
Iron Status and Short-Term Recovery after Non-Severe Acute Myocarditis: A Prospective Observational Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Population
2.2. Study Scheme
2.3. Basic Clinical Evaluation
2.4. Laboratory Parameters
2.5. Echocardiography
2.6. Other Diagnostic Procedures
- −
- coronary angiography or coronary computed tomographic angiography—to exclude obstructive coronary artery disease;
- −
- cardiac magnetic resonance—in search for the indices of MCD, to confirm the diagnosis.
2.7. Statistical Analyses
3. Results
3.1. Patients Characteristics
- −
- 3 with normal level of high sensitivity cardiac troponin I;
- −
- 18 without indices of MCD in cardiac magnetic resonance.
3.2. Clinical Manifestation of MCD
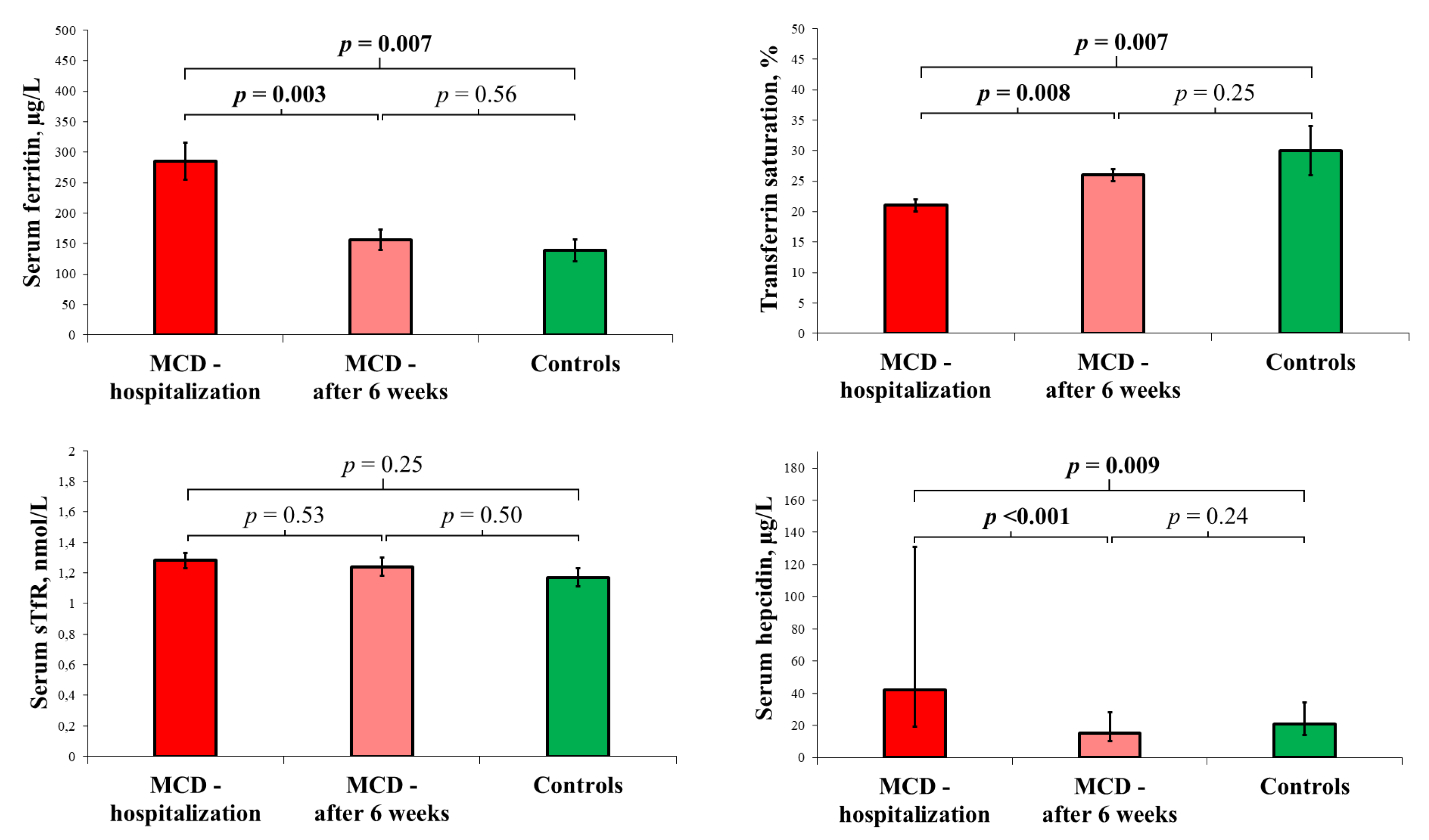
3.3. Follow-Up Visit
3.4. Relationship of Neurohormonal Activation, Cardiomyocyte Necrosis, Inflammatory Response, and Cardiac Dysfunction with In-Hospital Iron Status
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Caforio, A.L.P.; Cooper, L.T.; Felix, S.B.; Hare, J.M.; Heidecker, B.; Heymans, S.; Hübner, N.; et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2021, 18, 169–193. [Google Scholar] [CrossRef]
- Sagar, S.; Liu, P.P.; Cooper, L.T., Jr. Myocarditis. Lancet 2012, 379, 738–747. [Google Scholar] [CrossRef] [Green Version]
- Kindermann, I.; Barth, C.; Mahfoud, F.; Ukena, C.; Lenski, M.; Yilmaz, A.; Klingel, K.; Kandolf, R.; Sechtem, U.; Cooper, L.T.; et al. Update on Myocarditis. Am. Coll. Cardiol. 2012, 59, 779–792. [Google Scholar] [CrossRef]
- Anzini, M.; Merlo, M.; Sabbadini, G.; Barbati, G.; Finocchiaro, G.; Pinamonti, B.; Salvi, A.; Perkan, A.; Di Lenarda, A.; Bussani, R.; et al. Long-term evolution and prognostic stratification of biopsy-proven active myocarditis. Circulation 2013, 128, 2384–2394. [Google Scholar] [CrossRef] [Green Version]
- Kindermann, I.; Kindermann, M.; Kandolf, R.; Klingel, K.; Bültmann, B.; Müller, T.; Lindinger, A.; Böhm, M. Predictors of outcome in patients with suspected myocarditis. Circulation 2008, 118, 639–648. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, A.; Ferreira, V.; Antunes, M.M.; Lousinha, A.; Pereira-da-Silva, T.; Antunes, D.; Cunha, P.S.; Oliveira, M.; Ferreira, R.C.; Rosa, S.A. Dilated Cardiomyopathy: A Comprehensive Approach to Diagnosis and Risk Stratification. Biomedicines 2023, 11, 834. [Google Scholar] [CrossRef]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef]
- Sawicki, K.T.; De Jesus, A.; Ardehali, H. Iron Metabolism in Cardiovascular Disease: Physiology, Mechanisms, and Therapeutic Targets. Circ. Res. 2023, 132, 379–396. [Google Scholar] [CrossRef]
- Zhang, H.; Zhabyeyev, P.; Wang, S.; Oudit, G.Y. Role of iron metabolism in heart failure: From iron deficiency to iron overload. Biochim. Biophys. Acta Mol. Basis. Dis. 2019, 1865, 1925–1937. [Google Scholar] [CrossRef]
- Murphy, C.J.; Oudit, G.Y. Iron-overload cardiomyopathy: Pathophysiology, diagnosis, and treatment. J. Card. Fail. 2010, 16, 888–900. [Google Scholar] [CrossRef]
- Hoes, M.F.; Grote Beverborg, N.; Kijlstra, J.D.; Kuipers, J.; Swinkels, D.W.; Giepmans, B.N.G.; Rodenburg, R.J.; van Veldhuisen, D.J.; de Boer, R.A.; van der Meer, P. Iron deficiency impairs contractility of human cardiomyocytes through decreased mitochondrial function. Eur. J. Heart Fail. 2018, 20, 910–919. [Google Scholar] [CrossRef] [Green Version]
- Anand, I.S.; Gupta, P. Anemia and Iron Deficiency in Heart Failure: Current Concepts and Emerging Therapies. Circulation 2018, 138, 80–98. [Google Scholar] [CrossRef]
- Zhang, H.; Jamieson, K.L.; Grenier, J.; Nikhanj, A.; Tang, Z.; Wang, F.; Wang, S.; Seidman, J.G.; Seidman, C.E.; Thompson, R.; et al. Myocardial Iron Deficiency and Mitochondrial Dysfunction in Advanced Heart Failure in Humans. J. Am. Heart Assoc. 2022, 11, e022853. [Google Scholar] [CrossRef]
- Fratta Pasini, A.M.; Stranieri, C.; Busti, F.; Di Leo, E.G.; Girelli, D.; Cominacini, L. New Insights into the Role of Ferroptosis in Cardiovascular Diseases. Cells 2023, 12, 867. [Google Scholar] [CrossRef]
- Gordan, R.; Wongjaikam, S.; Gwathmey, J.K.; Chattipakorn, N.; Chattipakorn, S.C.; Xie, L.H. Involvement of cytosolic and mitochondrial iron in iron overload cardiomyopathy: An update. Heart Fail. Rev. 2018, 23, 801–816. [Google Scholar] [CrossRef]
- Beard, J.L. Iron biology in immune function, muscle metabolism and neuronal functioning. J. Nutr. 2001, 131, 568S–579S. [Google Scholar] [CrossRef] [Green Version]
- Mu, Q.; Chen, L.; Gao, X.; Shen, S.; Sheng, W.; Min, J.; Wang, F. The role of iron homeostasis in remodeling immune function and regulating inflammatory disease. Sci. Bull. 2021, 66, 1806–1816. [Google Scholar] [CrossRef]
- Ni, S.; Yuan, Y.; Kuang, Y.; Li, X. Iron Metabolism and Immune Regulation. Front. Immunol. 2022, 13, 816282. [Google Scholar] [CrossRef]
- Haschka, D.; Hoffmann, A.; Weiss, G. Iron in immune cell function and host defense. Semin. Cell Dev. Biol. 2021, 115, 27–36. [Google Scholar] [CrossRef]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef]
- Kunireddy, N.; Jacob, R.; Khan, S.A.; Yadagiri, B.; Sai Baba, K.S.S.; Rajendra Vara Prasad, I.; Mohan, I.K. Hepcidin and Ferritin: Important Mediators in Inflammation Associated Anemia in Systemic Lupus Erythematosus Patients. Indian J. Clin. Biochem. 2018, 33, 406–413. [Google Scholar] [CrossRef]
- Wang, W.; Knovich, M.A.; Coffman, L.G.; Torti, F.M.; Torti, S.V. Serum ferritin: Past, present and future. Biochim. Biophys. Acta 2010, 1800, 760–769. [Google Scholar] [CrossRef] [Green Version]
- Nemeth, E.; Valore, E.V.; Territo, M.; Schiller, G.; Lichtenstein, A.; Ganz, T. Hepcidin, a putative mediator of anemia of inflammation, is a type II acute-phase protein. Blood 2003, 101, 2461–2463. [Google Scholar] [CrossRef] [Green Version]
- Hortová-Kohoutková, M.; Skotáková, M.; Onyango, I.G.; Slezáková, M.; Panovský, R.; Opatřil, L.; Slanina, P.; De Zuani, M.; Mrkva, O.; Andrejčinová, I.; et al. Hepcidin and ferritin levels as markers of immune cell activation during septic shock, severe COVID-19 and sterile inflammation. Front. Immunol. 2023, 14, 1110540. [Google Scholar] [CrossRef]
- Nemeth, E.; Ganz, T. The role of hepcidin in iron metabolism. Acta Haematol. 2009, 122, 78–86. [Google Scholar] [CrossRef] [Green Version]
- Fertrin, K.Y. Diagnosis and management of iron deficiency in chronic inflammatory conditions (CIC): Is too little iron making your patient sick? Hematol. Am. Soc. Hematol. Educ. Program 2020, 2020, 478–486. [Google Scholar] [CrossRef]
- Muñoz, M.; García-Erce, J.A.; Remacha, A.F. Disorders of iron metabolism. Part 1: Molecular basis of iron homoeostasis. J. Clin. Pathol. 2011, 64, 281–286. [Google Scholar] [CrossRef]
- Peters, H.P.; Rumjon, A.; Bansal, S.S.; Laarakkers, C.M.; van den Brand, J.A.; Sarafidis, P.; Musto, R.; Malyszko, J.; Swinkels, D.W.; Wetzels, J.F.; et al. Intra-individual variability of serum hepcidin-25 in haemodialysis patients using mass spectrometry and ELISA. Nephrol. Dial. Transplant. 2012, 27, 3923–3929. [Google Scholar] [CrossRef] [Green Version]
- Kozłowska, B.; Sochanowicz, B.; Kraj, L.; Palusińska, M.; Kołsut, P.; Szymański, Ł.; Lewicki, S.; Kruszewski, M.; Załęska-Kocięcka, M.; Leszek, P. Clinical and Molecular Aspects of Iron Metabolism in Failing Myocytes. Life 2022, 12, 1203. [Google Scholar] [CrossRef]
- Blayney, L.; Bailey-Wood, R.; Jacobs, A.; Henderson, A.; Muir, J. The effects of iron deficiency on the respiratory function and cytochrome content of rat heart mitochondria. Circ. Res. 1976, 39, 744–748. [Google Scholar] [CrossRef]
- Kasztura, M.; Dzięgała, M.; Kobak, K.; Bania, J.; Mazur, G.; Banasiak, W.; Ponikowski, P.; Jankowska, E.A. Both iron excess and iron depletion impair viability of rat H9C2 cardiomyocytes and L6G8C5 myocytes. Kardiol. Pol. 2017, 75, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Dziegala, M.; Kasztura, M.; Kobak, K.; Bania, J.; Banasiak, W.; Ponikowski, P.; Jankowska, E.A. Influence of the availability of iron during hypoxia on the genes associated with apoptotic activity and local iron metabolism in rat H9C2 cardiomyocytes and L6G8C5 skeletal myocytes. Mol. Med. Rep. 2016, 14, 3969–3977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massaiu, I.; Campodonico, J.; Mapelli, M.; Salvioni, E.; Valerio, V.; Moschetta, D.; Myasoedova, V.A.; Cappellini, M.D.; Pompilio, G.; Poggio, P.; et al. Dysregulation of Iron Metabolism-Linked Genes at Myocardial Tissue and Cell Levels in Dilated Cardiomyopathy. Int. J. Mol. Sci. 2023, 24, 2887. [Google Scholar] [CrossRef]
- Huang, Y.; Zhou, B. Mitochondrial Dysfunction in Cardiac Diseases and Therapeutic Strategies. Biomedicines 2023, 11, 1500. [Google Scholar]
- Chung, Y.J.; Luo, A.; Park, K.C.; Loonat, A.A.; Lakhal-Littleton, S.; Robbins, P.A.; Swietach, P. Iron-deficiency anemia reduces cardiac contraction by downregulating RyR2 channels and suppressing SERCA pump activity. JCI Insight 2019, 4, e125618. [Google Scholar] [CrossRef] [Green Version]
- Toblli, J.E.; Cao, G.; Rivas, C.; Giani, J.F.; Dominici, F.P. Intravenous iron sucrose reverses anemia-induced cardiac remodeling, prevents myocardial fibrosis, and improves cardiac function by attenuating oxidative/nitrosative stress and inflammation. Int. J. Cardiol. 2016, 212, 84–91. [Google Scholar] [CrossRef]
- Anker, S.D.; Khan, M.S.; Butler, J.; von Haehling, S.; Jankowska, E.A.; Ponikowski, P.; Friede, T. Effect of intravenous iron replacement on recurrent heart failure hospitalizations and cardiovascular mortality in patients with heart failure and iron deficiency: A Bayesian meta-analysis. Eur. J. Heart Fail. 2023, in press. [Google Scholar] [CrossRef]
- Reinhold, J.; Burra, V.; Corballis, N.; Tsampasian, V.; Matthews, G.; Papadopoulou, C.; Vassiliou, V.S. Effects of Intravenous Iron Replacement Therapy on Cardiovascular Outcomes in Patients with Heart Failure: A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2023, 10, 116. [Google Scholar] [CrossRef]
- Ponikowski, P.; Kirwan, B.A.; Anker, S.D.; McDonagh, T.; Dorobantu, M.; Drozdz, J.; Fabien, V.; Filippatos, G.; Göhring, U.M.; Keren, A.; et al. Ferric carboxymaltose for iron deficiency at discharge after acute heart failure: A multicentre, double-blind, randomised, controlled trial. Lancet 2020, 396, 1895–1904. [Google Scholar] [CrossRef] [PubMed]
- Maeder, M.T.; Khammy, O.; dos Remedios, C.; Kaye, D.M. Myocardial and systemic iron depletion in heart failure implications for anemia accompanying heart failure. J. Am. Coll. Cardiol. 2011, 58, 474–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leszek, P.; Sochanowicz, B.; Szperl, M.; Kolsut, P.; Brzóska, K.; Piotrowski, W.; Rywik, T.M.; Danko, B.; Polkowska-Motrenko, H.; Różański, J.M.; et al. Myocardial iron homeostasis in advanced chronic heart failure patients. Int. J. Cardiol. 2012, 159, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Melenovsky, V.; Petrak, J.; Mracek, T.; Benes, J.; Borlaug, B.A.; Nuskova, H.; Pluhacek, T.; Spatenka, J.; Kovalcikova, J.; Drahota, Z.; et al. Myocardial iron content and mitochondrial function in human heart failure: A direct tissue analysis. Eur. J. Heart Fail. 2017, 19, 522–530. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All Diagnostic Criteria for Acute Myocarditis Must Have Been Met: |
|---|
| (1) new onset symptoms suggestive of myocarditis (shortness of breath, effort intolerance, fatigue, palpitations, or chest pain), |
| (2) elevated high sensitivity cardiac troponin I, |
| (3) exclusion of obstructive coronary artery disease in coronary angiography or coronary computed tomographic angiography, |
| (4) features suggestive of myocarditis in cardiac magnetic resonance, and |
| (5) age ≥ 18 years. |
| Variables, Units | MCD Patients (n = 42) | Control Group (n = 15) | p-Value |
|---|---|---|---|
| Age, year | 32 (1) | 31 (1) | 0.66 |
| Male gender, yes | 41 (97%) | 13 (87%) | 0.10 |
| Smoking, packet-year | 0.2 (0.0–6.5) | 0.0 (0.0–0.0) | 0.20 |
| Alcohol, g per week | 90 (25–155) | 25 (25–50) | 0.01 |
| SBP on admission, mmHg | 135 (3) | 118 (3) | 0.003 |
| DBP on admission, mmHg | 80 (3) | 77 (3) | 0.62 |
| HR on admission, mmHg | 86 (3) | 73 (4) | 0.02 |
| Basic laboratory parameters (cardiology department) | |||
| Serum hemoglobin, g/dL | 15.0 (0.2) | 15.2 (0.3) | 0.59 |
| Red blood cell count, 106/µL | 5.0 (0.1) | 5.0 (0.1) | 0.65 |
| White blood cell count, 103/µL | 7.9 (0.4) | 6.3 (0.4) | 0.03 |
| Neutrophil count, 103/µL | 5.0 (0.3) | 3.2 (0.3) | 0.004 |
| Lymphocyte count, 103/µL | 2.0 (0.1) | 2.3 (0.2) | 0.19 |
| Monocyte count, 103/µL | 0.7 (0.1) | 0.4 (0.1) | 0.008 |
| Neutrophil-to-lymphocyte ratio | 2.3 (1.9–3.0) | 1.2 (1.1–1.9) | <0.001 |
| Reticulocyte hemoglobin content, pg | 30 (3) | 37 (5) | 0.03 |
| Reticulocytes, % | 0.98 (0.82–1.30) | 1.26 (1.06–1.56) | 0.60 |
| C-reactive protein, mg/L | 54 (5) | 3 (0) | <0.001 |
| NT-proBNP, pg/mL | 340 (185–594) | 31 (18–46) | <0.001 |
| Hs-cTnI, µg/L | 2.44 (0.53–6.33) | 0.01 (0.01–0.01) | <0.001 |
| Serum creatinine, mg/dL | 0.91 (0.02) | 0.98 (0.03) | 0.11 |
| ALT, U/L | 38 (27–48) | 20 (13–30) | <0.001 |
| Serum insulin, uIU/mL | 13.4 (1.1) | 7.9 (1.3) | 0.01 |
| TSH, mIU/L | 2.0 (0.2) | 2.7 (0.3) | 0.07 |
| Iron status indices | |||
| Serum iron, µg/dL | 70 (5) | 101 (12) | 0.006 |
| Serum ferritin, µg/L | 285 (30) | 139 (18) | 0.007 |
| TSAT, % | 21 (1) | 30 (4) | 0.007 |
| sTfR, nmol/L | 1.28 (0.05) | 1.17 (0.06) | 0.25 |
| Serum hepcidin, µg/L | 44 (24–131) | 21 (13–44) | 0.009 |
| Transthoracic echocardiography | |||
| LVEF, % | 56 (1) | 63 (1) | 0.01 |
| TAPSE, mm | 21 (1) | 23 (1) | 0.045 |
| Cardiology Department | ||||||
|---|---|---|---|---|---|---|
| Variables #, Units | NT-proBNP, 1 ln pg/mL | Hs-cTnI, 1 ln µg/L | CRP, 1 ln mg/L | LVEF, 1% | LV GLS, 1 | TAPSE, 1 mm |
| Serum iron, 1 µg/dL | −0.345 * | −0.086 | −0.315 * | 0.169 | −0.029 | 0.037 |
| Serum ferritin, 1 µg/L | 0.093 | 0.155 | 0.309 * | 0.019 | −0.135 | 0.167 |
| TSAT, 1% | −0.319 * | 0.018 | −0.281 | 0.223 | −0.093 | 0.122 |
| sTfR, 1 nmol/L | −0.101 | 0.094 | 0.052 | −0.020 | 0.235 | −0.101 |
| Serum hepcidin, 1 ln µg/L | 0.283 | 0.095 | 0.308 * | −0.113 | −0.196 | 0.229 |
| NT-proBNP, 1 ln pg/mL | X | −0.022 | 0.166 | −0.614 *** | 0.111 | −0.031 |
| Hs-TnI, 1 ln µg/L | −0.022 | X | 0.245 | 0.082 | 0.188 | 0.078 |
| CRP, 1 ln mg/L | 0.166 | 0.245 | X | −0.029 | 0.040 | −0.173 |
| Baseline | 6 Weeks after Hospital Discharge | |||||
|---|---|---|---|---|---|---|
| Variables, Units | NT-proBNP, 1 ln pg/mL | hs-cTnI, 1 ln µg/L | CRP, 1 ln mg/L | LVEF, 1% | LV GLS, 1 | TAPSE, 1 mm |
| Serum iron, 1 µg/dL | −0.012 | −0.014 | −0.067 | 0.388 * | −0.392 * | 0.327 |
| Serum ferritin, 1 µg/L | −0.104 | −0.020 | 0.325 | 0.134 | −0.279 | 0.126 |
| TSAT, 1% | 0.031 | 0.037 | −0.104 | 0.391 * | −0.408 * | 0.285 |
| sTfR, 1 nmol/L | −0.013 | 0.219 | −0.213 | −0.209 | 0.241 | 0.067 |
| Serum hepcidin, 1 ln µg/L | −0.263 | −0.034 | 0.110 | 0.179 | 0.073 | 0.142 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franczuk, P.; Tkaczyszyn, M.; Kosiorek, A.; Kulej-Łyko, K.; Kobak, K.A.; Kasztura, M.; Sołtowska, A.; Jaroch, J.; Ponikowski, P.; Jankowska, E.A. Iron Status and Short-Term Recovery after Non-Severe Acute Myocarditis: A Prospective Observational Study. Biomedicines 2023, 11, 2136. https://doi.org/10.3390/biomedicines11082136
Franczuk P, Tkaczyszyn M, Kosiorek A, Kulej-Łyko K, Kobak KA, Kasztura M, Sołtowska A, Jaroch J, Ponikowski P, Jankowska EA. Iron Status and Short-Term Recovery after Non-Severe Acute Myocarditis: A Prospective Observational Study. Biomedicines. 2023; 11(8):2136. https://doi.org/10.3390/biomedicines11082136
Chicago/Turabian StyleFranczuk, Paweł, Michał Tkaczyszyn, Aneta Kosiorek, Katarzyna Kulej-Łyko, Kamil Aleksander Kobak, Monika Kasztura, Alicja Sołtowska, Joanna Jaroch, Piotr Ponikowski, and Ewa Anita Jankowska. 2023. "Iron Status and Short-Term Recovery after Non-Severe Acute Myocarditis: A Prospective Observational Study" Biomedicines 11, no. 8: 2136. https://doi.org/10.3390/biomedicines11082136