
Long-Interval Intracortical Inhibition and the Cortical Silent Period in Youth

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. TMS and EMG Procedures and Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fatih, P.; Kucuker, M.U.; Vande Voort, J.L.; Camsari, D.D.; Farzan, F.; Croarkin, P.E. A Systematic Review of Long-Interval Intracortical Inhibition as a Biomarker in Neuropsychiatric Disorders. Front. Psychiatry 2021, 12, 678088. [Google Scholar] [CrossRef] [PubMed]
- Mehta, U.M.; Ektare, A.; Jakhar, J.; Basavaraju, R.; Sanjay, T.N.; Naik, S.S.; Syed, F.A.; Bhargav, P.H.; Reddy, P.V.; Kelkar, R.S.; et al. A transdiagnostic evaluation of cortical inhibition in severe mental disorders using Transcranial Magnetic Stimulation. J. Psychiatr. Res. 2021, 143, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Cryan, J.F.; Kaupmann, K. Don’t worry ‘B’ happy!: A role for GABAB receptors in anxiety and depression. Trends Pharmacol. Sci. 2005, 26, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Jeng, J.-S.; Li, C.-T.; Lin, H.-C.; Tsai, S.-J.; Bai, Y.-M.; Su, T.-P.; Chang, Y.-W.; Cheng, C.-M. Antidepressant-resistant depression is characterized by reduced short- and long-interval cortical inhibition. Psychol. Med. 2019, 50, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Kinjo, M.; Wada, M.; Nakajima, S.; Tsugawa, S.; Nakahara, T.; Blumberger, D.M.; Mimura, M.; Noda, Y. Transcranial magnetic stimulation neurophysiology of patients with major depressive disorder: A systematic review and meta-analysis. Psychol. Med. 2020, 51, 1–10. [Google Scholar] [CrossRef]
- Ziemann, U.; Reis, J.; Schwenkreis, P.; Rosanova, M.; Strafella, A.; Badawy, R.; Müller-Dahlhaus, F. TMS and drugs revisited 2014. Clin. Neurophysiol. 2015, 126, 1847–1868. [Google Scholar] [CrossRef] [PubMed]
- Mooney, R.A.; Cirillo, J.; Byblow, W.D. GABA and primary motor cortex inhibition in young and older adults: A multimodal reliability study. J. Neurophysiol. 2017, 118, 425–433. [Google Scholar] [CrossRef] [Green Version]
- McGinley, M.; Hoffman, R.L.; Russ, D.W.; Thomas, J.S.; Clark, B.C. Older adults exhibit more intracortical inhibition and less intracortical facilitation than young adults. Exp. Gerontol. 2010, 45, 671–678. [Google Scholar] [CrossRef] [Green Version]
- Croarkin, P.E.; Nakonezny, P.A.; Lewis, C.P.; Zaccariello, M.J.; Huxsahl, J.E.; Husain, M.M.; Kennard, B.D.; Emslie, G.J.; Daskalakis, Z.J. Developmental aspects of cortical excitability and inhibition in depressed and healthy youth: An exploratory study. Front. Hum. Neurosci. 2014, 8, 669. [Google Scholar] [CrossRef] [Green Version]
- Croarkin, P.E.; Nakonezny, P.A.; Husain, M.M.; Melton, T.; Buyukdura, J.S.; Kennard, B.D.; Emslie, G.J.; Kozel, F.A.; Daskalakis, Z.J. Evidence for Increased Glutamatergic Cortical Facilitation in Children and Adolescents with Major Depressive Disorder. JAMA Psychiatry 2013, 70, 291–299. [Google Scholar] [CrossRef]
- Croarkin, P.E.; Nakonezny, P.A.; Husain, M.M.; Port, J.D.; Melton, T.; Kennard, B.D.; Emslie, G.J.; Kozel, F.A.; Daskalakis, Z.J. Evidence for Pretreatment LICI Deficits Among Depressed Children and Adolescents with Nonresponse to Fluoxetine. Brain Stimul. 2014, 7, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Lewis, C.P.; Nakonezny, P.A.; Blacker, C.; Vande Voort, J.L.; Port, J.D.; Worrell, G.A.; Jo, H.J.; Daskalakis, Z.J.; Croarkin, P.E. Cortical inhibitory markers of lifetime suicidal behavior in depressed adolescents. Neuropsychopharmacology 2018, 43, 1822–1831. [Google Scholar] [CrossRef] [PubMed]
- Keel, J.C.; Smith, M.J.; Wassermann, E.M. A safety screening questionnaire for transcranial magnetic stimulation. Clin. Neurophysiol. 2001, 112, 720. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.; Birmaher, B.; Brent, D.; Rao, U.; Flynn, C.; Moreci, P.; Williamson, D.; Ryan, N. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): Initial Reliability and Validity Data. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Mayes, T.L.; Bernstein, I.H.; Haley, C.L.; Kennard, B.D.; Emslie, G.J. Psychometric properties of the Children’s Depression Rating Scale-Revised in adolescents. J. Child Adolesc. Psychopharmacol. 2010, 20, 513–516. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, P.B.; Brown, T.L.; Marston, N.A.; Oxley, T.; de Castella, A.; Daskalakis, Z.J.; Kulkarni, J. A transcranial magnetic stimulation study of abnormal cortical inhibition in schizophrenia. Psychiatry Res. 2003, 118, 197–207. [Google Scholar] [CrossRef]
- Daskalakis, Z.J.; Christensen, B.K.; Chen, R.; Fitzgerald, P.B.; Zipursky, R.B.; Kapur, S. Evidence for impaired cortical inhibition in schizophrenia using transcranial magnetic stimulation. Arch. Gen. Psychiatry 2002, 59, 347–354. [Google Scholar] [CrossRef] [Green Version]
- Rossini, P.M.; Burke, D.; Chen, R.; Cohen, L.G.; Daskalakis, Z.; Di Iorio, R.; Di Lazzaro, V.; Ferreri, F.; Fitzgerald, P.B.; George, M.S.; et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N. Committee. Clin. Neurophysiol. 2015, 126, 1071–1107. [Google Scholar] [CrossRef]
- De Beaumont, L.; Mongeon, D.; Tremblay, S.; Messier, J.; Prince, F.; Leclerc, S.; Lassonde, M.; Théoret, H. Persistent Motor System Abnormalities in Formerly Concussed Athletes. J. Athl. Train. 2011, 46, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Farzan, F.; Barr, M.S.; Levinson, A.J.; Chen, R.; Wong, W.; Fitzgerald, P.B.; Daskalakis, Z.J. Reliability of Long-Interval Cortical Inhibition in Healthy Human Subjects: A TMS–EEG Study. J. Neurophysiol. 2010, 104, 1339–1346. [Google Scholar] [CrossRef]
- Tremblay, S.; Beaulé, V.; Lepage, J.; Théoret, H. Anodal transcranial direct current stimulation modulates GABAB-related intracortical inhibition in the M1 of healthy individuals. NeuroReport 2013, 24, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Benwell, N.; Mastaglia, F.L.; Thickbroom, G.W. Differential changes in long-interval intracortical inhibition and silent period duration during fatiguing hand exercise. Exp. Brain Res. 2007, 179, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Kimiskidis, V.K.; Papagiannopoulos, S.; Kazis, D.A.; Sotirakoglou, K.; Vasiliadis, G.; Zara, F.; Kazis, A.; Mills, K.R. Lorazepam-induced effects on silent period and corticomotor excitability. Exp. Brain Res. 2006, 173, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Kilb, W. Development of the GABAergic System from Birth to Adolescence. Neuroscientist 2011, 18, 613–630. [Google Scholar] [CrossRef]
- Rakhade, S.N.; Jensen, F.E. Epileptogenesis in the immature brain: Emerging mechanisms. Nat. Rev. Neurol. 2009, 5, 380–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverstein, F.S.; Jensen, F.E. Neonatal seizures. Ann. Neurol. 2007, 62, 112–120. [Google Scholar] [CrossRef]
- Hermans, L.; Levin, O.; Maes, C.; van Ruitenbeek, P.; Heise, K.-F.; Edden, R.A.; Puts, N.A.; Peeters, R.; King, B.R.; Meesen, R.L.J.; et al. GABA levels and measures of intracortical and interhemispheric excitability in healthy young and older adults: An MRS-TMS study. Neurobiol. Aging 2018, 65, 168–177. [Google Scholar] [CrossRef]
- Fung, S.J.; Webster, M.J.; Weickert, C.S. Expression of VGluT1 and VGAT mRNAs in human dorsolateral prefrontal cortex during development and in schizophrenia. Brain Res. 2011, 1388, 22–31. [Google Scholar] [CrossRef]
- Zeugin, D.; Ionta, S. Anatomo-Functional Origins of the Cortical Silent Period: Spotlight on the Basal Ganglia. Brain Sci. 2021, 11, 705. [Google Scholar] [CrossRef]
- Beynel, L.; Chauvin, A.; Guyader, N.; Harquel, S.; Marendaz, C. Age-related changes in intracortical inhibition are mental-cognitive state-dependent. Biol. Psychol. 2014, 101, 9–12. [Google Scholar] [CrossRef]
- Northoff, G.; Sibille, E. Why are cortical GABA neurons relevant to internal focus in depression? A cross-level model linking cellular, biochemical and neural network findings. Mol. Psychiatry 2014, 19, 966–977. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Total Sample (n = 61) | Healthy (n = 16) | Depression (n = 45) |
|---|---|---|---|
| Age, y | 15.5 (1.7) | 14.3 (1.7) | 15.9 (1.6) |
| Sex | |||
| Female | 34 (56) | 5 (31) | 29 (64) |
| Male | 27 (44) | 11 (69) | 16 (36) |
| Right-handed | 56 (92) | 14 (88) | 42 (93) |
| Race/ethnicity | |||
| Asian | 1 (2) | 0 (0) | 1 (2) |
| Black | 7 (11) | 5 (31) | 2 (4) |
| Hispanic/Latino | 2 (3) | 1 (6) | 1 (2) |
| Multiple/Other | 6 (10) | 2 (13) | 4 (9) |
| White | 45 (74) | 8 (50) | 37 (82) |
| CDRS-R score | 36.1 (15.5) | 19.6 (1.9) | 41.9 (13.8) |
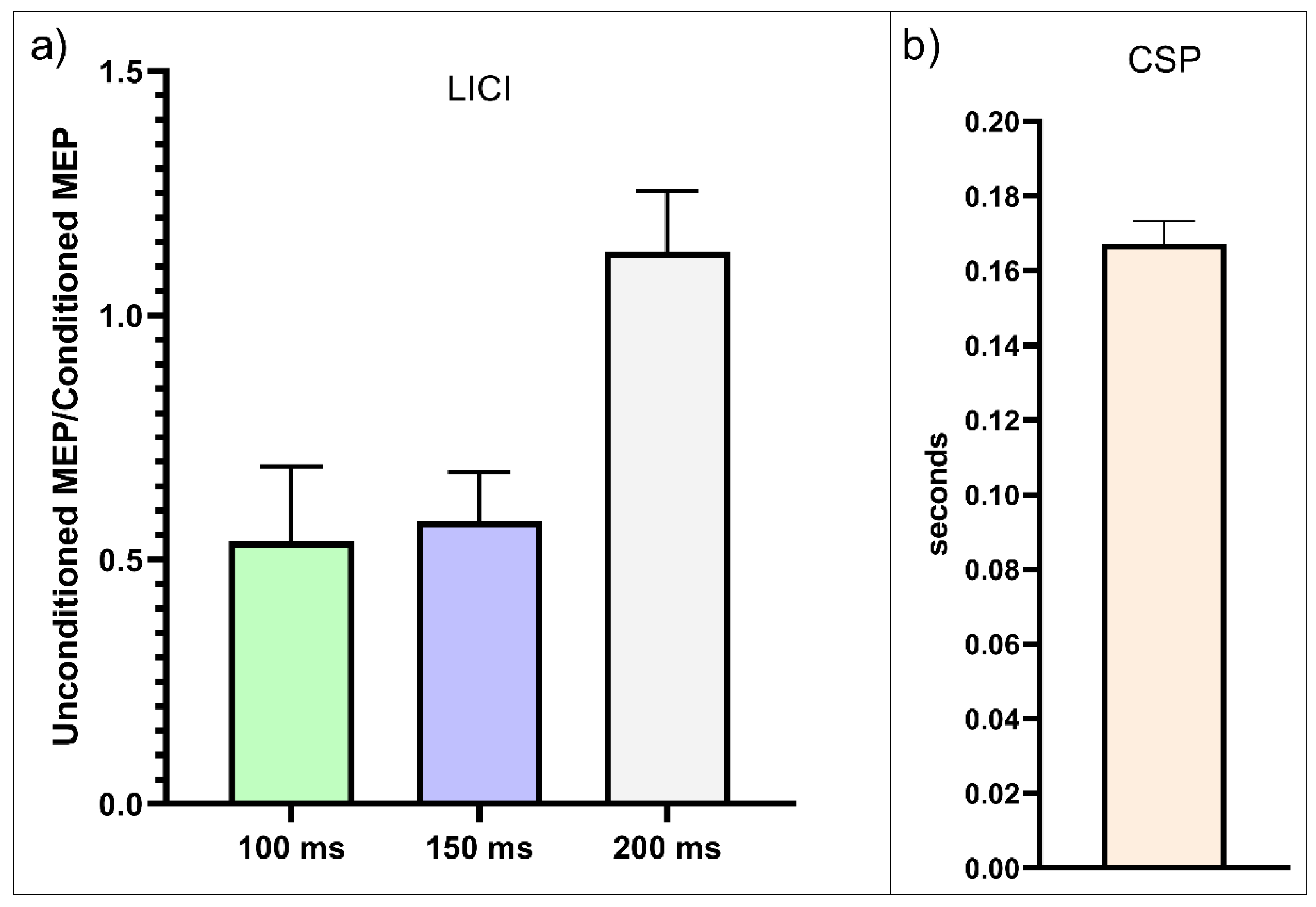
| CSP a | 167.2 (48.1) | 179.8 (43.6) | 162.7 (49.2) |
| LICI b | |||
| ISI = 100 ms | 0.5 (1.2) | 0.21 (0.3) | 0.65 (1.37) |
| ISI = 150 ms | 0.58 (0.79) | 0.36 (0.51) | 0.66 (0.86) |
| ISI = 200 ms | 1.13 (1) | 1.33 (1.2) | 1.06 (0.88) |
| Duration of depression, y | NA | NA | 2.0 (1.8) |
| Prescribed psychotropic medications | 27 (44) | 0 (0) | 27 (60) |
| Family psychiatric history | 44 (72) | 0 (0) | 44 (98) |
| Total Sample (n = 61) | Healthy (n = 16) | Depression (n = 45) | ||||
|---|---|---|---|---|---|---|
| Interstimulus Interval, ms | Spearman p | p Value | Spearman p | p Value | Spearman p | p Value |
| 100 | −0.2421 | 0.06 | −0.4059 | 0.12 | −0.1132 | 0.46 |
| 150 | −0.1612 | 0.21 | −0.318 | 0.24 | −0.0042 | 0.98 |
| 200 | −0.0507 | 0.70 | −0.2971 | 0.30 | −0.0004 | >0.99 |
| Total Sample (n = 57) | Healthy (n = 16) | Depression (n = 41) | ||||
|---|---|---|---|---|---|---|
| Interstimulus Interval, ms | Spearman p | p Value | Spearman p | p Value | Spearman p | p Value |
| 100 | −0.285 | 0.03 * | −0.4059 | 0.12 | −0.172 | 0.28 |
| 150 | −0.1944 | 0.14 | −0.318 | 0.24 | −0.0395 | 0.8 |
| 200 | −0.076 | 0.05 | −0.2971 | 0.3 | −0.027 | 0.867 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahern, K.B.; Garzon, J.F.; Yuruk, D.; Saliba, M.; Ozger, C.; Vande Voort, J.L.; Croarkin, P.E. Long-Interval Intracortical Inhibition and the Cortical Silent Period in Youth. Biomedicines 2023, 11, 409. https://doi.org/10.3390/biomedicines11020409
Ahern KB, Garzon JF, Yuruk D, Saliba M, Ozger C, Vande Voort JL, Croarkin PE. Long-Interval Intracortical Inhibition and the Cortical Silent Period in Youth. Biomedicines. 2023; 11(2):409. https://doi.org/10.3390/biomedicines11020409
Chicago/Turabian StyleAhern, Kelly B., Juan F. Garzon, Deniz Yuruk, Maria Saliba, Can Ozger, Jennifer L. Vande Voort, and Paul E. Croarkin. 2023. "Long-Interval Intracortical Inhibition and the Cortical Silent Period in Youth" Biomedicines 11, no. 2: 409. https://doi.org/10.3390/biomedicines11020409