
Urine Dipstick Analysis on Automated Platforms: Is a Reliable Screening Tool for Proteinuria? An Experience from Umberto I Hospital in Rome

 , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
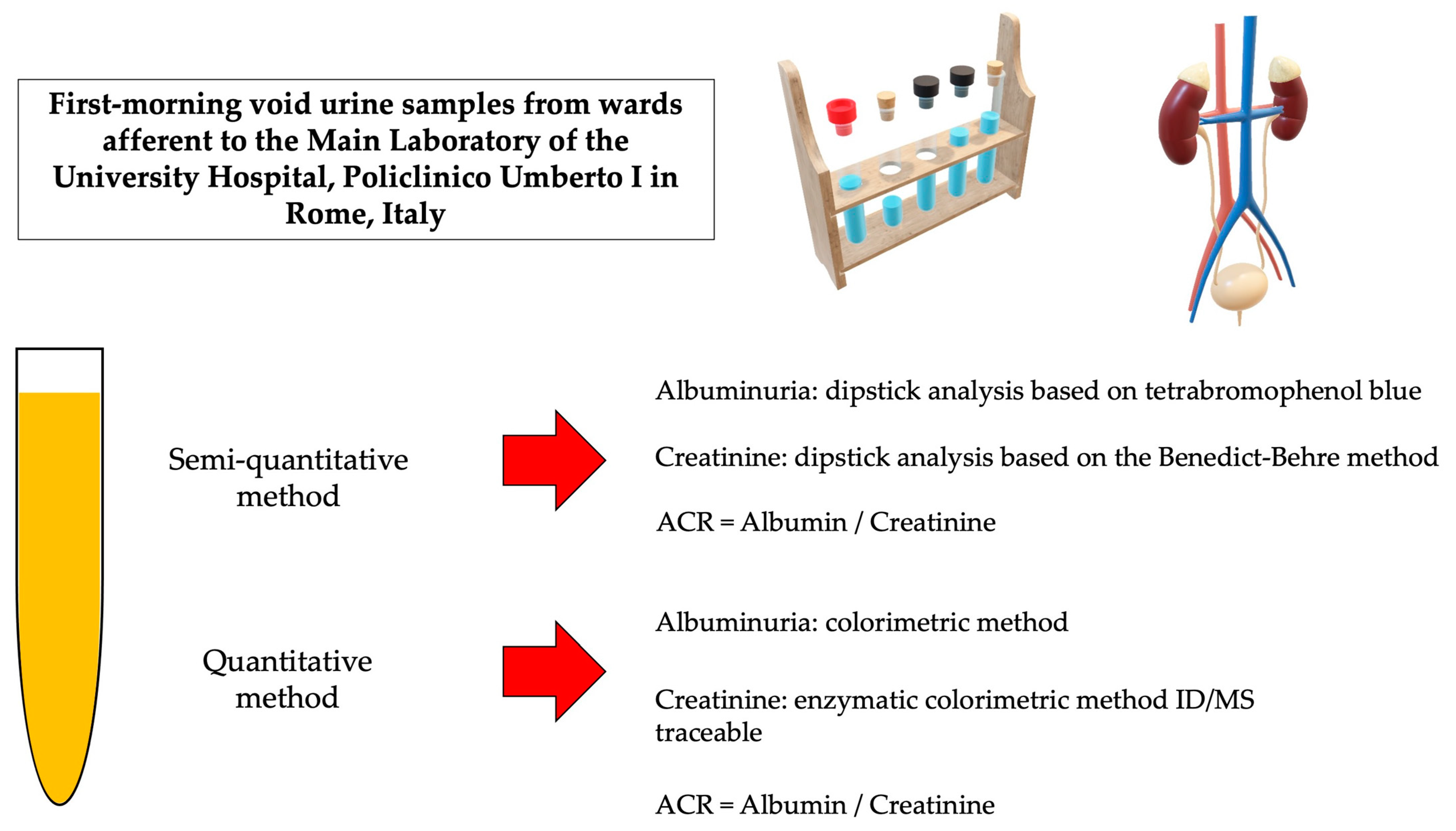
2. Materials and Methods
2.1. Participant’s Selection and Study Design
2.2. Data Collection
2.3. Laboratory Examination
2.4. Statistical Analysis
3. Results
3.1. Comparison between Albumin/Creatinine Ratio Calculated Using the Semi-Quantitative and the Quantitative Methods
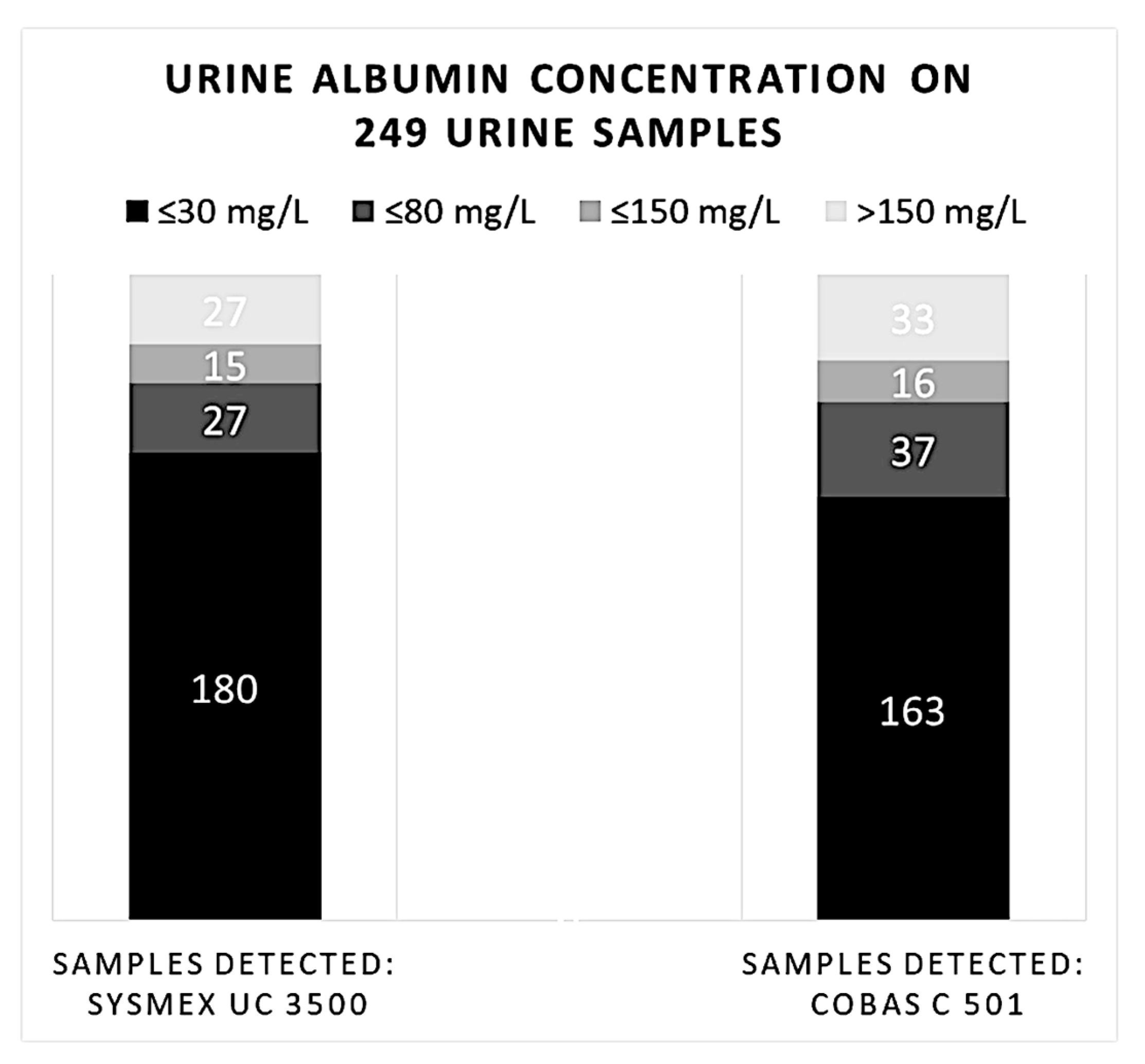
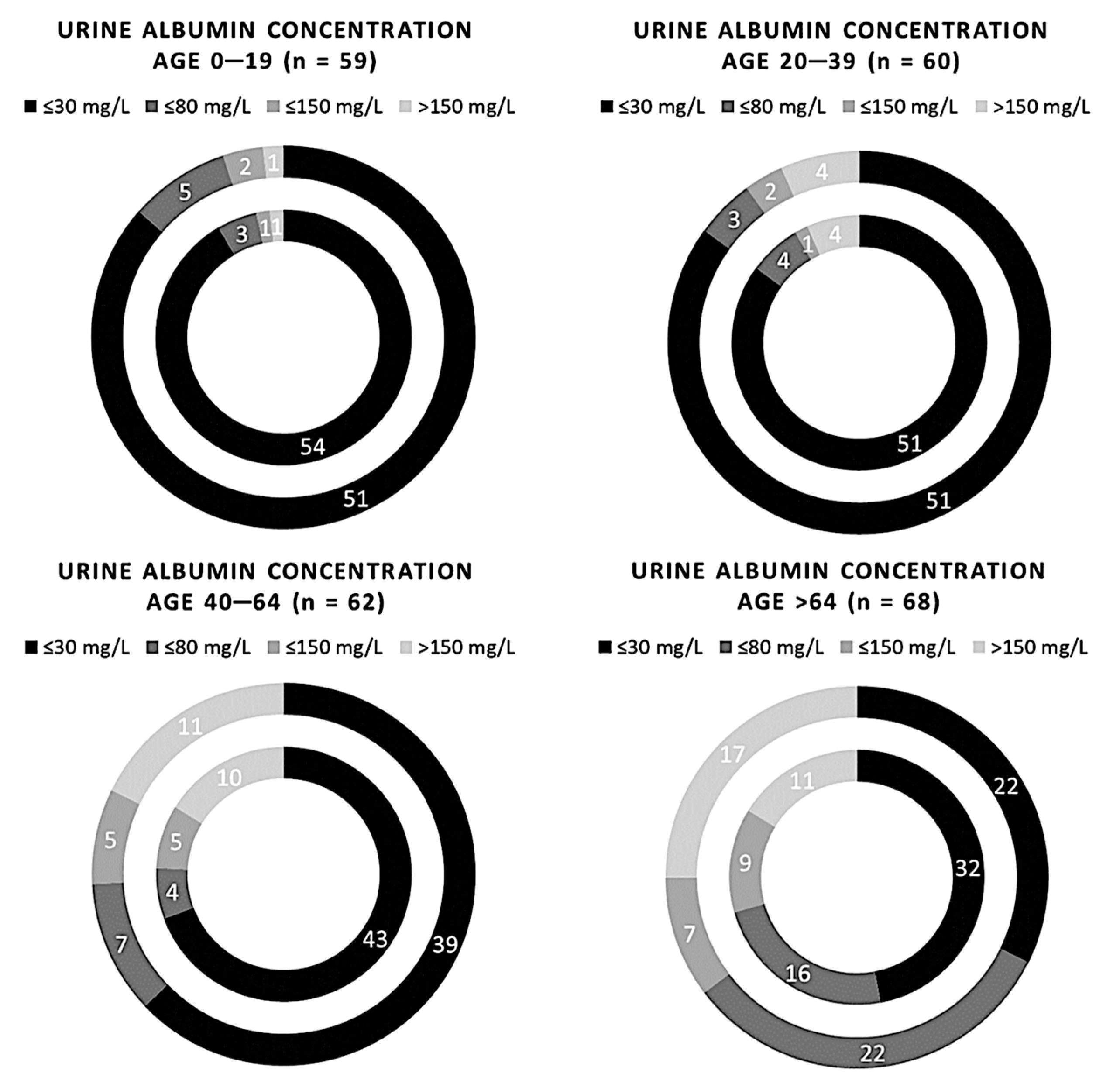
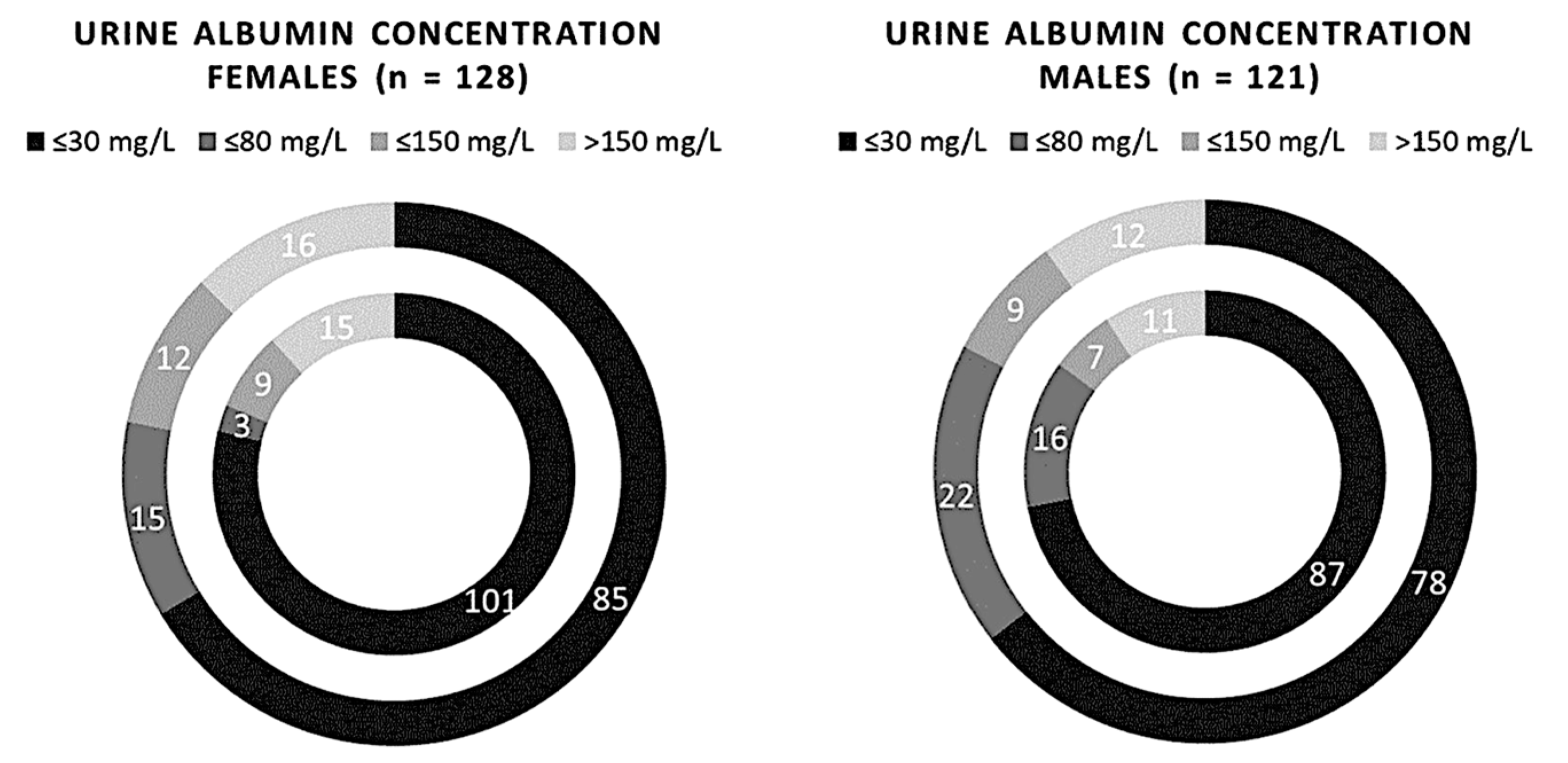
3.2. Comparison between Albuminuria Analyzed Using the Semi-Quantitative and the Quantitative Methods
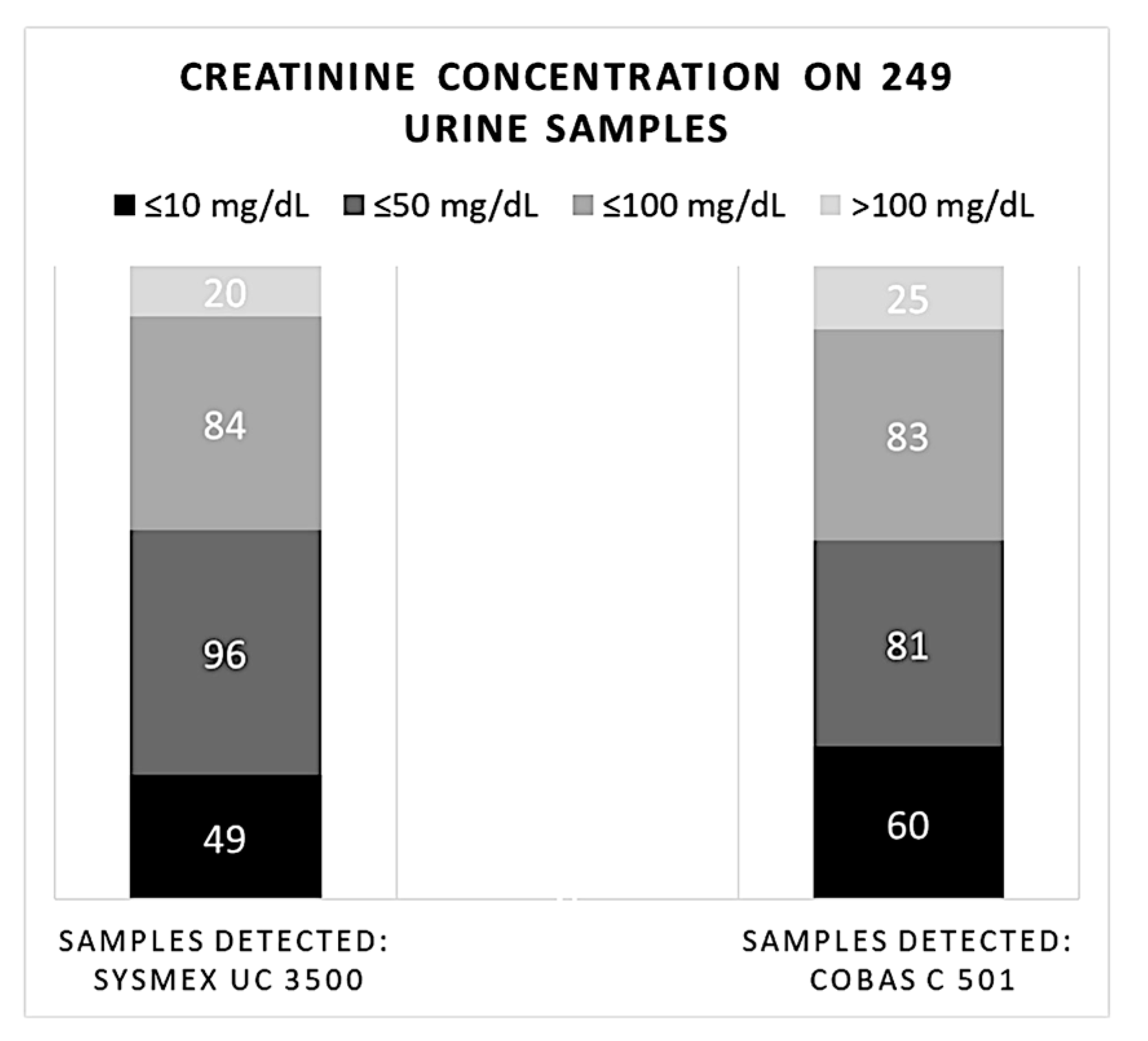
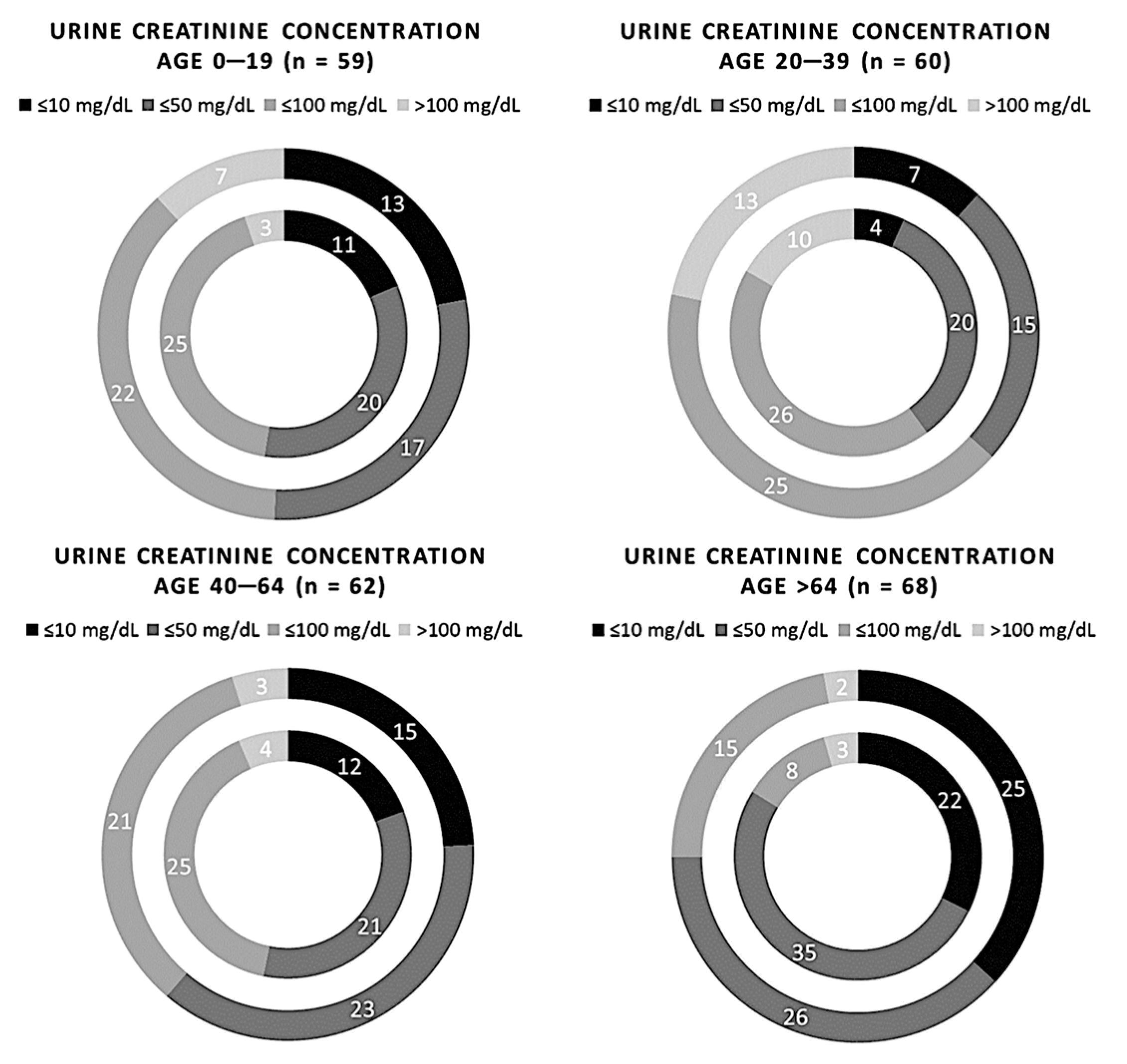
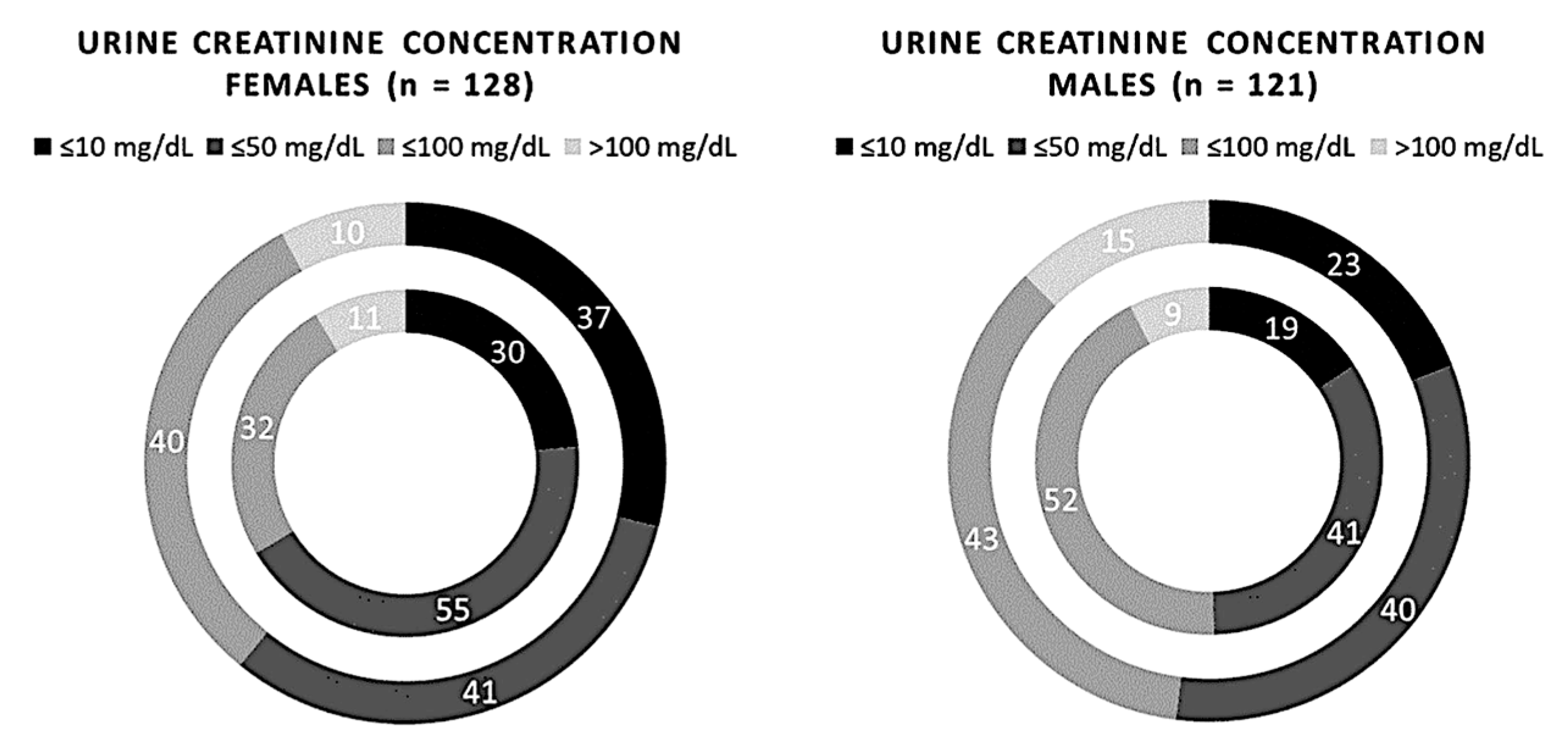
3.3. Comparison between Creatinuria Analyzed Using the Semi-Quantitative and the Quantitative Methods
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lim, S.; Yu, H.J.; Lee, S.; Park, H.; Kwon, M.J.; Woo, H.Y. Evaluation of the URiSCAN 2 ACR Strip to estimate the urine albumin/creatinine ratios. J. Clin. Lab. Anal. 2018, 32, 6–11. [Google Scholar] [CrossRef] [Green Version]
- Mcgrath, K.; Kimmel, S.; College, M. Diabetic kidney ds aafp 2019. Am. Fam. Physician. 2019, 99, 751–759. [Google Scholar]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic kidney disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Cameron, F.J.; Wherrett, D.K. Care of diabetes in children and adolescents: Controversies, changes, and consensus. Lancet 2015, 385, 2096–2106. [Google Scholar] [CrossRef]
- James, M.T.; Hemmelgarn, B.R.; Tonelli, M. Early recognition and prevention of chronic kidney disease. Lancet 2010, 375, 1296–1309. [Google Scholar] [CrossRef]
- Collier, G.; Greenan, M.C.; Brady, J.J.; Murray, B.; Cunningham, S.K. A study of the relationship between albuminuria, proteinuria and urinary reagent strips. Ann. Clin. Biochem. 2009, 46, 247–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heerspink, H.J.L.; Gansevoort, R.T. Albuminuria is an appropriate therapeutic target in patients with CKD: The pro view. Clin. J. Am. Soc. Nephrol. 2015, 10, 1079–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, D.; Lee, D.Y.; Cho, S.H.; Kim, O.Z.; Cho, S.W.; An, S.K.; Kim, H.W.; Moon, K.H.; Lee, M.H.; Kim, B. Diagnostic accuracy of urine dipstick for proteinuria in older outpatients. Kidney Res. Clin. Pract. 2014, 33, 199–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guy, M.; Borzomato, J.K.; Newall, R.G.; Kalra, P.A.; Price, C.P. Protein and albumin-to-creatinine ratios in random urines accurately predict 24 h protein and albumin loss in patients with kidney disease. Ann. Clin. Biochem. 2009, 46, 468–476. [Google Scholar] [CrossRef] [Green Version]
- Witte, E.C.; Heerspink, H.J.L.; De Zeeuw, D.; Bakker, S.J.L.; De Jong, P.E.; Gansevoort, R. First morning voids are more reliable than spot urine samples to assess microalbuminuria. J. Am. Soc. Nephrol. 2009, 20, 436–443. [Google Scholar] [CrossRef] [Green Version]
- Erman, A.; Rahamimov, R.; Mashraki, T.; Levy-Drummer, R.S.; Winkler, J.; David, I.; Hirsh, Y.; Gafter, U.; Chagnac, A. The urine albumin-to-creatinine ratio: Assessment of its performance in the renal transplant recipient population. Clin. J. Am. Soc. Nephrol. 2011, 6, 892–897. [Google Scholar] [CrossRef] [Green Version]
- Guy, M.; Newall, R.; Borzomato, J.; Kalra, P.A.; Price, C. Diagnostic accuracy of the urinary albumin: Creatinine ratio determined by the CLINITEK Microalbumin and DCA 2000+ for the rule-out of albuminuria in chronic kidney disease. Clin. Chim. Acta 2009, 399, 54–58. [Google Scholar] [CrossRef]
- Oyaert, M.; Delanghe, J. Progress in automated urinalysis. Ann. Lab. Med. 2018, 39, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.Y.; Hur, M. Advances in automated urinalysis systems, flow cytometry and digitized microscopy. Ann. Lab. Med. 2018, 39, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Delanghe, J.R.; Himpe, J.; De Cock, N.; Delanghe, S.; De Herde, K.; Stove, V.; Speeckaert, M.M. Sensitive albuminuria analysis using dye-binding based test strips. Clin. Chim. Acta 2017, 471, 107–112. [Google Scholar] [CrossRef]
- White, S.L.; Yu, R.; Craig, J.C.; Polkinghorne, K.R.; Atkins, R.C.; Chadban, S.J. Diagnostic accuracy of urine dipsticks for detection of albuminuria in the general community. Am. J. Kidney Dis. 2011, 58, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Parsons, M.; Newman, D.J.; Pugia, M.; Newall, R.G.; Price, C.P. Performance of a reagent strip device for quantitation of the urine albumin: Creatinine ratio in a point of care setting. Clin. Nephrol. 1999, 51, 220–227. [Google Scholar]
- Decavele, A.-S.C.; Fiers, T.; Penders, J.; Delanghe, J.R. A sensitive quantitative test strip based point-of-care albuminuria screening assay. Clin. Chem. Lab. Med. 2012, 50, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Serarcangeli, C.; Giovenale, A.M. The Rome Policlinico Umberto I: An innovative project. Med. Secoli. 2002, 14, 155–175. [Google Scholar]
- Ferraguti, G.; Merlino, L.; Battagliese, G.; Piccioni, M.G.; Barbaro, G.; Carito, V.; Messina, M.P.; Scalese, B.; Coriale, G.; Fiore, M.; et al. Fetus morphology changes by second-trimester ultrasound in pregnant women drinking alcohol. Addict. Biol. 2020, 25, e12724. [Google Scholar] [CrossRef] [PubMed]
- Ferraguti, G.; Ciolli, P.; Carito, V.; Battagliese, G.; Mancinelli, R.; Ciafrè, S.; Tirassa, P.; Ciccarelli, R.; Cipriani, A.; Messina, M.P.; et al. Ethylglucuronide in the urine as a marker of alcohol consumption during pregnancy: Comparison with four alcohol screening questionnaires. Toxicol. Lett. 2017, 275, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Angelucci, F.; Piermaria, J.; Gelfo, F.; Shofany, J.; Tramontano, M.; Fiore, M.; Caltagirone, C.; Peppe, A. The effects of motor rehabilitation training on clinical symptoms and serum BDNF levels in parkinson’s disease subjects. Can. J. Physiol. Pharmacol. 2016, 94, 455–461. [Google Scholar] [CrossRef] [Green Version]
- Currin, S.D.; Gondwe, M.S.; Mayindi, N.B.; Chipungu, S.; Khoza, B.L.; Tollman, S.; Fabian, J.; George, J.A. Diagnostic accuracy of semiquantitative point of care urine albumin to creatinine ratio and urine dipstick analysis in a primary care resource limited setting in South Africa. BMC Nephrol. 2021, 22, 103. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Song, S.A.; Jun, K.R.; Lee, J.N. Performance evaluation of MEDITAPE UC-11A strip test in estimating the urine albumin-to-creatinine ratio and urine protein-to-creatinine ratio. Lab. Med. Online 2020, 10, 52. [Google Scholar] [CrossRef]
- Kondo, M.; Yamagata, K.; Hoshi, S.L.; Saito, C.; Asahi, K.; Moriyama, T.; Tsuruya, K.; Yoshida, H.; Iseki, K.; Watanabe, T. Cost-effectiveness of chronic kidney disease mass screening test in Japan. Clin. Exp. Nephrol. 2012, 16, 279–291. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Yang, L.; Wang, F.; Zhang, L. Strategies and cost-effectiveness evaluation of persistent albuminuria screening among high-risk population of chronic kidney disease. BMC Nephrol. 2017, 18, 135. [Google Scholar] [CrossRef] [Green Version]
- Boulware, L.E.; Jaar, B.G.; Tarver-Carr, M.E.; Brancati, F.L.; Powe, N.R. Screening for proteinuria in US adults: A cost-effectiveness analysis. J. Am. Med. Assoc. 2003, 290, 3101–3114. [Google Scholar] [CrossRef] [Green Version]
- Crews, D.C.; Boulware, L.E.; Gansevoort, R.T.; Jaar, B.G. Albuminuria: Is it time to screen the general population? Adv. Chronic. Kidney Dis. 2011, 18, 249–257. [Google Scholar] [CrossRef]
- Anavekar, N.S.; Gans, D.J.; Berl, T.; Rohde, R.D.; Cooper, W.; Bhaumik, A.; Hunsicker, L.G.; Rouleau, J.L.; Lewis, J.B.; Rosendorff, C.; et al. Predictors of cardiovascular events in patients with type 2 diabetic nephropathy and hypertension: A case for albuminuria. Kidney Int. Suppl. 2004, 66, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Webb, D.R.; Zaccardi, F.; Davies, M.J.; Griffin, S.J.; Wareham, N.J.; Simmons, R.K.; Rutten, G.E.; Sandbaek, A.; Lauritzen, T.; Borch-Johnsen, K.; et al. Cardiovascular risk factors and incident albuminuria in screen-detected type 2 diabetes. Diabetes Metab. Res. Rev. 2017, 33, e2877. [Google Scholar] [CrossRef]
- Kahkoska, A.R.; Isom, S.; Divers, J.; Mayer-Davis, E.J.; Dolan, L.; Shah, A.S.; Afkarian, M.; Pettitt, D.J.; Lawrence, J.M.; Marcovina, S.; et al. The early natural history of albuminuria in young adults with youth-onset type 1 and type 2 diabetes. J. Diabetes Complicat. 2018, 32, 1160–1168. [Google Scholar] [CrossRef]
- Weir, M.R. Albuminuria predicting outcome in diabetes: Incidence of microalbuminuria in Asia-Pacific Rim. Kidney Int. Suppl. 2004, 66, 38–39. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, L.; Milne, E.; Waite, N.; Cooke, M.; Cook, K.; Chang, F.; Sproule, B.A. Sex and gender-based analysis in pharmacy practice research: A scoping review. Res. Soc. Adm. Pharm. 2017, 13, 1045–1054. [Google Scholar] [CrossRef] [PubMed]
- Lebensburger, J.D.; Aban, I.; Pernell, B.; Kasztan, M.; Feig, D.I.; Hilliard, L.M.; Askenazi, D.J. Hyperfiltration during early childhood precedes albuminuria in pediatric sickle cell nephropathy. Am. J. Hematol. 2019, 94, 417–423. [Google Scholar] [CrossRef] [Green Version]
- Matsushita, K.; van der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; de Jong, P.E. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 2010, 375, 2073–2081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jong, P.E.; Curhan, G.C. Screening, monitoring, and treatment of albuminuria: Public health perspectives. J. Am. Soc. Nephrol. 2006, 17, 2120–2126. [Google Scholar] [CrossRef] [Green Version]
- Kuritzky, L.; Toto, R.; Van Buren, P. Identification and management of albuminuria in the primary care setting. J. Clin. Hypertens. 2011, 13, 438–449. [Google Scholar] [CrossRef]
- De Jong, P.E.; Brenner, B.M. From secondary to primary prevention of progressive renal disease: The case for screening for albuminuria. Kidney Int. 2004, 66, 2109–2118. [Google Scholar] [CrossRef] [Green Version]
- de Zeeuw, D. Albuminuria: A target for treatment of type 2 diabetic nephropathy. Semin. Nephrol. 2007, 27, 172–181. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hospital Departments | n (249) | AGE | M/F |
|---|---|---|---|
| Occupational Medicine | 22 | 35 (28–60) | 7/15 |
| Gastroenterology | 5 | 58 (30–74) | 4/1 |
| Daily Surgery | 1 | 46 | 0/1 |
| Transplants | 31 | 54 (4–74) | 22/9 |
| Cardiology | 5 | 71 (56–90) | 3/2 |
| Intensive Care Unit | 5 | 50 (35–60) | 4/1 |
| Neurosurgery | 11 | 57 (25–87) | 8/3 |
| Pediatrics | 58 | 13 (1–24) | 27/31 |
| Radiotherapy | 2 | 80 (72–88) | 2/0 |
| Infectious Diseases | 19 | 67 (45–87) | 11/8 |
| Internal Medicine | 30 | 69 (14–96) | 12/18 |
| Pneumology | 8 | 58 (30–89) | 6/2 |
| Clinical Immunology | 3 | 64 (38–84) | 3/0 |
| Diabetology and Obesity | 5 | 17 (7–29) | 3/2 |
| Tropical Diseases | 3 | 67 (49–89) | 1/2 |
| Rheumatology | 11 | 66 (29–92) | 2/9 |
| Geriatrics | 2 | 76 (70–81) | 2/0 |
| Physical Medicine and Rehabilitation | 2 | 83 (82–84) | 0/2 |
| Nephrology | 1 | 35 | 0/1 |
| Gynecology and Obstetrics | 18 | 33 (23–53) | 0/18 |
| Neurology | 2 | 87 (82–92) | 1/1 |
| Laboratory External Users | 5 | 52 (34–62) | 3/2 |
| Patient n. | Sex M/F | Age | Ratio Sysmex | Ratio Cobas (mg/g) |
|---|---|---|---|---|
| 15 | 6/9 | 34 (1–81) | ND | <30 |
| 9 | 5/4 | 47 (11–90) | ND | 30–300 |
| 2 | F | 85 (74–96) | ND | >300 |
| Ratio Range (mg/g) | Sysmex UC 3500 (n) | Cobas C 501 (n) |
|---|---|---|
| <30 | 107 | 141 |
| 30–300 | 68 | 58 |
| >300 | 48 | 24 |
| Tot. | 223 | 223 |
| Age | Sysmex UC 3500 (mg/g→n) | Cobas C 501 (mg/g→n) |
|---|---|---|
| 0–19 (n = 50) | <30→33 30–300→16 >300→1 | <30→44 30–300→5 >300→1 |
| 20–39 (n = 56) | <30→35 30–300→17 >300→4 | <30→48 30–300→6 >300→2 |
| 40–64 (n = 56) | <30→26 30–300→13 >300→17 | <30→32 30–300→12 >300→12 |
| >64 (n = 61) | <30→13 30–300→22 >300→26 | <30→17 30–300→35 >300→9 |
| Sex | Sysmex UC 3500 (mg/g→n) | Cobas C 501 (mg/g→n) |
|---|---|---|
| Female (n = 113) | <30→56 30–300→27 >300→30 | <30→73 30–300→27 >300→13 |
| Male (n = 110) | <30→51 30–300→41 >300→18 | <30→68 30–300→30 >300→12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terracina, S.; Pallaria, A.; Lucarelli, M.; Angeloni, A.; De Angelis, A.; Ceci, F.M.; Caronti, B.; Francati, S.; Blaconà, G.; Fiore, M.; et al. Urine Dipstick Analysis on Automated Platforms: Is a Reliable Screening Tool for Proteinuria? An Experience from Umberto I Hospital in Rome. Biomedicines 2023, 11, 1174. https://doi.org/10.3390/biomedicines11041174
Terracina S, Pallaria A, Lucarelli M, Angeloni A, De Angelis A, Ceci FM, Caronti B, Francati S, Blaconà G, Fiore M, et al. Urine Dipstick Analysis on Automated Platforms: Is a Reliable Screening Tool for Proteinuria? An Experience from Umberto I Hospital in Rome. Biomedicines. 2023; 11(4):1174. https://doi.org/10.3390/biomedicines11041174
Chicago/Turabian StyleTerracina, Sergio, Antonio Pallaria, Marco Lucarelli, Antonio Angeloni, Annarita De Angelis, Flavio Maria Ceci, Brunella Caronti, Silvia Francati, Giovanna Blaconà, Marco Fiore, and et al. 2023. "Urine Dipstick Analysis on Automated Platforms: Is a Reliable Screening Tool for Proteinuria? An Experience from Umberto I Hospital in Rome" Biomedicines 11, no. 4: 1174. https://doi.org/10.3390/biomedicines11041174