
Effect of Silver Diamine Fluoride on Bacterial Biofilms—A Review including In Vitro and In Vivo Studies

 and
and
Abstract
:1. Introduction
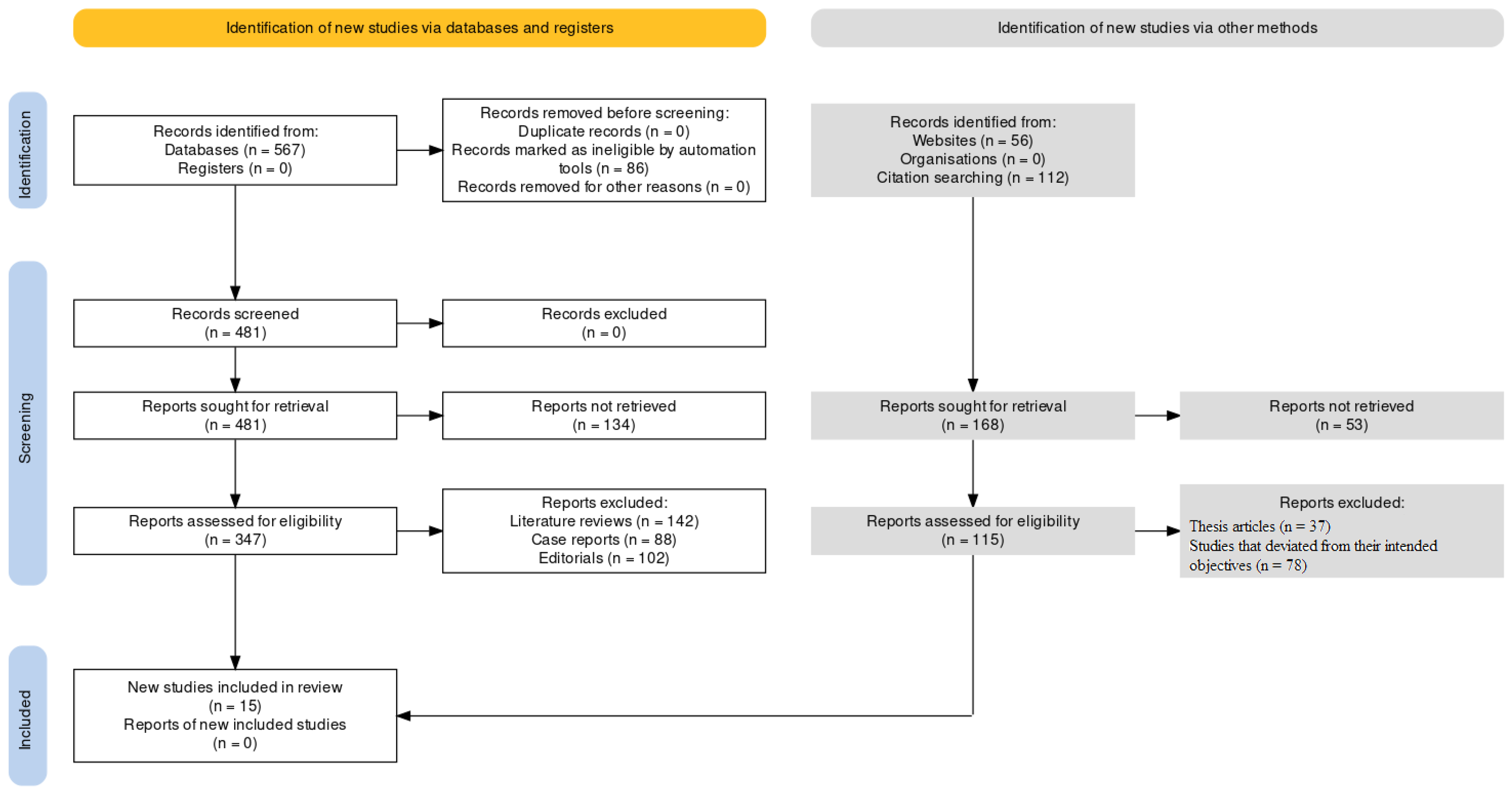
2. Materials and Methods
2.1. Eligibility Criteria
- (P)
- Participants in this systematic review are patients with bacterial biofilms. To include all relevant studies, the Boolean operator “OR” was used to combine different keywords related to bacterial biofilms, such as “biofilm”, “plaque” and “microbial colonies”.
- (I)
- The intervention consisted of Silver Diamine Fluoride (SDF). To ensure that all relevant studies on SDF were included in the review, the Boolean operator “OR” was used to combine different variations of the keyword, such as “silver diamine fluoride” or “AgF”.
- (C)
- The comparison consisted of control groups that compared SDF to other chemical compounds. To identify studies that compare SDF to other biomarkers/control groups, the Boolean operator “AND” was used to combine the intervention and comparison groups that were considered as interventions.
- (O)
- The outcome measures the effect of SDF on bacterial biofilms. To identify studies that measure the effect of SDF on bacterial biofilms, the Boolean operator “AND” was used to combine the intervention and outcome keywords.
2.2. Search Strategy
2.3. Data Extraction
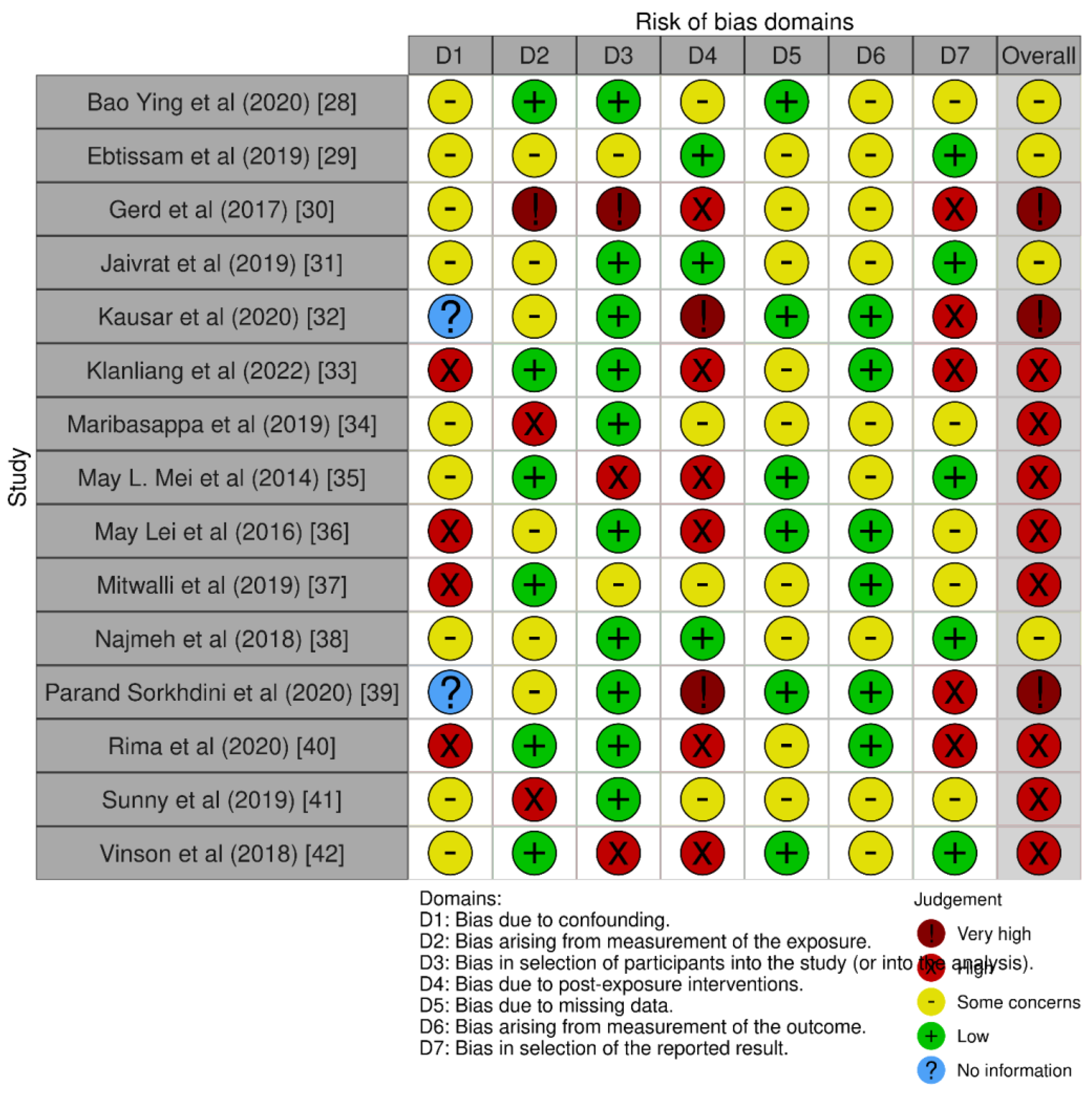
2.4. Quality Assessment
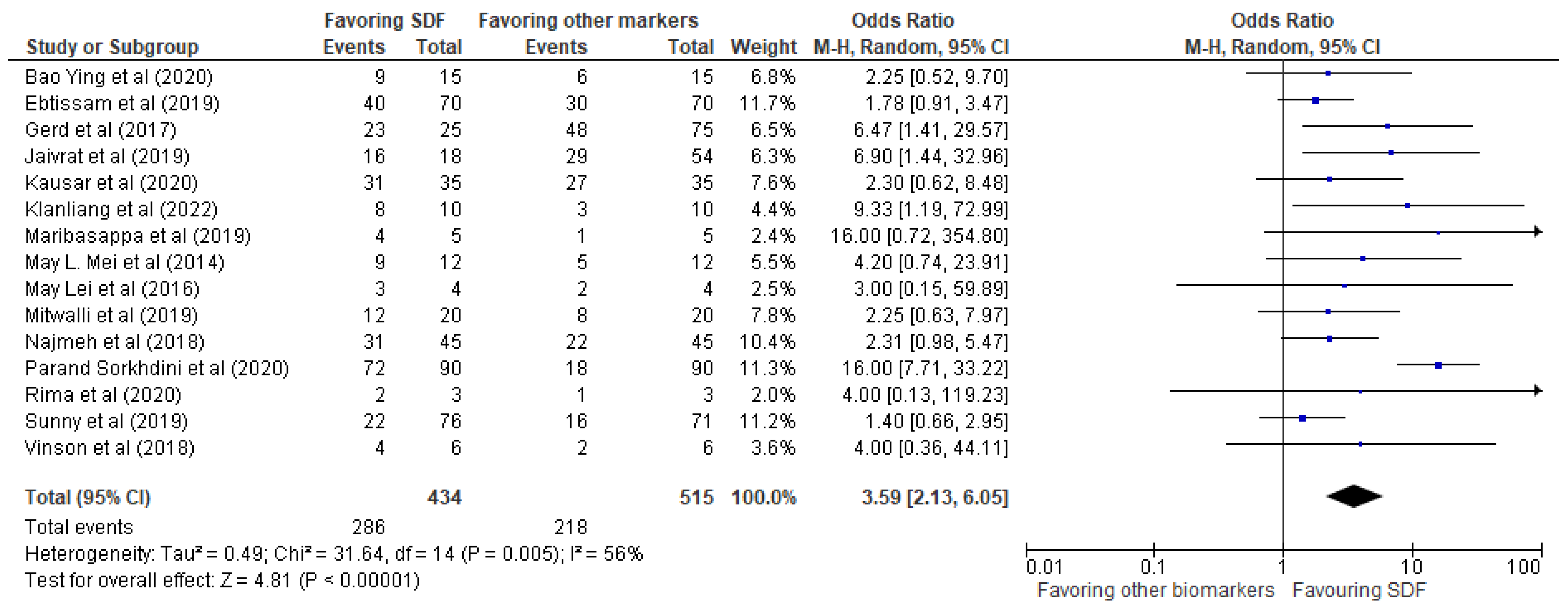
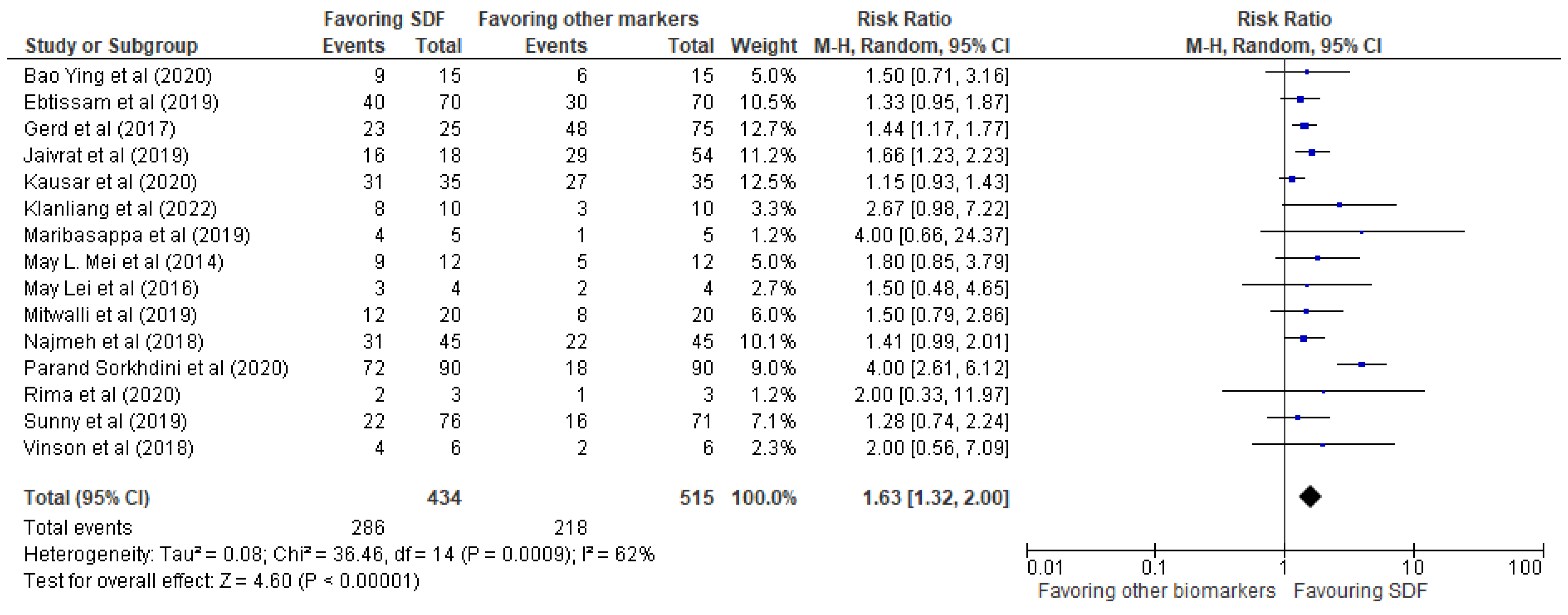
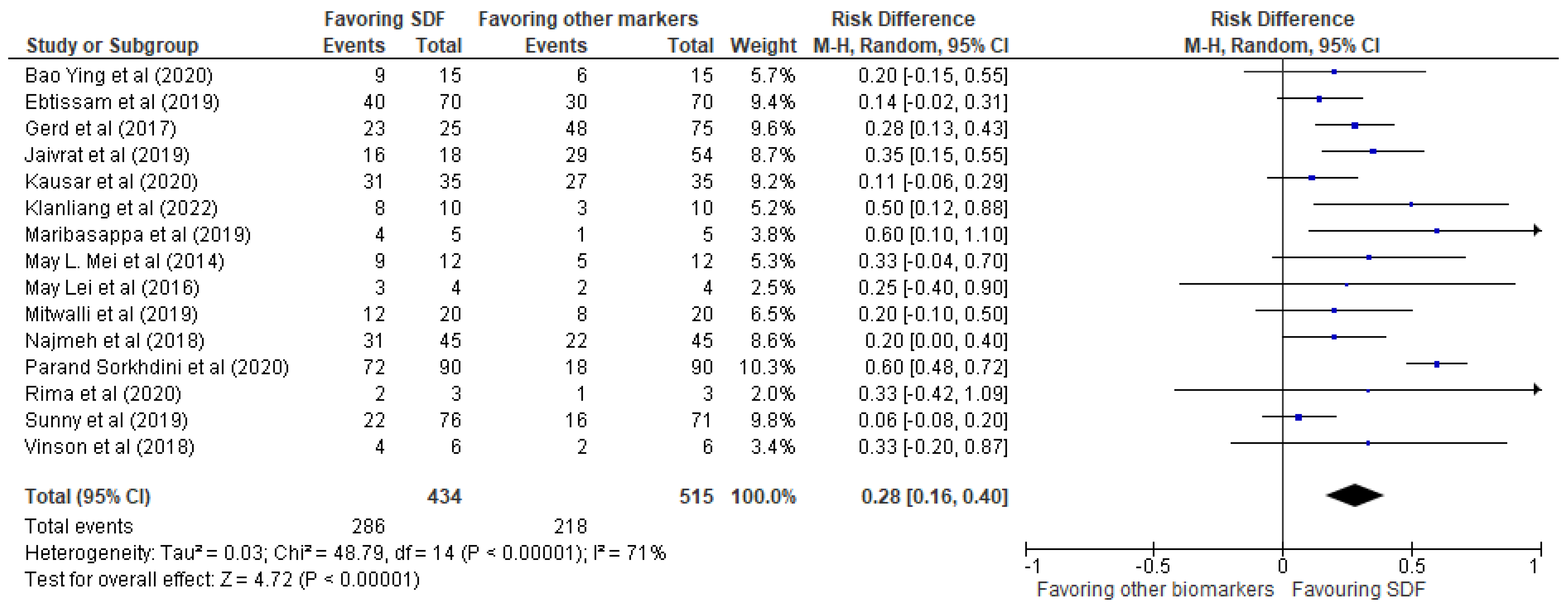
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SDF | Silver diamine fluoride |
| CHX | Chlorhexidine |
| HA | Hydroxyapatite |
| SDF-KI | Silver diamine fluoride + Potassium iodide |
| AgNPs | Silver nanoparticles |
| DW | Deionized water |
| PAA | Polyacrylic acid (PAA) |
References
- Marsh, P.D.; Moter, A.; Devine, D.A. Dental plaque biofilms: Communities, conflict and control. Periodontol. 2000 2011, 55, 16–35. [Google Scholar] [CrossRef]
- Maiorana, C.; Beretta, M.; Grossi, G.B.; Santoro, F.; Herford, A.S.; Nagursky, H.; Cicciù, M. Histomorphometric Evaluation of Anorganic Bovine Bone Coverage to Reduce Autogenous Grafts Resorption: Preliminary Results. Open Dent. J. 2011, 5, 71–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rengo, C.; Spagnuolo, G.; Ametrano, G.; Juloski, J.; Rengo, S.; Ferrari, M. Micro-Computerized Tomographic Analysis of Premolars Restored with Oval and Circular Posts. Clin. Oral Investig. 2014, 18, 571–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicciù, M.; Herford, A.S.; Stoffella, E.; Cervino, G.; Cicciù, D. Protein-Signaled Guided Bone Regeneration Using Titanium Mesh and Rh-BMP2 in Oral Surgery: A Case Report Involving Left Mandibular Reconstruction after Tumor Resection. Open Dent. J. 2012, 6, 51–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosaddad, S.A.; Tahmasebi, E.; Yazdanian, A.; Rezvani, M.B.; Seifalian, A.; Yazdanian, M.; Tebyanian, H. Oral microbial biofilms: An update. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 2005–2019. [Google Scholar] [CrossRef] [PubMed]
- Mira, A.; Simon-Soro, A.; Curtis, M.A. Role of microbial communities in the pathogenesis of periodontal diseases and caries. J. Clin. Periodontol. 2017, 44, S23–S38. [Google Scholar] [CrossRef] [Green Version]
- Marsh, P.D. Are dental diseases examples of ecological catastrophes? Microbiology 2003, 149, 279–294. [Google Scholar] [CrossRef]
- Marsh, P.D. Dental plaque as a biofilm and a microbial community—Implications for health and disease. BMC Oral Health 2006, 6, S14. [Google Scholar] [CrossRef] [Green Version]
- Marimallappa, T.R.; Pal, S.; Ashok, K.K.R.; Bhat, P.; Raghupathy, R.K. Acomparative microbiological study of polyglycolic acid and silk sutures in oral surgical procedures. Minerva Dent. Oral Sci. 2021, 70, 239–247. [Google Scholar]
- Bowen, W.H.; Burne, R.A.; Wu, H.; Koo, H. Oral Biofilms: Pathogens, Matrix, and Polymicrobial Interactions in Microenvironments. Trends Microbiol. 2018, 26, 229–242. [Google Scholar] [CrossRef]
- Takahashi, N.; Nyvad, B. Ecological Hypothesis of Dentin and Root Caries. Caries Res. 2016, 50, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Gati, D.; Vieira, A.R. Elderly at Greater Risk for Root Caries: A Look at the Multifactorial Risks with Emphasis on Genetics Susceptibility. Int. J. Dent. 2011, 2011, 647168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steele, J.G.; Sheiham, A.; Marcenes, W.; Fay, N.; Walls, A.W.G. Clinical and behavioural risk indicators for root caries in older people. Gerodontology 2001, 18, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Uccioli, U.; Fonzar, A.; Lanzuolo, S.; Meloni, S.M.; Lumbau, A.I.; Cicciù, M.; Tallarico, M. Tissue Recession around a Dental Implant in Anterior Maxilla: How to Manage Soft Tissue When Things Go Wrong? Prosthesis 2021, 3, 209–220. [Google Scholar] [CrossRef]
- Kleinberg, I. A mixed-bacteria ecological approach to understanding the role of the oral bacteria in dental caries causation: An alternative to Streptococcus mutans and the specific-plaque hypothesis. Crit. Rev. Oral Biol. Med. 2002, 13, 108–125. [Google Scholar] [CrossRef] [PubMed]
- Tanzer, J.M.; Livingston, J.; Thompson, A.M. The Microbiology of Primary Dental Caries in Humans. J. Dent. Educ. 2001, 65, 1028–1037. [Google Scholar] [CrossRef] [PubMed]
- Femiano, F.; Femiano, R.; Femiano, L.; Nucci, L.; Minervini, G.; Antonelli, A.; Bennardo, F.; Barone, S.; Scotti, N.; Sorice, V.; et al. A New Combined Protocol to Treat the Dentin Hypersensitivity Associated with Non-Carious Cervical Lesions: A Randomized Controlled Trial. Appl. Sci. 2020, 11, 187. [Google Scholar] [CrossRef]
- Hamada, S.; Slade, H.D. Biology, immunology, and cariogenicity of Streptococcus mutans. Microbiol. Rev. 1980, 44, 331–384. [Google Scholar] [CrossRef]
- Loesche, W.J. Role of Streptococcus mutans in human dental decay. Microbiol. Rev. 1986, 50, 353–380. [Google Scholar] [CrossRef]
- Peng, J.-Y.; Tsoi, J.K.H.; Matinlinna, J.P.; Botelho, M.G. Silver deposition on demineralized dentine surface dosed by silver diammine fluoride with different saliva. J. Investig. Clin. Dent. 2019, 10, e12382. [Google Scholar] [CrossRef] [Green Version]
- Chu, C.H.; Lo, E.C.M.; Lin, H.C. Effectiveness of Silver Diamine Fluoride and Sodium Fluoride Varnish in Arresting Dentin Caries in Chinese Pre-school Children. J. Dent. Res. 2002, 81, 767–770. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.-H.; Lee, A.H.C.; Zheng, L.; Mei, M.L.; Chan, G.C.-F. Arresting rampant dental caries with silver diamine fluoride in a young teenager suffering from chronic oral graft versus host disease post-bone marrow transplantation: A case report. BMC Res. Notes 2014, 7, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amenta, F.; Battineni, G.; Kalyan, L.; Reddy, V.; Madithati, P.; Reddy Narapureddy, B. Personalized Medicine Perception about Health Applications (Apps) in Smartphones towards Telemedicine during COVID-19: A Cross-Sectional Study. J. Pers. Med. 2022, 12, 12. [Google Scholar]
- Fiori, A.; Minervini, G.; Nucci, L.; d’Apuzzo, F.; Perillo, L.; Grassia, V. Predictability of crowding resolution in clear aligner treatment. Prog. Orthod. 2022, 23, 43. [Google Scholar] [CrossRef]
- Hendre, A.D.; Taylor, G.W.; Chávez, E.M.; Hyde, S. A systematic review of silver diamine fluoride: Effectiveness and application in older adults. Gerodontology 2017, 34, 411–419. [Google Scholar] [CrossRef]
- Tan, H.P.; Lo, E.C.M.; Dyson, J.E.; Luo, Y.; Corbet, E.F. A Randomized Trial on Root Caries Prevention in Elders. J. Dent. Res. 2010, 89, 1086–1090. [Google Scholar] [CrossRef]
- Knight, G.M.; McIntyre, J.M.; Craig, G.G.; Mulyani Zilm, P.S.; Gully, N.J. Inability to form a biofilm of Streptococcus mutans on silver fluoride—And potassium iodide-treated demineralized dentin. Quintessence Int. 2009, 40, 155–161. [Google Scholar] [PubMed]
- Mei, M.L.; Ito, L.; Cao, Y.; Li, Q.L.; Lo, E.C.M.; Chu, C.H. Inhibitory effect of silver diamine fluoride on dentine demineralisation and collagen degradation. J. Dent. 2013, 41, 809–817. [Google Scholar] [CrossRef]
- Chu, C.H.; Mei, L.E.I.; Seneviratne, C.J.; Lo, E.C.M. Effects of silver diamine fluoride on dentine carious lesions induced by Streptococcus mutans and Actinomyces naeslundii biofilms. Int. J. Paediatr. Dent. 2012, 22, 2–10. [Google Scholar] [CrossRef]
- Mei, M.L.; Nudelman, F.; Marzec, B.; Walker, J.M.; Lo, E.C.M.; Walls, A.W.; Chu, C.H. Formation of Fluorohydroxyapatite with Silver Diamine Fluoride. J. Dent. Res. 2017, 96, 1122–1128. [Google Scholar] [CrossRef] [Green Version]
- Knight, G.; McIntyre, J.; Craig, G.; Mulyani Zilm, P.; Gully, N. An in vitro model to measure the effect of a silver fluoride and potassium iodide treatment on the permeability of demineralized dentine to Streptococcus mutans. Aust. Dent. J. 2005, 50, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Mei, M.L.; Li, Q.; Chu, C.-H.; Lo, E.-M.; Samaranayake, L.P. Antibacterial effects of silver diamine fluoride on multi-species cariogenic biofilm on caries. Ann. Clin. Microbiol. Antimicrob. 2013, 12, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mei, M.L.; Chu, C.H.; Low, K.H.; Che, C.M.; Lo, E.C.M. Caries arresting effect of silver diamine fluoride on dentine carious lesion with S. mutans and L. acidophilus dual-species cariogenic biofilm. Med. Oral Patol. Oral Cir. Bucal. 2013, 18, e824–e831. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Mehta, V.; Fiorillo, L.; Badnjević, A.; Cervino, G.; Cicciù, M. The Association between COVID-19 Related Anxiety, Stress, Depression, Temporomandibular Disorders, and Headaches from Childhood to Adulthood: A Systematic Review. Brain Sci 2023, 13, 481. [Google Scholar] [CrossRef]
- Qamar, Z.; Alghamdi, A.M.S.; Bin Haydarah, N.K.; Balateef, A.A.; Alamoudi, A.A.; Abumismar, M.A.; Shivakumar, S.; Cicciù, M.; Minervini, G. Impact of Temporomandibular Disorders on Oral Health Related Quality of Life: A Systematic Review and Meta-analysis. J. Oral Rehabil. 2023. [Google Scholar] [CrossRef]
- Watson, P.S.; Pontefract, H.A.; Devine, D.A.; Shore, R.C.; Nattress, B.R.; Kirkham, J.; Robinson, C. Penetration of Fluoride into Natural Plaque Biofilms. J. Dent. Res. 2005, 84, 451–455. [Google Scholar] [CrossRef]
- Prada-López, I.; Quintas, V.; Vilaboa, C.; Suárez-Quintanilla, D.; Tomás, I. Devices for In situ Development of Non-disturbed Oral Biofilm. A Systematic Review. Front Microbiol. 2016, 7, 1055. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.-Y.; Liu, J.; Zhang, D.; Yang, Z.-L.; Feng, Y.-P.; Wang, M. Effect of silver diammine fluoride on micro-ecology of plaque from extensive caries of deciduous teeth—In vitro study. BMC Oral Health 2020, 20, 151. [Google Scholar] [CrossRef]
- Al-Madi, E.M.; Al-Jamie, M.A.; Al-Owaid, N.M.; Almohaimede, A.A.; Al-Owid, A.M. Antibacterial efficacy of silver diamine fluoride as a root canal irrigant. Clin. Exp. Dent. Res. 2019, 5, 551–556. [Google Scholar] [CrossRef] [Green Version]
- Göstemeyer, G.; Schulze, F.; Paris, S.; Schwendicke, F. Arrest of Root Carious Lesions via Sodium Fluoride, Chlorhexidine and Silver Diamine Fluoride In Vitro. Materials 2017, 11, 9. [Google Scholar] [CrossRef] [Green Version]
- Gupta, J.; Thomas, M.; Radhakrishna, M.; Srikant, N.; Ginjupalli, K. Effect of silver diamine fluoride-potassium iodide and 2% chlorhexidine gluconate cavity cleansers on the bond strength and microleakage of resin-modified glass ionomer cement. J. Conserv. Dent. 2019, 22, 201. [Google Scholar] [PubMed]
- Fakhruddin, K.S.; Egusa, H.; Ngo, H.C.; Panduwawala, C.; Pesee, S.; Venkatachalam, T.; Samaranayake, L.P. Silver diamine fluoride (SDF) used in childhood caries management has potent antifungal activity against oral Candida species. BMC Microbiol. 2020, 20, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klanliang, K.; Asahi, Y.; Maezono, H.; Sotozono, M.; Kuriki, N.; Machi, H.; Ebisu, S.; Hayashi, M. An extensive description of the microbiological effects of silver diamine fluoride on dental biofilms using an oral in situ model. Sci. Rep. 2022, 12, 7435. [Google Scholar] [CrossRef] [PubMed]
- Karched, M.; Ali, D.; Ngo, H. In vivo antimicrobial activity of silver diammine fluoride on carious lesions in dentin. J. Oral Sci. 2019, 61, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Mei, M.L.; Ito, L.; Cao, Y.; Lo, E.C.M.; Li, Q.L.; Chu, C.H. An ex vivo study of arrested primary teeth caries with silver diamine fluoride therapy. J. Dent. 2014, 42, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Mei, M.L.; Zhao, I.S.; Ito, L.; Lo, E.C.-M.; Chu, C.-H. Prevention of secondary caries by silver diamine fluoride. Int. Dent. J. 2016, 66, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Mitwalli, H.; Mourao, M.D.A.; Dennison, J.; Yaman, P.; Paster, B.J.; Fontana, M. Effect of Silver Diamine Fluoride Treatment on Microbial Profiles of Plaque Biofilms from Root/Cervical Caries Lesions. Caries Res. 2019, 53, 555–566. [Google Scholar] [CrossRef]
- Mohammadi, N.; Farahmand Far, M. Effect of fluoridated varnish and silver diamine fluoride on enamel demineralization resistance in primary dentition. J. Indian Soc. Pedod. Prev. Dent. 2018, 36, 257. [Google Scholar] [CrossRef]
- Sorkhdini, P.; Gregory, R.L.; Crystal, Y.O.; Tang, Q.; Lippert, F. Effectiveness of in vitro primary coronal caries prevention with silver diamine fluoride—Chemical vs biofilm models. J. Dent. 2020, 99, 103418. [Google Scholar] [CrossRef]
- Alshahni, R.Z.; Alshahni, M.M.; Hiraishi, N.; Makimura, K.; Tagami, J. Effect of Silver Diamine Fluoride on Reducing Candida albicans Adhesion on Dentine. Mycopathologia 2020, 185, 691–698. [Google Scholar] [CrossRef]
- Tirupathi, S.; Nirmala, S.V.S.G.; Rajasekhar, S.; Nuvvula, S. Comparative cariostatic efficacy of a novel Nano-silver fluoride varnish with 38% silver diamine fluoride varnish a double-blind randomized clinical trial. J. Clin. Exp. Dent. 2019, 11, e105–e112. [Google Scholar] [CrossRef] [PubMed]
- Vinson, L.A.; Gilbert, P.R.; Sanders, B.J.; Moser, E.; Gregory, R.L. Silver Diamine Fluoride and Potassium Iodide Disruption of In Vitro Streptococcus mutans Biofilm. J. Dent. Child. 2018, 85, 120–124. [Google Scholar]
- Li, R.; Lo, E.C.M.; Liu, B.Y.; Wong, M.C.M.; Chu, C.H. Randomized clinical trial on arresting dental root caries through silver diammine fluoride applications in community-dwelling elders. J. Dent. 2016, 51, 15–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wierichs, R.J.; Meyer-Lueckel, H. Systematic Review on Noninvasive Treatment of Root Caries Lesions. J. Dent. Res. 2015, 94, 261–271. [Google Scholar] [CrossRef]
- Duangthip, D.; Chu, C.H.; Lo, E.C.M. A randomized clinical trial on arresting dentine caries in preschool children by topical fluorides—18 month results. J. Dent. 2016, 44, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Llodra, J.C.; Rodriguez, A.; Ferrer, B.; Menardia, V.; Ramos, T.; Morato, M. Efficacy of Silver Diamine Fluoride for Caries Reduction in Primary Teeth and First Permanent Molars of Schoolchildren: 36-month Clinical Trial. J. Dent. Res. 2005, 84, 721–724. [Google Scholar] [CrossRef]
- Lau, N.; O’Daffer, A.; Yi-Frazier, J.P.; Rosenberg, A.R. Popular Evidence-Based Commercial Mental Health Apps: Analysis of Engagement, Functionality, Aesthetics, and Information Quality. JMIR Mhealth Uhealth 2021, 9, e29689. [Google Scholar] [CrossRef]
- Greenwall-Cohen, J.; Greenwall, L.; Barry, S. Silver diamine fluoride—An overview of the literature and current clinical techniques. Br. Dent. J. 2020, 228, 831–838. [Google Scholar] [CrossRef]
- Al Qranei, M.S.; Balhaddad, A.A.; Melo, M.A.S. The burden of root caries: Updated perspectives and advances on management strategies. Gerodontology 2021, 38, 136–153. [Google Scholar] [CrossRef]
- Jiang, M.; Mei, M.L.; Wong, M.C.M.; Chu, C.H.; Lo, E.C.M. Effect of silver diamine fluoride solution application on the bond strength of dentine to adhesives and to glass ionomer cements: A systematic review. BMC Oral Health 2020, 20, 40. [Google Scholar] [CrossRef] [Green Version]
- Jiang, M.; Wong, M.C.M.; Chu, C.H.; Dai, L.; Lo, E.C.M. Effects of restoring SDF-treated and untreated dentine caries lesions on parental satisfaction and oral health related quality of life of preschool children. J. Dent. 2019, 88, 103171. [Google Scholar] [CrossRef] [PubMed]
- Knight, G.; McIntyre, J.; Craig, G.; Zilm, P.; Gully, N. Differences between normal and demineralized dentine pretreated with silver fluoride and potassium iodide after an in vitro challenge by Streptococcus mutans. Aust. Dent. J. 2007, 52, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Sayed, M.; Matsui, N.; Hiraishi, N.; Nikaido, T.; Burrow, M.; Tagami, J. Effect of Glutathione Biomolecule on Tooth Discoloration Associated with Silver Diammine Fluoride. Int. J. Mol. Sci. 2018, 19, 1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sayed, M.; Hiraishi, N.; Matin, K.; Abdou, A.; Burrow, M.F.; Tagami, J. Effect of silver-containing agents on the ultra-structural morphology of dentinal collagen. Dent. Mater. 2020, 36, 936–944. [Google Scholar] [CrossRef]
- Schwass, D.R.; Lyons, K.M.; Love, R.; Tompkins, G.R.; Meledandri, C.J. Antimicrobial Activity of a Colloidal AgNP Suspension Demonstrated In Vitro against Monoculture Biofilms: Toward a Novel Tooth Disinfectant for Treating Dental Caries. Adv. Dent. Res. 2018, 29, 117–123. [Google Scholar] [CrossRef]
- Ramazanli, V.N.; Ahmadov, I.S. Synthesis of Silver Nanoparticles by Using Extract of Olive Leaves. Adv. Biol. Earth Sci. 2022, 7, 238–244. [Google Scholar]
- Baran, A.; Fırat Baran, M.; Keskin, C.; Hatipoğlu, A.; Yavuz, Ö.; İrtegün Kandemir, S.; Eftekhari, A. Investigation of antimicrobial and cytotoxic properties and specification of silver nanoparticles (AgNPs) derived from Cicer arietinum L. green leaf extract. Front. Bioeng. Biotechnol. 2022, 10, 263. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PubMed: (“silver diamine fluoride” OR “SDF”) AND (“bacterial biofilms” OR “anti-bacterial agents”[MeSH Terms] OR “fluorides”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “Streptococcus mutans”[MeSH Terms] OR “dental plaque”[MeSH Terms] OR “biofilms”[MeSH Terms]) AND English[lang] |
| Web of Sciences: (“silver diamine fluoride” OR “SDF”) AND (“bacterial biofilms” OR “anti-bacterial agents” OR “fluorides” OR “dental caries” OR “Streptococcus mutans” OR “dental plaque” OR “biofilms”) AND Language: (English) |
| Scopus: (“silver diamine fluoride” OR “SDF”) AND (“bacterial biofilms” OR “anti-bacterial agents” OR “fluorides” OR “dental caries” OR “Streptococcus mutans” OR “dental plaque” OR “biofilms”) AND (LIMIT-TO (DOCTYPE, “ar”) OR LIMIT-TO (DOCTYPE, “re”)) AND (LIMIT-TO (LANGUAGE, “English”)) |
| ID and Year | Study Sample (n) | Objectives | Design | Assessment Drawn |
|---|---|---|---|---|
| Bao Ying et al. (2020) [38] | Five children | To evaluate the antibacterial performance of SDF in dentine biofilms | In vitro | Microbial diversity fell after SDF application. |
| Ebtissam et al. (2019) [39] | Seventy dentin discs (made from extracted human teeth) | To evaluate the antibacterial performance of CHX and NaOCl as compared to SDF | Case control | SDF exhibited higher antibacterial efficacy as compared to the controls. |
| Gerd et al. (2017) [40] | 100 samples of bovine dentin. | To evaluate the antibacterial performance of NaF and CHX as compared to SDF | In vitro | When compared to control, SDF dramatically reduced bacterial numbers. |
| Jaivrat et al. (2019) [41] | 32 extracted human molars and 32 extracted human premolars | To evaluate the antibacterial performance of CHX, distilled water and PAA as compared to SDF | Case control | SDF-KI was deemed to be effective in eliminating S. mutans. |
| Kausar et al. (2020) [42] | 35 Candida isolates | To evaluate the antifungal performance of SDF in isolation | In vitro | SDF appeared to successfully stop fungal filamentation even at extremely low doses, complementing its antibacterial activity |
| Klanliang et al. (2022) [43] | 10 healthy individuals (aged between 26–31 years) | To evaluate the microbiological performance of SDF in dentine biofilms | In situ | Dental biofilm development was inhibited and the percentage of killed bacteria was enhanced when SDF was applied to demineralized dentin but only up to 4 days |
| Maribasappa et al. (2019) [44] | 5 patients with carious lesions | To evaluate the antibacterial performance of SDF + potassium iodide (KI). | In vivo | In four of the five patients, SDF + KI totally stopped the growth of S. mutans |
| May L. Mei et al. (2014) [45] | 12 primary upper-central carious incisors | To evaluate the physicochemical performance of SDF in carious teeth | Ex vivo | Clinical SDF application enhanced the levels of dentine remineralization |
| May Lei et al. (2016) [46] | 6 premolars | To evaluate the antibacterial performance of SDF in two different types of restorations | In vitro | SDF application made both the types of restorations more resistant to subsequent caries. |
| Mitwalli et al. (2019) [47] | 20 participants (who had at least one cervical carious lesion or soft cavitated root) | To evaluate the microbiological performance of SDF in carious lesions | In vitro | Several bacterium species showed a substantial decrease in relative abundance following SDF treatment. |
| Najmeh et al. (2018) [48] | 45 extracted deciduous canines | To evaluate the antibacterial performance of fluorinated varnish as compared to SDF | In vitro | No significant differences between the antibacterial performance of both the compounds were observed |
| Parand Sorkhdini et al. (2020) [49] | 90 human enamel samples | To evaluate the antibacterial performance of AgNO3, KF and water as compared to SDF | Case control | SDF performed on a similar parlance as DW and KF that SDF was compared with. |
| Rima et al. (2020) [50] | Samples of bovine dentin divided into 3 groups | To evaluate the antifungal performance of SDF in isolation | In vitro | SDF appeared to successfully stop fungal filamentation even at extremely low doses, complementing its antibacterial activity |
| Sunny et al. (2019) [51] | 159 active dentinal carious lesions from primary molars | To evaluate the antibacterial performance of AgF as compared to SDF | RCT | SDF performed on a similar parlance as NaF that SDF was compared to |
| Vinson et al. (2018) [52] | S. mutans biofilm in six-well tissue culture plates | To evaluate the antibacterial performance of KI as compared to SDF | In vitro | SDF + KI performed with the highest efficacy, followerd by KI and SDF alone. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mubaraki, H.; Ingle, N.A.; Baseer, M.A.; AlMugeiren, O.M.; Mubaraki, S.; Cicciù, M.; Minervini, G. Effect of Silver Diamine Fluoride on Bacterial Biofilms—A Review including In Vitro and In Vivo Studies. Biomedicines 2023, 11, 1641. https://doi.org/10.3390/biomedicines11061641
Mubaraki H, Ingle NA, Baseer MA, AlMugeiren OM, Mubaraki S, Cicciù M, Minervini G. Effect of Silver Diamine Fluoride on Bacterial Biofilms—A Review including In Vitro and In Vivo Studies. Biomedicines. 2023; 11(6):1641. https://doi.org/10.3390/biomedicines11061641
Chicago/Turabian StyleMubaraki, Hind, Navin Anand Ingle, Mohammad Abdul Baseer, Osamah M AlMugeiren, Sarah Mubaraki, Marco Cicciù, and Giuseppe Minervini. 2023. "Effect of Silver Diamine Fluoride on Bacterial Biofilms—A Review including In Vitro and In Vivo Studies" Biomedicines 11, no. 6: 1641. https://doi.org/10.3390/biomedicines11061641