
Impact of CPAP Therapy on the Autonomic Nervous System


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Study Design
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lévy, P.; Kohler, M.; McNicholas, W.T.; Barbé, F.; McEvoy, R.D.; Somers, V.K.; Lavie, L.; Pépin, J.L. Obstructive sleep apnoea syndrome. Nat. Rev. Dis. Primers 2015, 1, 15015. [Google Scholar] [CrossRef]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.-L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Veasey, S.C.; Rosen, I.M. Obstructive Sleep Apnea in Adults. N. Engl. J. Med. 2019, 380, 1442–1449. [Google Scholar] [CrossRef] [PubMed]
- Franklin, K.A.; Sahlin, C.; Stenlund, H.; Lindberg, E. Sleep apnoea is a common occurrence in females. Eur. Respir. J. 2013, 41, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2018, 138, e484–e594. [Google Scholar] [CrossRef]
- Yeghiazarians, Y.; Jneid, H.; Tietjens, J.R.; Redline, S.; Brown, D.L.; El-Sherif, N.; Mehra, R.; Bozkurt, B.; Ndumele, C.E.; Somers, V.K. Obstructive Sleep Apnea and Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation 2021, 144, e56–e67. [Google Scholar] [CrossRef] [PubMed]
- Muxfeldt, E.S.; Margallo, V.S.; Guimarães, G.M.; Salles, G.F. Prevalence and associated factors of obstructive sleep apnea in patients with resistant hypertension. Am. J. Hypertens. 2014, 27, 1069–1078. [Google Scholar] [CrossRef]
- Abbasi, A.; Gupta, S.S.; Sabharwal, N.; Meghrajani, V.; Sharma, S.; Kamholz, S.; Kupfer, Y. A comprehensive review of obstructive sleep apnea. Sleep Sci. 2021, 14, 142–154. [Google Scholar] [CrossRef]
- Sasaki, N.; Ozono, R.; Edahiro, Y.; Ishii, K.; Seto, A.; Okita, T.; Teramen, K.; Fujiwara, S.; Kihara, Y. Impact of non-dipping on cardiovascular outcomes in patients with obstructive sleep apnea syndrome. Clin. Exp. Hypertens. 2015, 37, 449–453. [Google Scholar] [CrossRef]
- Kanclerska, J.; Wieckiewicz, M.; Nowacki, D.; Szymanska-Chabowska, A.; Poreba, R.; Mazur, G.; Martynowicz, H. Sleep architecture and vitamin D in hypertensives with obstructive sleep apnea: A polysomnographic study. Dent. Med. Probl. 2023. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Ryan, S. Mechanisms of cardiovascular disease in obstructive sleep apnoea. J. Thorac. Dis. 2018, 10 (Suppl. S34), S4201–S4211. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wu, H.; Zhang, X.; Wei, X.; Hou, F.; Ma, Y. Sleep heart rate variability assists the automatic prediction of long-term cardiovascular outcomes. Sleep Med. 2020, 67, 217–224. [Google Scholar] [CrossRef]
- Camm, A.J.; Malik, M.; Bigger, J.T.; Breithardt, G.; Cerutti, S.; Cohen, R.J.; Coumel, P.; Fallen, E.; Kennedy, H.; Kleiger, R.; et al. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar]
- Hayano, J.; Yuda, E. Pitfalls of assessment of autonomic function by heart rate variability. J. Physiol. Anthropol. 2019, 38, 3. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, C.; Pengo, M.F.; Parati, G. Obstructive sleep apnea syndrome and autonomic dysfunction. Auton. Neurosci. 2019, 221, 102563. [Google Scholar] [CrossRef]
- Sequeira, V.C.C.; Bandeira, P.M.; Azevedo, J.C.M. Heart rate variability in adults with obstructive sleep apnea: A systematic review. Sleep Sci. 2019, 12, 214–221. [Google Scholar] [CrossRef]
- Urbanik, D.; Gać, P.; Martynowicz, H.; Podgórski, M.; Poręba, M.; Mazur, G.; Poręba, R. Obstructive Sleep Apnea as a Predictor of Arrhythmias in 24-h ECG Holter Monitoring. Brain Sci. 2021, 11, 486. [Google Scholar] [CrossRef] [PubMed]
- Maniaci, A.; Di Luca, M.; Lechien, J.R.; Iannella, G.; Grillo, C.; Grillo, C.M.; Merlino, F.; Calvo-Henriquez, C.; De Vito, A.; Magliulo, G.; et al. Lateral pharyngoplasty vs. traditional uvulopalatopharyngoplasty for patients with OSA: Systematic review and meta-analysis. Sleep Breath. 2022, 26, 1539–1550. [Google Scholar] [CrossRef]
- Martynowicz, H.; Wieczorek, T.; Macek, P.; Wojakowska, A.; Poręba, R.; Gać, P.; Mazur, G.; Skomro, R.; Smardz, J.; Więckiewicz, M. The effect of continuous positive airway pressure and mandibular advancement device on sleep bruxism intensity in obstructive sleep apnea patients. Chron. Respir. Dis. 2022, 19, 14799731211052301. [Google Scholar] [CrossRef] [PubMed]
- Randerath, W.; Verbraecken, J.; de Raaff, C.A.; Hedner, J.; Herkenrath, S.; Hohenhorst, W.; Jakob, T.; Marrone, O.; Marklund, M.; McNicholas, W.T.; et al. European Respiratory Society guideline on non-CPAP therapies for obstructive sleep apnoea. Eur. Respir. Rev. 2021, 30, 210200. [Google Scholar] [CrossRef]
- Greenlund, I.M.; Carter, J.R. Sympathetic neural responses to sleep disorders and insufficiencies. Am. J. Physiol. Heart Circ. Physiol. 2022, 322, H337–H349. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, R.D.; Antic, N.A.; Heeley, E.; Luo, Y.; Ou, Q.; Zhang, X.; Mediano, O.; Chen, R.; Drager, L.F.; Liu, Z.; et al. CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea. N. Engl. J. Med. 2016, 375, 919–931. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-De-La-Torre, M.; Sánchez-De-La-Torre, A.; Bertran, S.; Abad, J.; Duran-Cantolla, J.; Cabriada, V.; Mediano, O.; Masdeu, M.J.; Alonso, M.L.; Masa, J.F.; et al. Effect of obstructive sleep apnoea and its treatment with continuous positive airway pressure on the prevalence of cardiovascular events in patients with acute coronary syndrome (ISAACC study): A randomised controlled trial. Lancet Respir. Med. 2020, 8, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Peker, Y.; Glantz, H.; Eulenburg, C.; Wegscheider, K.; Herlitz, J.; Thunström, E. Effect of Positive Airway Pressure on Cardiovascular Outcomes in Coronary Artery Disease Patients with Nonsleepy Obstructive Sleep Apnea. The RICCADSA Randomized Controlled Trial. Am. J. Respir. Crit. Care Med. 2016, 194, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Baratta, F.; Pastori, D.; Fabiani, M.; Fabiani, V.; Ceci, F.; Lillo, R.; Lolli, V.; Brunori, M.; Pannitteri, G.; Cravotto, E.; et al. Severity of OSAS, CPAP and cardiovascular events: A follow-up study. Eur. J. Clin. Investig. 2018, 48, e12908. [Google Scholar] [CrossRef]
- Javaheri, S.; Martinez-Garcia, M.A.; Campos-Rodriguez, F.; Muriel, A.; Peker, Y. Continuous Positive Airway Pressure Adherence for Prevention of Major Adverse Cerebrovascular and Cardiovascular Events in Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2020, 201, 607–610. [Google Scholar] [CrossRef]
- Friščić, T.; Perčić, M.; Vidović, D.; Štajduhar, A.; Galić, E. Impact of CPAP Therapy on New Inflammation Biomarkers. J. Clin. Med. 2022, 11, 6113. [Google Scholar] [CrossRef]
- Fava, C.; Dorigoni, S.; Vedove, F.D.; Danese, E.; Montagnana, M.; Guidi, G.C.; Narkiewicz, K.; Minuz, P. Effect of CPAP on blood pressure in patients with OSA/hypopnea a systematic review and meta-analysis. Chest 2014, 145, 762–771. [Google Scholar] [CrossRef]
- Labarca, G.; Schmidt, A.; Dreyse, J.; Jorquera, J.; Enos, D.; Torres, G.; Barbe, F. Efficacy of continuous positive airway pressure (CPAP) in patients with obstructive sleep apnea (OSA) and resistant hypertension (RH): Systematic review and meta-analysis. Sleep Med. Rev. 2021, 58, 101446. [Google Scholar] [CrossRef]
- Feldstein, C.A. Blood pressure effects of CPAP in nonresistant and resistant hypertension associated with OSA: A systematic review of randomized clinical trials. Clin. Exp. Hypertens. 2016, 38, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Kim, S.Y.; Park, D.Y.; Wu, H.W.; Hwang, G.S.; Kim, H.J. Clinical Implication of Heart Rate Variability in Obstructive Sleep Apnea Syndrome Patients. J. Craniofac Surg. 2015, 26, 1592–1595. [Google Scholar] [CrossRef] [PubMed]
- Nastałek, P.; Bochenek, G.; Kania, A.; Celejewska-Wójcik, N.; Mejza, F.; Sładek, K. Heart Rate Variability in the Diagnostics and CPAP Treatment of Obstructive Sleep Apnea. Adv. Exp. Med. Biol. 2019, 1176, 25–33. [Google Scholar] [CrossRef]
- Tobaldini, E.; Nobili, L.; Strada, S.; Casali, K.R.; Braghiroli, A.; Montano, N. Heart rate variability in normal and pathological sleep. Front. Physiol. 2013, 4, 294. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.; Choi, K.H.; Park, J.H.; Song, T.-J.; Choi, Y.S.; Kim, J.-H.; Kim, H.J.; Lee, H.W. Sympathetic Overactivity Based on Heart-Rate Variability in Patients with Obstructive Sleep Apnea and Cerebral Small-Vessel Disease. J. Clin. Neurol. 2018, 14, 310–319. [Google Scholar] [CrossRef]
- Jaramillo, A.P.; Yasir, M.; Iyer, N.; Hussein, S.; Sn, V.P. Sudden Cardiac Death: A Systematic Review. Cureus 2023, 15, e42859. [Google Scholar] [CrossRef]
- Rossi, V.A.; Stoewhas, A.-C.; Camen, G.; Steffel, J.; Bloch, K.E.; Stradling, J.R.; Kohler, M. The effects of continuous positive airway pressure therapy withdrawal on cardiac repolarization: Data from a randomized controlled trial. Eur. Heart J. 2012, 33, 2206–2212. [Google Scholar] [CrossRef]
- Viigimae, M.; Karai, D.; Pilt, K.; Pirn, P.; Huhtala, H.; Polo, O.; Meigas, K.; Kaik, J. QT interval variability index and QT interval duration during different sleep stages in patients with obstructive sleep apnea. Sleep Med. 2017, 37, 160–167. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (years) | 53 ± 10 |
| Male/female gender | 29/8 |
| BMI (kg/m2) | 34.4 ± 6.1 |
| Smoker (number/%) | 10/27 |
| Comorbidities | |
| Hypertension (number/%) | 19/51 |
| CVD | 1 * |
| COPD | 2 |
| Diabetes mellitus (number/%) | 6/16 |
| CKD | 1 * |
| Polysomnographic parameters | |
| AHI (events/h) | 58.4 ± 22 |
| CA (events/h) | 1.3 |
| OA (events/h) | 33.35 |
| Hypopnea (events/h) | 11.15 |
| Average apnea duration (s) | 24.2 ± 6.1 |
| Minimum O2 saturation (%) | 74.03 ± 11.36 |
| ESS | 10.6 ± 5.2 |
| Average time of CPAP therapy per night (min) | 322.3 ± 51.3 |
| Duration of CPAP therapy (days) | 290.49 ± 56.7 |
| Before CPAP Therapy | After CPAP Therapy | p-Value | |
|---|---|---|---|
| Systolic blood pressure | |||
| Diurnal (mmHg) | 147 (131–156) | 139 (131–156) | 0.7833 |
| Nocturnal (mmHg) | 137 (129–150) | 130 (117–146) | 0.0853 |
| 24 h (mmHg) | 145 (128–153) | 139 (125–154) | 0.3814 |
| Maximum value (mmHg) | 176.81 ± 26.35 | 177.43 ± 22.85 | 0.9027 |
| Diastolic blood pressure | |||
| Diurnal (mmHg) | 82 (76–90) | 80 (73–89) | 0.4319 |
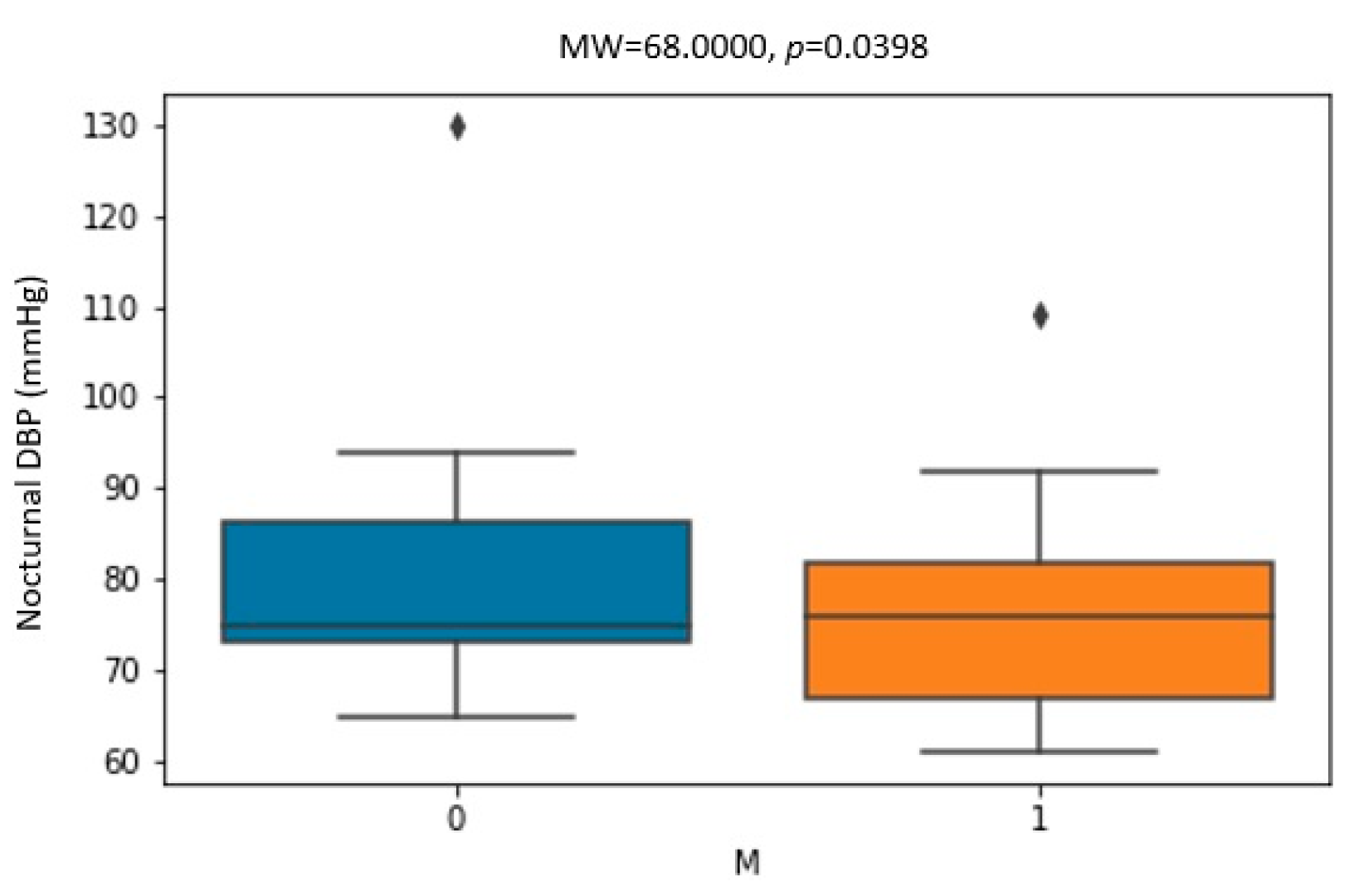
| Nocturnal (mmHg) | 76 (68–84) | 74 (63–80) | 0.0439 |
| 24 h (mmHg) | 81 (73–88) | 78 (72–85) | 0.141 |
| Maximum value (mmHg) | 107 (96–118) | 107 (96–119) | 0.8621 |
| SBP dipping (mmHg) | 4.57 ± 7.97 | 7.31 ± 7.67 | 0.0706 |
| DBP dipping (mmHg) | 9.3 (2.9–15.8) | 10.5 (4.2–18.7) | 0.1818 |
| Before CPAP Therapy | After CPAP Therapy | p-Value | |
|---|---|---|---|
| Minimum HR (/min) | 49.08 ± 6.09 | 49.73 ± 5.59 | 0.5013 |
| Maximum HR (/min) | 129 (118–140) | 124 (116–137) | 0.8937 |
| Average HR (/min) | 78 (73–82) | 74 (69–79) | 0.0165 |
| SVEB (number) | 12 (3–60) | 7 (2–46) | 0.5437 |
| VEB (number) | 5 (1–72) | 4 (0–50) | 0.1629 |
| VT (1—yes, 0—no) | 0 | 0 | |
| Pauses >2 s (1—yes, 0—no) | 0 | 0 | |
| Time domain | |||
| SDNN-24 h (ms) | 128.25 ± 31.79 | 128.61 ± 30.24 | 0.9396 |
| SDANN index (ms) | 120 (97.5–142) | 109 (96.5–137) | 0.8844 |
| SDNN index (ms) | 47 (39–56.5) | 44 (39–53.5) | 0.9715 |
| RMSSD-24 h (ms) | 23 (18–27) | 20 (18–26.5) | 0.3632 |
| pNN50-24 h (%) | 3 (1–6) | 3 (1–5.5) | 0.2529 |
| SDNN day (ms) | 103.53 ± 25.84 | 104.12 ± 25.81 | 0.8738 |
| RMSSD day (ms) | 17.5 (15–21.75) | 18 (15–23) | 0.6396 |
| pNN50 day (%) | 1 (0–2.75) | 1 (0–4) | 0.8641 |
| SDNN night (ms) | 101.5 (88–122) | 95 (73.75–108) | 0.0492 |
| RMSSD night (ms) | 29.5 (22.25–39.75) | 26 (20.5–31.75) | 0.0193 |
| pNN50 night (%) | 7 (3–15.25) | 6 (2–10.75) | 0.0892 |
| Frequency domain | |||
| Spectral power average (ms2) | 2470 (1529–3754) | 2187 (1636–3203) | 0.9499 |
| VLF average (ms2) | 1855 (1138–2911) | 1677 (1116–2294) | 0.7432 |
| LF average (ms2) | 508 (289.35–76.8) | 393.9 (294.6–685.6) | 0.359 |
| HF average (ms2) | 155.6 (71.25–219.9) | 92.6 (71.75–175.45) | 0.1318 |
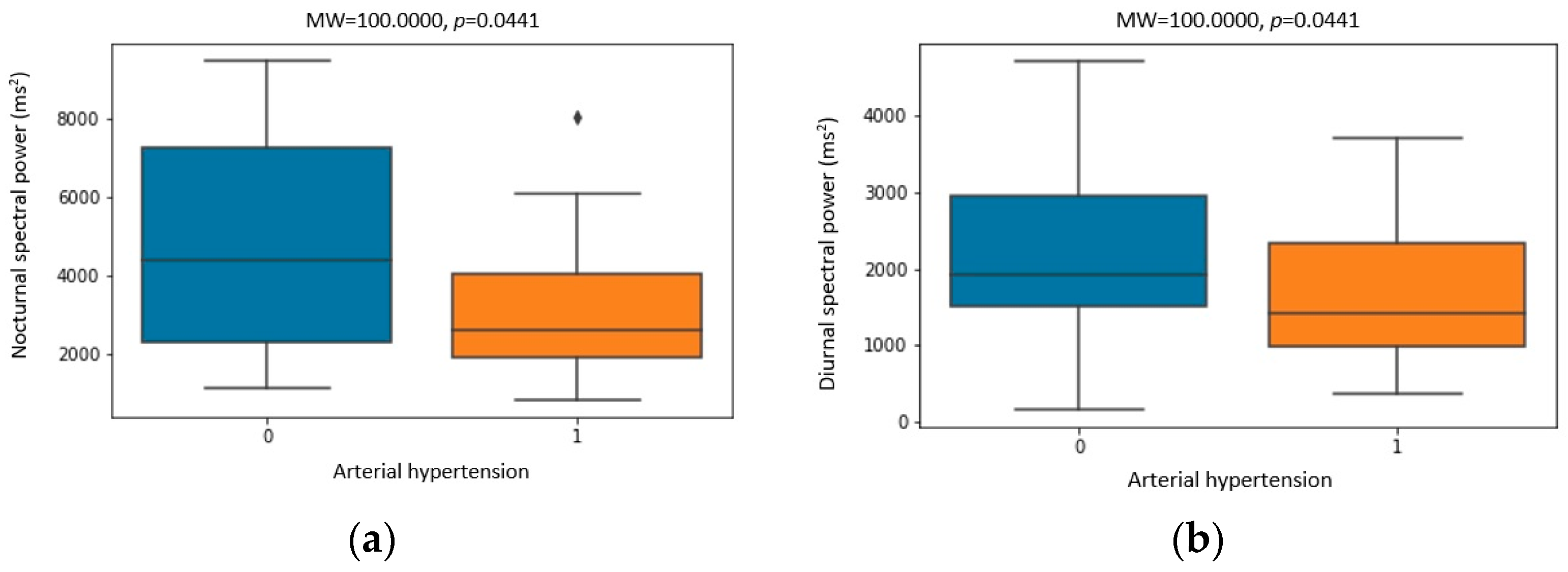
| Spectral power day (ms2) | 1742 (1205–2794) | 2112 (1457–2721) | 0.0282 |
| VLF day (ms2) | 1328 (972–2083) | 1586 (1069–1989) | 0.0513 |
| LF day (ms2) | 378.5 (204.85–627.2) | 396 (220.4–625.9) | 0.3339 |
| HF day (ms2) | 69.8 (37.95–123.6) | 66.6 (44.25–125.75) | 0.7432 |
| Spectral power night (ms2) | 3256 (1923–5603) | 2124 (1544–4129) | 0.0097 |
| VLF night (ms2) | 2493 (1348–3735) | 1485 (1072–2727) | 0.0176 |
| LF night (ms2) | 638.7 (377.85–1273.85) | 473 (315.50–949.95) | 0.0097 |
| HF night (ms2) | 234.9 (118.95–360.2) | 135.7 (98.00–286.1) | 0.0319 |
| LF/HF average | 3.18 (2.36–5.92) | 4.03 (2.73–5.03) | 0.5445 |
| LF/HF day | 4.98 (3.14–6.56) | 4.63 (3.26–6.47) | 0.9608 |
| LF/HF night | 3.08 (1.85–5.12) | 3.14 (2.06–4.73) | 0.7186 |
| QT (ms) | 465 (444–483) | 456 (442–480) | 0.7063 |
| QTc (ms) | 492 (481–539) | 499 (481.5–509) | 0.3898 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Friščić, T.; Vidović, D.; Alfirević, I.; Galić, E. Impact of CPAP Therapy on the Autonomic Nervous System. Biomedicines 2023, 11, 3210. https://doi.org/10.3390/biomedicines11123210
Friščić T, Vidović D, Alfirević I, Galić E. Impact of CPAP Therapy on the Autonomic Nervous System. Biomedicines. 2023; 11(12):3210. https://doi.org/10.3390/biomedicines11123210
Chicago/Turabian StyleFriščić, Tea, Domagoj Vidović, Igor Alfirević, and Edvard Galić. 2023. "Impact of CPAP Therapy on the Autonomic Nervous System" Biomedicines 11, no. 12: 3210. https://doi.org/10.3390/biomedicines11123210