
Immunomodulatory Role of Vitamin D on Gut Microbiome in Children




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Eligibility Criteria
3. Results
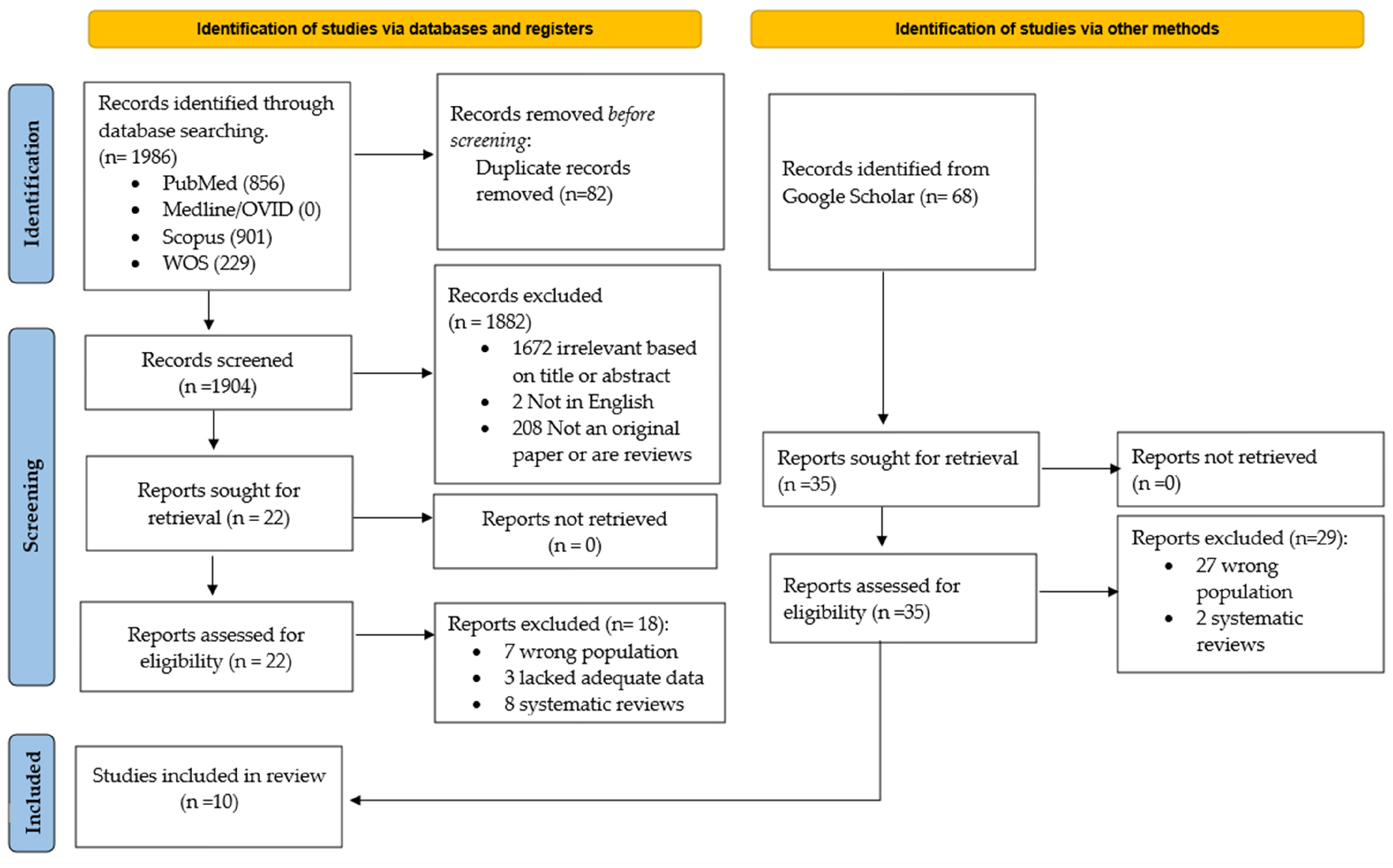
3.1. Study Selection
3.2. Study Characteristics
3.3. Association of Vitamin D with Microbial Composition and Diversity
3.4. Vitamin D Effects on the Phyla
3.5. Alteration of the Other Taxa with Vitamin D
4. Discussion
4.1. Pediatric Gut Microbiome and Immune System
4.2. Vitamin D and Immune Response
4.3. The Role of Vitamin D in Pediatric Gut Microbiome and Diseases
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| No. | Search Strategy |
|---|---|
| #1 | Vitamin D AND microbiome |
| #2 | Vitamin D AND microbiome AND immun * |
| #3 | Vitamin D AND microbiome AND infection |
| #4 | Vitamin D AND microbiome AND inflammat * |
| #5 | Vitamin D AND microbiome AND profiling |
| #6 | Vitamin D AND microbiome AND transcript * |
| #7 | Vitamin D AND microbiome AND pediatric |
| #8 | Vitamin D AND microbiome AND immune AND infection AND inflammation AND profiling AND transcript * AND pediatric |
| Databases | PubMed, SCOPUS, WOS, MEDLINE/OVID |
|---|---|
| Date of search | from January 1996 to January 2023 |
| Study type | Books and documents were excluded |
| Limit | Conference abstracts were excluded |
| Other databases | Google Scholar was used with the same keywords as the main databases |
References
- Fan, Y.; Pedersen, O. Gut Microbiota in Human Metabolic Health and Disease. Nat. Rev. Microbiol. 2020, 19, 55–71. [Google Scholar] [CrossRef] [PubMed]
- Yukgehnaish, K.; Kumar, P.; Sivachandran, P.; Marimuthu, K.; Arshad, A.; Paray, B.A.; Arockiaraj, J. Gut Microbiota Metagenomics in Aquaculture: Factors Influencing Gut Microbiome and Its Physiological Role in Fish. Rev. Aquac. 2020, 12, 1903–1927. [Google Scholar] [CrossRef]
- Xiao, H.; Kang, S. The Role of the Gut Microbiome in Energy Balance With a Focus on the Gut-Adipose Tissue Axis. Front. Genet. 2020, 11, 297. [Google Scholar] [CrossRef]
- Sanna, S.; van Zuydam, N.R.; Mahajan, A.; Kurilshikov, A.; Vich Vila, A.; Võsa, U.; Mujagic, Z.; Masclee, A.A.M.; Jonkers, D.M.A.E.; Oosting, M.; et al. Causal Relationships among the Gut Microbiome, Short-Chain Fatty Acids and Metabolic Diseases. Nat. Genet. 2019, 51, 600–605. [Google Scholar] [CrossRef]
- Das, P.; Babaei, P.; Nielsen, J. Metagenomic analysis of microbe-mediated vitamin metabolism in the human gut microbiome. BMC Genom. 2019, 20, 208. [Google Scholar] [CrossRef]
- Bosco, N.; Noti, M. The aging gut microbiome and its impact on host immunity. Genes. Immun. 2021, 22, 289–303. [Google Scholar] [CrossRef] [PubMed]
- Ronan, V.; Yeasin, R.; Claud, E.C. Childhood Development and the Microbiome-The Intestinal Microbiota in Maintenance of Health and Development of Disease During Childhood Development. Gastroenterology 2021, 160, 495–506. [Google Scholar] [CrossRef] [PubMed]
- Kapourchali, F.R.; Cresci, G.A.M. Early-Life Gut Microbiome-The Importance of Maternal and Infant Factors in Its Establishment. Nutr. Clin. Pr. 2020, 35, 386–405. [Google Scholar] [CrossRef]
- Saeed, N.K.; Al-Beltagi, M.; Bediwy, A.S.; El-Sawaf, Y.; Toema, O. Gut microbiota in various childhood disorders: Implication and indications. World J. Gastroenterol. 2022, 28, 1875–1901. [Google Scholar] [CrossRef]
- Chiu, C.Y.; Chan, Y.L.; Tsai, M.H.; Wang, C.J.; Chiang, M.H.; Chiu, C.C. Gut microbial dysbiosis is associated with allergen-specific IgE responses in young children with airway allergies. World Allergy Organ. J. 2019, 12, 100021. [Google Scholar] [CrossRef] [PubMed]
- Harbison, J.E.; Roth-Schulze, A.J.; Giles, L.C.; Tran, C.D.; Ngui, K.M.; Penno, M.A.; Thomson, R.L.; Wentworth, J.M.; Colman, P.G.; Craig, M.E.; et al. Gut Microbiome Dysbiosis and Increased Intestinal Permeability in Children with Islet Autoimmunity and Type 1 Diabetes: A Prospective Cohort Study. Pediatr. Diabetes 2019, 20, 574–583. [Google Scholar] [CrossRef]
- Fitzgerald, R.S.; Sanderson, I.R.; Claesson, M.J. Paediatric Inflammatory Bowel Disease and its Relationship with the Microbiome. Microb. Ecol. 2021, 82, 833–844. [Google Scholar] [CrossRef] [PubMed]
- Tremlett, H.; Zhu, F.; Arnold, D.; Bar-Or, A.; Bernstein, C.N.; Bonner, C.; Forbes, J.D.; Graham, M.; Hart, J.; Knox, N.C.; et al. The Gut Microbiota in Pediatric Multiple Sclerosis and Demyelinating Syndromes. Ann. Clin. Transl. Neurol. 2021, 8, 2252–2269. [Google Scholar] [CrossRef]
- Hufnagl, K.; Pali-Schöll, I.; Roth-Walter, F.; Jensen-Jarolim, E. Dysbiosis of the gut and lung microbiome has a role in asthma. Semin. Immunopathol. 2020, 42, 75–93. [Google Scholar] [CrossRef] [PubMed]
- Zhong, H.; Penders, J.; Shi, Z.; Ren, H.; Cai, K.; Fang, C.; Ding, Q.; Thijs, C.; Blaak, E.E.; Stehouwer, C.D.A.; et al. Impact of Early Events and Lifestyle on the Gut Microbiota and Metabolic Phenotypes in Young School-Age Children. Microbiome 2019, 7, 2. [Google Scholar] [CrossRef]
- McDonnell, L.; Gilkes, A.; Ashworth, M.; Rowland, V.; Harries, T.H.; Armstrong, D.; White, P. Association between Antibiotics and Gut Microbiome Dysbiosis in Children: Systematic Review and Meta-Analysis. Gut Microbes 2021, 13, 1870402. [Google Scholar] [CrossRef]
- Galazzo, G.; van Best, N.; Bervoets, L.; Dapaah, I.O.; Savelkoul, P.H.; Hornef, M.W.; Lau, S.; Hamelmann, E.; Penders, J.; Hutton, E.K.; et al. Development of the Microbiota and Associations with Birth Mode, Diet, and Atopic Disorders in a Longitudinal Analysis of Stool Samples, Collected from Infancy through Early Childhood. Gastroenterology 2020, 158, 1584–1596. [Google Scholar] [CrossRef] [PubMed]
- Fehr, K.; Moossavi, S.; Sbihi, H.; Boutin, R.C.T.; Bode, L.; Robertson, B.; Yonemitsu, C.; Field, C.J.; Becker, A.B.; Mandhane, P.J.; et al. Breastmilk Feeding Practices Are Associated with the Co-Occurrence of Bacteria in Mothers’ Milk and the Infant Gut: The CHILD Cohort Study. Cell Host Microbe 2020, 28, 285–297.e4. [Google Scholar] [CrossRef]
- Clark, A.; Mach, N. Role of vitamin D in the hygiene hypothesis: The interplay between vitamin D, vitamin D receptors, gut microbiota, and immune response. Front. Immunol. 2016, 7, 627. [Google Scholar] [CrossRef]
- Singh, P.; Rawat, A.; Alwakeel, M.; Sharif, E.; Al Khodor, S. The potential role of vitamin D supplementation as a gut microbiota modifier in healthy individuals. Sci. Rep. 2020, 10, 21641. [Google Scholar] [CrossRef]
- Zhou, H.; Zhao, X.; Sun, L.; Liu, Y.; Lv, Y.; Gang, X.; Wang, G. Gut Microbiota Profile in Patients with Type 1 Diabetes Based on 16S RRNA Gene Sequencing: A Systematic Review. Dis. Mrk. 2020, 2020, 1–11. [Google Scholar] [CrossRef]
- Almonacid, D.E.; Kraal, L.; Ossandon, F.J.; Budovskaya, Y.V.; Cardenas, J.P.; Bik, E.M.; Goddard, A.D.; Richman, J.; Apte, Z.S. Correction: 16S RRNA Gene Sequencing and Healthy Reference Ranges for 28 Clinically Relevant Microbial Taxa from the Human Gut Microbiome. PLoS ONE 2019, 14, e0212474. [Google Scholar] [CrossRef] [PubMed]
- Durazzi, F.; Sala, C.; Castellani, G.; Manfreda, G.; Remondini, D.; De Cesare, A. Comparison between 16S rRNA and shotgun sequencing data for the taxonomic characterization of the gut microbiota. Sci. Rep. 2021, 11, 3030. [Google Scholar] [CrossRef]
- Bellerba, F.; Muzio, V.; Gnagnarella, P.; Facciotti, F.; Chiocca, S.; Bossi, P.; Cortinovis, D.; Chiaradonna, F.; Serrano, D.; Raimondi, S.; et al. The association between Vitamin D and gut microbiota: A systematic review of human studies. Nutrients 2021, 13, 3378. [Google Scholar] [CrossRef] [PubMed]
- Cyprian, F.; Lefkou, E.; Varoudi, K.; Girardi, G. Immunomodulatory Effects of Vitamin D in Pregnancy and Beyond. Front. Immunol. 2019, 10, 2739. [Google Scholar] [CrossRef] [PubMed]
- Kalmarzi, R.N.; Ahmadi, S.; Rahehagh, R.; Fathallahpour, A.; Khalafi, B.; Kashefi, H.; Roshani, D.; Zaryan, R.N.; Mohamadi, S.; Kooti, W. The Effect of Vitamin D Supplementation on Clinical Outcomes of Asthmatic Children with Vitamin D Insufficiency. Endocr. Metab. Immune Disord.-Drug. Targets 2020, 20, 149–155. [Google Scholar] [CrossRef]
- Bhardwaj, B.; Singh, J. Efficacy of Vitamin D Supplementation in Allergic Rhinitis. Indian. J. Otolaryngol. Head. Neck Surg. 2021, 73, 152–159. [Google Scholar] [CrossRef]
- Guo, Y.; Zhang, T.; Wang, Y.; Liu, R.; Chang, M.; Wang, X. Effects of oral vitamin D supplementation on inflammatory bowel disease: A systematic review and meta-analysis. Food Funct. 2021, 12, 7588–7606. [Google Scholar] [CrossRef]
- Fakhoury, H.M.A.; Kvietys, P.R.; AlKattan, W.; Anouti, F.A.; Elahi, M.A.; Karras, S.N.; Grant, W.B. Vitamin D and Intestinal Homeostasis: Barrier, Microbiota, and Immune Modulation. J. Steroid Biochem. Mol. Biol. 2020, 200, 105663. [Google Scholar] [CrossRef]
- Wu, Z.; Liu, D.; Deng, F. The Role of Vitamin D in Immune System and Inflammatory Bowel Disease. J. Inflamm. Res. 2022, 15, 3167–3185. [Google Scholar] [CrossRef]
- Tang, W.; Rong, Y.; Zhang, H.; Zhan, Z.; Yuan, L.; Ning, Y.; Lin, W. The Correlation between a Th1/Th2 Cytokines Imbalance and Vitamin D Level in Patients with Early Chronic Obstructive Pulmonary Disease (COPD), Based on Screening Results. Front. Physiol. 2023, 14, 1032786. [Google Scholar] [CrossRef]
- Luthold, R.V.; Fernandes, G.R.; Franco-de-Moraes, A.C.; Folchetti, L.G.D.; Ferreira, S.R.G. Gut microbiota interactions with the immunomodulatory role of vitamin D in normal individuals. Metabolism 2017, 69, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Luo, M.; Pan, L.; Chen, Y.; Guo, S.; Luo, D.; Zhu, L.; Liu, Y.; Pan, L.; Xu, S.; et al. Vitamin D Signaling Maintains Intestinal Innate Immunity and Gut Microbiota: Potential Intervention for Metabolic Syndrome and NAFLD. Am. J. Physiol.-Gastrointest. Liver Physiol. 2020, 318, G542–G553. [Google Scholar] [CrossRef]
- Sordillo, J.E.; Zhou, Y.; McGeachie, M.J.; Ziniti, J.; Lange, N.; Laranjo, N.; Savage, J.R.; Carey, V.; O’Connor, G.; Sandel, M.; et al. Factors Influencing the Infant Gut Microbiome at Age 3–6 Months: Findings from the Ethnically Diverse Vitamin D Antenatal Asthma Reduction Trial (VDAART). J. Allergy Clin. Immunol. 2017, 139, 482–491.e14. [Google Scholar] [CrossRef]
- Hjelmsø, M.H.; Shah, S.A.; Thorsen, J.; Rasmussen, M.; Vestergaard, G.; Mortensen, M.S.; Brejnrod, A.; Brix, S.; Chawes, B.; Bønnelykke, K.; et al. Prenatal Dietary Supplements Influence the Infant Airway Microbiota in a Randomized Factorial Clinical Trial. Nat. Commun. 2020, 11, 426. [Google Scholar] [CrossRef] [PubMed]
- Lei, W.-T.; Huang, K.-Y.; Jhong, J.-H.; Chen, C.-H.; Weng, S.-L. Metagenomic Analysis of the Gut Microbiome Composition Associated with Vitamin D Supplementation in Taiwanese Infants. Sci. Rep. 2021, 11, 2856. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Bu, S.; Paneth, N.; Kerver, J.M.; Comstock, S.S. Vitamin D Supplementation in Exclusively Breastfed Infants Is Associated with Alterations in the Fecal Microbiome. Nutrients 2022, 14, 202. [Google Scholar] [CrossRef]
- Talsness, C.E.; Penders, J.; Jansen, E.H.J.M.; Damoiseaux, J.; Thijs, C.; Mommers, M. Influence of Vitamin D on Key Bacterial Taxa in Infant Microbiota in the KOALA Birth Cohort Study. PLoS ONE 2017, 12, e0188011. [Google Scholar] [CrossRef]
- Tabatabaeizadeh, S.-A.; Fazeli, M.; Meshkat, Z.; Khodashenas, E.; Esmaeili, H.; Mazloum, S.; Ferns, G.A.; Abdizadeh, M.F.; Ghayour-Mobarhan, M. The Effects of High Doses of Vitamin D on the Composition of the Gut Microbiome of Adolescent Girls. Clin. Nutr. ESPEN 2020, 35, 103–108. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, M.; Ran, Z.; Wang, J.; Ma, W.; Sheng, Q. Effect of Different Doses of Vitamin D on the Intestinal Flora of Babies with Eczema: An Experimental Study. Life 2022, 12, 1409. [Google Scholar] [CrossRef]
- Singh, P.; Rawat, A.; Saadaoui, M.; Elhag, D.; Tomei, S.; Elanbari, M.; Akobeng, A.K.; Mustafa, A.; Abdelgadir, I.; Udassi, S.; et al. Tipping the Balance: Vitamin D Inadequacy in Children Impacts the Major Gut Bacterial Phyla. Biomedicines 2022, 10, 278. [Google Scholar] [CrossRef]
- Drall, K.M.; Field, C.J.; Haqq, A.M.; de Souza, R.J.; Tun, H.M.; Morales-Lizcano, N.P.; Konya, T.B.; Guttman, D.S.; Azad, M.B.; Becker, A.B.; et al. Vitamin D Supplementation in Pregnancy and Early Infancy in Relation to Gut Microbiota Composition and C. Difficile Colonization: Implications for Viral Respiratory Infections. Gut Microbes 2020, 12, 1799734. [Google Scholar] [CrossRef] [PubMed]
- Kassem, Z.; Sitarik, A.; Levin, A.M.; Lynch, S.V.; Havstad, S.; Fujimura, K.; Kozyrskyj, A.; Ownby, D.R.; Johnson, C.C.; Yong, G.J.M.; et al. Maternal and Cord Blood Vitamin D Level and the Infant Gut Microbiota in a Birth Cohort Study. Matern. Health Neonatol. Perinatol. 2020, 6, 5. [Google Scholar] [CrossRef]
- Jasirwan, C.O.M.; Muradi, A.; Hasan, I.; Simadibrata, M.; Rinaldi, I. Correlation of Gut Firmicutes/Bacteroidetes Ratio with Fibrosis and Steatosis Stratified by Body Mass Index in Patients with Non-Alcoholic Fatty Liver Disease. Biosci. Microbiota Food Health 2020, 40, 50–58. [Google Scholar] [CrossRef]
- Zakerska-Banaszak, O.; Tomczak, H.; Gabryel, M.; Baturo, A.; Wolko, L.; Michalak, M.; Malinska, N.; Mankowska-Wierzbicka, D.; Eder, P.; Dobrowolska, A.; et al. Dysbiosis of Gut Microbiota in Polish Patients with Ulcerative Colitis: A Pilot Study. Sci. Rep. 2021, 11, 2166. [Google Scholar] [CrossRef]
- Deering, K.E.; Devine, A.; O’sullivan, T.A.; Lo, J.; Boyce, M.C.; Christophersen, C.T. Characterizing the Composition of the Pediatric Gut Microbiome: A Systematic Review. Nutrients 2019, 12, 16. [Google Scholar] [CrossRef] [PubMed]
- Das, B.; Nair, G.B. Homeostasis and dysbiosis of the gut microbiome in health and disease. J. Biosci. 2019, 44, 1–8. [Google Scholar] [CrossRef]
- Antonini, M.; Conte, M.L.; Sorini, C.; Falcone, M. How the interplay between the commensal microbiota, gut barrier integrity, and mucosal immunity regulates brain autoimmunity. Front. Immunol. 2019, 10, 1937. [Google Scholar] [CrossRef]
- Rinninella, E.; Raoul, P.; Cintoni, M.; Franceschi, F.; Miggiano, G.; Gasbarrini, A.; Mele, M. What Is the Healthy Gut Microbiota Composition? A Changing Ecosystem across Age, Environment, Diet, and Diseases. Microorganisms 2019, 7, 14. [Google Scholar] [CrossRef]
- Eslami, M.; Bahar, A.; Hemati, M.; Rasouli Nejad, Z.; Mehranfar, F.; Karami, S.; Kobyliak, N.M.; Yousefi, B. Dietary Pattern, Colonic Microbiota and Immunometabolism Interaction: New Frontiers for Diabetes Mellitus and Related Disorders. Diabetic Medicine 2020, 38, 255. [Google Scholar] [CrossRef]
- Martinez-Guryn, K.; Leone, V.; Chang, E.B. Regional Diversity of the Gastrointestinal Microbiome. Cell Host Microbe 2019, 26(3), 314–324. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Hu, Y.-X.; He, M.-Y.; Xie, Y.-H.; Su, W.; Long, D.; Zhao, R.; Wang, J.; Dai, C.; Li, H.; et al. Gut-Lung Dysbiosis Accompanied by Diabetes Mellitus Leads to Pulmonary Fibrotic Change through the NF-ΚB Signaling Pathway. Am. J. Pathol. 2021, 191, 838–856. [Google Scholar] [CrossRef] [PubMed]
- White, J.H. Emerging Roles of Vitamin D-Induced Antimicrobial Peptides in Antiviral Innate Immunity. Nutrients 2022, 14, 284. [Google Scholar] [CrossRef] [PubMed]
- Gubatan, J.; Rogalla, S.; Holman, D.R.; Puntasecca, C.J.; Polevoi, D.; Rubin, S.J.S. Antimicrobial peptides and the gut microbiome in inflammatory bowel disease. World J. Gastroenterol. 2021, 27, 506–520. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Sun, L.; Zhang, S.; Zhao, X.; Gang, X.; Wang, G. Evaluating the Causal Role of Gut Microbiota in Type 1 Diabetes and Its Possible Pathogenic Mechanisms. Front. Endocrinol. 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Yao, Y.; Cai, X.; Fei, W.; Ye, Y.; Zhao, M.; Zheng, C. The role of short-chain fatty acids in immunity, inflammation and metabolism. Crit. Rev. Food Sci. Nutr. 2020, 62, 3803–3816. [Google Scholar] [CrossRef]
- Takeuchi, T.; Miyauchi, E.; Kanaya, T.; Kato, T.; Nakanishi, Y.; Watanabe, T.; Kitami, T.; Taida, T.; Sasaki, T.; Negishi, H.; et al. Acetate Differentially Regulates IgA Reactivity to Commensal Bacteria. Nature 2021, 595, 560–564. [Google Scholar] [CrossRef]
- Danne, C.; Sokol, H. Butyrate, a new microbiota-dependent player in CD8+ T cells immunity and cancer therapy? Cell Rep. Med. 2021, 2, 1032–1043. [Google Scholar] [CrossRef]
- Zhang, Y.; Garrett, S.; Carroll, R.E.; Xia, Y.; Sun, J. Vitamin D receptor upregulates tight junction protein claudin-5 against colitis-associated tumorigenesis. Mucosal Immunol. 2022, 15, 683–697. [Google Scholar] [CrossRef]
- Arora, J.; Wang, J.; Weaver, V.; Zhang, Y.; Cantorna, M.T. Novel Insight into the Role of the Vitamin D Receptor in the Development and Function of the Immune System. J. Steroid Biochem. Mol. Biol. 2022, 219, 106084. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhao, Y.; Zhu, X.-D.; Guo, Y.; Yang, Y.; Jiang, Y.; Liu, B.-C. Active Vitamin D Regulates Macrophage M1/M2 Phenotypes via the STAT-1-TREM-1 Pathway in Diabetic Nephropathy. J. Cell. Physiol. 2019, 234, 6917–6926. [Google Scholar] [CrossRef]
- Ricca, C.; Aillon, A.; Bergandi, L.; Alotto, D.; Castagnoli, C.; Silvagno, F. Vitamin D Receptor Is Necessary for Mitochondrial Function and Cell Health. Int. J. Mol. Sci. 2018, 19, 1672. [Google Scholar] [CrossRef] [PubMed]
- Fantini, C.; Corinaldesi, C.; Lenzi, A.; Migliaccio, S.; Crescioli, C. Vitamin D as a Shield against Aging. Int. J. Mol. Sci. 2023, 24, 4546. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Singh, S.N.; Kumar, R.; Sehra, R. Vitamin D: A Modulator of Allergic Rhinitis. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 2225–2230. [Google Scholar] [CrossRef] [PubMed]
- Kourosh, A.; Luna, R.A.; Balderas, M.; Nance, C.; Anagnostou, A.; Devaraj, S.; Davis, C.M. Fecal Microbiome Signatures Are Different in Food-Allergic Children Compared to Siblings and Healthy Children. Pediatr. Allergy Immunol. 2018, 29, 545–554. [Google Scholar] [CrossRef]
- Liu, X.; Cheng, Y.-W.; Shao, L.; Sun, S.-H.; Wu, J.; Song, Q.-H.; Zou, H.-S.; Ling, Z.-X. Gut Microbiota Dysbiosis in Chinese Children with Type 1 Diabetes Mellitus: An Observational Study. World J. Gastroenterol. 2021, 27, 2394–2414. [Google Scholar] [CrossRef]
- de Freitas, M.B.; Moreira, E.A.M.; Tomio, C.; Moreno, Y.M.F.; Daltoe, F.P.; Barbosa, E.; Ludwig Neto, N.; Buccigrossi, V.; Guarino, A. Altered Intestinal Microbiota Composition, Antibiotic Therapy and Intestinal Inflammation in Children and Adolescents with Cystic Fibrosis. PLoS ONE 2018, 13, e0198457. [Google Scholar] [CrossRef]
- Metzger, M.I.; Graeber, S.Y.; Stahl, M.; Sommerburg, O.; Mall, M.A.; Dalpke, A.H.; Boutin, S. A Volatile and Dynamic Longitudinal Microbiome Is Associated with Less Reduction in Lung Function in Adolescents with Cystic Fibrosis. Front. Cell. Infect. Microbiol. 2021, 11, 2235–2988. [Google Scholar] [CrossRef] [PubMed]
- Grigor’eva, I.N. Gallstone Disease, Obesity and the Firmicutes/Bacteroidetes Ratio as a Possible Biomarker of Gut Dysbiosis. J. Pers. Med. 2020, 11, 13. [Google Scholar] [CrossRef]
- Stojanov, S.; Berlec, A.; Štrukelj, B. The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel Disease. Microorganisms 2020, 8, 1715. [Google Scholar] [CrossRef]
- Dong, T.S.; Guan, M.; Mayer, E.A.; Stains, J.; Liu, C.; Vora, P.; Jacobs, J.P.; Lagishetty, V.; Chang, L.; Barry, R.L.; et al. Obesity Is Associated with a Distinct Brain-Gut Microbiome Signature That Connects Prevotella and Bacteroides to the Brain’s Reward Center. Gut Microbes 2022, 14, 1–20. [Google Scholar] [CrossRef] [PubMed]
- White, J.H. Vitamin D deficiency and the pathogenesis of Crohn’s disease. J. Steroid Biochem. Mol. Biol. 2018, 175, 23–28. [Google Scholar] [CrossRef]
- Xue, G.; Gao, R.; Liu, Z.; Xu, N.; Cao, Y.; Zhao, B.; Du, J. Vitamin D/VDR Signaling Inhibits Colitis by Suppressing HIF-1α Activation in Colonic Epithelial Cells. Am. J. Physiol.-Gastrointest. Liver Physiol. 2021, 320, G837–G846. [Google Scholar] [CrossRef] [PubMed]
- Mailhot, G.; White, J.H. Vitamin D and Immunity in Infants and Children. Nutrients 2020, 12, 1233. [Google Scholar] [CrossRef]
- Yang, Y.; Cui, X.; Li, J.; Wang, H.; Li, Y.; Chen, Y.; Zhang, H. Clinical Evaluation of Vitamin D Status and Its Relationship with Disease Activity and Changes of Intestinal Immune Function in Patients with Crohn’s Disease in the Chinese Population. Scand. J. Gastroenterol. 2021, 56, 20–29. [Google Scholar] [CrossRef]
- Battistini, C.; Ballan, R.; Herkenhoff, M.E.; Saad, S.M.I.; Sun, J. Vitamin D Modulates Intestinal Microbiota in Inflammatory Bowel Diseases. Int. J. Mol. Sci. 2020, 22, 362. [Google Scholar] [CrossRef] [PubMed]
- Martens, P.-J.; Centelles-Lodeiro, J.; Ellis, D.; Cook, D.P.; Sassi, G.; Verlinden, L.; Verstuyf, A.; Raes, J.; Mathieu, C.; Gysemans, C. High Serum Vitamin D Concentrations, Induced via Diet, Trigger Immune and Intestinal Microbiota Alterations Leading to Type 1 Diabetes Protection in NOD Mice. Front. Immunol. 2022, 13, 1664–3224. [Google Scholar] [CrossRef]
- Tabatabaeizadeh, S.-A.; Tafazoli, N.; Ferns, G.A.; Avan, A.; Ghayour-Mobarhan, M. Vitamin D, the gut microbiome and inflammatory bowel disease. J. Res. Med. Sci. 2018, 23, 75. [Google Scholar] [CrossRef]


| Title | Reference | Objective | Type of Study | Sample Size | Age Range | Lab Findings |
|---|---|---|---|---|---|---|
| Factors influencing the infant gut microbiome at age 3–6 months: findings from the ethnically diverse Vitamin D Antenatal Asthma Reduction Trial (VDAART). | [34] | To ascertain the effects of prenatal and early life factors on the gut microbiome in a sizable, ethnically diverse study population of infants who were enrolled in the Vitamin D Antenatal Asthma Reduction Trial, a clinical trial of Vitamin D supplementation in pregnancy to prevent allergies and asthma in offspring. | Cross-sectional (nested within an RCT) | 333 | 3–6 months old | Lachnobacterium, Lachnospiraceae and U. clostridiales coabundance, and a decrease in Lactococcus, were all associated with Vitamin D levels in cord blood immediately following birth (in utero) |
| Prenatal dietary supplements influence the infant airway microbiota in a randomized factorial clinical trial | [35] | To determine if providing mothers with n-3 LCPUFA and Vitamin D influences the microbiome of the infant and mother and to clarify if the protective impact of these supplements on asthma can be regulated by the microbiota. | Random-ized clinical trials | 580 | Prenatal–1-year-old | No significant data |
| Metagenomic analysis of the gut microbiome composition associated with Vitamin D supplementation in Taiwanese infants | [36] | To ascertain the impact of Vitamin D supplementation on the development of the infant gut microbiome in Taiwan, as well as to look into the distribution and diversity of the infant gut microbiota under various feeding regimens, both with and without Vitamin D administration. | Clinical trials | 62 | 0–4 months old | Infants that received Vitamin D supplements showed elevated levels of the genus Lactobacillus, Streptococcus, and Bifidobacterium, as well as a greater F/B ratio. Supplementing with Vitamin D decreased the amount of Bacteroides. The majority of the pathways identified were found to be engaged in various types of antibiotic production, which suggests that microbial communities exist in highly competitive environments, according to the metabolic analysis profiles in breastfed infants with Vitamin D deficiency. |
| Vitamin D Supplementation in Exclusively Breastfed Infants Is Associated with Alterations in the Fecal Microbiome | [37] | In order to ascertain the relationship between maternal and infant characteristics, infant feeding practises, and the gut microbiota profiles in 3- to 9-month-old infants, we separately analysed infants who were exclusively breastfed and those who were not in order to evaluate the impact of different feeding practises features on the microbiotas of the infants in each group. | Cohort study | 191 | 3–9 months old | Infants who were exclusively breastfed and received Vitamin D supplements saw a decline in hemophilus |
| Influence of Vitamin D on key bacterial taxa in infant microbiota in the KOALA Birth Cohort Study | [38] | To determine if maternal Vitamin D administration, maternal plasma 25-hydroxyvitamin D concentration, or newborn Vitamin D administration directly affects major bacterial taxa within newborns’ microbiome at one month old. | Cohort study | 913 | 1 month old | Bifidobacterium spp. decreased when maternal Vitamin D supplementation levels increased. C. difficile levels in breastfed infants with Vitamin D supplements were lower as well. |
| The effects of high doses of Vitamin D on the composition of the gut microbiome of adolescent girls | [39] | To assess the impact of a high-dose Vitamin D supplement on the gut microbiome’s composition. | Cohort study | 50 | 12–18 years old | The expression folds of Enterococcus (1.05), Bifidobacterium (1.20), and Firmicutes (1.50) all increase with Vitamin D treatment. While Lactobacillus 24% (p = 0.006) and Bacteroidetes 72% (p < 0.0001) declined. |
| Effect of Different Doses of Vitamin D on the Intestinal Flora of Babies with Eczema: An Experimental Study | [40] | To determine whether altering the Vitamin D dosage can restore the immune system and intestinal flora of infants with eczema who typically consume 400 IU of Vitamin D per day. | 32 | 1–12 months | With low Vitamin D dosage compared to no supplementation, Prevotella, species Prevotella copri, and family Prevotellaceae decreased in children with eczema. Children with eczema had higher levels of the bacteria Bacteroides vulgatus, Phascolarctobacterium faecium, order Acidaminococcales, family Acidaminococcaceae, genus Phascolarctobacterium, f-Sutterellaceae, and species Parasutterella excrementihominis with low Vitamin D supplementation compared to no supplementation. | |
| Tipping the Balance: Vitamin D Inadequacy in Children Impacts the Major Gut Bacterial Phyla | [41] | To comprehend the incidence, causes of it, and effects of inadequate Vitamin D in Qatari children. | Cohort study | 64 | 4–14 years old | Prevotella 9 and Bacteroidetes increased in Vitamin D-deficient children (50 nmol/L), but Firmicutes, Bacteroides, Alistipes, B/P ratio, and F/B reduced. Prevotella dislens, Prevotella bivia, Bacteroides massillensis, Alistipes marseille, and Alistipes indistinctus were among the species that were more prevalent. Bacteroides and Alistipes, including Alistipes finegoldii, Alistipes sp. AL1, Alistipes sp. N15 MGS-157, Bacteroides caceae, Bacteroides eggerthii, and Bacteroides plebeius, were more prevalent in Vitamin D non-deficient (>50 nmol/L) individuals. |
| Vitamin D supplementa-tion in pregnancy and early infancy in relation to gut microbiota composition and C. difficile colonization: Implications for viral respiratory infections | [42] | In 1157 mother–infant couples participating in the CHILD (Canadian Healthy Infant Longitudinal Development) Cohort Study from 2009 to 2012, the connection between maternal and newborn Vitamin D supplementation, infant gut microbiota makeup, and Clostridioides difficile colonisation was examined. | Cohort study | 1157 | 3–4 months old | Genus Megamonas declines in infants receiving Vitamin D supplements. In breastfed newborns, Bilophila (-) and Lachnospiraceae decrease with maternal Vitamin D administration, but Haemophilus rises. Once breastfeeding status and other variables were taken into account, neither infant nor maternal Vitamin D supplementation was linked to C. difficile colonisation. Infant colonisation with C. difficile was less likely when mothers drank milk that was supplemented with Vitamin D. |
| Maternal and cord blood Vitamin D level, and the infant gut microbiota in a birth cohort study | [43] | To investigate relationships between newborn gut microbiota and plasma 25[OH]D levels throughout pregnancy or at birth (cord blood). | Cohort study | 499 | 1–6 months old | Acinetobacter and Corynebacterium increased with maternal and cord Vitamin D. Ruminococcus gnavus decreased with Vitamin D treatment in Cord. Supplementing with prenatal Vitamin D led to a rise in Ruminococcus gnavus. |
| Reference | Dosage | Study Time | Placebo or Comparator | Health Condition | Alpha Diversity and Beta Diversity of the Gut Microbiota |
|---|---|---|---|---|---|
| [34] | 4000 IU vitamin D + prenatal vitamins or 400 IU vitamin D + prenatal vitamins | 18 months | Different doses | Infants of asthmatic or allergic parent | No significant differences in the alpha diversity or beta diversity of the infant gut microbiota (p > 0.05) |
| [35] | 2800 IU/day or 400 IU/day + placebo | 3 months | Different doses with Placebo | Wheezing or asthmatic mothers | No significant differences were observed between the Vitamin D supplementation group and the control group for the bacterial diversity at 1 week, 1 month, or 1 year postpartum (p = 0.955, p = 0.865, p = 0.971). |
| [36] | 400 IU of vitamin D/day or placebo | 4 months | Placebo | Healthy | For the beta diversity, the gut bacteria composition differed significantly at the different time points (ANOSIM, R = 0.742, p = 2.14 × 10−5). The alpha diversity index strongly reduced in infants during the period from birth to term age while having no obvious change after 1 month |
| [37] | Vitamin D supplement vs. no Vitamin D supplement in past 24 h | 24 h | Vitamin D doses or no doses | Healthy | Alpha diversity: lower Shannon index (p-value < 0.007) than those infants who were not given a Vitamin D. Beta diversity: p-value = 0.02 |
| [38] | Maternal VDS: 0 μg or <10 μg/day or ≥10 μg/day. Infant VDS: classified as yes or no | 6 months | Different doses or no dose | Healthy | N/A |
| [39] | 50,000 IU/week | 9 weeks | Before and after supplementation | Healthy | N/A |
| [40] | Vitamin D 400 IU/day or vitamin D 400 IU/day + vitamin D 200 (D-LOW) or 400 IU/day + vitamin D 400 IU/day (D-MED) or 400 IU/day+ 800 IU/day (D-HIGH) | 1 month | Comparison between doses | Healthy infants and infant with Eczema | For alpha diversity, no significant difference in the richness in the groups. Diversity in the D–HIGH group was lower (p < 0.01). For beta diversity, there were similarities between eczema and D–MID group, as well as control and D-LOW group. Other groups differed significantly. |
| [41] | N/A | N/A | Vitamin D deficient and non-deficient | Healthy | No significant difference in alpha diversity beta diversity measure (p < 0.01) |
| [42] | Maternal and infant VDS of >400 IU/day/<400 IU/day/400 IU/day | 3 months | Different doses or no dose | Healthy | N/A |
| [43] | N/A | N/A | Vitamin D levels | Higher risk for asthma | Higher prenatal 25(OH)D level was significantly associated with decreased richness (p = 0.028) and diversity (p = 0.012) of the gut microbiota at 1-month infants. Prenatal and cord 25(OH)D levels were significantly associated with 1-month microbiota composition. |
| Phylum | Class | Order | Family | Genus | Species |
|---|---|---|---|---|---|
| Actinobacteria | Actinomycetia | Mycobacteriales | Corynebacteriaceae | Corynebacterium | |
| Actinobacteria | Actinomycetia | Bifidobacteriales | Bifidobacteriaceae | Bifidobacterium spp. | |
| Bacteroidetes | Bacteroidia | Bacteroidales | Prevotellaceae | Prevotella | Prevotella dislens |
| Bacteroidetes | Bacteroidia | Bacteroidales | Prevotellaceae | Prevotella | Prevotella bivia |
| Bacteroidetes | Bacteroidia | Bacteroidales | Prevotellaceae | Prevotella | Prevotella copri |
| Bacteroidetes | Bacteroidia | Bacteroidales | Rikenellaceae | Alistipes | Alistipes finegoldii |
| Bacteroidetes | Bacteroidia | Bacteroidales | Rikenellaceae | Alistipes | Alistipes sp. AL1 |
| Bacteroidetes | Bacteroidia | Bacteroidales | Rikenellaceae | Alistipes | Alistipes sp. N15 MGS-157 |
| Bacteroidetes | Bacteroidia | Bacteroidales | Rikenellaceae | Alistipes | Alistipes marseille |
| Bacteroidetes | Bacteroidia | Bacteroidales | Rikenellaceae | Alistipes | Alistipes indistinctus |
| Bacteroidetes | Bacteroidia | Bacteroidales | Bacteroidaceae | Bacteroides | Bacteroides massillensis |
| Bacteroidetes | Bacteroidia | Bacteroidales | Bacteroidaceae | Bacteroides | Bacteroides caceae |
| Bacteroidetes | Bacteroidia | Bacteroidales | Bacteroidaceae | Bacteroides | Bacteroides eggerthii |
| Bacteroidetes | Bacteroidia | Bacteroidales | Bacteroidaceae | Bacteroides | Bacteroides plebeius |
| Bacteroidetes | Bacteroidia | Bacteroidales | Bacteroidaceae | Bacteroides | Bacteroides vulgatus |
| Firmicutes | Clostridia | Eubacteriales | Lachnospiraceae | Lachnobacterium | |
| Firmicutes | Clostridia | Clostridiales | Ruminococcaceae | Ruminococcus | Ruminococcus gnavus |
| Firmicutes | Bacilli | Lactobacillales | Streptococcaceae | Lactococcus | |
| Firmicutes | Bacilli | Lactobacillales | Lactobacillaceae | Lactobacillus | |
| Firmicutes | Bacilli | Lactobacillales | Prcoccaceae | Streptococcus | |
| Firmicutes | Clostridia | Clostridiales | Unclassified Clostridiales | ||
| Firmicutes | Bacilli | Lactobacillales | Enterococcaceae | Enterococcus | |
| Firmicutes | Clostridia | Eubacteriales | Peptostreptococcaceae | Clostridioides | C. difficile |
| Firmicutes | Negativicutes | Selenomonadales | Selenomonadaceae | Megamonas | |
| Firmicutes | Negativicutes | Acidaminococcales | Acidaminococcaceae | Phascolarctobacterium | Phascolarctobacterium faecium |
| Proteobacteria | Gammaproteobacteria | Pasteurellales | Pasteurellaceae | Haemophilus | |
| Proteobacteria | Gammaproteobacteria | Pseudomonadales | Moraxellaceae | Acinetobacter | |
| Proteobacteria | Deltaproteobacteria | Desulfovibrionales | Desulfovibrionaceae | Bilophila | |
| Proteobacteria | Betaproteobacteria | Burkholderiales | Sutterellaceae | Parasutterella | Parasutterella excrementihominis |
 taxa decreased with Vitamin D.
taxa decreased with Vitamin D.  taxa increased with Vitamin D.
taxa increased with Vitamin D.  taxa that both increased and decreased with Vitamin D.
taxa that both increased and decreased with Vitamin D.  taxa not significantly altered with Vitamin D. Green represents the taxa that were increased with Vitamin D levels, and red represents the taxa that were decreased with Vitamin D levels. Orange represents the taxa that were both increased and decreased and white represents the taxa that were unchanged.
taxa not significantly altered with Vitamin D. Green represents the taxa that were increased with Vitamin D levels, and red represents the taxa that were decreased with Vitamin D levels. Orange represents the taxa that were both increased and decreased and white represents the taxa that were unchanged.Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabassum, A.; Ali, A.; Zahedi, F.D.; Ismail, N.A.S. Immunomodulatory Role of Vitamin D on Gut Microbiome in Children. Biomedicines 2023, 11, 1441. https://doi.org/10.3390/biomedicines11051441
Tabassum A, Ali A, Zahedi FD, Ismail NAS. Immunomodulatory Role of Vitamin D on Gut Microbiome in Children. Biomedicines. 2023; 11(5):1441. https://doi.org/10.3390/biomedicines11051441
Chicago/Turabian StyleTabassum, Anika, Adli Ali, Farah Dayana Zahedi, and Noor Akmal Shareela Ismail. 2023. "Immunomodulatory Role of Vitamin D on Gut Microbiome in Children" Biomedicines 11, no. 5: 1441. https://doi.org/10.3390/biomedicines11051441