
Antiarrhythmic Drug Therapy in Arrhythmogenic Right Ventricular Cardiomyopathy

Abstract
:1. Introduction
2. Overview/Pathogenesis
3. Indications/Guidelines
4. AAD Drug Trials/Current Evidence
5. Major Trials on AAD Therapy in ARVC
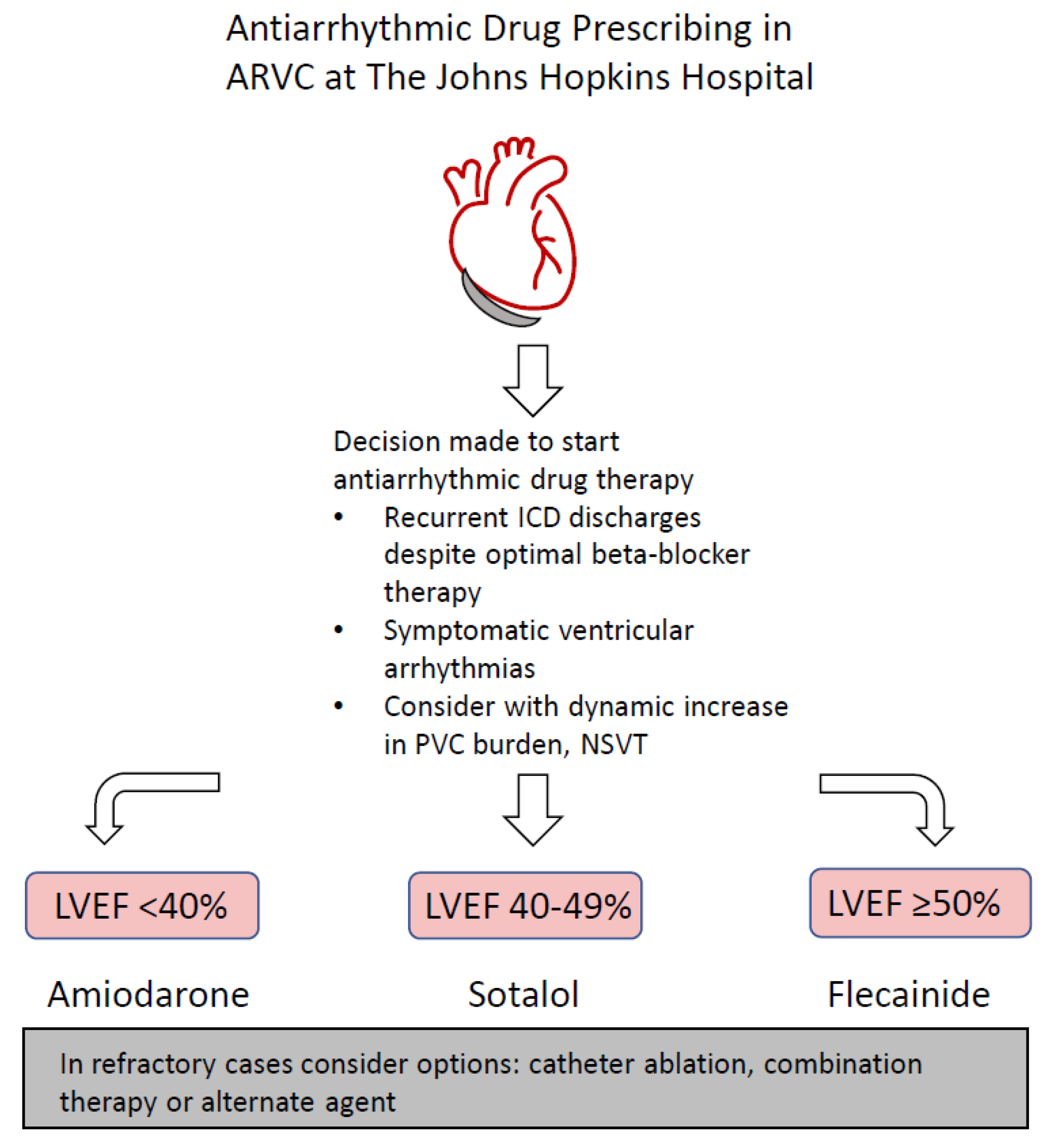
6. Current Practice at the Johns Hopkins Hospital
7. Discussion
8. Future Directions
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Corrado, D.; Link, M.S.; Calkins, H. Arrhythmogenic Right Ventricular Cardiomyopathy. New Engl. J. Med. 2017, 376, 61–72. [Google Scholar] [CrossRef]
- Corrado, D.; Wichter, T.; Link, M.S.; Hauer, R.N.; Marchlinski, F.E.; Anastasakis, A.; Bauce, B.; Basso, C.; Brunckhorst, C.; Tsatsopoulou, A.; et al. Treatment of Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia. Circulation 2015, 132, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Dalal, D.; Jain, R.; Tandri, H.; Dong, J.; Eid, S.M.; Prakasa, K.; Tichnell, C.; James, C.; Abraham, T.; Russell, S.D.; et al. Long-Term Efficacy of Catheter Ablation of Ventricular Tachycardia in Patients with Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy. J. Am. Coll. Cardiol. 2007, 50, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.; Trümmel, M.; Meyners, W. Prevalence of right ventricular dysplasia-cardiomyopathy in a non-referral hospital. Int. J. Cardiol. 2004, 97, 499–501. [Google Scholar] [CrossRef] [PubMed]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–423. [Google Scholar] [CrossRef]
- Alblaihed, L.; Kositz, C.; Brady, W.J.; Al-Salamah, T.; Mattu, A. Diagnosis and management of arrhythmogenic right ventricular cardiomyopathy. Am. J. Emerg. Med. 2023, 65, 146–153. [Google Scholar] [CrossRef]
- Buja, G.; Estes, N.A., 3rd; Wichter, T.; Corrado, D.; Marcus, F.; Thiene, G. Arrhythmogenic right ventricular cardiomyopathy/dysplasia: Risk stratification and therapy. Prog. Cardiovasc. Dis. 2008, 50, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Nava, A.; Bauce, B.; Basso, C.; Muriago, M.; Rampazzo, A.; Villanova, C.; Daliento, L.; Buja, G.; Corrado, D.; Danieli, G.A.; et al. Clinical profile and long-term follow-up of 37 families with arrhythmogenic right ventricular cardiomyopathy. J. Am. Coll. Cardiol. 2000, 36, 2226–2233. [Google Scholar] [CrossRef]
- Lemola, K.; Brunckhorst, C.; Helfenstein, U.; Oechslin, E.; Jenni, R.; Duru, F. Predictors of adverse outcome in patients with arrhythmogenic right ventricular dysplasia/cardiomyopathy: Long term experience of a tertiary care centre. Heart 2005, 91, 1167–1172. [Google Scholar] [CrossRef]
- Corrado, D.; Zorzi, A.; Cerrone, M.; Rigato, I.; Mongillo, M.; Bauce, B.; Delmar, M. Relationship Between Arrhythmogenic Right Ventricular Cardiomyopathy and Brugada Syndrome: New Insights from Molecular Biology and Clinical Implications. Circ. Arrhythm. Electrophysiol. 2016, 9, e003631. [Google Scholar] [CrossRef]
- Cerrone, M.; Delmar, M. Desmosomes and the sodium channel complex: Implications for arrhythmogenic cardiomyopathy and Brugada syndrome. Trends Cardiovasc. Med. 2014, 24, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Valle, G.; Furlan, S.; Nani, A.; Gyorke, S.; Fill, M.; Volpe, P. Mechanism of calsequestrin regulation of single cardiac ryanodine receptor in normal and pathological conditions. J. Gen. Physiol. 2013, 142, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Cerrone, M.; Montnach, J.; Lin, X.; Zhao, Y.-T.; Zhang, M.; Agullo-Pascual, E.; Leo-Macias, A.; Alvarado, F.J.; Dolgalev, I.; Karathanos, T.V.; et al. Plakophilin-2 is required for transcription of genes that control calcium cycling and cardiac rhythm. Nat. Commun. 2017, 8, 106. [Google Scholar] [CrossRef] [PubMed]
- Moccia, F.; Lodola, F.; Stadiotti, I.; Pilato, C.A.; Bellin, M.; Carugo, S.; Pompilio, G.; Sommariva, E.; Maione, A.S. Calcium as a Key Player in Arrhythmogenic Cardiomyopathy: Adhesion Disorder or Intracellular Alteration? Int. J. Mol. Sci. 2019, 20, 3986. [Google Scholar] [CrossRef]
- Hilliard, F.A.; Steele, D.S.; Laver, D.; Yang, Z.; Le Marchand, S.J.; Chopra, N.; Piston, D.W.; Huke, S.; Knollmann, B.C. Flecainide inhibits arrhythmogenic Ca2+ waves by open state block of ryanodine receptor Ca2+ release channels and reduction of Ca2+ spark mass. J. Mol. Cell. Cardiol. 2010, 48, 293–301. [Google Scholar] [CrossRef]
- Castelletti, S.; Orini, M.; Vischer, A.S.; McKenna, W.J.; Lambiase, P.D.; Pantazis, A.; Crotti, L. Circadian and Seasonal Pattern of Arrhythmic Events in Arrhythmogenic Cardiomyopathy Patients. Int. J. Environ. Res. Public Health 2023, 20, 2872. [Google Scholar] [CrossRef]
- Corrado, D.; Leoni, L.; Link, M.S.; Della Bella, P.; Gaita, F.; Curnis, A.; Salerno, J.U.; Igidbashian, D.; Raviele, A.; Disertori, M.; et al. Implantable Cardioverter-Defibrillator Therapy for Prevention of Sudden Death in Patients with Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia. Circulation 2003, 108, 3084–3091. [Google Scholar] [CrossRef]
- Towbin, J.A.; McKenna, W.J.; Abrams, D.J.; Ackerman, M.J.; Calkins, H.; Darrieux, F.C.C.; Daubert, J.P.; de Chillou, C.; DePasquale, E.C.; Desai, M.Y.; et al. HRS expert consensus statement on evaluation, risk stratification, and management of arrhythmogenic cardiomyopathy. Heart Rhythm 2019, 16, e301–e372. [Google Scholar] [CrossRef]
- Romero, J.; Patel, K.; Briceno, D.; Alviz, I.; Gabr, M.; Diaz, J.C.; Trivedi, C.; Mohanty, S.; Della Rocca, D.; Al-Ahmad, A.; et al. Endo-epicardial ablation vs endocardial ablation for the management of ventricular tachycardia in arrhythmogenic right ventricular cardiomyopathy: A systematic review and meta-analysis. J. Cardiovasc. Electrophysiol. 2020, 31, 2022–2031. [Google Scholar] [CrossRef]
- Gasperetti, A.; Tandri, H. Catheter Ablation of Ventricular Tachycardia in Arrhythmogenic Right Ventricular Cardiomyopathy. Card. Electrophysiol. Clin. 2022, 14, 679–683. [Google Scholar] [CrossRef]
- Philips, B.; Madhavan, S.; James, C.; Tichnell, C.; Murray, B.; Needleman, M.; Bhonsale, A.; Nazarian, S.; Laurita, K.R.; Calkins, H.; et al. High Prevalence of Catecholamine-facilitated Focal Ventricular Tachycardia in Patients with Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy. Circ. Arrhythmia Electrophysiol. 2013, 6, 160–166. [Google Scholar] [CrossRef]
- Hondeghem, L.M.; Snyders, D.J. Class III antiarrhythmic agents have a lot of potential but a long way to go. Reduced effectiveness and dangers of reverse use dependence. Circulation 1990, 81, 686–690. [Google Scholar] [CrossRef]
- Hosaka, F.; Shiga, T.; Sakomura, Y.; Wakaumi, M.; Matsuda, N.; Kasanuki, H. Amiodarone distribution in human tissues after long-term therapy: A case of arrhythmogenic right ventricular cardiomyopathy. Heart Vessel. 2002, 16, 154–156. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.W. Amiodarone. N. Engl. J. Med. 1987, 316, 455–466. [Google Scholar] [PubMed]
- Andrikopoulos, G.K. Flecainide: Current status and perspectives in arrhythmia management. World J. Cardiol. 2015, 7, 76. [Google Scholar] [CrossRef]
- Kannankeril, P.J.; Moore, J.P.; Cerrone, M.; Priori, S.G.; Kertesz, N.J.; Ro, P.S.; Batra, A.S.; Kaufman, E.S.; Fairbrother, D.L.; Saarel, E.V.; et al. Efficacy of Flecainide in the Treatment of Catecholaminergic Polymorphic Ventricular Tachycardia. JAMA Cardiol. 2017, 2, 759. [Google Scholar] [CrossRef] [PubMed]
- Echt, D.S.; Liebson, P.R.; Mitchell, L.B.; Peters, R.W.; Obias-Manno, D.; Barker, A.H.; Arensberg, D.; Baker, A.; Friedman, L.; Greene, H.L.; et al. Mortality and Morbidity in Patients Receiving Encainide, Flecainide, or Placebo. N. Engl. J. Med. 1991, 324, 781–788. [Google Scholar] [CrossRef]
- Cerrone, M.; Lin, X.; Zhang, M.; Agullo-Pascual, E.; Pfenniger, A.; Chkourko Gusky, H.; Novelli, V.; Kim, C.; Tirasawadichai, T.; Judge, D.P.; et al. Missense mutations in plakophilin-2 cause sodium current deficit and associate with a Brugada syndrome phenotype. Circulation 2014, 129, 1092–1103. [Google Scholar] [CrossRef] [PubMed]
- Wichter, T.; Borggrefe, M.; Haverkamp, W.; Chen, X.; Breithardt, G. Efficacy of antiarrhythmic drugs in patients with arrhythmogenic right ventricular disease. Results in patients with inducible and noninducible ventricular tachycardia. Circulation 1992, 86, 29–37. [Google Scholar] [CrossRef]
- Marcus, G.M.; Glidden, D.; Polonsky, B.; Zareba, W.; Smith, L.M.; Cannom, D.S.; Estes, N.M.; Marcus, F.; Scheinman, M.M. Efficacy of Antiarrhythmic Drugs in Arrhythmogenic Right Ventricular Cardiomyopathy. J. Am. Coll. Cardiol. 2009, 54, 609–615. [Google Scholar] [CrossRef]
- Ermakov, S.; Gerstenfeld, E.P.; Svetlichnaya, Y.; Scheinman, M.M. Use of flecainide in combination antiarrhythmic therapy in patients with arrhythmogenic right ventricular cardiomyopathy. Heart Rhythm 2017, 14, 564–569. [Google Scholar] [CrossRef]
- Ermakov, S.; Hoffmayer, K.S.; Gerstenfeld, E.P.; Scheinman, M.M. Combination drug therapy for patients with intractable ventricular tachycardia associated with right ventricular cardiomyopathy. Pacing Clin. Electrophysiol. 2014, 37, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Cappelletto, C.; Gregorio, C.; Barbati, G.; Romani, S.; De Luca, A.; Merlo, M.; Mestroni, L.; Stolfo, D.; Sinagra, G. Antiarrhythmic therapy and risk of cumulative ventricular arrhythmias in arrhythmogenic right ventricle cardiomyopathy. Int. J. Cardiol. 2021, 334, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Rolland, T.; Badenco, N.; Maupain, C.; Duthoit, G.; Waintraub, X.; Laredo, M.; Himbert, C.; Frank, R.; Hidden-Lucet, F.; Gandjbakhch, E. Safety and efficacy of flecainide associated with beta-blockers in arrhythmogenic right ventricular cardiomyopathy. EP Eur. 2021, 24, 278–284. [Google Scholar]
- Wu, H.Y.; Cao, Y.W.; Gao, T.J.; Fu, J.L.; Liang, L. Arrhythmogenic right ventricular cardiomyopathy characterized by recurrent syncope during exercise: A case report. World J. Clin. Cases 2021, 9, 4095–4103. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.Q.; Wang, C.; Li, X.M.; Wang, H. Propafenone-Induced QRS Widening in a Child with Arrhythmogenic Right Ventricular Cardiomyopathy: A Case Report and Literatures Review. Front. Pediatr. 2020, 8, 481330. [Google Scholar] [CrossRef] [PubMed]
- Saikawa, T.; Niwa, H.; Nakamura, S.; Takakura, T.; Nakagawa, M.; Fukuoka, Y.; Tamura, M.; Yonemochi, H.; Ito, S.; Takaki, R. A Case of Arrhythmogenic Right Ventricular Dysplasia with Prominent Late Potential. Jpn. Heart J. 1988, 29, 107–113. [Google Scholar] [CrossRef]
- Honda, T.; Kanai, Y.; Ohno, S.; Ando, H.; Honda, M.; Niwano, S.; Ishii, M. Fetal arrhythmogenic right ventricular cardiomyopathy with double mutations in TMEM43. Pediatr. Int. 2016, 58, 409–411. [Google Scholar] [CrossRef]
- Gasperetti, A.; Cappelletto, C.; Carrick, R.; Targetti, M.; Tichnell, C.; Martino, A.; Murray, B.; Compagnucci, P.; Stolfo, D.; Bisson, J.; et al. Association of Premature Ventricular Contraction Burden on Serial Holter Monitoring with Arrhythmic Risk in Patients with Arrhythmogenic Right Ventricular Cardiomyopathy. JAMA Cardiol. 2022, 7, 378–385. [Google Scholar] [CrossRef]
- Ermakov, S.; Scheinman, M. Arrhythmogenic Right Ventricular Cardiomyopathy—Antiarrhythmic Therapy. Arrhythmia Electrophysiol. Rev. 2015, 4, 86. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Chung, F.-P.; Nwe, N.; Hsieh, Y.-C.; Li, C.-H.; Lin, Y.-J.; Chang, S.-L.; Lo, L.-W.; Hu, Y.-F.; Tuan, T.-C.; et al. Impact of Amiodarone Therapy on the Ablation Outcome of Ventricular Tachycardia in Arrhythmogenic Right Ventricular Cardiomyopathy. J. Clin. Med. 2022, 11, 7265. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Wichter et al., (1992) [29] | Marcus et al., (2009) [30] | Erkamov et al., (2017) [31] | Capelletto et al., (2021) [33] | Rolland et al., (2022) [34] | |
|---|---|---|---|---|---|
| Study population/Design | 81 patients. Retrospective and prospective analysis. | 95 patients. Retrospective analysis. | Flecainide combination therapy: n = 8 Case series. | 123 patients. Retrospective analysis. | 100 patients. Retrospective analysis. |
| Cohort characteristic/Diagnosis | Proven or highly suspected. EMB proven (54.7%). | Definite ARVC with ICD (100%). | Definite ARVC (100%). | Definite ARVC (100%). 36% with ICD. | Definite ARVC (86%). Borderline ARVC (14%). PKP2 mutation (38%). |
| Duration | 34 ± 25 months (inducible cohort) 14 ± 13 months (non-inducible cohort). | 480+/−389 days. | NA—case series. | 132 months range (61–255 months). | 47 months (IQR 23–73). |
| Medications examined: | Multiple: Sotalol, Amiodarone, β-blocker, Verapamil, Class 1a/b (grouped), Class c (grouped), combination therapy. | β-blocker (n = 58), Sotalol (n = 38), Amiodarone (n = 10). | Flecainide & Sotalol (n = 5/8), Flecainide & Metoprolol (n = 3/8). | β-blocker, Sotalol, Amiodarone. | Flecainide (n = 100) with β-blocker (n = 91). |
| Endpoint: | IVT cohort (42/81): Complete response: No VT inducibility. Partial response: more difficult to stimulate > 2 steps in basic drive. Failure: unchanged or spontaneous recurrence. Non-IVT cohort (39/81): 48-h Holter guided therapy and symptom-limited treadmill testing. Complete response: 100% suppression of sVT, nsVT, v-runs, ≥70% reduction in couplets/PVCs. Partial: 100% sVT, nsVT suppression but with ≥70–99% v-runs suppression and >70% reduction in couplets/PVCs. Failure: <100% sVT +/− nsVT suppression OR <70% v-runs reduction OR <70% couplets/PVC reduction. | Clinically relevant arrhythmia (sustained VT/VF requiring ICD ATP or shock), first clinically relevant arrhythmia or first ICD shock. | Ventricular arrhythmia/ICD-shock-free period. | Primary endpoint: Composite of SCD or MVA (sudden cardiac arrest/sustained VT/appropriate ICD intervention) including recurrent MVA in patients >1 MVA. Secondary endpoint: Time to first event (SCD/first MVA). | Sustained VA (VT/VF >30 s) or ICD therapy. PVC burden. PVS. |
| Efficacy/Outcomes: | IVT (1) Sotalol response: complete 22/38 (57.9%), partial 4/35, overall 26/38 (68.4%). (2) Amiodarone response: complete 2/13 (15.4%), partial 0/13, overall 2/13 (15.4%). (3) Verapamil response: overall 0/5 (0%) (4) β-blocker response 0/7 (0%) (5) Class 1a/b response: complete 0/18, partial 1/18, overall (5.6%) 6) Class 1c response: complete 1/25 (4%), partial 2/25, overall 3/25 (12%) 7) Combination therapy: Two class 1 drugs: 0/5 (0%) Class 1 + β-blocker: 0/7 (0%) Class 1 + sotalol: complete 2/10, partial 0/10, overall 2/10 (20%) Class 1 + amiodarone: complete 0/4 (0%), partial 2/4, overall 2/4 (50%). Non-IVT (1) Sotalol response: complete 23/35 (65.7%), partial 6/35, overall 29/35 (82.8%). (2) Amiodarone response: complete 0/4 (0%), partial 1/4, overall 1/4 (25%). (3) Verapamil response: complete 7/24 (29.2%), partial 5/24, overall 12/24 (50%) (4) β-blocker response: complete 0/7 (0%), partial 2/7, overall 2/7 (28.6%) (5) Class 1a/b response: overall 0/16 (0%) (6) Class 1c response: complete 1/23 (4.4%), partial 3/23, overall 4/23 (17.4%) (7) Combination therapy: Two class 1 drugs: 0/5 (0%) Class 1 + β-blocker: 0/7 (0%) Class 1 + sotalol: overall 0/10 (0%) Class 1 + amiodarone: complete 0/2 (0%), partial 1/2, overall 1/2 (50%). | Overall VA event rate: 25% event rate per patient-year. Clinically relevant arrhythmia: (1) β-blocker: HR 1.75, 95% CI (0.48–6.37, p = 0.40) (2) Sotalol: HR 2.55, 95% CI (1.02–6.39, p = 0.045) (3) Amiodarone: HR 0.25, 95% CI (0.07–0.95) Any ICD shock: (1) β-blocker: HR 0.54, 95% CI (0.25–1.18, p = 0.12) (2) Sotalol: HR 2.16, 95% CI (1.15–4.07, p = 0.017) (3) Amiodarone: HR 0 (in all the first events occurred in those not taking amiodarone before they occurred in those taking amiodarone) First ICD shock: (1) β-blocker: not associated with reduced risk (2) Sotalol: HR 1.59, 95% CI (0.69–3.63, p = 0.28) (3) Amiodarone: HR 0 | Case (1) 116 months— sotalol/flecainide Case (2) 38 months—sotalol/flecainide Case (3) 46 months—sotalol/flecainide Case (4) 22 months—sotalol/flecainide Case (5) 18 months—metoprolol/flecainide Case (6) sotalol/flecainide—failure within 2 months Case (7) 24 months—metoprolol/flecainide Case (8) metoprolol/flecainide—failure within 2 months | Primary endpoint: β-blocker: HR 0.54, 95% CI (0.13–2.14, p = 0.378) β-blocker (≥50% target dose): HR 0.10, 95% CI (0.02–0.46, p = 0.004) Sotalol: HR 1.55, 95% CI (0.71–3.4. p = 0.269) Amiodarone: HR 0.7, 95% CI (0.25–1.93, p = 0.492) Secondary endpoint: β-blocker: HR 0.82, 95% CI (0.33–2.05, p = 0.669) β-blocker (≥50% target dose): HR 0.42, 95% CI (0.09–1.91, p = 0.260) Sotalol: HR 1.37, 95% CI (0.46–4.15. p = 0.572) Amiodarone: HR 2.63, 95% CI (0.70–9.86, p = 0.151) | Overall VA event rate: <5% per patient-year, 25% at 5 years. PVC burden: available for 46 patients—decrease in 24-h PVC burden under flecainide [median 2370 (IQR 1572–3400) before vs. 415 (97–730), p < 0.0001]. PVS: 33 patients had PVS performed before and after the introduction of flecainide. Among them, 94% (n = 31) had a positive PVS result off-treatment vs. 40% (n = 13) on-treatment (p < 0.001). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaine, S.P.; Calkins, H. Antiarrhythmic Drug Therapy in Arrhythmogenic Right Ventricular Cardiomyopathy. Biomedicines 2023, 11, 1213. https://doi.org/10.3390/biomedicines11041213
Gaine SP, Calkins H. Antiarrhythmic Drug Therapy in Arrhythmogenic Right Ventricular Cardiomyopathy. Biomedicines. 2023; 11(4):1213. https://doi.org/10.3390/biomedicines11041213
Chicago/Turabian StyleGaine, Sean P., and Hugh Calkins. 2023. "Antiarrhythmic Drug Therapy in Arrhythmogenic Right Ventricular Cardiomyopathy" Biomedicines 11, no. 4: 1213. https://doi.org/10.3390/biomedicines11041213