
Cardiac Resynchronization Therapy and Hypertrophic Cardiomyopathy: A Comprehensive Review


 , , , ,
, , , ,
Abstract
:1. Background
2. HCM in a Nutshell
3. Clinical and Imaging Approach in HCM
4. Current Advances in CRT
5. Distinguishing Patients with HCM Who Might Benefit from CRT
5.1. Electrical Parameters in Stratifying Patients with HCM for CRT
5.2. Imaging Parameters in Stratifying Patients with HCM for CRT
6. Current Prospects of CRT in Patients with HCM
7. Future Perspectives
8. Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maron:, B.J.; Desai, M.Y.; Nishimura, R.A.; Spirito, P.; Rakowski, H.; Towbin, J.A.; Rowin, E.J.; Maron, M.S.; Sherrid, M.V. Diagnosis and Evaluation of Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2022, 79, 372–389. [Google Scholar] [CrossRef] [PubMed]
- Muresan, I.D.; Agoston-Coldea, L. Phenotypes of hypertrophic cardiomyopathy: Genetics, clinics, and modular imaging. Heart Fail. Rev. 2021, 26, 1023–1036. [Google Scholar] [CrossRef] [PubMed]
- Marstrand, P.; Han, L.; Day, S.M.; Olivotto, I.; Ashley, E.A.; Michels, M.; Pereira, A.C.; Wittekind, S.G.; Helms, A.; Saberi, S.; et al. Hypertrophic Cardiomyopathy with Left Ventricular Systolic Dysfunction. Circulation 2020, 141, 1371–1383. [Google Scholar] [CrossRef]
- Keene, D.; I Whinnett, Z. Advances in cardiac resynchronisation therapy: Review of indications and delivery options. Heart 2022, 108, 889–897. [Google Scholar] [CrossRef]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Cheng, X.; Chen, J.; Zhou, M.; Qian, T.; Zhang, Z.; Yin, J.; Zhang, H.; Dai, G.; Qin, Y.; et al. Left Bundle Pacing for Left Bundle Branch Block and Intermittent Third-Degree Atrioventricular Block in a MYH7 Mutation-Related Hypertrophic Cardiomyopathy with Restrictive Phenotype in a Child. Front. Pediatr. 2020, 8, 312. [Google Scholar] [CrossRef]
- Zheng, R.; Dong, Y.; Wu, S.; Su, L.; Zhao, D.; Chen, X.; Cai, B.; Fang, X.; Vijayaraman, P.; Huang, W. Conduction system pacing following septal myectomy: Insights into site of conduction block. J. Cardiovasc. Electrophysiol. 2022, 33, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Cui, H.; Schaff, H.V.; Nishimura, R.A.; Geske, J.B.; Dearani, J.A.; Lahr, B.D.; Ommen, S.R. Conduction Abnormalities and Long-Term Mortality Following Septal Myectomy in Patients with Obstructive Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2019, 74, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Salden, O.A.; Vernooy, K.; van Stipdonk, A.M.; Cramer, M.J.; Prinzen, F.W.; Meine, M. Strategies to Improve Selection of Patients without Typical Left Bundle Branch Block for Cardiac Resynchronization Therapy. JACC Clin. Electrophysiol. 2020, 6, 129–142. [Google Scholar] [CrossRef]
- Stankovic, I.; Prinz, C.; Ciarka, A.; Daraban, A.M.; Kotrc, M.; Aarones, M.; Szulik, M.; Winter, S.; Belmans, A.; Neskovic, A.N.; et al. Relationship of visually assessed apical rocking and septal flash to response and long-term survival following cardiac resynchronization therapy (PREDICT-CRT). Eur. Heart J. Cardiovasc. Imaging 2016, 17, 262–269. [Google Scholar] [CrossRef]
- Valzania, C.; Gadler, F.; Boriani, G.; Rapezzi, C.; Eriksson, M.J. Cardiac implantable electrical devices in patients with hypertrophic cardiomyopathy: Single center implant data extracted from the Swedish pacemaker and ICD registry. Scand. Cardiovasc. J. 2020, 54, 239–247. [Google Scholar] [CrossRef]
- Kappenberger, L.; Linde, C.; Daubert, C.; McKenna, W.; Meisel, E.; Sadoul, N.; Chojnowska, L.; Guize, L.; Gras, D.; Jeanrenaud, X.; et al. Pacing in hypertrophic obstructive cardiomyopathy: A randomized crossover study. Eur. Heart J. 1997, 18, 1249–1256. [Google Scholar] [CrossRef]
- Leung, C.; Fifer, M.; Singh, J.; Parks, K. Cardiac Resynchronization Therapy in a Patient with Hypertrophic Cardiomyopathy and Symptomatic Heart Failure with Preserved Ejection Fraction. J. Card. Fail. 2017, 23, S71. [Google Scholar] [CrossRef]
- Arregle, F.; Hourdain, J.; Habib, G.; Lavagna, F.; Peres, N.; Torras, O.; Koutbi, L.; Dognin, N.; Maille, B.; Franceschi, F.; et al. Contribution of cardiac resynchronization therapy in hypertrophic cardiomyopathy with systolic dysfunction: A case-control study. Arch. Cardiovasc. Dis. Suppl. 2020, 12, 116. [Google Scholar] [CrossRef]
- Marian, A.J.; Braunwald, E. Hypertrophic Cardiomyopathy. Circ. Res. 2017, 121, 749–770. [Google Scholar] [CrossRef] [PubMed]
- Konno, T.; Chang, S.; Seidman, J.G.; Seidman, C.E. Genetics of hypertrophic cardiomyopathy. Curr. Opin. Cardiol. 2010, 25, 205–209. [Google Scholar] [CrossRef]
- Chen, S.N.; Czernuszewicz, G.; Tan, Y.; Lombardi, R.; Jin, J.; Willerson, J.T.; Marian, A.J. Human Molecular Genetic and Functional Studies Identify TRIM63, Encoding Muscle RING Finger Protein 1, as a Novel Gene for Human Hypertrophic Cardiomyopathy. Circ. Res. 2012, 111, 907–919. [Google Scholar] [CrossRef]
- Helms, A.S.; Alvarado, F.J.; Yob, J.; Tang, V.T.; Pagani, F.; Russell, M.W.; Valdivia, H.H.; Day, S.M. Genotype-Dependent and -Independent Calcium Signaling Dysregulation in Human Hypertrophic Cardiomyopathy. Circulation 2016, 134, 1738–1748. [Google Scholar] [CrossRef]
- Ruggiero, A.; Chen, S.N.; Lombardi, R.; Rodriguez, G.; Marian, A.J. Pathogenesis of hypertrophic cardiomyopathy caused by myozenin 2 mutations is independent of calcineurin activity. Cardiovasc. Res. 2013, 97, 44–54. [Google Scholar] [CrossRef]
- Fatkin, D.; McConnell, B.K.; Mudd, J.O.; Semsarian, C.; Moskowitz, I.G.; Schoen, F.J.; Giewat, M.; Seidman, C.E.; Seidman, J. An abnormal Ca2+ response in mutant sarcomere protein–mediated familial hypertrophic cardiomyopathy. J. Clin. Investig. 2000, 106, 1351–1359. [Google Scholar] [CrossRef] [PubMed]
- Teekakirikul, P.; Eminaga, S.; Toka, O.; Alcalai, R.; Wang, L.; Wakimoto, H.; Nayor, M.; Konno, T.; Gorham, J.M.; Wolf, C.M.; et al. Cardiac fibrosis in mice with hypertrophic cardiomyopathy is mediated by non-myocyte proliferation and requires Tgf-β. J. Clin. Investig. 2010, 120, 3520–3529. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Li, Y.; He, F.; Wu, H. Microarray profiling of long non-coding RNA (lncRNA) associated with hypertrophic cardiomyopathy. BMC Cardiovasc. Disord. 2015, 15, 62. [Google Scholar] [CrossRef] [PubMed]
- Velicki, L.; Jakovljevic, D.G.; Preveden, A.; Golubovic, M.; Bjelobrk, M.; Ilic, A.; Stojsic, S.; Barlocco, F.; Tafelmeier, M.; Okwose, N.; et al. Genetic determinants of clinical phenotype in hypertrophic cardiomyopathy. BMC Cardiovasc. Disord. 2020, 20, 516. [Google Scholar] [CrossRef]
- Woo, A.; Jedrzkiewicz, S. The Mitral Valve in Hypertrophic Cardiomyopathy. Circulation 2011, 124, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Desai, M.Y.; Nishimura, R.A.; Spirito, P.; Rakowski, H.; Towbin, J.A.; Dearani, J.A.; Rowin, E.J.; Maron, M.S.; Sherrid, M.V. Management of Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2022, 79, 390–414. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.; Dong, S.-Y.; Ren, M.-S.; Wang, R. Ventricular arrhythmia and sudden cardiac death in hypertrophic cardiomyopathy: From bench to bedside. Front. Cardiovasc. Med. 2022, 9, 949294. [Google Scholar] [CrossRef]
- Amano, Y.; Kitamura, M.; Takano, H.; Yanagisawa, F.; Tachi, M.; Suzuki, Y.; Kumita, S.; Takayama, M. Cardiac MR Imaging of Hypertrophic Cardiomyopathy: Techniques, Findings, and Clinical Relevance. Magn. Reson. Med Sci. 2018, 17, 120–131. [Google Scholar] [CrossRef]
- Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; Mahrholdt, H.; et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar] [CrossRef]
- Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; Kantor, P.; et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients with Hypertrophic Cardiomyopathy. Circulation 2020, 142, e558–e631. [Google Scholar] [CrossRef]
- Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; Kantor, P.; et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy. J. Thorac. Cardiovasc. Surg. 2021, 162, e23–e106. [Google Scholar] [CrossRef]
- Mandeş, L.; Roşca, M.; Ciupercă, D.; Popescu, B.A. The role of echocardiography for diagnosis and prognostic stratification in hypertrophic cardiomyopathy. J. Echocardiogr. 2020, 18, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Cazeau, S.; Leclercq, C.; Lavergne, T.; Walker, S.; Varma, C.; Linde, C.; Garrigue, S.; Kappenberger, L.; Haywood, G.A.; Santini, M.; et al. Effects of Multisite Biventricular Pacing in Patients with Heart Failure and Intraventricular Conduction Delay. N. Engl. J. Med. 2001, 344, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Fisher, W.G.; Smith, A.L.; Delurgio, D.B.; Leon, A.R.; Loh, E.; Kocovic, D.Z.; Packer, M.; Clavell, A.L.; Hayes, D.L.; et al. Cardiac Resynchronization in Chronic Heart Failure. N. Engl. J. Med. 2002, 346, 1845–1853. [Google Scholar] [CrossRef] [PubMed]
- Leclercq, C. Comparative effects of permanent biventricular and right-univentricular pacing in heart failure patients with chronic atrial fibrillation. Eur. Heart J. 2002, 23, 1780–1787. [Google Scholar] [CrossRef] [PubMed]
- Auricchio, A.; Stellbrink, C.; Sack, S.; Block, M.; Vogt, J.; Bakker, P.; Huth, C.; Schöndube, F.; Wolfhard, U.; Böcker, D.; et al. long-term clinical effect of hemodynamically optimized cardiac resynchronization therapy in patients with heart failure and ventricular conduction delay. J. Am. Coll. Cardiol. 2002, 39, 2026–2033. [Google Scholar] [CrossRef] [PubMed]
- Young, J.B. Combined Cardiac Resynchronization and Implantable Cardioversion Defibrillation in Advanced Chronic Heart Failure. JAMA 2003, 289, 2685–2694. [Google Scholar] [CrossRef] [PubMed]
- Higgins, S.L.; Hummel, J.D.; Niazi, I.K.; Giudici, M.C.; Worley, S.J.; Saxon, L.A.; Boehmer, J.P.; Higginbotham, M.B.; De Marco, T.; Foster, E.; et al. Cardiac resynchronization therapy for the treatment of heart failure in patients with intraventricular conduction delay and malignant ventricular tachyarrhythmias. J. Am. Coll. Cardiol. 2003, 42, 1454–1459. [Google Scholar] [CrossRef] [PubMed]
- Auricchio, A.; Stellbrink, C.; Butter, C.; Sack, S.; Vogt, J.; Misier, A.R.; Böcker, D.; Block, M.; Kirkels, J.H.; Kramer, A.; et al. Clinical efficacy of cardiac resynchronization therapy using left ventricular pacing in heart failure patients stratified by severity of ventricular conduction delay. J. Am. Coll. Cardiol. 2003, 42, 2109–2116. [Google Scholar] [CrossRef]
- Bristow, M.R.; Saxon, L.A.; Boehmer, J.; Krueger, S.; Kass, D.A.; De Marco, T.; Carson, P.; DiCarlo, L.; DeMets, D.; White, B.G.; et al. Cardiac-Resynchronization Therapy with or without an Implantable Defibrillator in Advanced Chronic Heart Failure. N. Engl. J. Med. 2004, 350, 2140–2150. [Google Scholar] [CrossRef]
- Cleland, J.G.; Daubert, J.-C.; Erdmann, E.; Freemantle, N.; Gras, D.; Kappenberger, L.; Tavazzi, L. The Effect of Cardiac Resynchronization on Morbidity and Mortality in Heart Failure. N. Engl. J. Med. 2005, 352, 1539–1549. [Google Scholar] [CrossRef]
- Linde, C.; Abraham, W.T.; Gold, M.R.; Sutton, M.S.J.; Ghio, S.; Daubert, C. Randomized Trial of Cardiac Resynchronization in Mildly Symptomatic Heart Failure Patients and in Asymptomatic Patients with Left Ventricular Dysfunction and Previous Heart Failure Symptoms. J. Am. Coll. Cardiol. 2008, 52, 1834–1843. [Google Scholar] [CrossRef] [PubMed]
- Moss, A.J.; Hall, W.J.; Cannom, D.S.; Klein, H.; Brown, M.W.; Daubert, J.P.; Estes, N.A.M., III; Foster, E.; Greenberg, H.; Higgins, S.L.; et al. Cardiac-Resynchronization Therapy for the Prevention of Heart-Failure Events. N. Engl. J. Med. 2009, 361, 1329–1338. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.S.; Wells, G.A.; Talajic, M.; Arnold, M.O.; Sheldon, R.; Connolly, S.; Hohnloser, S.H.; Nichol, G.; Birnie, D.H.; Sapp, J.L.; et al. Cardiac-Resynchronization Therapy for Mild-to-Moderate Heart Failure. N. Engl. J. Med. 2010, 363, 2385–2395. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Young, J.B.; León, A.R.; Adler, S.; Bank, A.J.; Hall, S.A.; Lieberman, R.; Liem, L.B.; O’Connell, J.B.; Schroeder, J.S.; et al. Effects of Cardiac Resynchronization on Disease Progression in Patients with Left Ventricular Systolic Dysfunction, an Indication for an Implantable Cardioverter-Defibrillator, and Mildly Symptomatic Chronic Heart Failure. Circulation 2004, 110, 2864–2868. [Google Scholar] [CrossRef]
- Ruschitzka, F.; Abraham, W.T.; Singh, J.P.; Bax, J.J.; Borer, J.S.; Brugada, J.; Dickstein, K.; Ford, I.; Gorcsan, J., III; Gras, D. Cardiac-resynchronization therapy in heart failure with a narrow QRS complex. N. Engl. J. Med. 2013, 369, 1395–1405. [Google Scholar] [CrossRef]
- Beshai, J.F.; Grimm, R.A.; Nagueh, S.F.; Baker, J.H.; Beau, S.L.; Greenberg, S.M.; Pires, L.A.; Tchou, P.J. Cardiac-Resynchronization Therapy in Heart Failure with Narrow QRS Complexes. N. Engl. J. Med. 2007, 357, 2461–2471. [Google Scholar] [CrossRef]
- Kusumoto, F.M.; Schoenfeld, M.H.; Barrett, C.; Edgerton, J.R.; Ellenbogen, K.A.; Gold, M.R.; Goldschlager, N.F.; Hamilton, R.M.; Joglar, J.A.; Kim, R.J.; et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients with Bradycardia and Cardiac Conduction Delay: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. Circulation 2019, 140, e333–e381. [Google Scholar] [CrossRef]
- Mele, D.; Trevisan, F.; Fiorencis, A.; Smarrazzo, V.; Bertini, M.; Ferrari, R. Current Role of Echocardiography in Cardiac Resynchronization Therapy: From Cardiac Mechanics to Flow Dynamics Analysis. Curr. Heart Fail. Rep. 2020, 17, 384–396. [Google Scholar] [CrossRef]
- Moskovitch, J.; Voskoboinik, A. Cardiac resynchronization therapy: A comprehensive review. Minerva Med. 2019, 110, 121–138. [Google Scholar] [CrossRef]
- Ploux, S.; Eschalier, R.; Whinnett, Z.I.; Lumens, J.; Derval, N.; Sacher, F.; Hocini, M.; Jaïs, P.; Dubois, R.; Ritter, P.; et al. Electrical dyssynchrony induced by biventricular pacing: Implications for patient selection and therapy improvement. Heart Rhythm. 2015, 12, 782–791. [Google Scholar] [CrossRef]
- Thibault, B.; Harel, F.; Ducharme, A.; White, M.; Ellenbogen, K.A.; Frasure-Smith, N.; Roy, D.; Philippon, F.; Dorian, P.; Talajic, M.; et al. Cardiac Resynchronization Therapy in Patients with Heart Failure and a QRS Complex <120 Milliseconds. Circulation 2013, 127, 873–881. [Google Scholar] [CrossRef]
- van Stipdonk, A.; Vanbelle, S.; ter Horst, I.; Luermans, J.; Meine, M.; Maass, A.; Auricchio, A.; Prinzen, F.; Vernooy, K. Large variability in clinical judgement and definitions of left bundle branch block to identify candidates for cardiac resynchronisation therapy. Int. J. Cardiol. 2019, 286, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.G.; Abraham, W.T.; Linde, C.; Gold, M.R.; Young, J.B.; Daubert, J.C.; Sherfesee, L.; Wells, G.A.; Tang, A.S. An individual patient meta-analysis of five randomized trials assessing the effects of cardiac resynchronization therapy on morbidity and mortality in patients with symptomatic heart failure. Eur. Heart J. 2013, 34, 3547–3556. [Google Scholar] [CrossRef] [PubMed]
- Eschalier, R.; Ploux, S.; Ritter, P.; Haïssaguerre, M.; Ellenbogen, K.A.; Bordachar, P. Nonspecific intraventricular conduction delay: Definitions, prognosis, and implications for cardiac resynchronization therapy. Heart Rhythm. 2015, 12, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- Kawata, H.; Bao, H.; Curtis, J.P.; Minges, K.E.; Mitiku, T.; Birgersdotter-Green, U.; Feld, G.K.; Hsu, J.C. Cardiac Resynchronization Defibrillator Therapy for Nonspecific Intraventricular Conduction Delay versus Right Bundle Branch Block. J. Am. Coll. Cardiol. 2019, 73, 3082–3099. [Google Scholar] [CrossRef]
- Qin, J.X.; Shiota, T.; Lever, H.M.; Asher, C.R.; Popović, Z.B.; Greenberg, N.L.; Agler, D.A.; Drinko, J.K.; Smedira, N.G.; Tuzcu, E.; et al. Conduction system abnormalities in patients with obstructive hypertrophic cardiomyopathy following septal reduction interventions. Am. J. Cardiol. 2004, 93, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Gionfriddo, W.; Burrows, A.; Narayanan, C.; Shrestha, S.; Rastegar, H.; Garlitski, A.; Weinstock, J.; Homoud, M.; Rowin, E.J.; Maron, M.S.; et al. Abstract 12214: Characterization of Iatrogenic Left Bundle Branch Block After Septal Myectomy for Hypertrophic Cardiomyopathy. Circulation 2021, 144, A12214. [Google Scholar] [CrossRef]
- Spartalis, M.; Tzatzaki, E.; Spartalis, E.; Damaskos, C.; Athanasiou, A.; Livanis, E.; Voudris, V. The Role of Echocardiography in the Optimization of Cardiac Resynchronization Therapy: Current Evidence and Future Perspectives. Open Cardiovasc. Med. J. 2017, 11, 133–145. [Google Scholar] [CrossRef]
- Ghani, A.; Delnoy, P.P.H.; Ottervanger, J.P.; Misier, A.R.R.; Smit, J.J.J.; Adiyaman, A.; Elvan, A. Apical rocking is predictive of response to cardiac resynchronization therapy. Int. J. Cardiovasc. Imaging 2015, 31, 717–725. [Google Scholar] [CrossRef]
- Kappenberger, L. Clinical progress after randomized on/off pacemaker treatment for hypertrophic obstructive cardiomyopathy. Europace 1999, 1, 77–84. [Google Scholar] [CrossRef]
- Galve, E.; Sambola, A.; Saldaña, G.; Quispe, I.; Nieto, E.; Diaz, A.; Evangelista, A.; Candell-Riera, J. Late benefits of dual-chamber pacing in obstructive hypertrophic cardiomyopathy: A 10-year follow-up study. Heart 2010, 96, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Lucon, A.; Palud, L.; Pavin, D.; Donal, E.; Behar, N.; Leclercq, C.; Mabo, P.; Daubert, J.-C. Very late effects of dual chamber pacing therapy for obstructive hypertrophic cardiomyopathy. Arch. Cardiovasc. Dis. 2013, 106, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.A.; Trusty, J.M.; Hayes, D.L.; Ilstrup, D.M.; Larson, D.R.; Hayes, S.N.; Allison, T.G.; Tajik, A. Dual-Chamber Pacing for Hypertrophic Cardiomyopathy: A Randomized, Double-Blind, Crossover Trial. J. Am. Coll. Cardiol. 1997, 29, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Nishimura, R.A.; McKenna, W.J.; Rakowski, H.; Josephson, M.E.; Kieval, R.S. Assessment of Permanent Dual-Chamber Pacing as a Treatment for Drug-Refractory Symptomatic Patients with Obstructive Hypertrophic Cardiomyopathy. Circulation 1999, 99, 2927–2933. [Google Scholar] [CrossRef] [PubMed]
- Olivotto, I.; Cecchi, F.; Poggesi, C.; Yacoub, M.H. Patterns of Disease Progression in Hypertrophic Cardiomyopathy. Circ. Heart Fail. 2012, 5, 535–546. [Google Scholar] [CrossRef]
- Victor, V.; Kumar, A.; Thakkar, S.; Patel, H.P.; Doshi, R.; Geske, J.; Deshmukh, A. Role of cardiac resynchronization therapy in hypertrophic cardiomyopathy: A meta-analysis. J. Am. Coll. Cardiol. 2021, 77, 275. [Google Scholar] [CrossRef]
- Gu, M.; Jin, H.; Hua, W.; Fan, X.-H.; Niu, H.-X.; Tian, T.; Ding, L.-G.; Wang, J.; Xue, C.; Zhang, S. Clinical outcome of cardiac resynchronization therapy in dilated-phase hypertrophic cardiomyopathy. J. Geriatr. Cardiol. 2017, 14, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Ikutaro Nakajima, T.N.K.M.Y.Y.H.O.K.S.T.A.W.S.N.A. and S.K. Effectiveness of Cardiac Resynchronization Therapy in Patients with End-Stage Phase of Hypertrophic Cardiomyopathy: Comparison with Idiopathic Dilated Cardio-myopathy. Circulation 2011, 124, A14996. [Google Scholar]
- Killu, A.M.; Park, J.-Y.; Sara, J.D.; Hodge, D.O.; Gersh, B.J.; Nishimura, R.A.; Asirvatham, S.J.; McLeod, C.J. Cardiac resynchronization therapy in patients with end-stage hypertrophic cardiomyopathy. EP Eur. 2018, 20, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Tower-Rader, A.; Kramer, C.M.; Neubauer, S.; Nagueh, S.F.; Desai, M.Y. Multimodality Imaging in Hypertrophic Cardiomyopathy for Risk Stratification. Circ. Cardiovasc. Imaging 2020, 13, e009026. [Google Scholar] [CrossRef] [PubMed]
- Woo, A.; Williams, W.G.; Choi, R.; Wigle, E.D.; Rozenblyum, E.; Fedwick, K.; Siu, S.; Ralph-Edwards, A.; Rakowski, H. Clinical and Echocardiographic Determinants of Long-Term Survival after Surgical Myectomy in Obstructive Hypertrophic Cardiomyopathy. Circulation 2005, 111, 2033–2041. [Google Scholar] [CrossRef] [PubMed]
- Ommen, S.R.; Maron, B.J.; Olivotto, I.; Maron, M.S.; Cecchi, F.; Betocchi, S.; Gersh, B.J.; Ackerman, M.J.; McCully, R.B.; Dearani, J.A.; et al. Long-Term Effects of Surgical Septal Myectomy on Survival in Patients with Obstructive Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2005, 46, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Cay, S.; Ozeke, O.; Ozcan, F.; Aras, D.; Topaloglu, S. A novel use of cardiac resynchronization therapy-defibrillator device in hypertrophic cardiomyopathy. Ann. Noninvasive Electrocardiol. 2019, 24, e12559. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
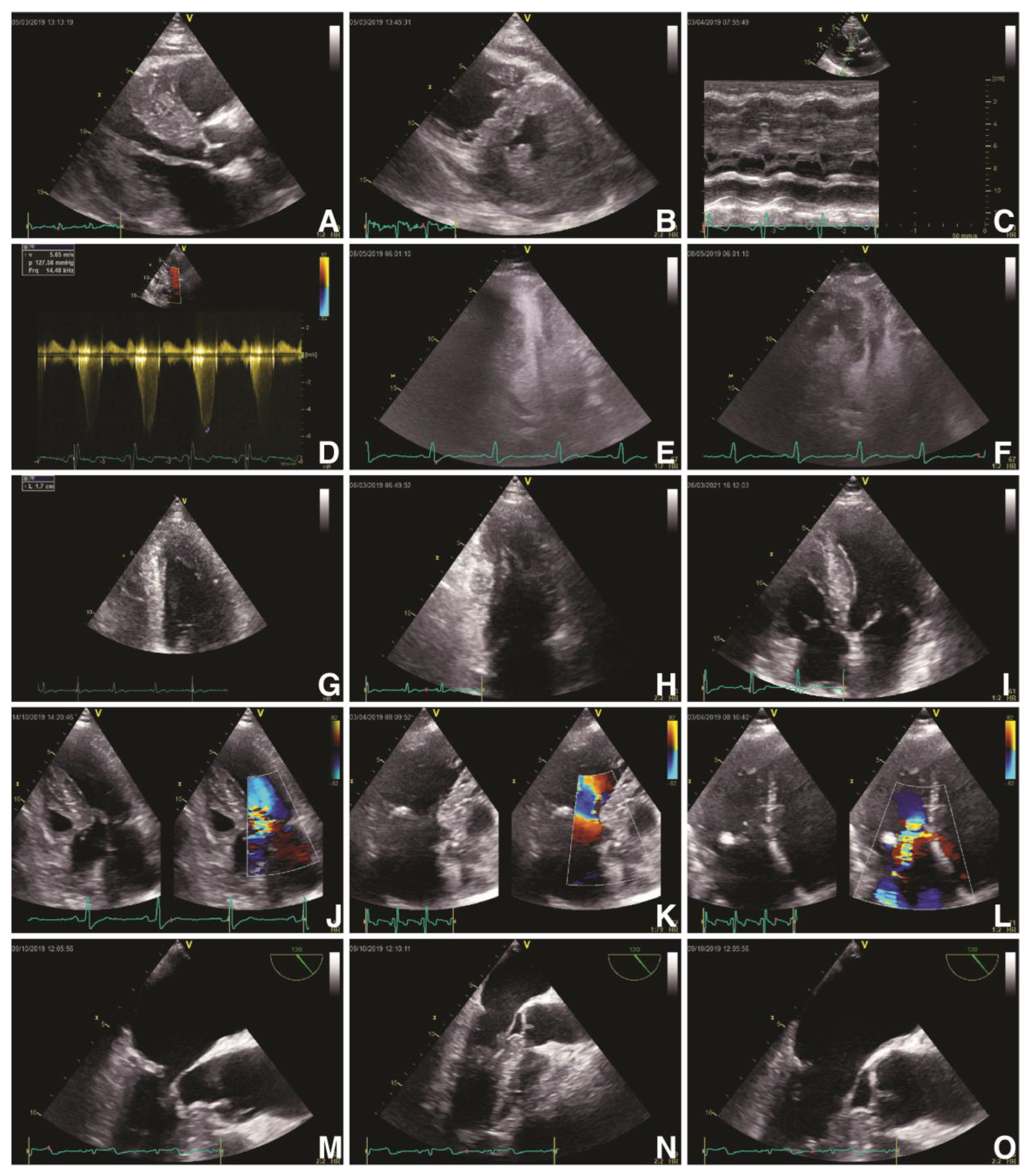
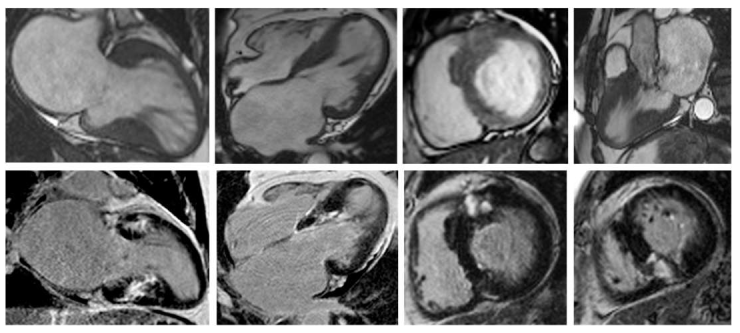
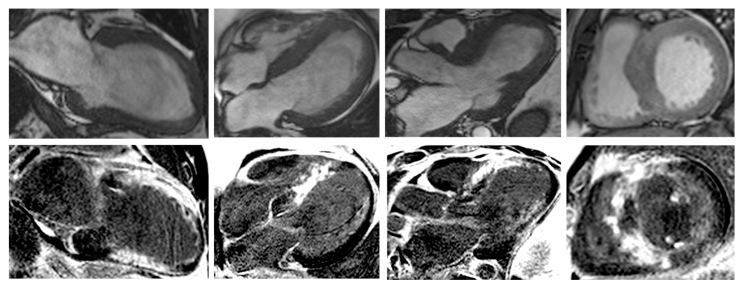
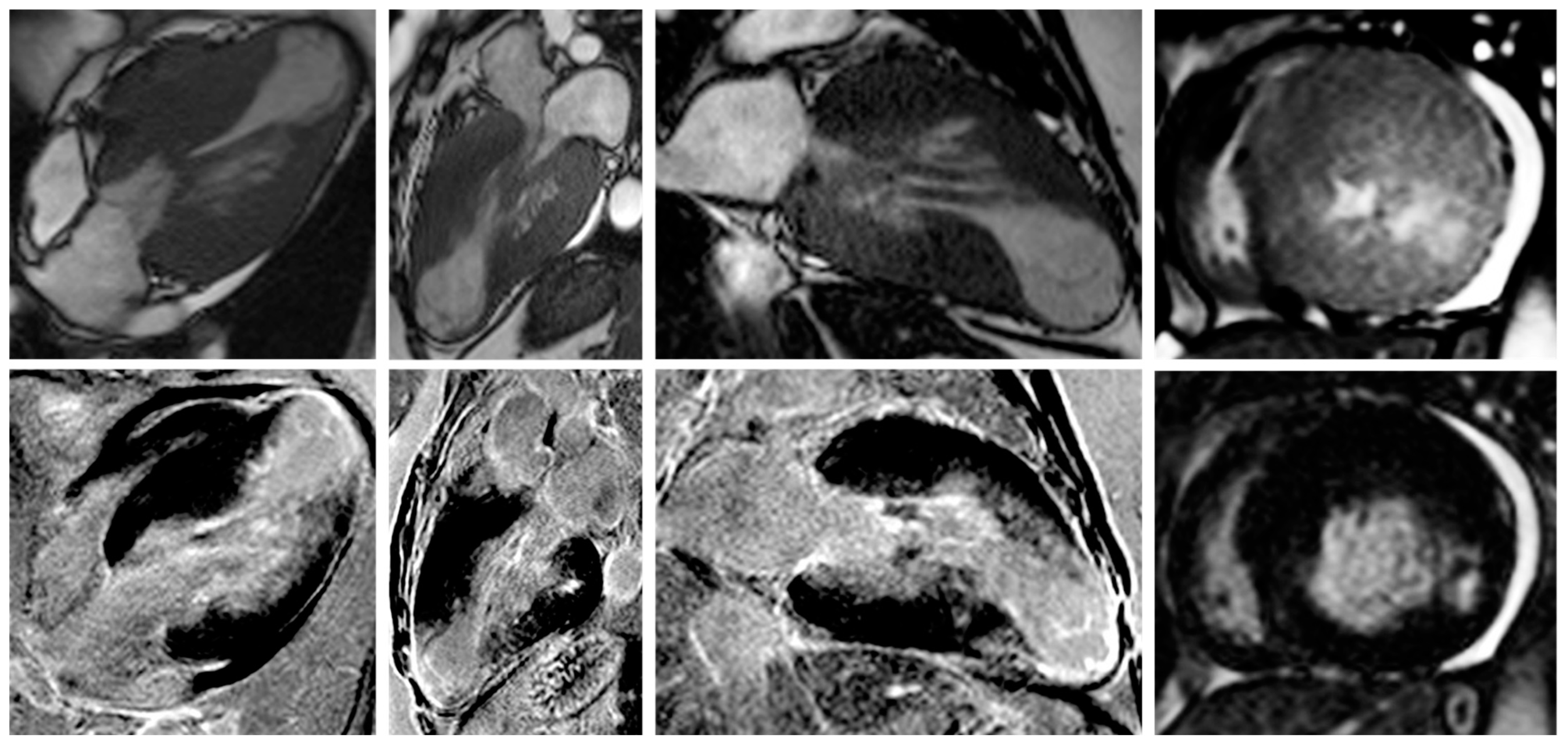
| IMAGING METHOD | FINDINGS | DETAILS |
|---|---|---|
| ECHOCARDIOGRAPHY | LV hypertrophy |
|
| LVOT dynamic obstruction |
| |
| SAM |
| |
| LV strain |
| |
| MV apparatus |
| |
| CMR | Cine SSFP CMR |
|
| LGE |
| |
| T2-weighted |
| |
| PC CMR |
| |
| T1-mapping |
|
| CLINICAL TRIAL | n | YEAR | NYHA CLASS | QRS (MS) | LVEF |
|---|---|---|---|---|---|
| MUSTIC-SR | 58 | 2001 | III | >150 | <35% |
| MIRACLE | 453 | 2002 | III, IV | >130 | <35% |
| MUSTIC-AF | 43 | 2002 | III | >200 | <35% |
| PATH-CHF | 41 | 2002 | III, IV | >120 | <35% |
| MIRACLE ICD | 369 | 2003 | III, IV | >130 | <35% |
| CONTAK CD | 227 | 2003 | III, IV | >120 | <35% |
| MIRACLE ICD II | 186 | 2004 | II | >130 | <35% |
| PATH-CHF II | 89 | 2004 | III, IV | >120 | <35% |
| COMPANION | 1520 | 2005 | III, IV | >120 | <35% |
| CARE-HF | 814 | 2006 | III, IV | >120 | <35% |
| REVERSE | 610 | 2008 | I, II | >120 | <40% |
| MADIT-CRT | 1800 | 2009 | I, II | >130 | <30% |
| RAFT | 1798 | 2010 | I, II | >130 | <30% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radu, A.D.; Cojocaru, C.; Onciul, S.; Scarlatescu, A.; Zlibut, A.; Nastasa, A.; Dorobantu, M. Cardiac Resynchronization Therapy and Hypertrophic Cardiomyopathy: A Comprehensive Review. Biomedicines 2023, 11, 350. https://doi.org/10.3390/biomedicines11020350
Radu AD, Cojocaru C, Onciul S, Scarlatescu A, Zlibut A, Nastasa A, Dorobantu M. Cardiac Resynchronization Therapy and Hypertrophic Cardiomyopathy: A Comprehensive Review. Biomedicines. 2023; 11(2):350. https://doi.org/10.3390/biomedicines11020350
Chicago/Turabian StyleRadu, Andrei Dan, Cosmin Cojocaru, Sebastian Onciul, Alina Scarlatescu, Alexandru Zlibut, Alexandrina Nastasa, and Maria Dorobantu. 2023. "Cardiac Resynchronization Therapy and Hypertrophic Cardiomyopathy: A Comprehensive Review" Biomedicines 11, no. 2: 350. https://doi.org/10.3390/biomedicines11020350