
The Association of Leptin with Left Ventricular Hypertrophy in End-Stage Kidney Disease Patients on Dialysis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Analytical Assays
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zoccali, C.; Benedetto, F.A.; Mallamaci, F.; Tripepi, G.; Giacone, G.; Cataliotti, A.; Seminara, G.; Stancanelli, B.; Malatino, L.S. Prognostic Value of Echocardiographic Indicators of Left Ventricular Systolic Function in Asymptomatic Dialysis Patients. J. Am. Soc. Nephrol. 2004, 15, 1029–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shlipak, M.G.; Fried, L.F.; Cushman, M.; Manolio, T.A.; Peterson, D.; Stehman-Breen, C.; Bleyer, A.; Newman, A.; Siscovick, D.; Psaty, B. Cardiovascular mortality risk in chronic kidney disease: Comparison of traditional and novel risk factors. JAMA 2005, 293, 1737–1745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, C.; Amaral, A.P.; Oskouei, B.; Hu, M.C.; Sloan, A.; Isakova, T.; Gutierrez, O.M.; Aguillon-Prada, R.; Lincoln, J.; Hare, J.M.; et al. FGF23 induces left ventricular hypertrophy. J. Clin. Investig. 2011, 121, 4393–4408. [Google Scholar] [CrossRef] [Green Version]
- Di Lullo, L.; Gorini, A.; Russo, D.; Santoboni, A.; Ronco, C. Left Ventricular Hypertrophy in Chronic Kidney Disease Patients: From Pathophysiology to Treatment. Cardiorenal Med. 2015, 5, 254–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charmetant, X.; Pecquet, M.; Poirie, P.; Agi, D.; Aupetit, J.F.; Villar, E. Impact of age and renal function on usefulness of NT-proBNP to diagnose heart failure. Clin. Nephrol. 2019, 92, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Zelnick, L.; Shlipak, M.G.; Anderson, A.; Christenson, R.; Deo, R.; deFilippi, C.; Feldman, H.; Lash, J.; He, J.; et al. Cardiac and Stress Biomarkers and Chronic Kidney Disease Progression: The CRIC Study. Clin. Chem. 2019, 65, 1448–1457. [Google Scholar] [CrossRef]
- Tuegel, C.; Katz, R.; Alam, M.; Bhat, Z.; Bellovich, K.; de Boer, I.; Brosius, F.; Gadegbeku, C.; Gipson, D.; Hawkins, J.; et al. GDF-15, Galectin 3, Soluble ST2, and Risk of Mortality and Cardiovascular Events in CKD. Am. J. Kidney Dis. 2018, 72, 519–528. [Google Scholar] [CrossRef]
- Claus, R.; Berliner, D.; Bavendiek, U.; Vodovar, N.; Lichtinghagen, R.; David, S.; Patecki, M.; Launay, J.M.; Bauersachs, J.; Haller, H.; et al. Soluble neprilysin, NT-proBNP, and growth differentiation factor-15 as biomarkers for heart failure in dialysis patients (SONGBIRD). Clin. Res. Cardiol. 2020, 109, 1035–1047. [Google Scholar] [CrossRef] [Green Version]
- Laville, M.; Fouque, D. Nutritional aspects in hemodialysis. Kidney Int. Suppl. 2000, 76, S133–S139. [Google Scholar] [CrossRef] [Green Version]
- Markaki, A.; Psylinakis, E.; Spyridaki, A. Adiponectin and end-stage renal disease. Hormones 2016, 15, 345–354. [Google Scholar] [CrossRef] [Green Version]
- Elokely, A.; Shoukry, A.; Ghonemy, T.A.; Atia, M.; Amr, G. Association of adiponectin with cardiovascular events in diabetic and non-diabetic hemodialysis patients. Saudi J. Kidney Dis. Transpl. 2012, 23, 736–742. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, S.; Reis, F.; Nunes, S.; Viana, S.; Valente, M.J.; Rocha, S.; Catarino, C.; Rocha-Pereira, P.; Bronze-da-Rocha, E.; Sameiro-Faria, M.; et al. The Protective Role of Adiponectin for Lipoproteins in End-Stage Renal Disease Patients: Relationship with Diabetes and Body Mass Index. Oxid. Med. Cell. Longev. 2019, 2019, 3021785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komaba, H.; Igaki, N.; Goto, S.; Yokota, K.; Takemoto, T.; Hirosue, Y.; Goto, T. Adiponectin is associated with brain natriuretic peptide and left ventricular hypertrophy in hemodialysis patients with type 2 diabetes mellitus. Nephron Clin. Pract. 2007, 107, c103–c108. [Google Scholar] [CrossRef] [PubMed]
- Alix, P.M.; Guebre-Egziabher, F.; Soulage, C.O. Leptin as an uremic toxin: Deleterious role of leptin in chronic kidney disease. Biochimie 2014, 105, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Kastarinen, H.; Kesaniemi, Y.A.; Ukkola, O. Leptin and lipid metabolism in chronic kidney failure. Scand. J. Clin. Lab. Investig. 2009, 69, 401–408. [Google Scholar] [CrossRef]
- Liu, B.; Qiao, J.; Hu, J.; Fan, M.; Zhao, Y.; Su, H.; Wang, Z.; Yu, Q.; Ma, Q.; Li, Y.; et al. Leptin promotes endothelial dysfunction in chronic kidney disease by modulating the MTA1-mediated WNT/beta-catenin pathway. Mol. Cell. Biochem. 2020, 473, 155–166. [Google Scholar] [CrossRef]
- Aguilera, A.; Bajo, M.A.; Rebollo, F.; Diez, J.J.; Diaz, C.; Paiva, A.; Codoceo, R.; Selgas, R. Leptin as a marker of nutrition and cardiovascular risk in peritoneal dialysis patients. Adv. Perit. Dial. 2002, 18, 212–217. [Google Scholar]
- Scholze, A.; Rattensperger, D.; Zidek, W.; Tepel, M. Low serum leptin predicts mortality in patients with chronic kidney disease stage 5. Obesity 2007, 15, 1617–1622. [Google Scholar] [CrossRef]
- Qin, Z.; Yang, Q.; Yang, M.; Han, M.; Xiong, Y.; Liao, R.; Su, B. Serum leptin concentration can predict cardiovascular outcomes and all-cause death in maintenance hemodialysis patients. Clin. Chim. Acta 2021, 520, 87–94. [Google Scholar] [CrossRef]
- Sweigert, P.J.; Bansal, V.K.; Hoppensteadt, D.A.; Saluk, J.L.; Syed, D.A.; Fareed, J. Inflammatory and Metabolic Syndrome Biomarker Analysis of Vascular Outcomes in End-stage Renal Disease. Int. J. Angiol. 2017, 26, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Templeton, G.F. A two-step approach for transforming continuous variables to normal: Implications and recommendations for IS research. Commun. Assoc. Inf. Syst. 2011, 28, 41–58. [Google Scholar] [CrossRef] [Green Version]
- Kamimura, D.; Suzuki, T.; Wang, W.; deShazo, M.; Hall, J.E.; Winniford, M.D.; Kullo, I.J.; Mosley, T.H.; Butler, K.R.; Hall, M.E. Higher plasma leptin levels are associated with reduced left ventricular mass and left ventricular diastolic stiffness in black women: Insights from the Genetic Epidemiology Network of Arteriopathy (GENOA) study. Hypertens. Res. 2018, 41, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Allison, M.A.; Bluemke, D.A.; McClelland, R.; Cushman, M.; Criqui, M.H.; Polak, J.F.; Lima, J.A. Relation of leptin to left ventricular hypertrophy (from the Multi-Ethnic Study of Atherosclerosis). Am. J. Cardiol. 2013, 112, 726–730. [Google Scholar] [CrossRef] [Green Version]
- Pladevall, M.; Williams, K.; Guyer, H.; Sadurni, J.; Falces, C.; Ribes, A.; Pare, C.; Brotons, C.; Gabriel, R.; Serrano-Rios, M.; et al. The association between leptin and left ventricular hypertrophy: A population-based cross-sectional study. J. Hypertens. 2003, 21, 1467–1473. [Google Scholar] [CrossRef] [PubMed]
- Lieb, W.; Sullivan, L.M.; Aragam, J.; Harris, T.B.; Roubenoff, R.; Benjamin, E.J.; Vasan, R.S. Relation of serum leptin with cardiac mass and left atrial dimension in individuals >70 years of age. Am. J. Cardiol. 2009, 104, 602–605. [Google Scholar] [CrossRef] [Green Version]
- Di Blasio, A.; Di Donato, F.; De Stefano, A.; Gallina, S.; Granieri, M.; Napolitano, G.; Petrella, V.; Riccardi, I.; Santarelli, F.; Valentini, P.; et al. Left ventricle relative wall thickness and plasma leptin levels: Baseline relationships and effects of 4 months of walking training in healthy overweight postmenopausal women. Menopause 2011, 18, 77–84. [Google Scholar] [CrossRef]
- Paduszynska, A.; Sakowicz, A.; Banach, M.; Maciejewski, M.; Dabrowa, M.; Bielecka-Dabrowa, A. Cardioprotective properties of leptin in patients with excessive body mass. Ir. J. Med. Sci. 2020, 189, 1259–1265. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Naseem, R.H.; Duplomb, L.; Park, B.H.; Garry, D.J.; Richardson, J.A.; Schaffer, J.E.; Unger, R.H. Hyperleptinemia prevents lipotoxic cardiomyopathy in acyl CoA synthase transgenic mice. Proc. Natl. Acad. Sci. USA 2004, 101, 13624–13629. [Google Scholar] [CrossRef] [Green Version]
- Barouch, L.A.; Berkowitz, D.E.; Harrison, R.W.; O’Donnell, C.P.; Hare, J.M. Disruption of leptin signaling contributes to cardiac hypertrophy independently of body weight in mice. Circulation 2003, 108, 754–759. [Google Scholar] [CrossRef] [Green Version]
- Trivedi, P.; Yang, R.; Barouch, L.A. Decreased p110alpha catalytic activity accompanies increased myocyte apoptosis and cardiac hypertrophy in leptin deficient ob/ob mice. Cell Cycle 2008, 7, 560–565. [Google Scholar] [CrossRef] [Green Version]
- Peterson, L.R.; Soto, P.F.; Herrero, P.; Mohammed, B.S.; Avidan, M.S.; Schechtman, K.B.; Dence, C.; Gropler, R.J. Impact of gender on the myocardial metabolic response to obesity. JACC Cardiovasc. Imaging 2008, 1, 424–433. [Google Scholar] [CrossRef] [Green Version]
- Hall, M.E.; Brinkley, T.E.; Chughtai, H.; Morgan, T.M.; Hamilton, C.A.; Jordan, J.H.; Stacey, R.B.; Soots, S.; Hundley, W.G. Adiposity Is Associated with Gender-Specific Reductions in Left Ventricular Myocardial Perfusion during Dobutamine Stress. PLoS ONE 2016, 11, e0146519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimada, Y.J. Is leptin protective against heart failure with preserved ejection fraction? A complex interrelationship among leptin, obesity, and left ventricular hypertrophy. Hypertens. Res. 2019, 42, 141–142. [Google Scholar] [CrossRef]
- Ramanath, V.; Gupta, D.; Jain, J.; Chaudhary, K.; Nistala, R. Anemia and chronic kidney disease: Making sense of the recent trials. Rev. Recent Clin. Trials 2012, 7, 187–196. [Google Scholar] [CrossRef]
- Group KDIGOKAW. KDIGO Clinical practice Guideline for Anemia in Chronic kidney disease. Kidney Int. Suppl. 2012, 2, 279–335. [Google Scholar]
- London, G. Pathophysiology of cardiovascular damage in the early renal population. Nephrol. Dial. Transplant. 2001, 16 (Suppl. S2), 3–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iseki, K.; Kohagura, K. Anemia as a risk factor for chronic kidney disease. Kidney Int. 2007, 72, S4–S9. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.; Bai, Y.H.; Chen, T.; Zhang, L.; Wang, Y.R.; Zhu, H.; Jiao, Y.X.; Sun, L. The relation of calcium-phosphorus metabolism-related indexes with cardiac damages. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 3244–3248. [Google Scholar]
- Hill Gallant, K.M.; Spiegel, D.M. Calcium Balance in Chronic Kidney Disease. Curr. Osteoporos. Rep. 2017, 15, 214–221. [Google Scholar] [CrossRef]
- Hwang, H.S.; Cho, J.S.; Hong, Y.A.; Chang, Y.K.; Kim, S.Y.; Shin, S.J.; Yoon, H.E. Vascular calcification and left ventricular hypertrophy in hemodialysis patients: Interrelationship and clinical impacts. Int. J. Med. Sci. 2018, 15, 557–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Wu, N.; Li, Y.; Ye, K.; He, M.; Hu, R. Cross-sectional analysis of serum calcium levels for associations with left ventricular hypertrophy in normocalcemia individuals with type 2 diabetes. Cardiovasc. Diabetol. 2015, 14, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumida, K.; Yamagata, K.; Iseki, K.; Tsubakihara, Y. Different impact of hemodialysis vintage on cause-specific mortality in long-term hemodialysis patients. Nephrol. Dial. Transplant. 2016, 31, 298–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.; Kim, B.K.; Lim, Y.H.; Kim, M.K.; Choi, B.Y.; Shin, J. The relationship between adiponectin and left ventricular mass index varies with the risk of left ventricular hypertrophy. PLoS ONE 2013, 8, e70246. [Google Scholar] [CrossRef] [PubMed]
- Hijazi, Z.; Verdecchia, P.; Oldgren, J.; Andersson, U.; Reboldi, G.; Di Pasquale, G.; Mazzotta, G.; Angeli, F.; Eikelboom, J.W.; Ezekowitz, M.D.; et al. Cardiac Biomarkers and Left Ventricular Hypertrophy in Relation to Outcomes in Patients with Atrial Fibrillation: Experiences from the RE—LY Trial. J. Am. Heart Assoc. 2019, 8, e010107. [Google Scholar] [CrossRef] [Green Version]
- Kou, H.; Jin, X.; Gao, D.; Ma, R.; Dong, X.; Wei, J.; Wang, X. Association between growth differentiation factor 15 and left ventricular hypertrophy in hypertensive patients and healthy adults. Clin. Exp. Hypertens. 2018, 40, 8–15. [Google Scholar] [CrossRef]
- Xue, H.; Fu, Z.; Chen, Y.; Xing, Y.; Liu, J.; Zhu, H.; Zhou, X. The association of growth differentiation factor-15 with left ventricular hypertrophy in hypertensive patients. PLoS ONE 2012, 7, e46534. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Kimball, T.R.; Lorenz, J.N.; Brown, D.A.; Bauskin, A.R.; Klevitsky, R.; Hewett, T.E.; Breit, S.N.; Molkentin, J.D. GDF15/MIC-1 functions as a protective and antihypertrophic factor released from the myocardium in association with SMAD protein activation. Circ. Res. 2006, 98, 342–350. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.Y.; Nie, Y.; Wang, F.F.; Bai, Y.; Lv, Z.Z.; Zhang, Y.Y.; Li, Z.J.; Gao, W. Growth differentiation factor (GDF)-15 blocks norepinephrine-induced myocardial hypertrophy via a novel pathway involving inhibition of epidermal growth factor receptor transactivation. J. Biol. Chem. 2014, 289, 10084–10094. [Google Scholar] [CrossRef] [Green Version]
- Kempf, T.; Eden, M.; Strelau, J.; Naguib, M.; Willenbockel, C.; Tongers, J.; Heineke, J.; Kotlarz, D.; Xu, J.; Molkentin, J.D.; et al. The transforming growth factor-beta superfamily member growth-differentiation factor-15 protects the heart from ischemia/reperfusion injury. Circ. Res. 2006, 98, 351–360. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| non-LVH (n = 65) | LVH (n = 131) | p Value | |
|---|---|---|---|
| Age (years) | 70.2 (60.5–79.5) | 71.8 (60.7–79.5) | 0.707 |
| Gender (n, Male/Female) | 35/30 | 69/62 | 0.878 |
| BMI (kg/m2) | 26.7 ± 4.6 | 25.6 ± 4.3 | 0.129 |
| Dialysis Vintage (years) | 2.5 (1.4–5.4) | 3.6 (1.8–7.1) | 0.081 |
| URR (%) | 80.0 (76.0–83.0) | 79.0 (75.0–83.0) | 0.418 |
| Kt/V | 1.82 ± 0.31 | 1.77 ± 0.32 | 0.349 |
| eKt/V | 1.66 ± 0.34 | 1.60 ± 0.30 | 0.218 |
| Ultrafiltration Volume (L) | 2.46 ± 0.88 | 2.37 ± 0.96 | 0.523 |
| SBP (mmHg) | 137 (126–148) | 137 (126–156) | 0.313 |
| DBP (mmHg) | 63 (56–72) | 61 (54–72) | 0.512 |
| Calcium (mg/dL) | 8.93 ± 0.50 | 9.11 ± 0.55 | 0.028 |
| Phosphorus (mg/dL) | 4.20 (3.51–5.04) | 4.17 (3.30–4.80) | 0.307 |
| PTH (pg/dL) | 349 (208–514) | 354 (212–510) | 0.622 |
| Albumin (g/dL) | 4.00 (3.75–4.10) | 3.90 (3.60–4.20) | 0.170 |
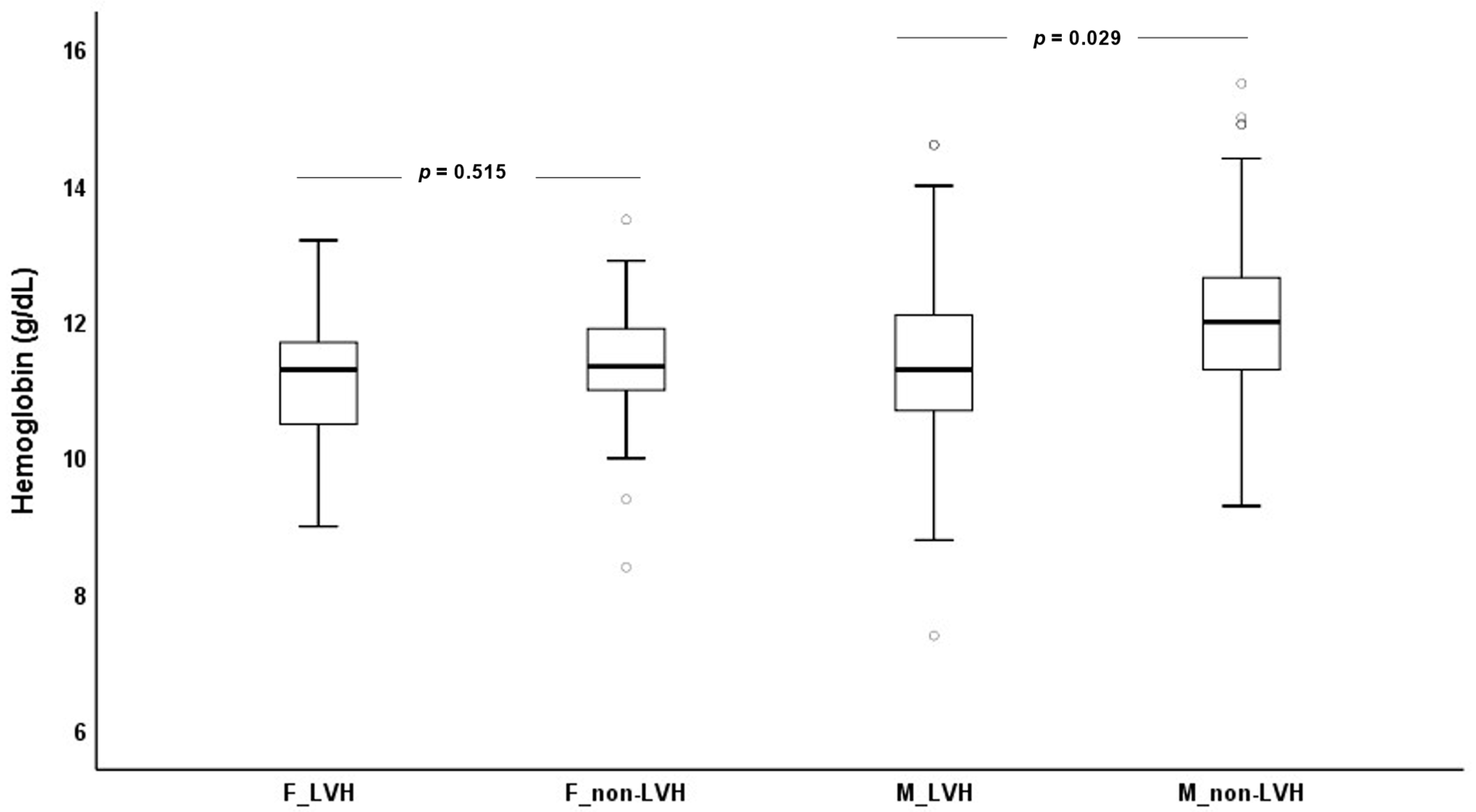
| Hemoglobin (g/dL) | 11.5 (11.0–12.5) | 11.3 (10.6–12.0) | 0.039 |
| NT-proBNP (ng/mL) | 10.8 (6.2–17.6) | 16.5 (9.0–29.8) | 0.002 |
| GDF-15 (ng/mL) | 10.6 (7.8–12.8) | 11.3 (8.4–14.5) | 0.048 |
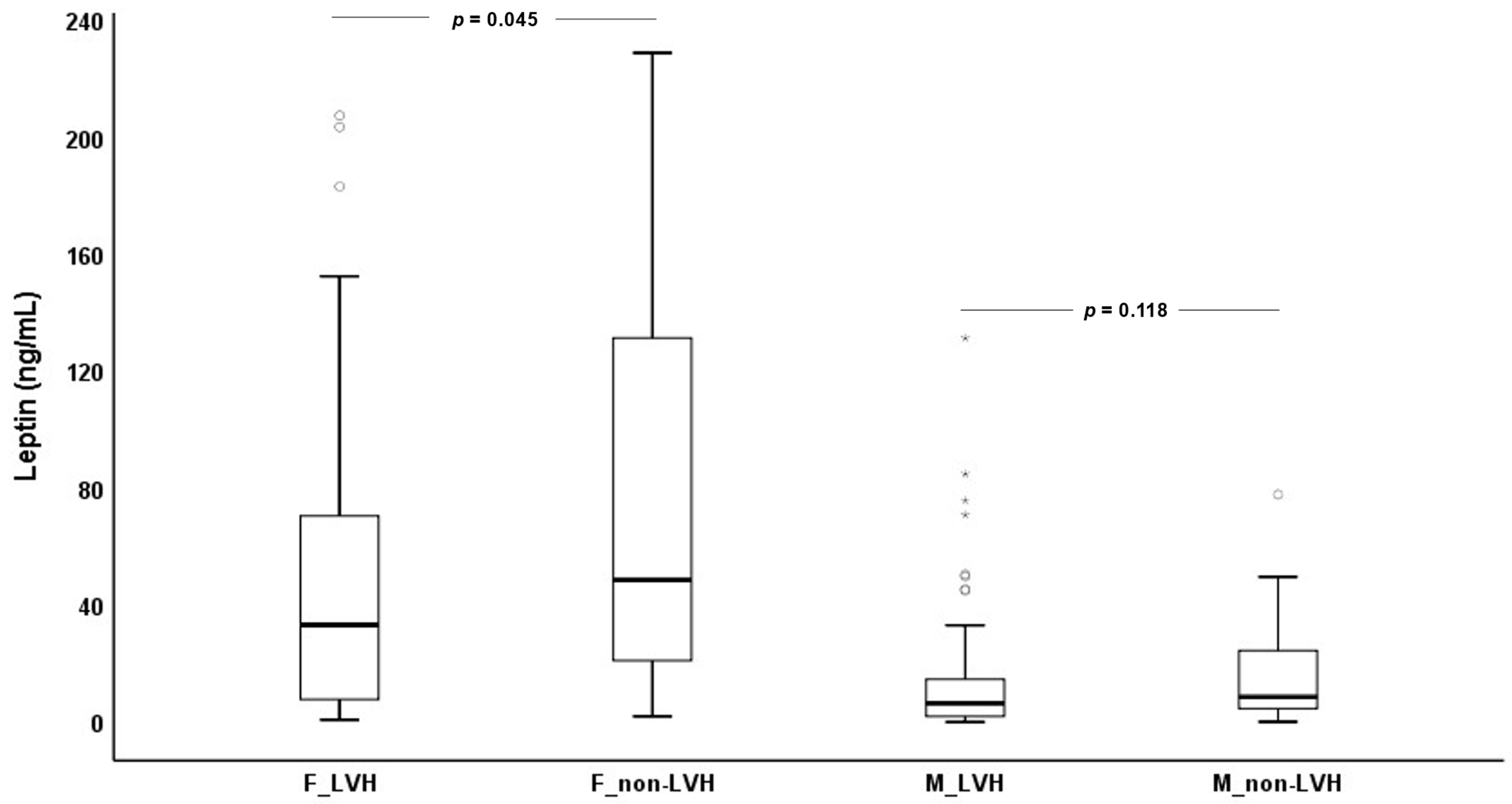
| Leptin (ng/mL) | 21.3 (6.7–51.2) | 13.7 (4.6–42.7) | 0.052 * |
| Adiponectin (ng/mL) | 10.8 (7.9–17.6) | 12.2 (7.2–20.1) | 0.503 |
| End-Stage Kidney Disease Patients (n = 196) | |||||
|---|---|---|---|---|---|
| Unstandardized Coefficients | Standardized Coefficients | t | p Value | ||
| Biomarkers | B | Standard error | β | ||
| Leptin | −0.160 | 0.041 | −0.263 | −3.860 | <0.001 |
| NT-proBNP | 0.240 | 0.060 | 0.273 | 4.012 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coimbra, S.; Catarino, C.; Sameiro Faria, M.; Nunes, J.P.L.; Rocha, S.; Valente, M.J.; Rocha-Pereira, P.; Bronze-da-Rocha, E.; Bettencourt, N.; Beco, A.; et al. The Association of Leptin with Left Ventricular Hypertrophy in End-Stage Kidney Disease Patients on Dialysis. Biomedicines 2023, 11, 1026. https://doi.org/10.3390/biomedicines11041026
Coimbra S, Catarino C, Sameiro Faria M, Nunes JPL, Rocha S, Valente MJ, Rocha-Pereira P, Bronze-da-Rocha E, Bettencourt N, Beco A, et al. The Association of Leptin with Left Ventricular Hypertrophy in End-Stage Kidney Disease Patients on Dialysis. Biomedicines. 2023; 11(4):1026. https://doi.org/10.3390/biomedicines11041026
Chicago/Turabian StyleCoimbra, Susana, Cristina Catarino, Maria Sameiro Faria, José Pedro L. Nunes, Susana Rocha, Maria João Valente, Petronila Rocha-Pereira, Elsa Bronze-da-Rocha, Nuno Bettencourt, Ana Beco, and et al. 2023. "The Association of Leptin with Left Ventricular Hypertrophy in End-Stage Kidney Disease Patients on Dialysis" Biomedicines 11, no. 4: 1026. https://doi.org/10.3390/biomedicines11041026