
Sputum-Rheology-Based Strategy for Guiding Azithromycin Prescription in COPD Patients with Frequent Exacerbations: A Randomized, Controlled Study (“COPD CARhE”)

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives
2.1.1. Primary Objective
2.1.2. Secondary Objectives
- -
- the exacerbation rates by severity (as observed throughout the study);
- -
- the evolution of symptoms, sputum rheology, and lung function (via repeated measurements collected every 3 months);
- -
- the medication usage and adverse events (follow-ups for the duration of the study);
- -
- the patient trajectories during follow-ups;
- -
- the overall clinical improvement achieved by the end of the study and changes in quality of life (via repeated measurements every 3 months); and
- -
- the changes in biomarkers of interest (baseline versus end of study).
- -
- We will compare the exacerbation rates, throughout the study, of the experimental arm without azithromycin prescription, and of the comparator arm without azithromycin; and between the experimental arm with azithromycin prescription and the comparator arm with azithromycin.
- -
- We will evaluate patients in the experimental arm who would have been managed differently using the CASA-Q versus rheology.
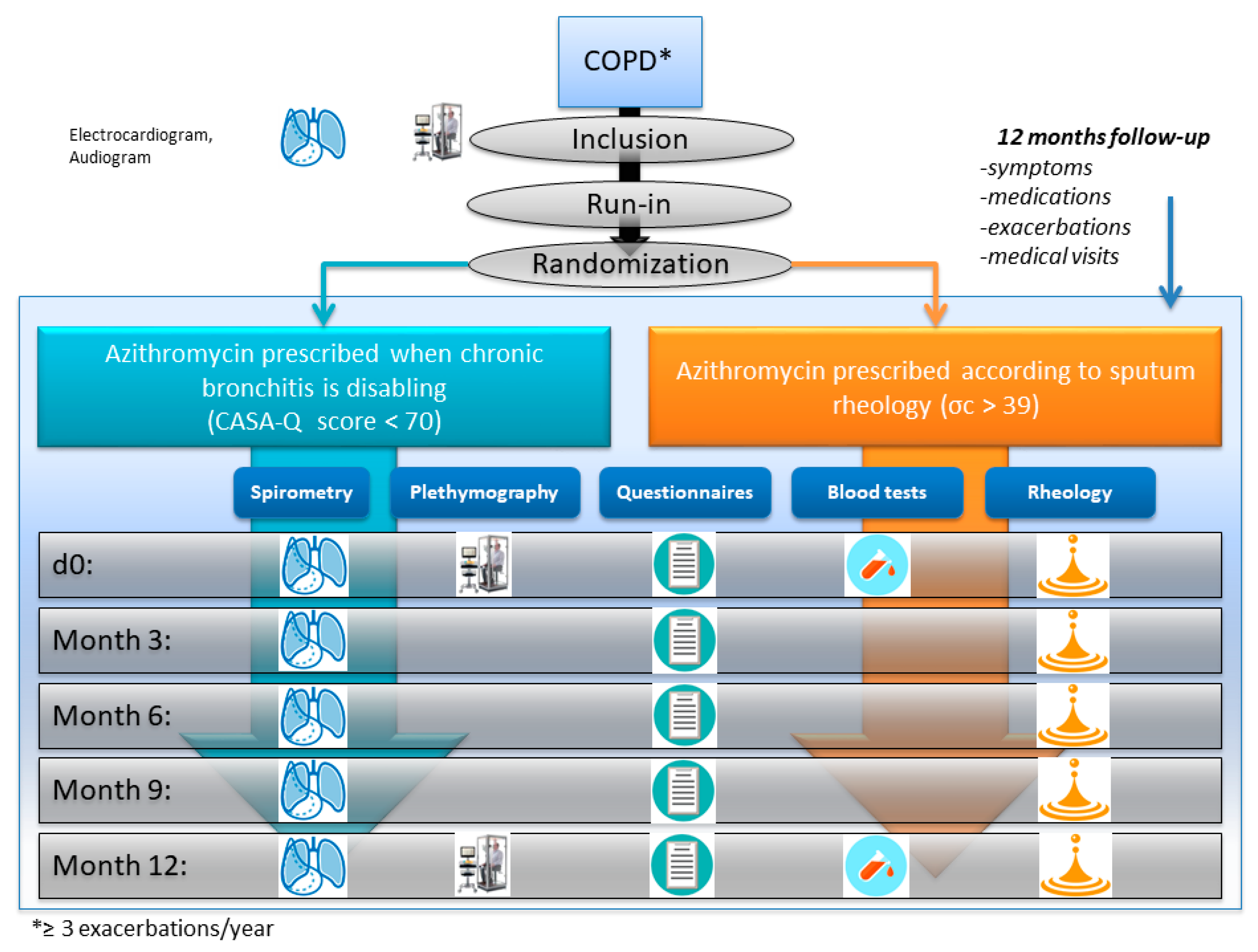
2.2. Study Design
2.3. Setting and Participant Eligibility
2.4. Interventions
2.4.1. Comparator Arm
- -
- If the patient presents a sputum symptom score of <70, azithromycin will be initiated for 3 months. This prescription will be renewable every 3 months during the 12 months of follow-up planned in this study if the patient continues to obtain a sputum symptom score of <70.
- -
- If the patient has a sputum symptom score of >70, management will not be changed.
2.4.2. Experimental Arm
- -
- If sputum has a critical stress σc >39, azithromycin will be initiated for 3 months. This prescription will be renewable every 3 months during the 12 months of follow-up planned in this study.
- -
- In the absence of sputum, azithromycin will not be prescribed.
2.5. Randomization and Blinding
2.6. Predicted and Explanatory Variables
2.7. Sputum Collection
2.8. Sputum Rheology
2.9. Pulmonary Function Tests
2.10. Blood Tests
2.11. Quality-of-Life Questionnaires
2.12. Prescription of Azithromycin
2.13. Ethics
2.14. Sample Size and Statistics
2.15. Study Schedule
- -
- Duration of the regulatory process: 6–9 months;
- -
- Duration of the inclusion period: 24 months;
- -
- Duration of the participation of each participant: 12 months;
- -
- Duration of the statistical analysis and writing of the final report: 12 months;
- -
- Anticipated duration of the study (inclusion and follow-up): 36 months;
- -
- Anticipated total study duration: 48 months;
- -
- Number of visits from the beginning of the study: 7 per patient (see Table 2).
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Adeloye, D.; Chua, S.; Lee, C.; Basquill, C.; Papana, A.; Theodoratou, E.; Nair, H.; Gasevic, D.; Sridhar, D.; Campbell, H.; et al. Global and regional estimates of COPD prevalence: Systematic review and meta–analysis. J. Glob. Health 2015, 5, 20415. [Google Scholar] [CrossRef] [PubMed]
- Terzikhan, N.; Verhamme, K.M.C.; Hofman, A.; Stricker, B.H.; Brusselle, G.G.; Lahousse, L. Prevalence and incidence of COPD in smokers and non-smokers: The Rotterdam Study. Eur. J. Epidemiol. 2016, 31, 785–792. [Google Scholar] [CrossRef] [Green Version]
- Burgel, P.-R.; Laurendeau, C.; Raherison, C.; Fuhrman, C.; Roche, N. An attempt at modeling COPD epidemiological trends in France. Respir. Res. 2018, 19, 130. [Google Scholar] [CrossRef] [PubMed]
- Kim, V.; Criner, G.J. Chronic Bronchitis and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2013, 187, 228–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Çolak, Y.; Afzal, S.; Marott, J.L.; Nordestgaard, B.G.; Vestbo, J.; Ingebrigtsen, T.S.; Lange, P. Prognosis of COPD depends on severity of exacerbation history: A population-based analysis. Respir. Med. 2019, 155, 141–147. [Google Scholar] [CrossRef]
- Molinari, N.; Briand, C.; Vachier, I.; Malafaye, N.; Aubas, P.; Georgescu, V.; Roche, N.; Chanez, P.; Bourdin, A. Hospitalizations for COPD Exacerbations: Trends and Determinants of Death. COPD 2015, 12, 621–627. [Google Scholar]
- Anthonisen, N.R. Antibiotic Therapy in Exacerbations of Chronic Obstructive Pulmonary Disease. Ann. Intern. Med. 1987, 106, 196–204. [Google Scholar] [CrossRef]
- McDonough, J.E.; Yuan, R.; Suzuki, M.; Seyednejad, N.; Elliott, W.M.; Sanchez, P.G.; Wright, A.C.; Gefter, W.B.; Litzky, L.; Coxson, H.O.; et al. Small-Airway Obstruction and Emphysema in Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2011, 365, 1567–1575. [Google Scholar] [CrossRef] [Green Version]
- Lahousse, L.; Seys, L.J.M.; Joos, G.F.; Franco, O.H.; Stricker, B.H.; Brusselle, G.G. Epidemiology and impact of chronic bronchitis in chronic obstructive pulmonary disease. Eur. Respir. J. 2017, 50, 1602470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kesimer, M.; Ford, A.A.; Ceppe, A.; Radicioni, G.; Cao, R.; Davis, C.W.; Doerschuk, C.M.; Alexis, N.E.; Anderson, W.H.; Henderson, A.G.; et al. Airway Mucin Concentration as a Marker of Chronic Bronchitis. N. Engl. J. Med. 2017, 377, 911–922. [Google Scholar] [CrossRef]
- Fahy, J.V.; Dickey, B.F. Airway mucus function and dysfunction. N. Engl. J. Med. 2010, 363, 2233–2247. [Google Scholar] [CrossRef] [Green Version]
- Charriot, J.; Volpato, M.; Petit, A.; Vachier, I.; Bourdin, A. Methods of Sputum and Mucus Assessment for Muco-Obstructive Lung Diseases in 2022: Time to “Unplug” from Our Daily Routine! Cells 2022, 11, 812. [Google Scholar] [CrossRef] [PubMed]
- Hogg, J.C.; Chu, F.; Utokaparch, S.; Woods, R.; Elliott, W.M.; Buzatu, L.; Cherniack, R.M.; Rogers, R.M.; Sciurba, F.C.; Coxson, H.O.; et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N. Engl. J. Med. 2004, 350, 2645–2653. [Google Scholar] [CrossRef] [PubMed]
- Boucherat, O.; Morissette, M.C.; Provencher, S.; Bonnet, S.; Maltais, F. Bridging Lung Development with Chronic Obstructive Pulmonary Disease. Relevance of Developmental Pathways in Chronic Obstructive Pulmonary Disease Pathogenesis. Am. J. Respir. Crit. Care Med. 2016, 193, 362–375. [Google Scholar] [CrossRef]
- Boue, S.; Fields, B.; Hoeng, J.; Park, J.; Peitsch, M.C.; Schlage, W.K.; Talikka, M.; Performers, T.C.B.; Binenbaum, I.; Bondarenko, V.; et al. Enhancement of COPD biological networks using a web-based collaboration interface. F1000Research 2015, 4, 32. [Google Scholar] [PubMed]
- O’Reilly, P.J.; Jackson, P.L.; Wells, J.M.; Dransfield, M.T.; Scanlon, P.D.; Blalock, J.E. Sputum PGP is reduced by azithromycin treatment in patients with COPD and correlates with exacerbations. BMJ Open 2013, 3, e004140. [Google Scholar] [CrossRef] [Green Version]
- Hodge, S.; Hodge, G.; Brozyna, S.; Jersmann, H.; Holmes, M.; Reynolds, P.N. Azithromycin increases phagocytosis of apoptotic bronchial epithelial cells by alveolar macrophages. Eur. Respir. J. 2006, 28, 486–495. [Google Scholar] [CrossRef]
- Shimizu, T.; Shimizu, S. Azithromycin inhibits mucus hypersecretion from airway epithelial cells. Mediat. Inflamm. 2012, 2012, 265714. [Google Scholar] [CrossRef]
- Albert, R.K.; Connett, J.; Bailey, W.C.; Casaburi, R.; Cooper, J.A.D.; Criner, G.J.; Curtis, J.L.; Dransfield, M.T.; Han, M.K.; Lazarus, S.C.; et al. Azithromycin for Prevention of Exacerbations of COPD. N. Engl. J. Med. 2011, 365, 689–698. [Google Scholar] [CrossRef]
- Uzun, S.; Djamin, R.S.; Kluytmans, J.A.J.W.; Mulder, P.G.H.; van’t Veer, N.E.; Ermens, A.A.M.; Pelle, A.J.; Hoogsteden, H.C.; Aerts, J.G.J.V.; van der Eerden, M.M. Azithromycin maintenance treatment in patients with frequent exacerbations of chronic obstructive pulmonary disease (COLUMBUS): A randomised, double-blind, placebo-controlled trial. Lancet Respir. Med. 2014, 2, 361–368. [Google Scholar] [CrossRef]
- Berkhof, F.F.; Hertog, N.E.; Uil, S.M.; Kerstjens, H.A.; van den Berg, J.W. Azithromycin and cough-specific health status in patients with chronic obstructive pulmonary disease and chronic cough: A randomised controlled trial. Respir. Res. 2013, 14, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodgson, D.; Anderson, J.; Reynolds, C.; Oborne, J.; Meakin, G.; Bailey, H.; Shaw, D.; Mortimer, K.; Harrison, T. The Effects of Azithromycin in Treatment-Resistant Cough: A Randomized, Double-Blind, Placebo-Controlled Trial. Chest 2016, 149, 1052–1060. [Google Scholar] [CrossRef] [Green Version]
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of COPD; GOLD: Fontana, WI, USA, 2017. [Google Scholar]
- Zysman, M.; Baptista, B.R.; Soumagne, T.; da Silva, V.M.; Martin, C.; de Menonville, C.T.; Boyer, L.; Degano, B.; Panzini, C.M.; Burgel, P.R.; et al. Optimisation du traitement médicamenteux des patients atteints de BPCO en état stable. Position de la Société de pneumologie de langue française. Actualisation 2021. Rev. Des. Mal. Respir. 2021, 38, 539–561. [Google Scholar] [CrossRef] [PubMed]
- Volpato, M.; Vialaret, J.; Hirtz, C.; Petit, A.; Suehs, C.; Patarin, J.; Matzner-Lober, E.; Vachier, I.; Molinari, N.; Bourdin, A.; et al. Rheology predicts sputum eosinophilia in patients with muco-obstructive lung diseases. Biochem. Biophys. Res. Commun. 2022, 622, 64–71. [Google Scholar] [CrossRef]
- Hastie, A.T.; Martinez, F.J.; Curtis, J.L.; Doerschuk, C.M.; Hansel, N.N.; Christenson, S.; Putcha, N.; Ortega, V.E.; Li, X.; Barr, R.G.; et al. Association of sputum and blood eosinophil concentrations with clinical measures of COPD severity: An analysis of the SPIROMICS cohort. Lancet Respir. Med. 2017, 5, 956–967. [Google Scholar] [CrossRef]
- Monz, B.U.; Sachs, P.; McDonald, J.; Crawford, B.; Nivens, M.C.; Tetzlaff, K. Responsiveness of the cough and sputum assessment questionnaire in exacerbations of COPD and chronic bronchitis. Respir. Med. 2010, 104, 534–541. [Google Scholar] [CrossRef] [Green Version]
- Crawford, B.; Monz, B.; Hohlfeld, J.; Roche, N.; Rubin, B.; Magnussen, H.; Nivens, C.; Ghafouri, M.; McDonald, J.; Tetzlaff, K. Development and validation of a cough and sputum assessment questionnaire. Respir. Med. 2008, 102, 1545–1555. [Google Scholar] [CrossRef] [PubMed]
- Deslee, G.; Burgel, P.-R.; Escamilla, R.; Chanez, P.; Court-Fortune, I.; Nesme-Meyer, P.; Brinchault-Rabin, G.; Perez, T.; Jebrak, G.; Caillaud, D.; et al. Impact of current cough on health-related quality of life in patients with COPD. Int. J. Chronic Obs. Pulmon. Dis. 2016, 11, 2091–2097. [Google Scholar] [CrossRef] [Green Version]
- Tagaya, E.; Yagi, O.; Sato, A.; Arimura, K.; Takeyama, K.; Kondo, M.; Tamaoki, J. Effect of tiotropium on mucus hypersecretion and airway clearance in patients with COPD. Pulm. Pharmacol. Ther. 2016, 39, 81–84. [Google Scholar] [CrossRef]
- Patarin, J.; Ghiringhelli, É.; Darsy, G.; Obamba, M.; Bochu, P.; Camara, B.; Quétant, S.; Cracowski, J.-L.; Cracowski, C.; Robert de Saint Vincent, M. Rheological analysis of sputum from patients with chronic bronchial diseases. Sci. Rep. 2020, 10, 15685. [Google Scholar] [CrossRef]
- Wedzicha, J.A.; Banerji, D.; Chapman, K.R.; Vestbo, J.; Roche, N.; Ayers, R.T.; Thach, C.; Fogel, R.; Patalano, F.; Vogelmeier, C.F. Indacaterol–Glycopyrronium versus Salmeterol–Fluticasone for COPD. N. Engl. J. Med. 2016, 374, 2222–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, M.K.; Muellerova, H.; Curran-Everett, D.; Dransfield, M.T.; Washko, G.R.; Regan, E.A.; Bowler, R.P.; Beaty, T.H.; Hokanson, J.E.; Lynch, D.A.; et al. GOLD 2011 disease severity classification in COPDGene: A prospective cohort study. Lancet Respir. Med. 2013, 1, 43–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Subjects aged 40–85 years | Patients who are pregnant or breastfeeding |
| Diagnosis of COPD for at least 1 year | Patients who are prisoners or under other forms of judicial protection |
| Optimal treatment according to GOLD guidelines | Patients under any form of guardianship |
| ≥3 exacerbations in the past 12 months | Participation in another interventional protocol |
| Spontaneous or induced sputum production | Patients who have received azithromycin in the past 3 months |
| Electrocardiogram: corrected QTC < 450 ms in men; QTC < 470 ms in women | Patients found to have bronchiectasis in a chest CT scan |
| Normal audiogram | Patients who have a known hypersensitivity to azithromycin, or any other macrolide |
| Written and signed informed consent form | Concomitant use of a medication contraindicated with azithromycin (dihydroergotamine, ergotamine, cisapride, or colchicine) |
| Subjects must be able to attend all planned visits and comply with all test procedures | Patients with other respiratory diseases or associated lung infections |
| Beneficiary of, or affiliated with, the French social security system | Severe hepatic insufficiency and severe cholestasis |
| GFR < 40 mL/min | |
| Patients with hematological malignancies who have undergone allogeneic hematopoietic stem-cell transplantation | |
| Patients with galactose intolerance, Lapp lactase deficiency, or glucose-galactose malabsorption syndrome (a rare hereditary disease) |
| Pre-Inclusion | Inclusion | Run-In | Follow-Up | |||||
|---|---|---|---|---|---|---|---|---|
| Vpre | Vinc * | RI | V0 | V3 | V6 | V9 | V12 | |
| d–60 to d–28 | d–30 to d–15 | 15 Days | d0 | 3 Mo ± 7 d | 6 Mo ± 7 d | 9 Mo ± 7 d | 12 Mo ± 7 d | |
| Eligibility/Inclusion | ||||||||
| Verification of Eligibility Criteria | ✓ | ✓ | ||||||
| Oral and Written Information | ✓ | |||||||
| Electrocardiogram | ✓ | |||||||
| Liver Blood Test | ✓ | |||||||
| Audiogram | ✓ | |||||||
| Written Consent | ✓ | |||||||
| Pregnancy Test (-hcg), if applicable | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Verification of Patient Stability (exacerbations) | ✓ | |||||||
| Experimental Intervention | ||||||||
| Randomization | ✓ | |||||||
| Standard Management, or according to sputum rheology | ✓ | |||||||
| Assessments | ||||||||
| Checking Patient’s Logbook: symptoms, exacerbations, unexpected use of drugs or medical resources | ✓ | |||||||
| Plethysmography | ✓ | ✓ | ||||||
| Spirometry | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Questionnaires | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Blood Test: blood cell count, CCSP * | ✓ | ✓ | ||||||
| Sputum Analysis: rheology, bacteriology | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Side Effects | ✓ | ✓ | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charriot, J.; Zysman, M.; Guilleminault, L.; Volpato, M.; Fort-Petit, A.; Vachier, I.; Patarin, J.; Suehs, C.; Ahmed, E.; Molinari, N.; et al. Sputum-Rheology-Based Strategy for Guiding Azithromycin Prescription in COPD Patients with Frequent Exacerbations: A Randomized, Controlled Study (“COPD CARhE”). Biomedicines 2023, 11, 740. https://doi.org/10.3390/biomedicines11030740
Charriot J, Zysman M, Guilleminault L, Volpato M, Fort-Petit A, Vachier I, Patarin J, Suehs C, Ahmed E, Molinari N, et al. Sputum-Rheology-Based Strategy for Guiding Azithromycin Prescription in COPD Patients with Frequent Exacerbations: A Randomized, Controlled Study (“COPD CARhE”). Biomedicines. 2023; 11(3):740. https://doi.org/10.3390/biomedicines11030740
Chicago/Turabian StyleCharriot, Jeremy, Maeva Zysman, Laurent Guilleminault, Mathilde Volpato, Aurelie Fort-Petit, Isabelle Vachier, Jeremy Patarin, Carey Suehs, Engi Ahmed, Nicolas Molinari, and et al. 2023. "Sputum-Rheology-Based Strategy for Guiding Azithromycin Prescription in COPD Patients with Frequent Exacerbations: A Randomized, Controlled Study (“COPD CARhE”)" Biomedicines 11, no. 3: 740. https://doi.org/10.3390/biomedicines11030740