
Endothelial Function and Hypoxic–Hyperoxic Preconditioning in Coronary Surgery with a Cardiopulmonary Bypass: Randomized Clinical Trial
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
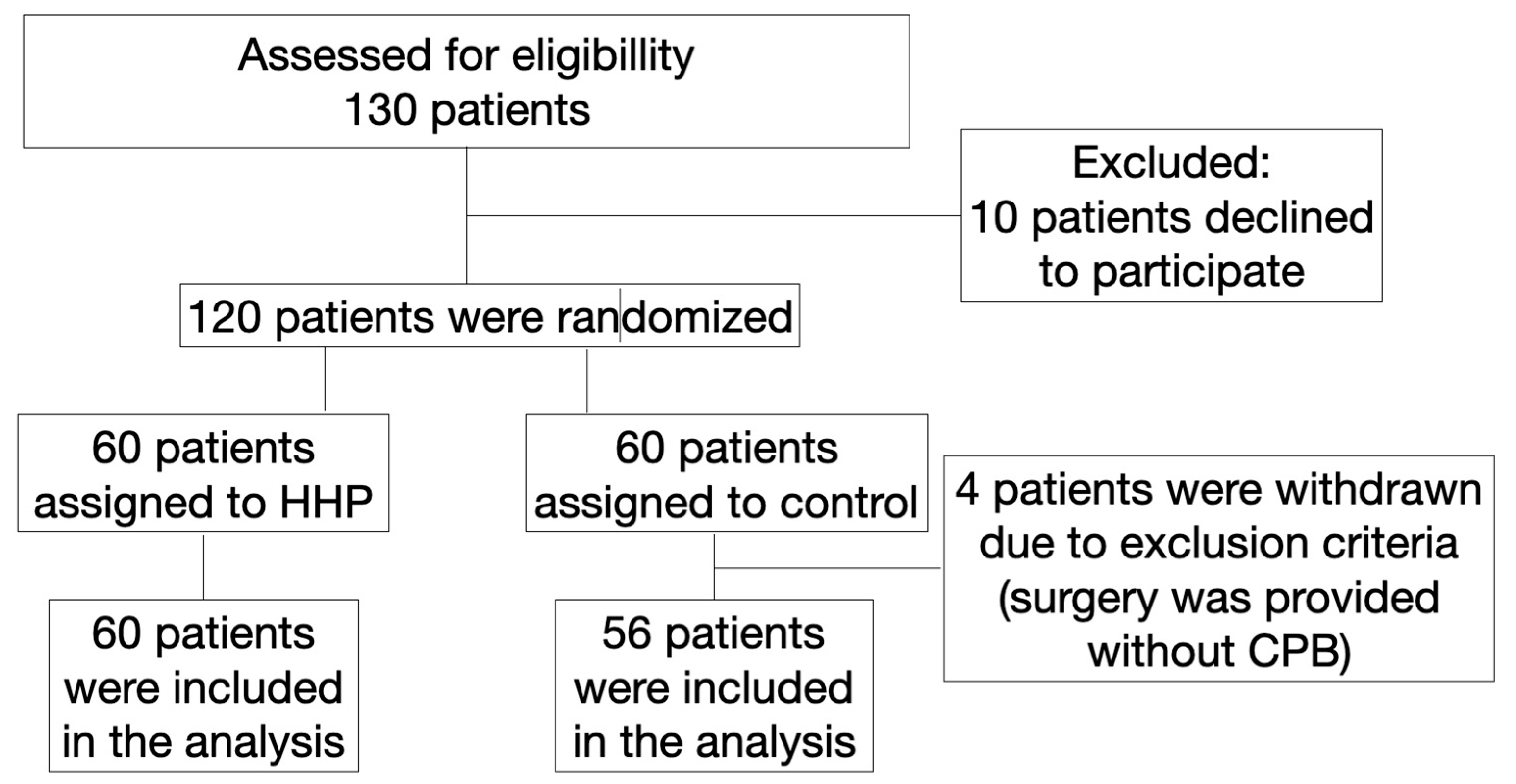
2.1. Study Design
2.2. The Anaerobic Threshold Measurement
2.3. Anesthesia and Hypoxic–Hyperoxic Preconditioning Procedure
2.4. Perioperative Monitoring
2.5. The Weaning Procedure from Mechanical Ventilation
2.6. Oxygen Transport Characteristics
Oxygen Balance Formulas
2.7. Endothelial Damage Markers
2.8. Cardiac Troponin T
2.9. Intragastric pH-Metry
2.10. Outcomes
2.11. Statistical Analysis
3. Results
3.1. Preoperative Characteristics of the Patients
3.2. Intraoperative Characteristics of the Patients
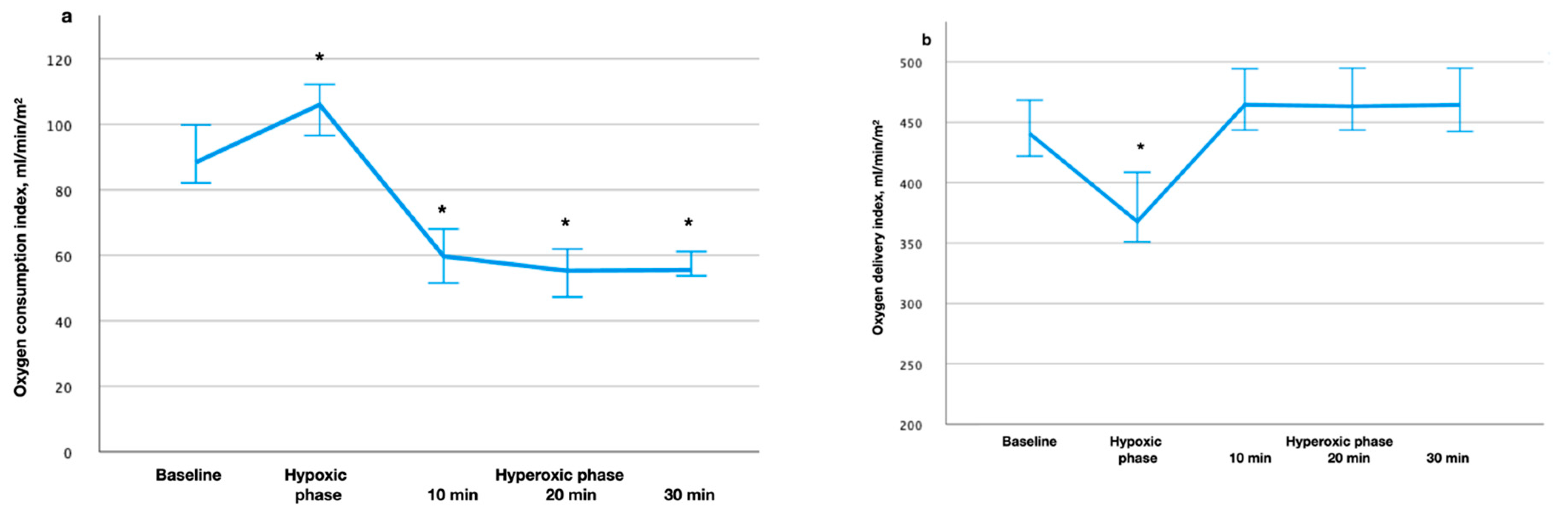
3.3. Oxygen Balance Characteristics during Hypoxic–Hyperoxic Preconditioning
3.4. The Dynamics of Endothelial Damage Markers in Blood Plasma
The Endothelial Damage Markers as Predictors of Postoperative Complications
3.5. Heart Rhythm Restoration after Cardiopulmonary Bypass
3.6. The Characteristics of the Postoperative Period
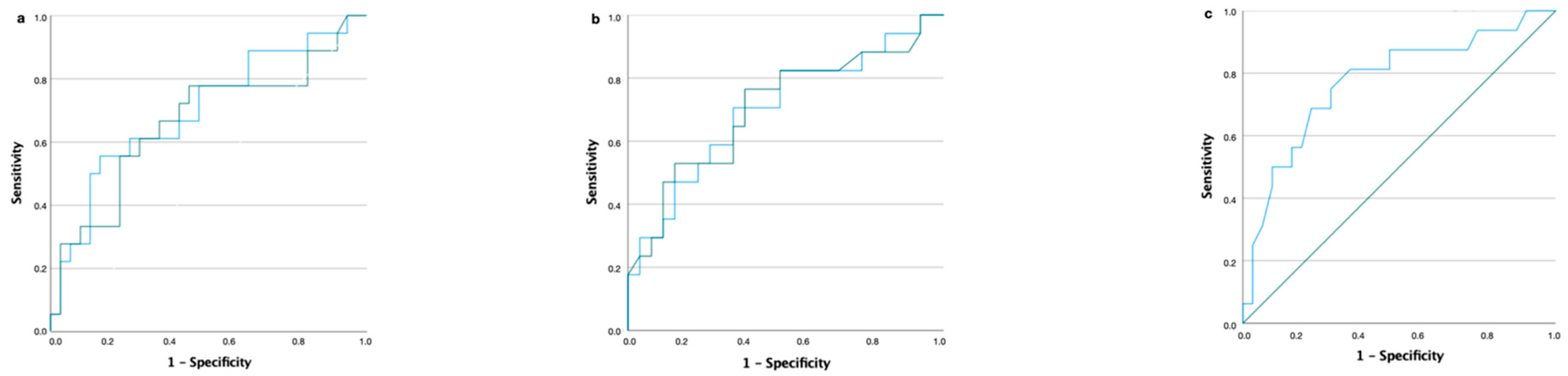
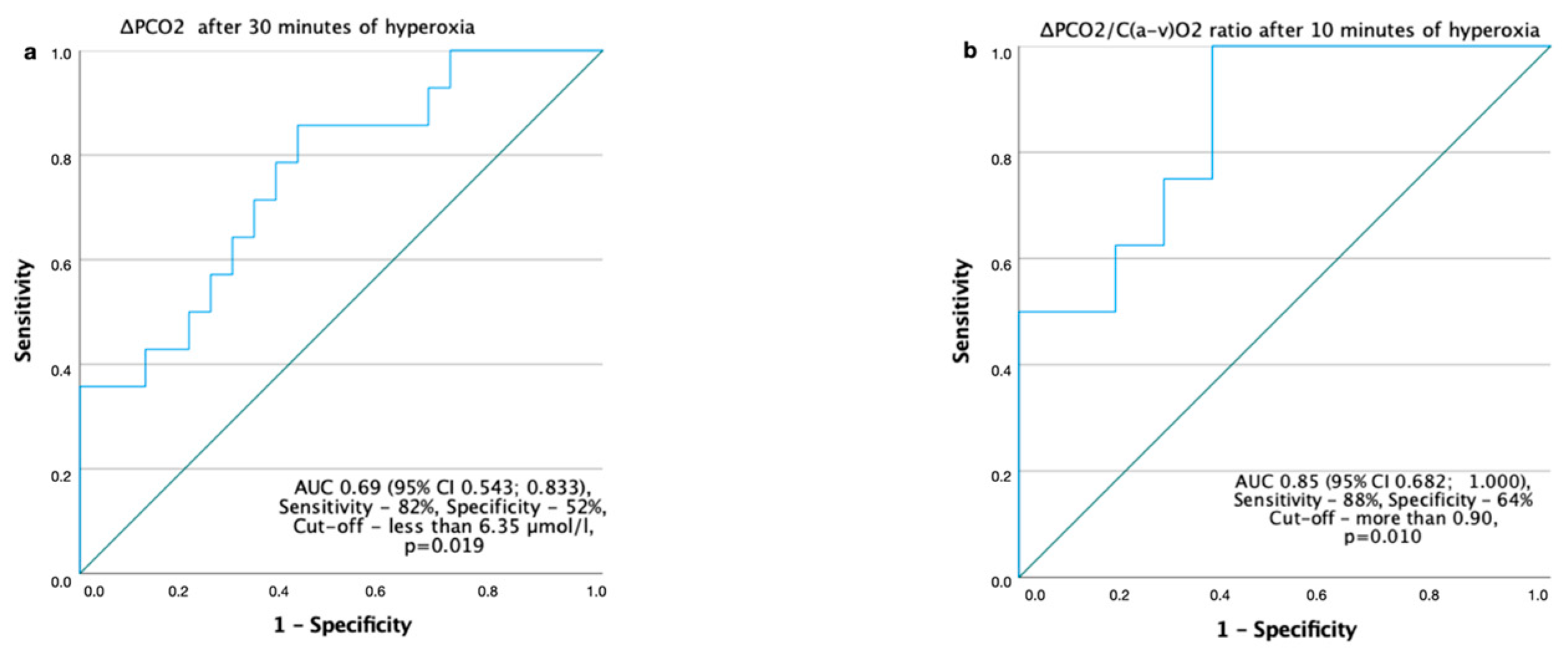
3.7. Relationship between the ΔPCO2, the p(v-a)CO2/C(a-v)O2 Ratio and Outcome in the HHP Group
4. Discussion
4.1. Possible Mechanism of Hypoxic–Hyperoxic Preconditioning
4.2. Monitoring and Modulation of Tissue Perfusion
4.3. Chronic Heart Failure and Hyperoxia
4.4. The ET-1 and NO Metabolites in the Perioperative Period
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deng, Q.W.; Xia, Z.Q.; Qiu, Y.X.; Wu, Y.; Liu, J.X.; Li, C.; Liu, K.X. Clinical benefits of aortic cross-clamping versus limb remote ischemic preconditioning in coronary artery bypass grafting with cardiopulmonary bypass: A meta-analysis of randomized controlled trials. J. Surg. Res. 2015, 193, 52–68. [Google Scholar] [CrossRef]
- Fischesser, D.M.; Bo, B.; Benton, R.P.; Su, H.; Jahanpanah, N.; Haworth, K.J. Controlling Reperfusion Injury With Controlled Reperfusion: Historical Perspectives and New Paradigms. J. Cardiovasc. Pharmacol. Ther. 2021, 26, 504–523. [Google Scholar] [CrossRef] [PubMed]
- Hancock, J.T. A Brief History of Oxygen: 250 Years on. Oxygen 2022, 2, 31–39. [Google Scholar] [CrossRef]
- Plicner, D.; Stolinski, J.; Wasowicz, M.; Gaweda, B.; Hymczak, H.; Kapelak, B.; Drwiła, R.; Undas, A. Preoperative values of inflammatory markers predict clinical outcomes in patients after CABG, regardless of the use of cardiopulmonary bypass. Indian Heart J. 2016, 68 (Suppl. S3), S10–S15. [Google Scholar] [CrossRef] [Green Version]
- Hausenloy, D.J.; Chilian, W.; Crea, F.; Davidson, S.M.; Ferdinandy, P.; Garcia-Dorado, D.; van Royen, N.; Schulz, R.; Heusch, G. The coronary circulation in acute myocardial ischaemia/reperfusion injury: A target for cardioprotection. Cardiovasc. Res. 2019, 115, 1143–1155. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Lamanna, J.C. Short-term hypoxic preconditioning improved survival following cardiac arrest and resuscitation in rats. Adv. Exp. Med. Biol. 2014, 812, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Petrosillo, G.; Di Venosa, N.; Moro, N.; Colantuono, G.; Paradies, V.; Tiravanti, E.; Federici, A.; Ruggiero, F.M.; Paradies, G. In vivo hyperoxic preconditioning protects against rat-heart ischemia/reperfusion injury by inhibiting mitochondrial permeability transition pore opening and cytochrome c release. Free Radic. Biol. Med. 2011, 50, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Sanada, S.; Komuro, I.; Kitakaze, M. Pathophysiology of myocardial reperfusion injury: Preconditioning, postconditioning, and translational aspects of protective measures. Am. J. Physiol. Heart Circ. Physiol. 2011, 301, H1723–H1741. [Google Scholar] [CrossRef] [Green Version]
- Tähepõld, P.; Ruusalepp, A.; Li, G.; Vaage, J.; Starkopf, J.; Valen, G. Cardioprotection by breathing hyperoxic gas-relation to oxygen concentration and exposure time in rats and mice. Eur. J. Cardiothorac. Surg. 2002, 6, 987–994. [Google Scholar] [CrossRef] [Green Version]
- Parthasarathi, K.; Lipowsky, H.H. Capillary recruitment in response to tissue hypoxia and its dependence on red cell deformability. J. Am. Physiol. 1999, 277, H2145–H2157. [Google Scholar] [CrossRef]
- Yuan, X.; Lee, J.W.; Bowser, J.L.; Neudecker, V.; Sridhar, S.; Eltzschig, H.K. Targeting Hypoxia Signaling for Perioperative Organ Injury. Anesth. Analg. 2018, 126, 308. [Google Scholar] [CrossRef] [PubMed]
- Maslov, L.N.; Lishmanov, Y.B.; Krylatov, A.V.; Sementsov, A.S.; Portnichenko, A.G.; Podoksenov, Y.K.; Khaliulin, I.G. Comparative analysis of early and delayed cardioprotective and antiarrhythmic efficacy of hypoxic preconditioning. Bull. Exp. Biol. Med. 2014, 156, 746–749. [Google Scholar] [CrossRef] [PubMed]
- Kopterides, P.; Kapetanakis, T.; Siempos, I.I.; Magkou, C.; Pelekanou, A.; Tsaganos, T. A Short-term administration of a high oxygen concentration is not injurious in an ex-vivo rabbit model of ventilator-induced lung injury. Anesth. Analg. 2009, 108, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Glazachev, O.; Kopylov, P.; Susta, D.; Dudnik, E.; Zagaynaya, E. Adaptations following an intermittent hypoxia-hyperoxia training in coronary artery disease patients: A controlled study. Clin. Cardiol. 2017, 40, 370–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Pascual, F.; Busnadiego, O.; Lagares, D.; Lamas, S. Role of endothelin in the cardiovascular system. Pharmacol. Res. 2011, 63, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Kolettis, T.M.; Barton, M.; Langleben, D.; Matsumura, Y. Endothelin in coronary artery disease and myocardial infarction. Cardiol. Rev. 2013, 21, 249–256. [Google Scholar] [CrossRef]
- Dorman, B.H.; Kratz, J.M.; Multani, M.M.; Baron, R.; Farrar, E.; Walton, S.; Payne, K.; Ikonomiois, J.; Reeves, S.; Mukherjee, R.; et al. A prospective, randomized study of endothelin and postoperative recovery in off-pump versus conventional coronary artery bypass surgery. J. Cardiothorac. Vasc. Anesth. 2004, 18, 25–29. [Google Scholar] [CrossRef]
- Lincoln, J.; Hoyle, C.H.V.; Burnstock, G. Nitric Oxide in Health and Disease. In Biomedical Research Topics (1) American Scientist; Cambridge University Press: Cambridge, UK, 1997; p. 363. ISBN 9780521559775. [Google Scholar]
- Schwedhelm, E.; Boger, R.H. The role of asymmetric and symmetric dimethylarginines in renal disease. Nat. Rev. Nephrol. 2011, 7, 275–285. [Google Scholar] [CrossRef]
- Konya, H.; Miuchi, M.; Satani, K.; Matsutani, S.; Yano, Y.; Tsunoda, T.; Ikawa, T.; Matsuo, T.; Ochi, F.; Kusunoki, Y.; et al. Asymmetric dimethylarginine, a biomarker of cardiovascular complications in diabetes mellitus. World J. Exp. Med. 2015, 5, 110–119. [Google Scholar] [CrossRef]
- Shechter, M.; Matetzky, S.; Arad, M.; Feinberg, M.S.; Freimark, D. Vascular endothelial function predicts mortality risk in patients with advanced ischaemic chronic heart failure. Eur. J. Heart Fail. 2009, 11, 588–593. [Google Scholar] [CrossRef]
- Young, R.W. Hyperoxia: A review of the risks and benefits in adult cardiac surgery. J. Extra-Corpor. Technol. 2012, 44, 241. [Google Scholar] [PubMed]
- Thielmann, M.; Sharma, V.; Al-Attar, N.; Bulluck, H.; Bisleri, G.; Bunge, J.J.H.; Czerny, M.; Ferdinandy, P.; Frey, U.H.; Heusch, G.; et al. ESC Joint Working Groups on Cardiovascular Surgery and the Cellular Biology of the Heart Position Paper: Perioperative myocardial injury and infarction in patients undergoing coronary artery bypass graft surgery. Eur. Heart J. 2017, 38, 2392–2407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandel, I.A.; Mikheev, S.L.; Podoksenov, Y.K.; Svirko, Y.S.; Suhodolo, I.V.; Shipulin, V.M. Hypoxic-hyperoxic preconditioning: A novel technique for myocardial protection against ischemia-reperfusion injury in coronary surgery. Eur. Heart J. 2017, 38, ehx493.P5809. [Google Scholar] [CrossRef]
- Mandel, I.A.; Podoksenov, Y.K.; Suhodolo, I.V.; An, D.A.; Mikheev, S.L.; Podoksenov, A.Y.; Svirko, Y.S.; Gusakova, A.M.; Shipulin, V.M.; Yavorovskiy, A.G. Influence of Hypoxic and Hyperoxic Preconditioning on Endothelial Function in a Model of Myocardial Ischemia-Reperfusion Injury with Cardiopulmonary Bypass (Experimental Study). Int. J. Mol. Sci. 2020, 21, 5336. [Google Scholar] [CrossRef] [PubMed]
- Helmerhorst, H.J.F.; Schultz, M.J.; van der Voort, P.H.; de Jonge, E.; van Westerloo, D.J. Bench-to-bedside review: The effects of hyperoxia during critical illness. Crit. Care 2015, 19, 284. [Google Scholar] [CrossRef] [Green Version]
- Rocco, M.; D’Itri, L.; De Bels, D.; Corazza, F.; Balestra, C. The “normobaric oxygen paradox”: A new tool for the anesthetist? Minerva Anestesiol. 2014, 80, 366–372. [Google Scholar]
- Guyton, A.C.; Hall, J.E. Textbook of Medical Physiology; Elsevier: New York, NY, USA, 2006. [Google Scholar]
- Schumacker, P.T.; Cain, S.M. The concept of a critical oxygen delivery. Intensive Care Med. 1987, 13, 223–229. [Google Scholar] [CrossRef]
- Nikolaenko, E.M. Critical level of oxygen transport in the early period after prosthetic heart valves surgery. Anesteziologiya-reanimatologiya 1986, 31, 26–30. (In Russian) [Google Scholar]
- Komatsu, T.; Shibutani, K.; Okamoto, K.; Kumar, V.; Kubal, K.; Sanchala, V.; Lees, D.E. Critical level of oxygen delivery after cardiopulmonary bypass. Crit. Care Med. 1987, 15, 194–197. [Google Scholar] [CrossRef]
- Mallat, J.; Mohammad, U.; Lemyze, M.; Meddour, M.; Jonard, M.; Pepy, F.; Gasan, G.; Barrailler, S.; Temime, J.; Vangrunderbeeck, N.; et al. Acute hyperventilation increases the central venous- to-arterial PCO2 difference in stable septic shock patients. Ann. Intensive Care 2017, 7, 31. [Google Scholar] [CrossRef] [Green Version]
- Tsutsumi, Y.M.; Yokoyama, T.; Horikawa, Y.; Roth, D.M.; Patel, H.H. Reactive oxygen species trigger ischemic and pharmacological postconditioning: In vivo and in vitro characterization. Life Sci. 2007, 81, 1223–1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garlid, A.O.; Jaburek, M.; Jacobs, J.P.; Garlid, K.D. Mitochondrial reactive oxygen species: Which ROS signals cardioprotection? Am. J. Physiol. Heart Circ. Physiol. 2013, 305, H960–H968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yellon, D.; Alkhulaifi, A.M.; Pugsley, W. B Preconditioning the human myocardium. Lancet 1993, 342, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Kolár, F.; Jezková, J.; Balková, P.; Breh, J.; Neckár, J.; Novák, F.; Nováková, O.; Tomásová, H.; Srbová, M.; Ost’ádal, B.; et al. Role of oxidative stress in PKC-delta upregulation and cardiopro- tection induced by chronic intermittent hypoxia. Am. J. Physiol. Heart Circ. Physiol. 2007, 292, H224–H230. [Google Scholar] [CrossRef]
- Kloner, R.A.; Creech, J.L.; Stone, G.W.; O’Neill, W.W.; Burkhoff, D.; Spears, J.R. Update on Cardioprotective Strategies for STEMI: Focus on Supersaturated Oxygen Delivery. JACC Basic Transl. Sci. 2021, 6, 1021–1033. [Google Scholar] [CrossRef]
- Crestanello, J.A.; Lingle, D.M.; Kamelgard, J.; Millili, J.; Whitman, G.J. Ischemic preconditioning decreases oxidative stress during reperfusion: A chemiluminescence study. J. Surg. Res. 1996, 65, 53–58. [Google Scholar] [CrossRef]
- Plestis, K.A.; Gold, J.P. Importance of blood pressure regulation in maintaining adequate tissue perfusion during cardiopulmonary bypass. Semin. Thorac. Cardiovasc. Surg. 2001, 13, 170–175. [Google Scholar] [CrossRef]
- Ohri, S.K. Systemic inflammatory response and the splanchnic bed in cardiopulmonary bypass. Perfusion 1996, 11, 200–212. [Google Scholar] [CrossRef]
- Monnet, X.; Julien, F.; Ait-Hamou, N.; Lequoy, M.; Gosset, C.; Jozwiak, M.; Persichini, R.; Anguel, N.; Richard, C.; Teboul, J.L. Lactate and venoarterial carbon dioxide difference/ arterial-venous oxygen difference ratio, but not central venous oxygen saturation, predict increase in oxygen consumption in fluid responders. Crit. Care Med. 2013, 41, 1412–1420. [Google Scholar] [CrossRef] [Green Version]
- Ltaief, Z.; Schneider, A.G.; Liaudet, L. Pathophysiology and clinical implications of the veno-arterial PCO2 gap. Crit Care 2021, 25, 318. [Google Scholar] [CrossRef]
- Mekontso-Dessap, A.; Castelain, V.; Anguel, N.; Bahloul, M.; Schauvliege, F.; Richard, C.; Teboul, J.L. Combination of venoarterial PCO2 difference with arteriovenous O2 content difference to detect anaerobic metabolism in patients. Intensive Care Med. 2002, 28, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Habicher, M.; von Heymann, C.; Spies, C.D.; Wernecke, K.D.; Sander, M. Central Venous-Arterial pCO2 and pH Difference Identifies Microcirculatory Hypoperfusion in Cardiac Surgical Patients with Normal Central Venous Oxygen Saturation: A Retrospective Analysis. J. Cardiothorac. Vasc. Anesth. 2015, 29, 646–655. [Google Scholar] [CrossRef] [PubMed]
- Tubek, S.; Niewinski, P.; Paleczny, B. Acute hyperoxia reveals tonic influence of peripheral chemoreceptors on systemic vascular resistance in heart failure patients. Sci. Rep. 2021, 11, 20823. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Zheng, D.; Chu, X.-Q.; Jiang, Y.-P.; Wang, C.-G.; Zhang, Q.-M.; Qian, L.-Z.; Yang, W.-Y.; Zhang, W.-Y.; Tung, T.-H.; et al. ΔPCO2 and ΔPCO2/C(a-cv)O2 Are Not Predictive of Organ Dysfunction after Cardiopulmonary Bypass Front. Cardiovasc. Med. 2021, 8, 759826. [Google Scholar] [CrossRef]
- Borges, J.P.; Mendes, F.S.N.S.; Lopes, G.O.; Sousa, A.S.; Mediano, M.F.F.; Tibiriçá, E. Is endothelial microvascular function equally impaired among patients with chronic Chagas and ischemic cardiomyopathy? Int. J. Cardiol. 2018, 15, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Vignon-Zellweger, N.; Heiden, S.; Miyauchi, T.; Emoto, N. Endothelin and endothelin receptors in the renal and cardiovascular systems. Life Sci. 2012, 91, 490–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | HHP Group, n = 60 | Control Group, n = 56 | p-Value |
|---|---|---|---|
| Age, years | 59 (55–64) | 61 (56; 65) | 0.236 |
| Sex (male), n (%) | 48 (60) | 48 (85.7) | 0.416 |
| Body mass index, kg/m2 | 27.6 (24.8–31.3) | 29.3 (25.5–32) | 0.545 |
| EuroSCORE, score (%) | 2–6 (1.51–5.89) | 2–6 (1.68–4.96) | 0.537 |
| Coexisting disease | |||
| Coronary artery disease, n (%) | 41 (68.3) | 36 (64.3) | 0.645 |
| Including ejection fraction of left ventricle, % | 56 (47.5–62.5) | 57.5 (50.8–62.3) | 0.826 |
| Coronary artery disease and Heart failure, n (%) | 19 (31.7) | 20 (35.7) | 0.645 |
| Including ejection fraction of left ventricle, % | 30 (28–36) | 33.5 (29.3–37.8) | 0.247 |
| Including, | |||
| NYHA I, n | 1 | 1 | |
| NYHA II, n | 15 | 17 | 0.850 |
| NYHA III, n | 3 | 2 | |
| HFpEF, n | 0 | 0 | |
| HFmrEF, n | 1 | 1 | |
| HFrEF, n | 18 | 19 | 0.970 |
| Arterial Hypertension, n (%) | 32 (53.3) | 34 (60.7) | 0.839 |
| Chronic Obstructive Pulmonary Disease, n (%) | 16 (26.7) | 13 (23.2) | 0.668 |
| Pulmonary Hypertension, n (%) | 9 (15) | 12 (21.4) | 0.369 |
| Chronic renal disease, n (%) | 6 (10) | 4 (7.1) | 0.472 |
| Cerebrovascular disease, n (%) | 17 (28.3) | 15 (26.8) | 0.159 |
| Stroke more than 1 year ago, n (%) | 6 (10) | 4 (7.1) | 0.480 |
| Gastrointestinal tract pathology, n (%) | 45 (75) | 38 (67.9) | 0.104 |
| Smoking, n (%) | 9 (15) | 9 (16.1) | 0.750 |
| Stenosis of femoral artheries, % | 30 (20–40) | 20 (5–33) | 0.224 |
| Stenosis of carotid artheries, % | 30 (20–55) | 30 (13–45) | 0.484 |
| Myocardial infarction > 1 year before surgery, n (%) | 35 (58.3) | 39 (69.6) | 0.205 |
| Parameter | HHP Group, n = 60 | Control Group, n = 56 | p-Value |
|---|---|---|---|
| Mean arterial pressure during CPB, mm Hg | 71 (65–75) | 60.5 (50–65) | 0.395 |
| Mean arterial pressure, lowest during CPB, mm Hg | 62 (58–67) | 60.5 (50–65) | 0.395 |
| Hemoglobin baseline, g/L | 130 (121–140) | 127 (118–137) | 0.171 |
| Hemoglobin, lowest during CPB, g/L | 84 (78–92) | 85 (77–95) | 0.669 |
| Hemoglobin, end of surgery, g/L | 103 (92–115) | 99 (93–111) | 0.326 |
| Creatinine 12 h after surgery, mkmol/L | 85 (80.3–94) | 85 (74.5–96) | 0.701 |
| Troponin T 12 h after surgery, pg/mL | 200 (140–290) | 221 (129–373) | 0.744 |
| pHg baseline | 5 (4.2–5.3) | 4.5 (4.1–5.2) | 0.386 |
| pHg during CPB (lowest) | 4 (3.8–4.1) | 3.8 (3.7–4.1) | 0.174 |
| pHg, end of surgery | 4 (3.7–4.3) | 4 (3.7–4.3) | 0.987 |
| pHg, 6 h after surgery | 4.1 (4.0–4.7) | 4.1 (4.0–4.7) | 0.934 |
| Intraoperative blood loss, mL | 350 (300–450) | 350 (300–450) | 0.934 |
| Po Spearmen’s | 95% Confidence Interval | p-Value | |
|---|---|---|---|
| pHg, end of surgery—length of surgery | −0.409 | −0.612; −0.156 | 0.002 |
| pHg, 6 h after surgery—legnth of surgery | −0.366 | −0.579; −0.106 | 0.006 |
| pHg, end of surgery—length of CPB | −0.267 | −0.501; 0.004 | 0.047 |
| pHg during CBP—Heart rhythm restoration after CPB (spontaneous sinus rhythm or VF and need for pacemaker) | −0.351 | −0.567; −0.089 | 0.008 |
| Parameter | HHP, n = 60 | Control, n = 56 | p-Value # |
|---|---|---|---|
| Changes in ET-1 concentration | |||
| ET-1, before surgery, fmol/mL | 0.785 (0.532–1.465) | 0.879 (0.691–1.888) | 0.275 |
| ET-1, end of surgery, fmol/mL | 0.804 (0.469–1.415) | 0.876 (0.521–1.511) p = 0.028 * | 0.194 |
| ET-1, 24 h after surgery, fmol/mL | 0.549 (0.445–0.969) p = 0.019 * | 0.626 (0.316–1.283) p = 0.001 * | 0.495 |
| Changes in NO2 total concentration | |||
| NO2 total, before surgery, µmol/L | 10.959 (8.715–16.785) | 11.788 (9.393–13.741) | 0.815 |
| NO2 total, end of surgery, µmol/L | 8.355 (6.815–11.527) p = 0.001 * | 7.244 (5.846–9.530) p = 0.001 * | 0.190 |
| NO2 total, 24 h after surgery, µmol/L | 9.165 (6.701–11.609) p = 0.005 * | 10.146 (6.450–13.053) p = 0.044 * | 0.511 |
| Changes in nitrite concentration | |||
| NO2 endo, before surgery, µmol/L | 1.004 (0.666–1.574) | 0.878 (0.631–1.574) | 0.848 |
| NO2 endo, end of surgery, µmol/L | 0.760 (0.474–1.048) p = 0.039 * | 0.809 (0.525–0.967) | 0.992 |
| NO2 endo, 24 h after surgery, µmol/L | 0.913 (0.649–1.118) | 0.874 (0.641–1.941) | 0.729 |
| Changes in nitrate concentration | |||
| NO3 endo, before surgery, µmol/L | 8.649 (6.063–14.071) | 10.153 (8.235–12.254) | 0.294 |
| NO3 endo, end of surgery, µmol/L | 6.934 (5.831–9.559) p = 0.001 * | 6.330 (5.478–8.324) p = 0.002 * | 0.476 |
| NO3 endo, 24 h after surgery, µmol/L | 8.206 (5.861; 10.215) | 9.290 (6.168–11.182) p = 0.025 * | 0.428 |
| Changes in ADMA concentration | |||
| ADMA, before surgery, µmol/L | 0.744 (0.584–0.951) | 0.606 (0.536–0.800) | 0.318 |
| ADMA, end of surgery, µmol/L | 0.776 (0.729–0.809) | 0.697 (0.551–0.820) | 0.036 |
| ADMA, 24 h after surgery, µmol/L | 0.848 (0.757–0.938) | 0.794 (0.626–0.999) | 0.084 |
| Parameter | Complicated Patients, n = 43 | Noncomplicated Patients, n = 73 | p-Value |
|---|---|---|---|
| ET-1, before surgery, fmol/mL | 1.506 (0.702–4.019) | 0.759 (0.577–1.120) | 0.049 |
| ET-1, end of surgery, fmol/mL | 1.217 (0.715–4.075) | 0.665 (0.510–1.168) | 0.053 |
| NO2 endo, end of surgery, µmol/L | 0.479 (0.410–0.749) | 0.852 (0.651–1.093) | 0.002 |
| ADMA, end of surgery, µmol/L | 0.715 (0.531–0.772) | 0.793 (0.735–0.862) | 0.045 |
| NO2 total, 24 h after surgery, µmol/L | 12.038 (8.754–14.041) | 8.093 (5.695–10.853) | 0.023 |
| NO3 endo, 24 h after surgery, µmol/L | 10.504 (7.461–12.412) | 7.317 (5.550–9.825) | 0.007 |
| Parameter | HHP Group, n = 60 | Control Group, n = 56 | p-Value |
|---|---|---|---|
| Number of complications (cumulative), n (%) | 14 (23.3) | 23 (41.1) | 0.041 |
| VIS after CPB, score | 6 (5–70) | 9.5 (6.3–15) | 0.001 |
| VIS 6 h, score | 3 (0–6) | 6 (5–11) | 0.001 |
| VIS 24 h, score | 0 (0–3) | 0 (0–3) | 0.929 |
| Need for pacing (temporary), n (%) | 3 (5) | 6 (10.7) | 0.251 |
| Length of mechanical ventilation, h | 10 (8–22) | 17 (11.3–24) | 0.015 |
| Need for intra-aortic balloon pump, n (%) | 2 (3.3) | 2 (3.6) | 0.944 |
| Revision for bleeding, n (%) | 0 | 1 (1.8) | |
| Myocardial infarction, n (%) | 0 | 0 | |
| Gastrointestinal dysfunction (stress ulcer bleeding, gastrostasis, intestinal hypomotility), n (%) | 3 (5.0) | 6 (10.7) | 0.251 |
| Respiratory complications (ARDS, pneumonia), n (%) | 1 (1.7) | 4 (7.1) | 0.148 |
| Pulmonary hypertension, n (%) | 1 (1.7) | 0 | 0.332 |
| Acute renal failure, n (%) | 2 (3.3) | 1 (1.8) | 0.600 |
| Delirium, n (%) | 1 (1.7) | 2 (3.6) | 0.519 |
| Mediastinitis, n (%) | 1 (1.7) | 1 (1.8) | 0.961 |
| Length of stay in ICU, days | 1 (1–2) | 1 (1–2) | 0.507 |
| Length of hospital stay, days | 12 (11–14) | 12 (11.3–14) | 0.161 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mandel, I.A.; Podoksenov, Y.K.; Mikheev, S.L.; Suhodolo, I.V.; Svirko, Y.S.; Shipulin, V.M.; Ivanova, A.V.; Yavorovskiy, A.G.; Yaroshetskiy, A.I. Endothelial Function and Hypoxic–Hyperoxic Preconditioning in Coronary Surgery with a Cardiopulmonary Bypass: Randomized Clinical Trial. Biomedicines 2023, 11, 1044. https://doi.org/10.3390/biomedicines11041044
Mandel IA, Podoksenov YK, Mikheev SL, Suhodolo IV, Svirko YS, Shipulin VM, Ivanova AV, Yavorovskiy AG, Yaroshetskiy AI. Endothelial Function and Hypoxic–Hyperoxic Preconditioning in Coronary Surgery with a Cardiopulmonary Bypass: Randomized Clinical Trial. Biomedicines. 2023; 11(4):1044. https://doi.org/10.3390/biomedicines11041044
Chicago/Turabian StyleMandel, Irina A., Yuriy K. Podoksenov, Sergey L. Mikheev, Irina V. Suhodolo, Yulia S. Svirko, Vladimir M. Shipulin, Anastasia V. Ivanova, Andrey G. Yavorovskiy, and Andrey I. Yaroshetskiy. 2023. "Endothelial Function and Hypoxic–Hyperoxic Preconditioning in Coronary Surgery with a Cardiopulmonary Bypass: Randomized Clinical Trial" Biomedicines 11, no. 4: 1044. https://doi.org/10.3390/biomedicines11041044