
The Interplay between Muscular Grip Strength and Bone Mineral Density with Consideration of Metabolic and Endocrine Parameters in Individuals with Turner Syndrome
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Biochemical Analyses
2.2.1. Assessment of Bone Mineralization
2.2.2. Assessment of Body Composition
2.3. Muscle Function Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schoenau, E. From mechanostat theory to development of the “Functional Muscle-Bone-Unit”. J. Musculoskelet. Neuronal Interact. 2005, 5, 232–238. [Google Scholar]
- Fuchs, R.K.; Shea, M. Bone health and resistance exercise. ACSM’s Health Fit. J. 1997, 1, 30–37. [Google Scholar]
- Turner, C.H.; Robling, A.G. Designing exercise regimens to increase bone strength. Exerc. Sport. Sci. Rev. 2003, 31, 45–50. [Google Scholar] [CrossRef]
- Steiner, M.; Saenger, P. Turner Syndrome: An Update. Adv. Pediatr. 2022, 69, 177–202. [Google Scholar] [CrossRef]
- Gravholt, C.H.; Viuff, M.; Just, J.; Sandahl, K.; Brun, S.; van der Velden, J.; Andersen, N.H.; Skakkebaek, A. The Changing Face of Turner Syndrome. Endocr. Rev. 2023, 44, 33–69. [Google Scholar] [CrossRef]
- Sybert, V.P. Turner syndrome. N. Engl. J. Med. 2008, 358, 1480–1482. [Google Scholar]
- Wong, S.C.; Ong, H.L.; Kaluarachchi, D.C.; Fort, P.; Roberts, K.D. Skeletal muscle in Turner syndrome: Relationships between muscle mass, muscle strength and function. J. Clin. Endocrinol. Metab. 2021, 106, e1667–e1681. [Google Scholar]
- Zeger, M.P.; Smith, J.R.; Owens, G.M.; Dunn, J.D.; Lee, P.A. Osteoporosis in Turner syndrome. J. Clin. Endocrinol. Metab. 2020, 105, e2329–e2339. [Google Scholar]
- Pirgon, O.; Atabek, M.E. Evaluation of bone mineral density in girls with Turner syndrome: A cross-sectional study. J. Clin. Res. Pediatr. Endocrinol. 2011, 3, 7–12. [Google Scholar]
- Högler, W.; Wehl, G.; van der Sluis, I.M.; Bath, L. Bone mass and body composition in young women with Turner syndrome. Bone 2006, 39, 480–487. [Google Scholar]
- Rauch, F.; Blum, W.F.; Klein, K.; Allolio, B.; Schönau, E. Skeletal response to growth hormone treatment in children with osteogenesis imperfecta. Horm. Res. 2003, 60 (Suppl. S3), 50–53. [Google Scholar]
- Manolagas, S.C.; Parfitt, A.M. What old means to bone. Trends Endocrinol. Metab. 2010, 21, 369–374. [Google Scholar] [CrossRef]
- Scott, D.; Ebeling, P.R. Handgrip strength as a predictor of outcomes in females over 20 years. Calcif. Tissue Int. 2018, 102, 531–541. [Google Scholar]
- Davenport, M.L. Approach to the patient with Turner syndrome. J. Clin. Endocrinol. Metab. 2010, 95, 1487–1495. [Google Scholar] [CrossRef]
- Stochholm, K.; Juul, S.; Juel, K.; Naeraa, R.W.; Gravholt, C.H. Prevalence, incidence, diagnostic delay, and mortality in Turner syndrome. J. Clin. Endocrinol. Metab. 2006, 91, 3897–3902. [Google Scholar] [CrossRef]
- Hägg, A.; Zemack, H.; Arver, S.; Dahlqvist, P. Muscle strength and aerobic capacity in Turner syndrome: A controlled study. J. Clin. Endocrinol. Metab. 2013, 98, E1162–E1168. [Google Scholar]
- Davenport, M.L. Approach to the patient: Growth disorders in girls with Turner syndrome. J. Clin. Endocrinol. Metab. 2015, 104, 2689–2700. [Google Scholar]
- Gravholt, C.H.; Andersen, N.H.; Conway, G.S.; Dekkers, O.M.; Geffner, M.E.; Klein, K.O.; Lin, A.E.; Mauras, N.; Quigley, C.A.; Rubin, K.; et al. Clinical practice guidelines for the care of girls and women with Turner syndrome: Proceedings from the 2016 Cincinnati International Turner Syndrome Meeting. Eur. J. Endocrinol. 2017, 177, G1–G70. [Google Scholar] [CrossRef]
- Bechtold, S.; Rauch, F.; Noelle, V.; Donhauser, S.; Neu, C.M.; Schoenau, E.; Schwarz, H.P. Musculoskeletal analyses of the forearm in young women with Turner syndrome: A study using peripheral quantitative computed tomography. J. Clin. Endocrinol. Metab. 2001, 86, 5819–5823. [Google Scholar] [CrossRef]
- Soucek, O.; Lebl, J.; Matyskova, J.; Snajderova, M.; Kolouskova, S.; Pruhova, S.; Hlavka, Z.; Sumnik, Z. Muscle function in Turner syndrome: Normal force but decreased power. Clin. Endocrinol. 2015, 82, 248–253. [Google Scholar] [CrossRef]
- Wasniewska, M.; Bombaci, S.; Matarazzo, P. Turner syndrome: Review of the literature. Acta Medica Mediterr. 2017, 33, 273–280. [Google Scholar]
- Meyer, G.; Rumpel, E.; Sänger, N.; Stücker, R.; Häger, C.; Günther, J. Effects of growth hormone therapy on muscle strength in men with AIDS wasting. Growth Horm. IGF Res. 2016, 29, 12–17. [Google Scholar]
- Ebeling, P.R.; Nguyen, H.H.; Aleksova, J.; Vincent, A.J.; Wong, P.; Milat, F. Secondary Osteoporosis. Endocr. Rev. 2022, 43, 240–313. [Google Scholar] [CrossRef]
- Augoulea, A.; Zachou, G.; Lambrinoudaki, I. Turner syndrome and osteoporosis. Maturitas 2019, 130, 41–49. [Google Scholar] [CrossRef]
- Fine, A.; Busza, A.; Allen, L.M.; Kelly, C.; Wolfman, W.; Jacobson, M.; Lega, I.C. Comparing estrogen-based hormonal contraceptives and hormone therapy on bone mineral density in women with premature ovarian insufficiency: A systematic review. Menopause 2022, 29, 351–359. [Google Scholar] [CrossRef]
- Robinson, J.A.; Harris, S.A.; Riggs, B.L.; Spelsberg, T.C. Estrogen regulation of human osteoblastic cell proliferation and differentiation. Endocrinology 1997, 138, 2919–2927. [Google Scholar] [CrossRef]
- Khosla, S. The effects of androgens on osteoblast function in vitro. Mayo Clin. Proc. 2000, 75, 51–54. [Google Scholar] [CrossRef]
- Gravholt, C.H.; Svenstrup, B.; Bennet, P.; Christiansen, J.S. Reducet androgen levels in adult Turner syndrome: Influence of female sex steroids and growth hormone status. Clin. Endocrinol. 1999, 50, 791–800. [Google Scholar] [CrossRef]
- Milde, K.; Tomaszewski, P.; Stupnicki, R. Physical fitness of schoolgirls with Turner syndrome. Pediatr. Exerc. Sci. 2013, 25, 27–42. [Google Scholar] [CrossRef]
- Gravholt, C.H.; Nyholm, B.; Saltin, B.; Schmitz, O.; Christiansen, J.S. Muscle fiber composition and capillary density in Turner syndrome: Evidence of increased muscle fiber size related to insulin resistance. Diabetes Care 2001, 24, 1668–1673. [Google Scholar] [CrossRef]
- Burr, D.B. Muscle strength, bone mass, and age-related bone loss. J. Bone Min. Res. 1997, 12, 1547–1551. [Google Scholar] [CrossRef]
- Frost, H.M.; Schönau, E. The “musclebone unit” in children and adolescents: A 2000 overview. J. Pediatr. Endocrinol. Metab. 2000, 3, 571–590. [Google Scholar]
- Malanowska, E.; Starczewski, A.; Bielewicz, W.; Balzarro, M. Assessment of Overactive Bladder after Laparoscopic Lateral Suspension for Pelvic Organ Prolapse. Biomed. Res. Int. 2019, 2019, 9051963. [Google Scholar] [CrossRef]
- Rauch, F.; Schönau, E. The developing bone: Slave or master of its cells and molecules? Pediatr. Res. 2001, 50, 309–314. [Google Scholar] [CrossRef]
- Gnacińska, M.; Magnuszewska, H.; Sworczak, K. Metabolic consequences of recombinant human growth hormone therapy in patients with Turner syndrome. Pediatr. Endocrinol. Diabetes Metab. 2023, 29, 16–21. [Google Scholar] [CrossRef]
- Larsson, H.; Ahren, B. Androgen activity as a risk factor for impaired glucose tolerance in postmenopausal women. Diabetes Care 1996, 19, 1399–1403. [Google Scholar] [CrossRef]
- Rutherford, O.M.; Jones, D.A. The relationship of muscle and bone loss and activity levels with age in women. Age Ageing 1992, 21, 286–293. [Google Scholar] [CrossRef]
- Phillips, S.K.; Rook, K.M.; Siddle, N.C.; Bruce, S.A.; Woledge, R.C. Muscle weakness in women occurs at an earlier age than in men, but strength is preserved by hormone replacement therapy. Clin. Sci. Colch. 1993, 84, 95–98. [Google Scholar] [CrossRef]
- Ruszala, A.; Wojcik, M.; Zygmunt-Gorska, A.; Janus, D.; Wojtys, J.; Starzyk, J.B. Prepubertal ultra-low-dose estrogen therapy is associated with healthier lipid profile than conventional estrogen replacement for pubertal induction in adolescent girls with Turner syndrome: Preliminary results. J. Endocrinol. Investig. 2017, 40, 875–879. [Google Scholar] [CrossRef]
- Schrager, M.A.; Metter, E.J.; Simonsick, E.; Ble, A.; Bandinelli, S.; Lauretani, F. Sarcopenic obesity and inflammation in the InCHIANTI study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 863–868. [Google Scholar] [CrossRef]
- Backeljauw, P.F.; Bondy, C.A. Turner syndrome update: Reproductive and cardiovascular issues. Fertil. Steril. 2012, 98, 787–793. [Google Scholar]
- Wojcik, M.; Janus, D.; Zygmunt-Gorska, A.; Starzyk, J.B. Insulin resistance in adolescents with Turner syndrome is comparable to obese peers, but the overall metabolic risk is lower due to unknown mechanism. J. Endocrinol. Investig. 2015, 38, 345–349. [Google Scholar] [CrossRef]
- Salgin, B.; Amin, R.; Yuen, K.; Williams, R.M.; Murgatroyd, P.; Dunger, D.B. Insulin resistance is an intrinsic defect independent of fat mass in women with Turner’s syndrome. Horm. Res. 2006, 65, 69–75. [Google Scholar] [CrossRef]
- Giordano, R.; Forno, D.; Lanfranco, F.; Manieri, C.; Ghizzoni, L.; Ghigo, E. Metabolic and cardiovascular outcomes in a group of adult patients with Turner’s syndrome under hormonal replacement therapy. Eur. J. Endocrinol. 2011, 164, 819–826. [Google Scholar] [CrossRef]
- Gravholt, C.H.; Hjerrild, B.E.; Naeraa, R.W.; Engbaek, F.; Mosekilde, L.; Christiansen, J.S. Effect of growth hormone and 17beta-oestradiol treatment on metabolism and body composition in girls with Turner syndrome. Clin. Endocrinol. 2005, 62, 616–622. [Google Scholar] [CrossRef]
- Ostberg, J.E.; Thomas, E.L.; Hamilton, G.; Attar, M.J.; Bell, J.D.; Conway, G.S. Excess visceral and hepatic adipose tissue in Turner syndrome determined by magnetic resonance imaging: Estrogen deficiency associated with hepatic adipose content. J. Clin. Endocrinol. Metab. 2005, 90, 2631–2635. [Google Scholar] [CrossRef]
- Gravholt, C.H.; Juul, S.; Naeraa, R.W.; Hansen, J. Morbidity in Turner syndrome. J. Clin. Epidemiol. 2009, 51, 147–158. [Google Scholar] [CrossRef]
- Lozano, P.; Henrikson, N.B.; Dunn, J.; Morrison, C.C.; Nguyen, M.; Whitlock, E.P. Lipid Screening in Childhood for Detection of Multifactorial Dyslipidemia: A Systematic Evidence review for the US Preventive Services Task Force. 2016. Available online: https://pubmed.ncbi.nlm.nih.gov/27559550/ (accessed on 16 September 2023).
- Bugajska, J.; Berska, J.; Wójcik, M.; Starzyk, J.B.; Sztefko, K. Metabolic Fingerprint of Turner Syndrome. J. Clin. Med. 2020, 9, 664. [Google Scholar] [CrossRef]
- Carvalho, C.M.B.; Coban-Akdemir, Z.; Hijazi, H.; Yuan, B.; Pendleton, M.; Harrington, E.; Beaulaurier, J.; Juul, S.; Turner, D.J.; Kanchi, R.S.; et al. Interchromosomal template-switching as a novel molecular mechanism for imprinting perturbations associated with Temple syndrome. Genome Med. 2019, 11, 25. [Google Scholar] [CrossRef]
- Casanova, G.; Bossardi Ramos, R.; Ziegelmann, P.; Spritzer, P. Effects of low-dose versus placebo or conventional dose postmenopausal hormone therapy on variables related to cardiovascular risk: A systematic review and meta-analyses of randomized clinical trials. J. Clin. Endocrinol. Metab. 2015, 100, 1028–1037. [Google Scholar] [CrossRef]
- Aycan, Z.; Cetinkaya, E.; Darendeliler, F.; Vidinlisan, S.; Bas, F.; Bideci, A.; Demirel, F.; Darcan, S.; Buyukgebiz, A.; Yildiz, M.; et al. The effect of growth hormone treatment on bone mineral density in prepubertal girls with Turner syndrome: A multicentre prospective clinical trial. Clin. Endocrinol. 2008, 68, 769–772. [Google Scholar] [CrossRef] [PubMed]
- Sass, T.C.; De Muinck Keizer-Schrama, S.M.; Stijnen, T.; Asarfi, A.; Van Leeuwen, W.J.; Van Teunenbroek, A.; Van Rijn, R.R.; Drop, S.L. A longitudinal study on bone mineral density until adulthood in girls with Turner’s syndrome participating in a growth hormone injection frequency-response trial. Clin. Endocrinol. 2000, 52, 531–536. [Google Scholar] [CrossRef]
- Gravholt, C.H.; Hjerrild, B.E.; Mosekilde, L.; Hansen, T.K.; Rasmussen, L.M.; Frystyk, J.; Flyvbjerg, A.; Christiansen, J.S. Body composition is distinctly altered in Turner syndrome: Relations to glucose metabolism, circulating adipokines, and endothelial adhesion molecules. Eur. J. Endocrinol. 2006, 155, 583–592. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | TS; SD; n = 42 | CG; SD; n = 70 | p-value |
|---|---|---|---|
| age [years] | 23.7; 2.01 | 23.1; 1.57 | 0.779 |
| BMI 1 [kg/cm2] | 26.9; 3.67 | 22.4; 4.40 | <0.01 |
| height [cm] | 159; 4.71 | 168; 5.60 | <0.01 |
| weight [kg] | 61.9; 7.53 | 63.9; 12.3 | 0.251 |
| Characteristic | TS; SD (n) | CG; SD (n) | p-value |
|---|---|---|---|
| Glucose [mg/dL] | 87.7; 8.74 (42) | 89.6; 6.75 (70) | 0.297 |
| Insulin [mU/mL] | 12.4; 5.02 (42) | 10.9; 6.12 (70) | 0.102 |
| HOMA-IR | 2.68; 1.15 (42) | 2.45; 1.52 (70) | 0.218 |
| 25-hydroxyvitamin D | 29.4; 5.43 (40) | 27.7; 6.5 (70) | 0.310 |
| Total cholesterol [mg/dL] | 170; 52.6 (40) | 181; 27 (70) | 0.261 |
| HDL [mg/dL] | 53.6; 13.5 (40) | 71; 18.3 (70) | <0.01 |
| LDL [mg/dL] | 132; 34.5 (40) | 104; 22.9 (70) | <0.01 |
| TG [mg/dL] | 118; 52.3 (40) | 83; 32.1 (70) | <0.01 |
| Ca total [mmol/L] | 2.41; 0.159 (41) | 2.42; 0.077 (64) | 0.067 |
| Ca ion [mmol/L] | 1.26; 0.027 (32) | 1.27; 0.0393 (63) | 0.348 |
| TSH [μIU/mL] | 2.95; 1.51 (38) | 2.17; 1.05 (70) | 0.065 |
| FT4 [pg/mL] | 1.3; 0.191 (38) | 1.23; 0.16 (66) | 0.119 |
| FSH [mIU/mL] | 42.5; 28.1 (39) | 6.06; 1.88 (70) | <0.01 |
| Estradiol [pg/mL] | 45.1; 29.6 (39) | 38.7; 25.6 (70) | 0.863 |
| Prolactin [ng/mL] | 21.1; 12.2 (38) | 18.7; 10.8 (70) | 0.337 |
| Testosterone [ng/mL] | 0.267; 0.224 (38) | 0.361; 0.159 (70) | 0.032 |
| DHEA-S [μg/mL] | 157; 77.3 (42) | 258; 120 (66) | <0.01 |
| Cortisol total [μg/mL] | 13.2; 5.27 (39) | 18.8; 7.68 (63) | <0.01 |
| ACTH [pmol/L] | 14.9; 7.11 (35) | 16.9; 6.1 (60) | 0.064 |
| Characteristic | TS; SD; n = 42 | CG; SD; n = 70 | p-value |
|---|---|---|---|
| Hand grip—left [kg] | 19.1; 4.68 | 28.3; 4.67 | <0.01 |
| Hand grip—right [kg] | 18.3; 4.93 | 26.7; 4.85 | <0.01 |
| Hand grip mean [kg] | 18.7; 4.65 | 27.5; 4.40 | <0.01 |
| BF [kg] | 22.4; 10.60 | 20.7; 9.55 | 0.619 |
| VF [kg] | 0.61; 0.46 | 0.39; 0.21 | <0.01 |
| BMD Total [g/cm2] | 1.02; 0.11 | 1.15; 0.10 | <0.01 |
| BMD Total (Z-Score) | −0.2; 1.2 | 0.2; 0.9 | <0.01 |
| BMD L1–L4 [g/cm2] | 1.08; 0.16 | 1.2; 0.13 | <0.01 |
| BMD L1–L4 (Z-Score) | −0.4; 1.1 | 0.1; 0.9 | <0.01 |
| Characteristic | TS rhGH < 2 years; SD; n = 12 | TS rhGH ≥ 2 years; SD; n = 30 | p-value |
|---|---|---|---|
| Hand grip—left [kg] | 18.2; 4.28 | 20.1; 4.17 | 0.084 |
| Hand grip—right [kg] | 18.0; 4.02 | 19.6; 4.92 | 0.134 |
| Hand grip mean [kg] | 18.4; 4.15 | 19.5; 4.41 | 0.103 |
| BF [kg] | 22.6; 10.68 | 22.2; 9.13 | 0.619 |
| VF [kg] | 0.63; 0.49 | 0.60; 0.41 | 0.095 |
| BMD Total [g/cm2] | 1.01; 0.098 | 1.04; 0.0982 | 0.621 |
| BMD Total (Z-Score) | −0.2; 1.2 | −0.2; 0.9 | 0.892 |
| BMD L1–L4 [g/cm2] | 1.07; 0.12 | 1.1; 0.13 | 0.172 |
| BMD L1–L4 (Z-Score) | −0.4; 1.1 | −0.2; 0.9 | 0.065 |
| Variable 1 = Hand grip mean | |||||||
|---|---|---|---|---|---|---|---|
| Variable 2 | Group | Variable 2 p-value | Linear Model Estimate | Estimate Standard Error | R-Squared | Beta Coefficient | Beta Standard Error |
| HOMA-IR | TS | 0.0388 * abc | 1.60 | 0.738 | 0.209 | n.d. | n.d. |
| CG | 0.152 abc | −0.534 | −0.534 | 0.0573 | n.d. | n.d. | |
| TG [mg/dL] | TS | 0.0164 * n | 0.0375 | 0.0167 | 0.0755 | 0.434 | 0.170 |
| CG | 0.272 abc | −0.0188 | 0.0170 | 0.0678 | n.d. | n.d. | |
| VF [kg] | TS | 0.216 abc | 0.00237 | 0.00187 | 0.123 | n.d. | n.d. |
| CG | 0.000139 *** b | −0.00832 | 0.00242 | 0.196 | −0.747 | 0.185 | |
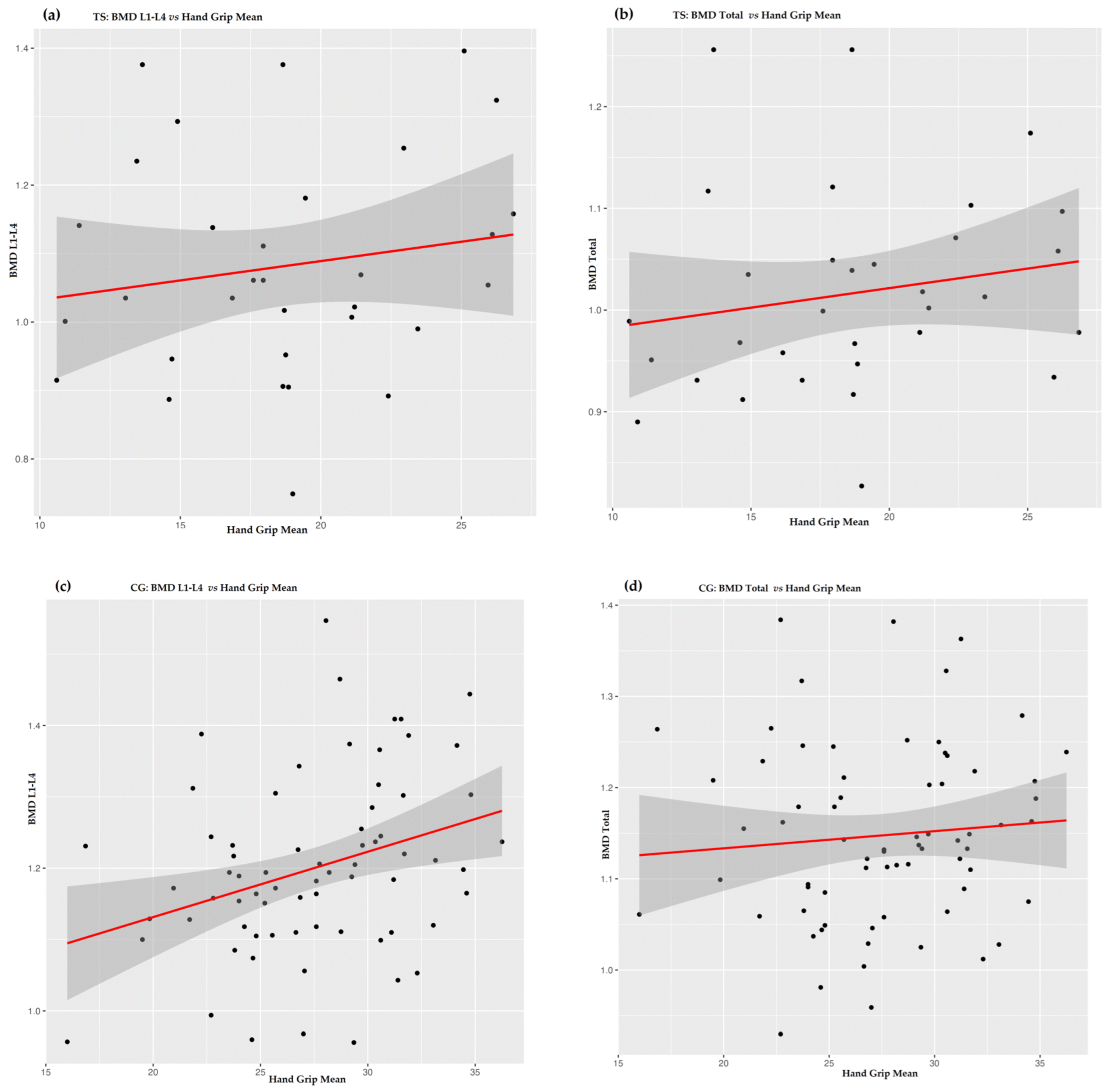
| BMD L1–L4 [g/cm2] | TS | 0.497 abc | 3.82 | 5.54 | 0.0866 | n.d. | n.d. |
| CG | 0.00622 ** | 12.0 | 4.14 | 0.163 | 0.324 | 0.115 | |
| Height | TS | 0.269 bc | −0.204 | 0.181 | −0.0291 | n.d. | n.d. |
| CG | 0.0476 * n | 0.180 | 0.0893 | 0.0432 | 0.239 | 0.119 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krzyścin, M.; Gruca-Stryjak, K.; Soszka-Przepiera, E.; Syrenicz, I.; Przepiera, A.; Cymbaluk-Płoska, A.; Bumbulienė, Ž.; Sowińska-Przepiera, E. The Interplay between Muscular Grip Strength and Bone Mineral Density with Consideration of Metabolic and Endocrine Parameters in Individuals with Turner Syndrome. Biomedicines 2023, 11, 3125. https://doi.org/10.3390/biomedicines11123125
Krzyścin M, Gruca-Stryjak K, Soszka-Przepiera E, Syrenicz I, Przepiera A, Cymbaluk-Płoska A, Bumbulienė Ž, Sowińska-Przepiera E. The Interplay between Muscular Grip Strength and Bone Mineral Density with Consideration of Metabolic and Endocrine Parameters in Individuals with Turner Syndrome. Biomedicines. 2023; 11(12):3125. https://doi.org/10.3390/biomedicines11123125
Chicago/Turabian StyleKrzyścin, Mariola, Karolina Gruca-Stryjak, Ewelina Soszka-Przepiera, Igor Syrenicz, Adam Przepiera, Aneta Cymbaluk-Płoska, Žana Bumbulienė, and Elżbieta Sowińska-Przepiera. 2023. "The Interplay between Muscular Grip Strength and Bone Mineral Density with Consideration of Metabolic and Endocrine Parameters in Individuals with Turner Syndrome" Biomedicines 11, no. 12: 3125. https://doi.org/10.3390/biomedicines11123125