
Prevalence of Autoimmune and Autoinflammatory Diseases in Chronic Urticaria: Pathogenetic, Diagnostic and Therapeutic Implications
 , ,
, ,  and
and 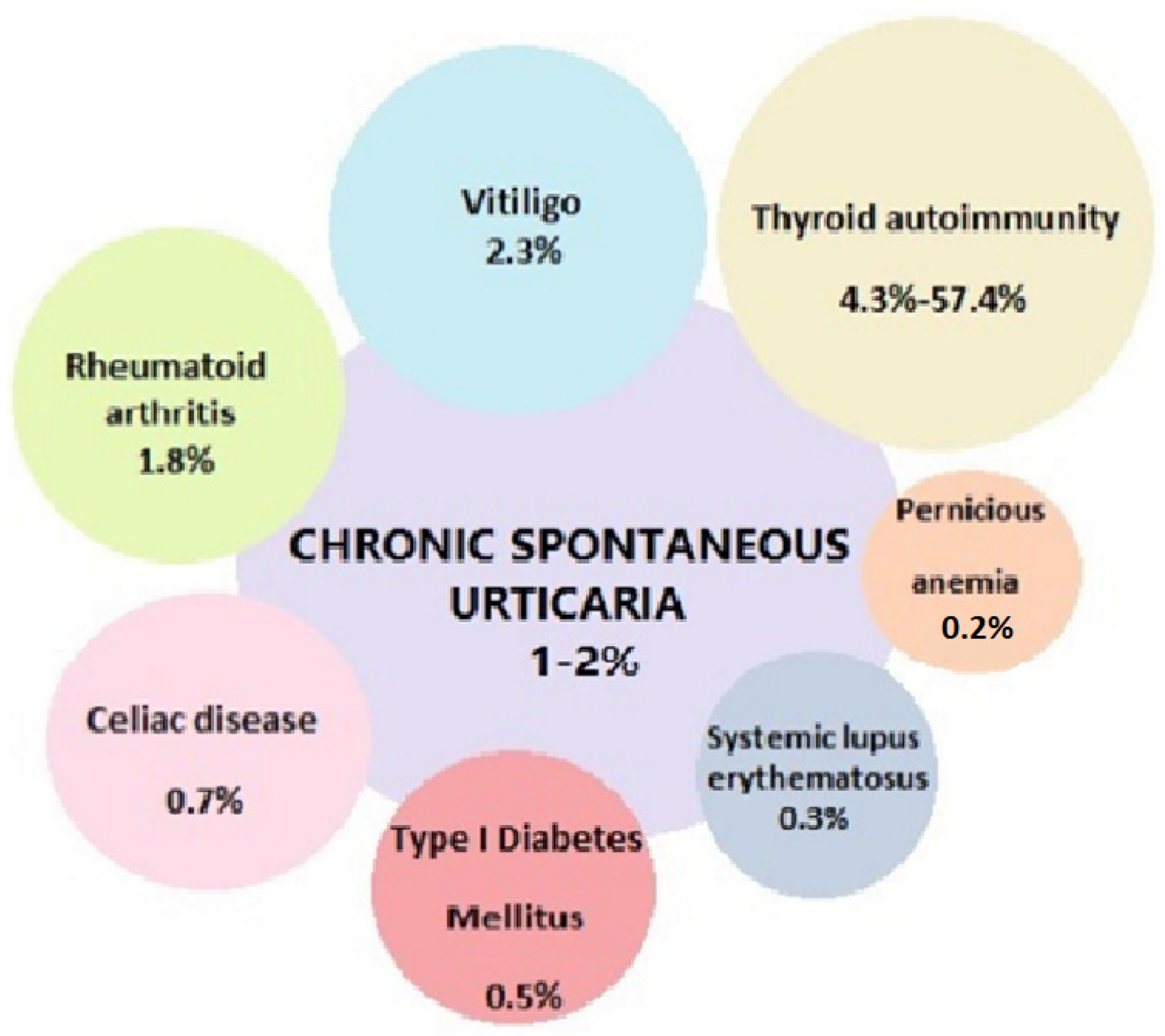{kind=link}
{kind=link}
Abstract
:1. Chronic Urticaria
1.1. Physiopathology
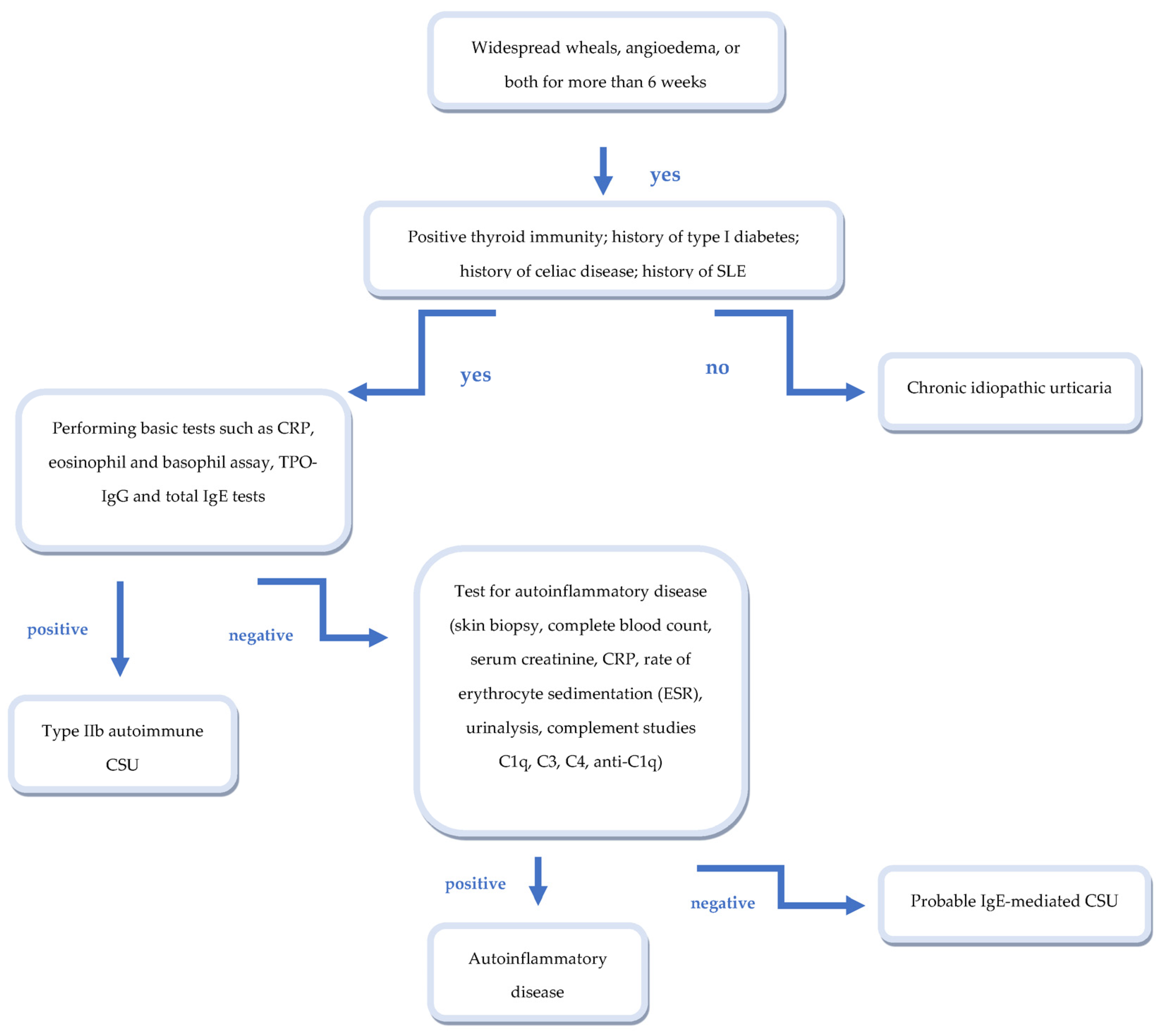
1.2. Two Endotypes of CSU
2. Associations with Other Autoimmune Diseases
2.1. Organ-Specific Autoimmune Disease and CSU
Thyroid Autoimmunity
2.2. Type I Diabetes Mellitus
2.3. Celiac Disease
2.4. Vitiligo
2.5. Pernicious Anemia
Addison’s Disease
3. Non-Organ Specific Autoimmune Diseases and CU
4. CU and Other Immune-Mediated Diseases
5. CSU and Autoinflammatory Diseases
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sánchez-Borges, M.; Ansotegui, I.J.; Baiardini, I.; Bernstein, J.; Canonica, G.W.; Ebisawa, M.; Gomez, M.; Gonzalez-Diaz, S.N.; Martin, B.; Morais-Almeida, M.; et al. The challenges of chronic urticaria part 1: Epidemiology, immunopathogenesis, comorbidities, quality of life, and management. World Allergy Organ. J. 2021, 14, 100533. [Google Scholar] [CrossRef]
- Wertenteil, S.; Strunk, A.; Garg, A. Prevalence estimates for chronic urticaria in the United States: A sex- and age-adjusted population analysis. J. Am. Acad. Dermatol. 2019, 81, 152–156. [Google Scholar] [CrossRef]
- Moestrup, K.; Ghazanfar, M.N.; Thomsen, S.F. Patient-reported outcomes (PROs) in chronic urticaria. Int. J. Dermatol. 2017, 56, 1342–1348. [Google Scholar] [CrossRef]
- Zuberbier, T.; Balke, M.; Worm, M.; Edenharter, G.; Maurer, M. Epidemiology of urticaria: A representative cross-sectional population survey. Clin. Exp. Dermatol. 2010, 35, 869–873. [Google Scholar] [CrossRef] [PubMed]
- Baiardini, I.; Giardini, A.; Pasquali, M.; Dignetti, P.; Guerra, L.; Specchia, C.; Braido, F.; Majani, G.; Canonica, G.W. Quality of life and patients’ satisfaction in chronic urticaria and respiratory allergy. Allergy 2003, 58, 621–623. [Google Scholar] [CrossRef]
- Staubach, P.; Eckhardt-Henn, A.; Dechene, M.; Vonend, A.; Metz, M.; Magerl, M.; Breuer, P.; Maurer, M. Quality of life in patients with chronic urticaria is differentially impaired and determined by psychiatric comorbidity. Br. J. Dermatol. 2006, 154, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Stepaniuk, P.; Kan, M.; Kanani, A. Natural history, prognostic factors and patient perceived response to treatment in chronic spontaneous urticaria. Allergy Asthma Clin. Immunol. 2020, 16, 63. [Google Scholar] [CrossRef] [PubMed]
- Gaig, P.; Olona, M.; Lejarazu, D.M.; Caballero, M.T.; Domínguez, F.J.; Echechipia, S.; Abujeta, J.L.G.; A Gonzalo, M.; Lleonart, R.; Cócera, C.M.; et al. Epidemiology of urticaria in Spain. J. Investig. Allergol. Clin. Immunol. 2004, 14, 214–220. [Google Scholar]
- Kolkhir, P.; Andre, F.; Church, M.K.; Maurer, M.; Metz, M. Potential blood biomarkers in chronic spontaneous urticaria. Clin. Exp. Allergy 2017, 47, 19–36. [Google Scholar] [CrossRef]
- Zuberbier, T.; Aberer, W.; Asero, R.; Bindslev-Jensen, C.; Brzoza, Z.; Canonica, G.W.; Church, M.K.; Ensina, L.F.; Giménez-Arnau, A.; Godse, K.; et al. The EAACI/GA2LEN/EDF/WAO Guideline for the definition, classification, diagnosis, and management of urticaria: The 2013 revision and update. Allergy 2014, 69, 868–887. [Google Scholar] [CrossRef]
- Ensina, L.F.; Cusato-Ensina, A.P.; Cardona, R. Advances in the pathogenesis representing definite outcomes in chronic urticaria. Curr. Opin. Allergy Clin. Immunol. 2019, 19, 193–197. [Google Scholar] [CrossRef]
- Schoepke, N.; Asero, R.; Ellrich, A.; Ferrer, M.; Gimenez-Arnau, A.; Al, E.; Schmid-Grendelmeier, P. Biomarkers and clinical characteristics of autoimmune chronic spontaneous urticaria: Results of the PURIST Study. Allergy 2019, 74, 2427–2436. [Google Scholar] [CrossRef]
- Chanprapaph, K.; Iamsumang, W.; Wattanakrai, P.; Vachiramon, V. Thyroid Autoimmunity and Autoimmunity in Chronic Spontaneous Urticaria Linked to Disease Severity, Therapeutic Response, and Time to Remission in Patients with Chronic Spontaneous Urticaria. BioMed Res. Int. 2018, 2018, 9856843. [Google Scholar] [CrossRef] [Green Version]
- Sánchez, J.; Sánchez, A.; Cardona, R. Causal Relationship Between Anti-TPO IgE and Chronic Urticaria by in Vitro and in Vivo Tests. Allergy Asthma Immunol. Res. 2019, 11, 29–42. [Google Scholar] [CrossRef]
- Altrichter, S.; Peter, H.J.; Pisarevskaja, D.; Metz, M.; Martus, P.; Maurer, M. IgE mediated autoallergy against thyroid peroxidase—A novel pathomechanism of chronic spontaneous urticaria? PLoS ONE 2011, 6, e14794. [Google Scholar] [CrossRef]
- Altrichter, S.; Zampeli, V.; Ellrich, A.; Zhang, K.; Church, M.K.; Maurer, M. IgM and IgA in addition to IgG autoantibodies against FcvarepsilonRIalpha are frequent and associated with disease markers of chronic spontaneous urticaria. Allergy 2020, 75, 3208–3215. [Google Scholar] [CrossRef]
- Bracken, S.J.; Abraham, S.; MacLeod, A.S. Autoimmune Theories of Chronic Spontaneous Urticaria. Front. Immunol. 2019, 10, 627. [Google Scholar] [CrossRef]
- Konstantinou, G.N.; Asero, R.; Ferrer, M.; Knol, E.F.; Maurer, M.; Raap, U.; Schmid-Grendelmeier, P.; Skol, P.S.; Grattan, C.E.H. EAACI taskforce position paper: Evidence for autoimmune urticaria and proposal for defining diagnostic criteria. Allergy 2013, 68, 27–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maurer, M.; Eyerich, K.; Eyerich, S.; Ferrer, M.; Gutermuth, J.; Hartmann, K.; Jakob, T.; Kapp, A.; Kolkhir, P.; Larenas-Linnemann, D.; et al. Urticaria: Collegium Internationale Allergologicum (CIA) Update 2020. Int. Arch. Allergy Immunol. 2020, 181, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Kolkhir, P.; Altrichter, S.; Asero, R.; Daschner, A.; Ferrer, M.; Giménez-Arnau, A.; Hawro, T.; Jakob, T.; Kinaciyan, T.; Kromminga, A.; et al. Autoimmune Diseases Are Linked to Type IIb Autoimmune Chronic Spontaneous Urticaria. Allergy Asthma Immunol. Res. 2021, 13, 545–559. [Google Scholar] [CrossRef] [PubMed]
- Kolkhir, P.; Borzova, E.; Grattan, C.; Asero, R.; Pogorelov, D.; Maurer, M. Autoimmune comorbidity in chronic spontaneous urticaria: A systematic review. Autoimmun. Rev. 2017, 16, 1196–1208. [Google Scholar] [CrossRef]
- Fridkis-Hareli, M. Immunogenetic mechanisms for the coexistence of organ-specific and systemic autoimmune diseases. J. Autoimmune Dis. 2008, 5, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Mastrandrea, L.D. An Overview of Organ-Specific Autoimmune Diseases Including Immunotherapy. Immunol. Investig. 2015, 44, 803–816. [Google Scholar] [CrossRef] [PubMed]
- Gangemi, S.; Saitta, S.; Lombardo, G.; Patafi, M.; Benvenga, S. Serum thyroid autoantibodies in patients with idiopathic either acute or chronic urticaria. J. Endocrinol. Investig. 2009, 32, 107–110. [Google Scholar] [CrossRef]
- Bagnasco, M.; Minciullo, P.L.; Schiavo, M.; Saraceno, G.; Gangemi, S.; Benvenga, S. Urticaria and Thyroid Autoimmunity. Thyroid 2011, 21, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Kolkhir, P.; Metz, M.; Altrichter, S.; Maurer, M. Comorbidity of chronic spontaneous urticaria and autoimmune thyroid diseases: A systematic review. Allergy 2017, 72, 1440–1460. [Google Scholar] [CrossRef] [Green Version]
- Confino-Cohen, R.; Chodick, G.; Shalev, V.; Leshno, M.; Kimhi, O.; Goldberg, A. Chronic urticaria and autoimmunity: Associations found in a large population study. J. Allergy Clin. Immunol. 2012, 129, 1307–1313. [Google Scholar] [CrossRef] [PubMed]
- Zuberbier, T.; Abdul Latiff, A.H.; Abuzakouk, M.; Aquilina, S.; Asero, R.; Baker, D.; Ballmer-Weber, B.; Bangert, C.; Ben-Shoshan, M.; Bernstein, J.A.; et al. The international EAACI/GA(2)LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy 2022, 77, 734–766. [Google Scholar] [CrossRef]
- Ruggeri, R.M.; Vita, G.; D’Angelo, A.G.; Quattrocchi, P.; Certo, R.; Benvenga, S.; Cannavò, S.; Gangemi, S. The unusual association of Graves’ disease, chronic spontaneous urticaria, and premature ovarian failure: Report of a case and HLA haplotype characterization. Arq. Bras. Endocrinol. Metabol. 2013, 57, 748–752. [Google Scholar] [CrossRef] [Green Version]
- Fusari, A.; Colangelo, C.; Bonifazi, F.; Antonicelli, L. The autologous serum skin test in the follow-up of patients with chronic urticaria. Allergy 2005, 60, 256–258. [Google Scholar] [CrossRef]
- Kilic, G.; Güler, N.; Süleyman, A.; Tamay, Z. Chronic urticaria and autoimmunity in children. Pediatr. Allergy Immunol. 2010, 21, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Schocket, A.L. Chronic urticaria: Pathophysiology and etiology, or the what and why. Allergy Asthma Proc. 2006, 27, 90–95. [Google Scholar] [PubMed]
- Tienforti, D.; Di Giulio, F.; Spagnolo, L.; Castellini, C.; Totaro, M.; Muselli, M.; Francavilla, S.; Baroni, M.G.; Barbonetti, A. Chronic urticaria and thyroid autoimmunity: A meta-analysis of case–control studies. J. Endocrinol. Investig. 2022, 45, 1317–1326. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Kishimoto, T. The Biology and Medical Implications of Interleukin-6. Cancer Immunol. Res. 2014, 2, 288–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasperska-Zajac, A.; Sztylc, J.; Machura, E.; Jop, G. Plasma IL-6 concentration correlates with clinical disease activity and serum C-reactive protein concentration in chronic urticaria patients. Clin. Exp. Allergy 2011, 41, 1386–1391. [Google Scholar] [CrossRef]
- Bai, X.; Sun, J.; Wang, W.; Shan, Z.; Zheng, H.; Li, Y.; Zhao, Y.; Gong, M.; Teng, W. Increased differentiation of Th22 cells in Hashimoto’s thyroiditis. Endocr. J. 2014, 61, 1181–1190. [Google Scholar] [CrossRef] [Green Version]
- Khan, F.A.; Al-Jameil, N.; Khan, M.F.; Al-Rashid, M.; Tabassum, H. Thyroid dysfunction: An autoimmune aspect. Int. J. Clin. Exp. Med. 2015, 8, 6677–6681. [Google Scholar]
- Valencia, X.; Lipsky, P.E. CD4+ CD25+ FoxP3+ regulatory T cells in autoimmune diseases. Nat. Clin. Pract. Rheumatol. 2007, 3, 619–626. [Google Scholar] [CrossRef]
- Arshi, S.; Babaie, D.; Nabavi, M.; Tebianian, M.; Ghalehbaghi, B.; Jalali, F.; Ahmadvand, A.; Gholami, R. Circulating level of CD4+ CD25+ FOXP3+ T cells in patients with chronic urticaria. Int. J. Dermatol. 2014, 53, e561–e566. [Google Scholar] [CrossRef]
- Sun, R.-S.; Sui, J.-F.; Chen, X.-H.; Ran, X.-Z.; Yang, Z.-F.; Guan, W.-D.; Yang, T. Detection of CD4+ CD25+ FOXP3+ regulatory T cells in peripheral blood of patients with chronic autoimmune urticaria. Australas. J. Dermatol. 2010, 52, e15–e18. [Google Scholar] [CrossRef]
- Chen, W.-C.; Chiang, B.-L.; Liu, H.E.; Leu, S.-J.; Lee, Y.-L. Defective functions of circulating CD4+ CD25+ and CD4+ CD25− T cells in patients with chronic ordinary urticaria. J. Dermatol. Sci. 2008, 51, 121–130. [Google Scholar] [CrossRef]
- Glick, A.B.; Wodzinski, A.; Fu, P.; Levine, A.D.; Wald, D.N.; Ramos-Leví, A.M.; Marazuela, M.; Inaba, H.; De Groot, L.J.; Akamizu, T.; et al. Impairment of Regulatory T-Cell Function in Autoimmune Thyroid Disease. Thyroid 2013, 23, 871–878. [Google Scholar] [CrossRef]
- Xue, H.; Yu, X.; Ma, L.; Song, S.; Li, Y.; Zhang, L.; Yang, T.; Liu, H. The possible role of CD4(+)CD25(high)Foxp3(+)/CD4(+)IL-17A(+) cell imbalance in the autoimmunity of patients with Hashimoto thyroiditis. Endocrine 2015, 50, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Rotondi, M.; Coperchini, F.; Magri, F.; Chiovato, L. Serum-negative autoimmune thyroiditis: What’s in a name? J. Endocrinol. Investig. 2014, 37, 589–591. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.-Y.; Lin, C.-L.; Hsu, W.-H.; Hsu, C.-Y.; Kao, C.-H. Risk of Urticaria in Children with Type 1 Diabetes Mellitus: A Nationwide Cohort Study. Int. J. Environ. Res. Public Health 2019, 17, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asero, R.; Orsatti, A.; Tedeschi, A.; Lorini, M. Autoimmune chronic urticaria associated with type 1 diabetes and Graves’ disease. J. Allergy Clin. Immunol. 2005, 115, 1088–1089. [Google Scholar] [CrossRef] [PubMed]
- Hyman, S.J.; Shreffler, W.G.; Rapaport, R. Type 1 diabetes, autoimmune thyroid disease, and chronic urticaria. Pediatr. Diabetes 2008, 9, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Jesenak, M.; Ciljakova, M.; Janickova, M.; Banovcin, P. Omalizumab in an 8-Year-Old Boy With Diabetes Mellitus and Refractory Chronic Spontaneous Urticaria. J. Investig. Allergol. Clin. Immunol. 2019, 29, 144–146. [Google Scholar] [CrossRef]
- Del Barba, P.; Del Tedesco, F.; Frontino, G.; Guarneri, M.P.; Bonfanti, R.; Barera, G. Case Report: Safety and Efficacy of Omalizumab in a 13-Year-Old Patient With Chronic Spontaneous Urticaria and Type 1 Diabetes. Front. Immunol. 2022, 13, 853561. [Google Scholar] [CrossRef]
- Hamada, S.; Kuroe, A.; Tsukino, M. Does omalizumab impair glucose homeostasis in a patient with severe persistent asthma and type 2 diabetes mellitus? Rev. Port. Pneumol. 2017, 23, 303–304. [Google Scholar] [CrossRef]
- Falay Gur, T.; Savas Erdogan, S.; Erdemir, V.A.; Dogan, B. Effect of omalizumab use on glucose homeostasis in non-diabetic patients with chronic urticaria. Cutan. Ocul. Toxicol. 2020, 39, 348–353. [Google Scholar] [CrossRef]
- Yalcin, A.D.; Gorczynski, R.M.; Cilli, A.; Strauss, L. Omalizumab (Anti-IgE) Therapy Increases Blood Glucose Levels in Severe Persistent Allergic Asthma Patients with Diabetes Mellitus: 18 Month follow-up. Clin. Lab. 2014, 60, 1561–1564. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Lindelöf, B.; Rashtak, S.; Rubio-Tapia, A.; Murray, J.A. Does urticaria risk increase in patients with celiac disease? A large population-based cohort study. Eur. J. Dermatol. 2013, 23, 681–687. [Google Scholar] [CrossRef]
- Haussmann, J.; Sekar, A. Chronic Urticaria: A Cutaneous Manifestation of Celiac Disease. Can. J. Gastroenterol. 2006, 20, 291–293. [Google Scholar] [CrossRef]
- Peroni, D.G.; Paiola, G.; Tenero, L.; Fornaro, M.; Bodini, A.; Pollini, F.; Piacentini, G.L. Chronic Urticaria and Celiac Disease: A Case Report. Pediatr. Dermatol. 2010, 27, 108–109. [Google Scholar] [CrossRef]
- Mendez Sanchez, A.; Pascual Perez, A.I.; Vazquez Pinera, M.A.; Fernandez Gonzalez, P. Cold urticaria and coeliac disease in a paediatric patient. An. Pediatr. 2019, 91, 410–411. [Google Scholar] [CrossRef]
- Candelli, M.; Nista, E.C.; Gabrielli, M.; Santarelli, L.; Pignataro, G.; Cammarota, G.; Gasbarrini, G.; Gasbarrini, A. CASE REPORT: Celiac Disease and Chronic Urticaria Resolution: A Case Report. Dig. Dis. Sci. 2004, 49, 1489–1490. [Google Scholar] [CrossRef]
- Scala, E.; Giani, M.; Pirrotta, L.; Guerra, E.; De Pità, O.; Puddu, P. Urticaria and adult celiac disease. Allergy 1999, 54, 1008–1009. [Google Scholar] [CrossRef]
- Levine, A.; Dalal, I.; Bujanover, Y. Celiac Disease Associated with Familial Chronic Urticaria and Thyroid Autoimmunity in a Child. Pediatrics 1999, 104, e25. [Google Scholar] [CrossRef] [Green Version]
- Mennini, M.; Fiocchi, A.; Trovato, C.M.; Ferrari, F.; Iorfida, D.; Cucchiara, S.; Montuori, M. Anaphylaxis after wheat ingestion in a patient with coeliac disease: Two kinds of reactions and the same culprit food. Eur. J. Gastroenterol. Hepatol. 2019, 31, 893–895. [Google Scholar] [CrossRef]
- Meneghetti, R.; Gerarduzzi, T.; Barbi, E.; Ventura, A. Chronic urticaria and coeliac disease. Arch. Dis. Child. 2004, 89, 293. [Google Scholar] [CrossRef] [Green Version]
- Caminiti, L.; Passalacqua, G.; Magazzu, G.; Comisi, F.; Vita, D.; Barberio, G.; Sferlazzas, C.; Pajno, G.B. Chronic urticaria and associated coeliac disease in children: A case-control study. Pediatr. Allergy Immunol. 2005, 16, 428–432. [Google Scholar] [CrossRef]
- Wong, T.; Ko, H.H.; Chan, E.S. IgE-Mediated allergy to wheat in a child with celiac disease—A case report. Allergy Asthma Clin. Immunol. 2014, 10, 56. [Google Scholar] [CrossRef] [Green Version]
- Lang, C.; Kaya, G. A Case of Adrenergic Urticaria Associated with Vitiligo. Dermatopathology 2016, 3, 83–86. [Google Scholar] [CrossRef]
- Kolkhir, P.; Pogorelov, D.; Kochergin, N. Chronic spontaneous urticaria associated with vitiligo and thyroiditis (autoimmune polyglandular syndrome IIIC): Case series. Int. J. Dermatol. 2017, 56, e89–e90. [Google Scholar] [CrossRef]
- Kasznicki, J.; Drzewoski, J. A case of autoimmune urticaria accompanying autoimmune polyglandular syndrome type III associated with Hashimoto’s disease, type 1 diabetes mellitus, and vitiligo. Endokrynol. Pol. 2014, 65, 320–323. [Google Scholar] [CrossRef] [Green Version]
- Magen, E.; Waitman, D.-A.; Dickstein, Y.; Davidovich, V.; Kahan, N.R. Clinical-laboratory characteristics of ANA-positive chronic idiopathic urticaria. Allergy Asthma Proc. 2015, 36, 138–144. [Google Scholar] [CrossRef]
- Mete, N.; Gulbahar, O.; Aydin, A.; Sin, A.Z.; Kokuludag, A.; Sebik, F. Low B12 levels in chronic idiopathic urticaria. J. Investig. Allergol. Clin. Immunol. 2004, 14, 292–299. [Google Scholar]
- Leznoff, A.; Sussman, G. Syndrome of idiopathic chronic urticaria and angioedema with thyroid autoimmunity: A study of 90 patients. J. Allergy Clin. Immunol. 1989, 84, 66–71. [Google Scholar] [CrossRef]
- Ghazanfar, M.N.; Kibsgaard, L.; Thomsen, S.F.; Vestergaard, C. Risk of comorbidities in patients diagnosed with chronic urticaria: A nationwide registry-study. World Allergy Organ. J. 2020, 13, 100097. [Google Scholar] [CrossRef] [Green Version]
- Fraser, K.; Robertson, L. Chronic urticaria and autoimmunity. Ski. Ther. Lett. 2013, 18, 5–9. [Google Scholar]
- Çildağ, S.; Sargın, G.; Şentürk, T. Clinical and laboratory characteristics of chronic spontaneous urticaria with connective tissue diseases: A cross-sectional study. Arch. Rheumatol. 2022, 37, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Yong, S.-B.; Su, K.-W.; Chen, H.-H.; Huang, J.-Y.; Wu, H.-J.; Wei, J.C.-C. Impact of chronic urticaria on systemic lupus erythematosus: A nationwide population-based study in Taiwan. J. Dermatol. 2019, 46, 26–32. [Google Scholar] [CrossRef]
- Chiu, H.-Y.; Muo, C.-H.; Sung, F.-C. Associations of chronic urticaria with atopic and autoimmune comorbidities: A nationwide population-based study. Int. J. Dermatol. 2018, 57, 822–829. [Google Scholar] [CrossRef]
- Kolkhir, P.; Pogorelov, D.; Olisova, O.; Maurer, M. Comorbidity and pathogenic links of chronic spontaneous urticaria and systemic lupus erythematosus—A systematic review. Clin. Exp. Allergy 2016, 46, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Ferriani, M.; Silva, M.F.C.; Pereira, R.M.R.; Terreri, M.T.; Magalhães, C.S.; Bonfá, E.; Pastorino, A.; Dos Santos, M.C.; Appenzeller, S.; Ferriani, V.P.L.; et al. Chronic Spontaneous Urticaria: A Survey of 852 Cases of Childhood-Onset Systemic Lupus Erythematosus. Int. Arch. Allergy Immunol. 2015, 167, 186–192. [Google Scholar] [CrossRef]
- Magen, E.; Chikovani, T.; Waitman, D.-A.; Kahan, N.R. Association of alopecia areata with atopic dermatitis and chronic spontaneous urticaria. Allergy Asthma Proc. 2018, 39, 96–102. [Google Scholar] [CrossRef]
- De Marchi, S.U.; Cecchin, E.; De Marchi, S. Autoimmune spontaneous chronic urticaria and generalized myasthenia gravis in a patient with polyglandular autoimmune syndrome type 3. Muscle Nerve 2015, 52, 440–444. [Google Scholar] [CrossRef]
- Rymarczyk, B.; Gluck, J.; Rogala, B.; Brzoza, Z. Chronic urticaria in myasthenia gravis patients—More than occasional coexistence? Allergol. Immunopathol. 2014, 42, 626–627. [Google Scholar] [CrossRef]
- Bonnekoh, H.; Krause, K.; Kolkhir, P. Chronic recurrent wheals—If not chronic spontaneous urticaria, what else? Allergol. Sel. 2023, 7, 8–16. [Google Scholar] [CrossRef]
- Bonnekoh, H.; Butze, M.; Kallinich, T.; Kambe, N.; Kokolakis, G.; Krause, K. Spectrum of Genetic Autoinflammatory Diseases Presenting with Cutaneous Symptoms. Acta Derm.-Venereol. 2020, 100, adv00091. [Google Scholar] [CrossRef]
- Krause, K.; Grattan, C.E.; Bindslev-Jensen, C.; Gattorno, M.; Kallinich, T.; Koning, H.D.; Lachmann, H.J.; Lipsker, D.; Navarini, A.A.; Simon, A.; et al. How not to miss autoinflammatory diseases masquerading as urticaria. Allergy 2012, 67, 1465–1474. [Google Scholar] [CrossRef]
- Matos, A.L.; Figueiredo, C.; Gonçalo, M. Differential Diagnosis of Urticarial Lesions. Front. Allergy 2022, 3, 808543. [Google Scholar] [CrossRef]
- Nham, T.; Saleh, C.; Chu, D.; Vakaljan, S.L.; Ohayon, J.A.; Siegal, D.M. Refractory urticaria and the importance of diagnosing Schnitzler’s syndrome. BMJ Case Rep. 2019, 12, e228546. [Google Scholar] [CrossRef]
- Bonnekoh, H.; Scheffel, J.; Maurer, M.; Krause, K. Use of skin biomarker profiles to distinguish Schnitzler syndrome from chronic spontaneous urticaria: Results of a pilot study. Br. J. Dermatol. 2018, 178, 561–562. [Google Scholar] [CrossRef]
- Davis, M.D.P.; van der Hilst, J.C.H. Mimickers of Urticaria: Urticarial Vasculitis and Autoinflammatory Diseases. J. Allergy Clin. Immunol. 2018, 6, 1162–1170. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murdaca, G.; Paladin, F.; Borro, M.; Ricciardi, L.; Gangemi, S. Prevalence of Autoimmune and Autoinflammatory Diseases in Chronic Urticaria: Pathogenetic, Diagnostic and Therapeutic Implications. Biomedicines 2023, 11, 410. https://doi.org/10.3390/biomedicines11020410
Murdaca G, Paladin F, Borro M, Ricciardi L, Gangemi S. Prevalence of Autoimmune and Autoinflammatory Diseases in Chronic Urticaria: Pathogenetic, Diagnostic and Therapeutic Implications. Biomedicines. 2023; 11(2):410. https://doi.org/10.3390/biomedicines11020410
Chicago/Turabian StyleMurdaca, Giuseppe, Francesca Paladin, Matteo Borro, Luisa Ricciardi, and Sebastiano Gangemi. 2023. "Prevalence of Autoimmune and Autoinflammatory Diseases in Chronic Urticaria: Pathogenetic, Diagnostic and Therapeutic Implications" Biomedicines 11, no. 2: 410. https://doi.org/10.3390/biomedicines11020410