93 ± 18.87 (n = 4) | 0.117 |
| LSM (kPa) | 7.58 ± 3.97 (n = 11) | 6.67 ± 2.39 (n = 11) | 0.437 | 7.94 ± 5.22 (n = 5) | 6.89 ± 3.20 (n = 5) | 0.560 | 9.43 ± 5.09 (n = 4) | 8.57 ± 6.53 (n = 4) | 0.714 |
| TC (mmol/L) | 4.65 ± 1.01 (n = 70) | 4.58 ± 1.12 (n = 70) | 0.350 | 4.63 ± 0.84 (n = 38) | 4.49 ± 0.88 (n = 38) | 0.250 | 4.69 ± 0.83 (n = 13) | 4.75 ± 1.02 (n = 13) | 0.688 |
| TG (mmol/L) | 1.15 ± 0.70 (n = 70) | 1.03 ± 0.47 (n = 70) | 0.053 | 1.21 ± 0.83 (n = 38) | 1.14 ± 0.76 (n = 38) | 0.288 | 1.04 ± 0.38 (n = 13) | 0.84 ± 0.27 (n = 13) | 0.059 |
| LDL-c (mmol/L) | 2.84 ± 0.90 (n = 70) | 2.80 ± 1.04 (n = 70) | 0.601 | 2.78 ± 0.70 (n = 38) | 2.67 ± 0.80 (n = 38) | 0.287 | 2.83 ± 0.60 (n = 13) | 2.90 ± 0.80 (n = 13) | 0.434 |
| HDL-c (mmol/L) | 1.30 ± 0.33 (n = 70) | 1.31 ± 0.35 (n = 70) | 0.808 | 1.32 ± 0.37 (n = 38) | 1.31 ± 0.27 (n = 38) | 0.742 | 1.39 ± 0.38 (n = 13) | 1.45 ± 0.34 (n = 13) | 0.106 |
| ApoB (g/L) | 0.89 ± 0.24 (n = 70) | 0.88 ± 0.26 (n = 70) | 0.665 | 0.90 ± 0.18 (n = 38) | 0.88 ± 0.20 (n = 38) | 0.481 | 0.88 ± 0.16 (n = 13) | 0.90 ± 0.23 (n = 13) | 0.565 |
| non-HDL-c (mmol/L) | 3.35 ± 0.95 (n = 70) | 3.27 ± 1.10 (n = 70) | 0.292 | 3.31 ± 0.72 (n = 38) | 3.18 ± 0.77 (n = 38) | 0.220 | 3.30 ± 0.58 (n = 13) | 3.30 ± 0.80 (n = 13) | 0.972 |
| LIP (mmol/L) | 68.94 ± 62.60 (n = 11) | 64.62 ± 75.96 (n = 11) | 0.696 | 75.15 ± 67 (n = 8) | 60.49 ± 48.7 (n = 8) | 0.351 | 109.25 ± 44.48 (n = 2) | 90.90 ± 70.43 (n = 2) | 0.500 |
| FBG (mmol/L) | 4.72 ± 1.03 (n = 97) | 4.70 ± 1.93 (n = 97) | 0.886 | 4.71 ± 1.06 (n = 53) | 4.53 ± 0.77 (n = 53) | 0.172 | 4.61 ± 0.54 (n = 23) | 4.70 ± 0.84 (n = 23) | 0.533 |
| HbA1c (%) | 5.15 ± 0.50 (n = 2) | 5.20 ± 0.71 (n = 2) | 0.795 | / | / | / | / | / | / |
| FI (μU/mL) | 6.93 ± 3.84 (n = 38) | 6.91 ± 3.44 (n = 38) | 0.970 | 7.52 ± 3.82 (n = 14) | 9.37 ± 5.82 (n = 14) | 0.208 | 8.45 ± 5.08 (n = 6) | 6.49 ± 2.18 (n = 6) | 0.319 |
| HOMA-IR | 1.55 ± 0.95 (n = 37) | 1.60 ± 1.28 (n = 37) | 0.755 | 1.76 ± 1.07 (n = 14) | 2.16 ± 1.71 (n = 14) | 0.171 | 1.77 ± 1.22 (n = 6) | 1.33 ± 0.55 (n = 6) | 0.301 |
| SBP (mmHg) | 120.89 ± 12.93 (n = 114) | 118.92 ± 10.83 (n = 114) | 0.133 | 120.51 ± 13.75 (n = 65) | 120.18 ± 12.09 (n = 65) | 0.866 | 119.96 ± 10.72 (n = 24) | 119.58 ± 9.32 (n = 24) | 0.858 |
| DBP (mmHg) | 76.13 ± 9.4 (n = 114) | 75.7 ± 8.64 (n = 114) | 0.649 | 75.57 ± 9.35 (n = 65) | 75.11 ± 8.00 (n = 65) | 0.734 | 75.42 ± 7.18 (n = 24) | 75.67 ± 8.47 (n = 24) | 0.878 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, L.; Lin, Z.-H.; Lu, X.-J.; Hu, X.; Zhong, H.-J.; Lin, D.-J.; Liu, T.; Xu, J.-T.; Lin, W.-Y.; Wu, Q.-P.; et al. Washed Microbiota Transplantation Improves Patients with Overweight by the Gut Microbiota and Sphingolipid Metabolism. Biomedicines 2023, 11, 2415. https://doi.org/10.3390/biomedicines11092415
Wu L, Lin Z-H, Lu X-J, Hu X, Zhong H-J, Lin D-J, Liu T, Xu J-T, Lin W-Y, Wu Q-P, et al. Washed Microbiota Transplantation Improves Patients with Overweight by the Gut Microbiota and Sphingolipid Metabolism. Biomedicines. 2023; 11(9):2415. https://doi.org/10.3390/biomedicines11092415
Chicago/Turabian StyleWu, Lei, Zi-Han Lin, Xin-Jian Lu, Xuan Hu, Hao-Jie Zhong, De-Jiang Lin, Tao Liu, Jia-Ting Xu, Wen-Ying Lin, Qing-Ping Wu, and et al. 2023. "Washed Microbiota Transplantation Improves Patients with Overweight by the Gut Microbiota and Sphingolipid Metabolism" Biomedicines 11, no. 9: 2415. https://doi.org/10.3390/biomedicines11092415