
Investigating the Influential Factors of Mild Water-Filtered Infrared-A Whole-Body Hyperthermia for Pain Relief in Fibromyalgia: A Mixed-Methods Approach Focusing on Predictors and Patient Perspectives

Abstract
:1. Introduction
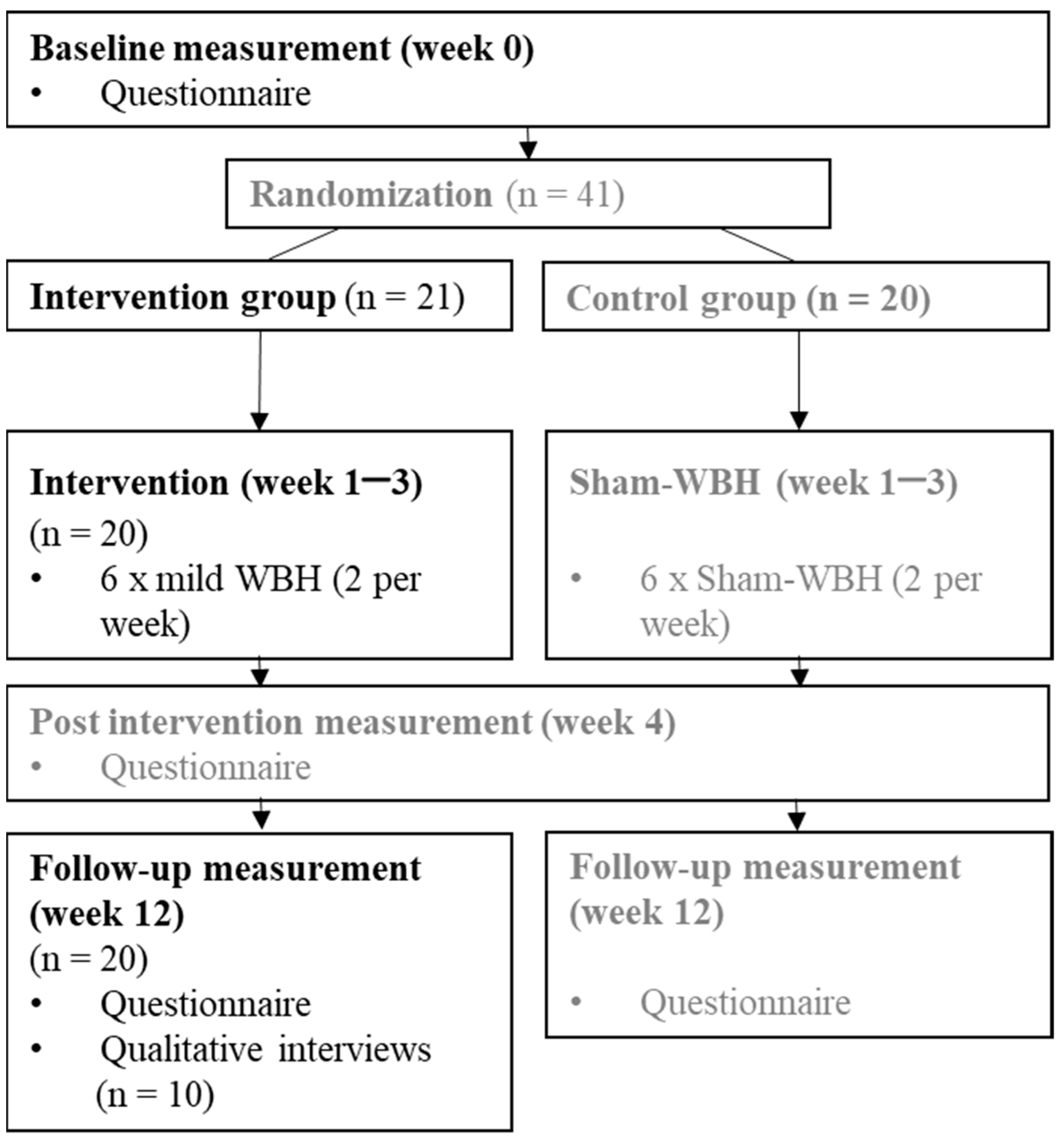
2. Materials and Methods
3. Results
3.1. Quantitative: Regression Analysis
3.2. Qualitative Interviews
“Very positive. Very positive. […] I really felt very well. Already since the first treatment. […] I did not have any circulatory problems, nor did my skin react in any way, nor anything else. Thus, I found this warmth extremely pleasant.”(P 03, female, 46 years)
“Well, the first time I was there […] And it wasn’t so great. Because I felt that at some point at the end, so the last half hour I actually felt very unpleasant. So hardly bearable and I mean, I guess I just react to everything a lot.”(P 07, female, 63 years)
“Sometimes it was okay, it was more like a sauna. And two or three times I had to struggle a lot. I was also on the verge of breaking off. So, it was very different, depending on the day-to-day condition probably.”(P 04, female, 33 years)
“Yes, because the pain was also gone, a suffering was also gone […]. And yes, I felt freer and lighter and (…) more relaxed too. […] a bit more liberated and fuller of life and joy of living.”(P 01, female, 61 years)
“Now it’s different […] it’s that things are easier for me now, much easier for me. Yes, I no longer have this daytime exhaustion, I also sleep really well. […] Yes, and the pain is there, but no longer at such a high level of pain and it no longer plays such a big role.”(P 03, female, 46 years)
“Already during the first application I thought I was almost on cloud nine, because it went much, much better. […] So the pain was not gone, but it was considerably reduced.”(P 01, female, 61 years)
“A few weeks after the study, I suddenly thought, huh? I don’t have any pain? I had then at least two weeks of no pain.”(P 08, female, 62 years)
“And two weeks after that, everything was back the same as before”;(P 04, female, 33 years)
“So the change that is quite clear is actually this improvement in getting up in the morning and the sleep is more relaxing […] And actually it is still like that now.”.(P 05, female, 54 years)
3.3. Mixed-Methods Perspective–Pain Reduction, Duration of Plateau Phase, and Improvement
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.P.; de Sousa do Espírito Santo, A.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of fibromyalgia: Literature review update. Rev. Bras. Reumatol. Engl. Ed. 2017, 57, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Creed, F. A review of the incidence and risk factors for fibromyalgia and chronic widespread pain in population-based studies. Pain 2020, 161, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Eich, W.; Bär, K.J.; Bernateck, M.; Burgmer, M.; Dexl, C.; Petzke, F.; Sommer, C.; Winkelmann, A.; Häuser, W. Definition, Klassifikation, klinische Diagnose und Prognose des Fibromyalgiesyndroms. Der Schmerz 2017, 31, 231–238. [Google Scholar] [CrossRef]
- Coles, M.L.; Weissmann, R.; Uziel, Y. Juvenile primary Fibromyalgia Syndrome: Epidemiology, etiology, pathogenesis, clinical manifestations and diagnosis. Pediatr. Rheumatol. 2021, 19, 22. [Google Scholar] [CrossRef]
- Coles, M.L.; Uziel, Y. Juvenile primary fibromyalgia syndrome: A Review—Treatment and Prognosis. Pediatr. Rheumatol. 2021, 19, 74. [Google Scholar] [CrossRef]
- Vittori, A.; Cascella, M.; Leonardi, M.; Monaco, F.; Nocerino, D.; Cuomo, A.; Ottaiano, A.; Perri, F.; Mascilini, I.; Francia, E.; et al. VOSviewer-Based Bibliometric Network Analysis for Evaluating Research on Juvenile Primary Fibromyalgia Syndrome (JPFS). Children 2022, 9, 637. [Google Scholar] [CrossRef]
- Üçeyler, N.; Burgmer, M.; Friedel, E.; Greiner, W.; Petzke, F.; Sarholz, M.; Schiltenwolf, M.; Winkelmann, A.; Sommer, C.; Häuser, W. Ätiologie und Pathophysiologie des Fibromyalgiesyndroms. Der Schmerz 2017, 31, 239–245. [Google Scholar] [CrossRef]
- Cagnie, B.; Coppieters, I.; Denecker, S.; Six, J.; Danneels, L.; Meeus, M. Central sensitization in fibromyalgia? A systematic review on structural and functional brain MRI. Semin. Arthritis Rheum. 2014, 44, 68–75. [Google Scholar] [CrossRef]
- Becker, S.; Schweinhardt, P. Dysfunctional Neurotransmitter Systems in Fibromyalgia, Their Role in Central Stress Circuitry and Pharmacological Actions on These Systems. Pain Res. Treat. 2012, 2012, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Martínez, L.-A.; Mora, T.; Vargas, A.; Fuentes-Iniestra, M.; Martínez-Lavín, M. Sympathetic Nervous System Dysfunction in Fibromyalgia, Chronic Fatigue Syndrome, Irritable Bowel Syndrome, and Interstitial Cystitis. J. Clin. Rheumatol. 2014, 20, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Tracy, L.M.; Ioannou, L.; Baker, K.S.; Gibson, S.J.; Georgiou-Karistianis, N.; Giummarra, M.J. Meta-analytic evidence for decreased heart rate variability in chronic pain implicating parasympathetic nervous system dysregulation. Pain 2016, 157, 7–29. [Google Scholar] [CrossRef] [PubMed]
- Üçeyler, N.; Zeller, D.; Kahn, A.-K.; Kewenig, S.; Kittel-Schneider, S.; Schmid, A.; Casanova-Molla, J.; Reiners, K.; Sommer, C. Small fibre pathology in patients with fibromyalgia syndrome. Brain 2013, 136, 1857–1867. [Google Scholar] [CrossRef]
- Morf, S.; Amann-Vesti, B.; Forster, A.; Franzeck, U.K.; Koppensteiner, R.; Uebelhart, D.; Sprott, H. Microcirculation abnormalities in patients with fibromyalgia—Measured by capillary microscopy and laser fluxmetry. Arthritis Res. Ther. 2005, 7, R209. [Google Scholar] [CrossRef] [PubMed]
- Gyorfi, M.; Rupp, A.; Abd-Elsayed, A. Fibromyalgia Pathophysiology. Biomedicines 2022, 10, 3070. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Ablin, J.; Fitzcharles, M.-A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Primers 2015, 1, 15022. [Google Scholar] [CrossRef]
- Marschall, U.; Arnold, B.; Häuser, W. Behandlung und Krankheitskosten des Fibromyalgiesyndroms in Deutschland. Der Schmerz 2011, 25, 402–410. [Google Scholar] [CrossRef]
- Sommer, C.; Alten, R.; Bär, K.J.; Bernateck, M.; Brückle, W.; Friedel, E.; Henningsen, P.; Petzke, F.; Tölle, T.; Üçeyler, N.; et al. Medikamentöse Therapie des Fibromyalgiesyndroms. Der Schmerz 2017, 31, 274–284. [Google Scholar] [CrossRef]
- Okifuji, A.; Gao, J.; Bokat, C.; Hare, B.D. Management of fibromyalgia syndrome in 2016. Pain Manag. 2016, 6, 383–400. [Google Scholar] [CrossRef]
- Häuser, W.; Bernardy, K.; Arnold, B.; Offenbächer, M.; Schiltenwolf, M. Efficacy of multicomponent treatment in fibromyalgia syndrome: A meta-analysis of randomized controlled clinical trials. Arthritis Rheum. 2009, 61, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Thieme, K.; Mathys, M.; Turk, D.C. Evidenced-Based Guidelines on the Treatment of Fibromyalgia Patients: Are They Consistent and If Not, Why Not? Have Effective Psychological Treatments Been Overlooked? J. Pain 2017, 18, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Crofford, L.J.; Appleton, B.E. Complementary and alternative therapies for fibromyalgia. Curr. Rheumatol. Rep. 2001, 3, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Baranowsky, J.; Klose, P.; Musial, F.; Haeuser, W.; Dobos, G.; Langhorst, J. Qualitative systemic review of randomized controlled trials on complementary and alternative medicine treatments in fibromyalgia. Rheumatol. Int. 2009, 30, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Jung, E.; Erbslöh-Möller, B.; Gesmann, M.; Kühn-Becker, H.; Petermann, F.; Langhorst, J.; Thoma, R.; Weiss, T.; Wolfe, F.; et al. The German fibromyalgia consumer reports—A cross-sectional survey. BMC Musculoskelet. Disord. 2012, 13, 74. [Google Scholar] [CrossRef]
- Petzke, F.; Brückle, W.; Eidmann, U.; Heldmann, P.; Köllner, V.; Kühn, T.; Kühn-Becker, H.; Strunk-Richter, M.; Schiltenwolf, M.; Settan, M.; et al. Allgemeine Behandlungsgrundsätze, Versorgungskoordination und Patientenschulung beim Fibromyalgiesyndrom. Der Schmerz 2017, 31, 246–254. [Google Scholar] [CrossRef]
- Heckel, M. Ganzkörperhyperthermie und Fiebertherapie: Grundlagen und Praxis; Hippokrates: Stuttgart, Germany, 1990. [Google Scholar]
- Brockow, T.; Wagner, A.; Franke, A.; Offenbächer, M.; Resch, K.L. A Randomized Controlled Trial on the Effectiveness of Mild Water-filtered Near Infrared Whole-body Hyperthermia as an Adjunct to a Standard Multimodal Rehabilitation in the Treatment of Fibromyalgia. Clin. J. Pain 2007, 23, 67–75. [Google Scholar] [CrossRef]
- Romeyke, T.; Scheuer, H.; Stummer, H. Fibromyalgia with severe forms of progression in a multidisciplinary therapy setting with emphasis on hyperthermia therapy—A prospective controlled study. Clin. Interv. Aging 2014, 10, 69–79. [Google Scholar] [CrossRef]
- Romeyke, T.; Stummer, H. Multi-Modal Pain Therapy of Fibromyalgia Syndrome with Integration of Systemic Whole-Body Hyperthermia—Effects on Pain Intensity and Mental State: A Non-Randomised Controlled Study. J. Musculoskelet. Pain 2014, 22, 341–355. [Google Scholar] [CrossRef]
- Schleenbecker, H.; Schmidt, K. Zur Wirkung einer iterativen milden Ganzkörperhyperthermie auf den Fibromyalgieschmerz—Pilotstudie. Phys. Med. Rehabilitationsmedizin Kurortmed. 1998, 8, 113–117. [Google Scholar] [CrossRef]
- Schwedtke, C. Evaluierung von Kurzzeit- und Serieneffekten von Milder Infrarot A-Hyperthermie auf Die Schmerzempfindung bei Patienten mit Fibromyalgie. Ph.D Thesis, Medizinische Fakultät Charité—Universitätsmedizin Berlin, Berlin, Germay, 2010. [Google Scholar]
- Walz, J.; Hinzmann, J.; Haase, I.; Witte, T. Ganzkörperhyperthermie in der Schmerztherapie. Der Schmerz 2013, 27, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Langhorst, J.; Koch, A.K.; Kehm, C.; Öznur, Ö.; Engler, H.; Häuser, W. Mild Water-Filtered Infrared-A Whole-Body Hyperthermia Reduces Pain in Patients with Fibromyalgia Syndrome—A Randomized Sham-Controlled Trial. J. Clin. Med. 2023, 12, 2945. [Google Scholar] [CrossRef]
- DGHT, e.V. Leitlinie zur Ganzkörperhyperthermie. Version 1.0, Oktober 2018. Available online: https://www.dght-ev.de/de/leitlinien (accessed on 15 September 2023).
- Arnold, L.M.; Williams, D.A.; Hudson, J.I.; Martin, S.A.; Clauw, D.J.; Crofford, L.J.; Wang, F.; Emir, B.; Lai, C.; Zablocki, R.; et al. Development of responder definitions for fibromyalgia clinical trials. Arthritis Rheum. 2012, 64, 885–894. [Google Scholar] [CrossRef] [PubMed]
- Patton, M.Q. Qualitative Research & Evaluation Methods: Integrating Theory and Practice, 4th ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Flick, U. An Introduction to Qualitative Research, 4th ed.; SAGE Publications, Inc.: Los Angeles, CA, USA, 2009. [Google Scholar]
- Creswell, J. Qualitative Inquiry and Research Design: Choosing among Five Approaches; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Saldana, J. Fundamentals of Qualitative Research; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Dresing, T.; Pehl, T. Praxisbuch Interview, Transkription & Analyse; dr Dresing & Pehl GmbH: Marburg, Germany, 2015. [Google Scholar]
- Cohen, J.; Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar]
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide; SAGE Publications, Inc.: London, UK, 2022. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Flick, U. Design and Process in Qualitative Research. In A Companion to Qualitative Research; Flick, U., Kardorff, E.V., Steinke, I., Eds.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2004; pp. 146–152. [Google Scholar]
- Flick, U. Managing quality in qualitative research. In The SAGE Qualitative Research Kit, 2nd ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Silva, A.; de Queiroz, S.S.; Andersen, M.L.; Mônico-Neto, M.; da Silveira Campos, R.M.; Roizenblatt, S.; Tufik, S.; de Mello, M.T. Passive body heating improves sleep patterns in female patients with fibromyalgia. Clinics 2013, 68, 135–139. [Google Scholar] [CrossRef]


{kind=link}
| Patients | Interview (Yes = 1, No = 0) a | Pain Intensity W0 a | Pain Intensity W12 a | Change in Pain Intensity [%] a,c | Duration PlatP Mean All Sessions [Minutes] a | Experience of the Intervention (Mainly) b | Perception of Pain Reduction b | Duration of Pain Reduction b |
|---|---|---|---|---|---|---|---|---|
| 1 | 1 | 5.3 | 5.3 | 0.0 | 15.0 | Positive | Yes | Medium |
| 2 | 1 | 4.6 | 2.8 | −40.6 | 17.0 | Mixed | Yes | Long |
| 3 | 1 | 6.5 | 2.0 | −69.2 | 23.3 | Positive | Yes | Long |
| 4 | 1 | 4.3 | 5.3 | 23.5 | 21.0 | Negative | Yes | Medium |
| 5 | 1 | 2.0 | 2.5 | 25.0 | 10.8 | Positive | Yes | Medium |
| 6 | 1 | 4.5 | 3.0 | −33.3 | 18.5 | Mixed | Yes | Medium |
| 7 | 1 | 6.8 | 7.0 | 3.7 | 4.0 | Negative | Yes | Medium |
| 8 | 1 | 7.0 | 5.5 | −21.4 | 9.8 | Negative | Yes | Medium |
| 9 | 1 | 7.0 | 6.4 | −8.9 | 22.0 | Positive | Yes | Short |
| 10 | 1 | 4.8 | 4.3 | −10.5 | 3.0 | Negative | Yes | Short |
| 11 | 0 | 5.0 | 3.6 | −28.6 | 7.5 | n.a. | n.a. | n.a. |
| 12 | 0 | 5.8 | 4.0 | −30.4 | 12.2 | n.a. | n.a. | n.a. |
| 13 | 0 | 4.3 | 1.8 | −58.8 | 24.8 | n.a. | n.a. | n.a. |
| 14 | 0 | 5.8 | 3.0 | −47.8 | 12.7 | n.a. | n.a. | n.a. |
| 15 | 0 | 4.8 | 2.3 | −52.6 | 21.2 | n.a. | n.a. | n.a. |
| 16 | 0 | 4.8 | 4.5 | −5.3 | 20.0 | n.a. | n.a. | n.a. |
| 17 | 0 | 5.3 | 5.3 | 0.0 | 13.5 | n.a. | n.a. | n.a. |
| 18 | 0 | 7.0 | 4.5 | −35.7 | 19.7 | n.a. | n.a. | n.a. |
| 19 | 0 | 7.3 | 6.3 | −13.8 | 5.0 | n.a. | n.a. | n.a. |
| 20 | 0 | 8.3 | 9.0 | 9.1 | 12.7 | n.a. | n.a. | n.a. |
| Mean total | n.a. | 5.5 | 4.4 | −19.8 | 14.7 | n.a. | n.a. | n.a. |
| Mean interview group | n.a. | 5.3 | 4.4 | −13.2 | 14.4 | n.a. | n.a. | n.a. |
| Statistical difference (t-tests) | n.a. | p = 0.644 | p = 0.989 | p = 0.539 | p = 0.930 | n.a. | n.a. | n.a. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Öznur, Ö.; Schlee, C.; Utz, S.; Langhorst, J. Investigating the Influential Factors of Mild Water-Filtered Infrared-A Whole-Body Hyperthermia for Pain Relief in Fibromyalgia: A Mixed-Methods Approach Focusing on Predictors and Patient Perspectives. Biomedicines 2023, 11, 2949. https://doi.org/10.3390/biomedicines11112949
Öznur Ö, Schlee C, Utz S, Langhorst J. Investigating the Influential Factors of Mild Water-Filtered Infrared-A Whole-Body Hyperthermia for Pain Relief in Fibromyalgia: A Mixed-Methods Approach Focusing on Predictors and Patient Perspectives. Biomedicines. 2023; 11(11):2949. https://doi.org/10.3390/biomedicines11112949
Chicago/Turabian StyleÖznur, Özlem, Christoph Schlee, Sandra Utz, and Jost Langhorst. 2023. "Investigating the Influential Factors of Mild Water-Filtered Infrared-A Whole-Body Hyperthermia for Pain Relief in Fibromyalgia: A Mixed-Methods Approach Focusing on Predictors and Patient Perspectives" Biomedicines 11, no. 11: 2949. https://doi.org/10.3390/biomedicines11112949