
FIB-4 Index and Neutrophil-to-Lymphocyte-Ratio as Death Predictor in Coronary Artery Disease Patients
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Characteristics of the Study Population
2.2. Blood Sampling
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Studied Population
3.2. Spearman’s Rank Correlation between NLR and FIB-4 and the Variables Included in the Calculation of the Two Indexes
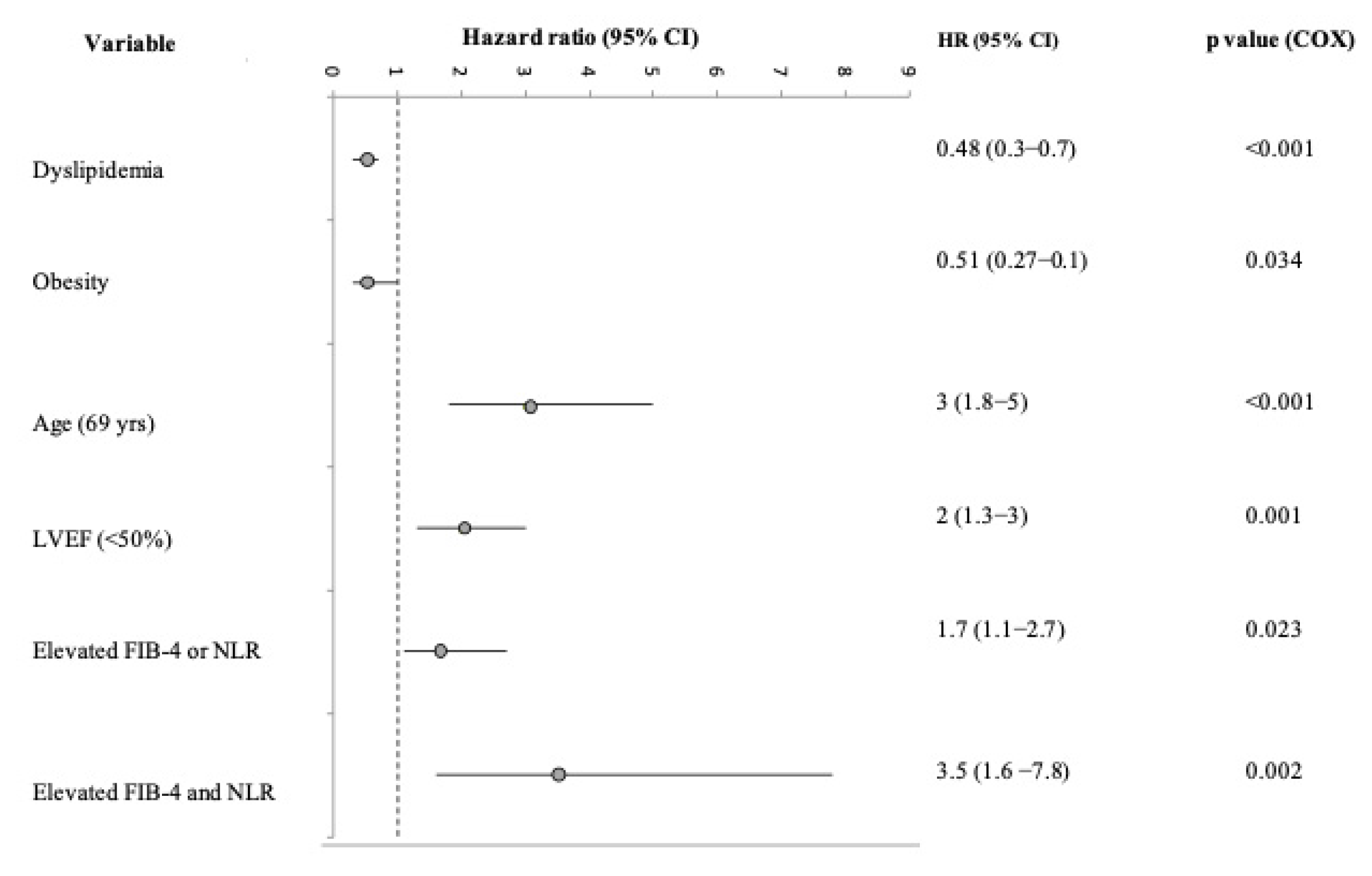
3.3. Unadjusted and Adjusted Logistic Analysis
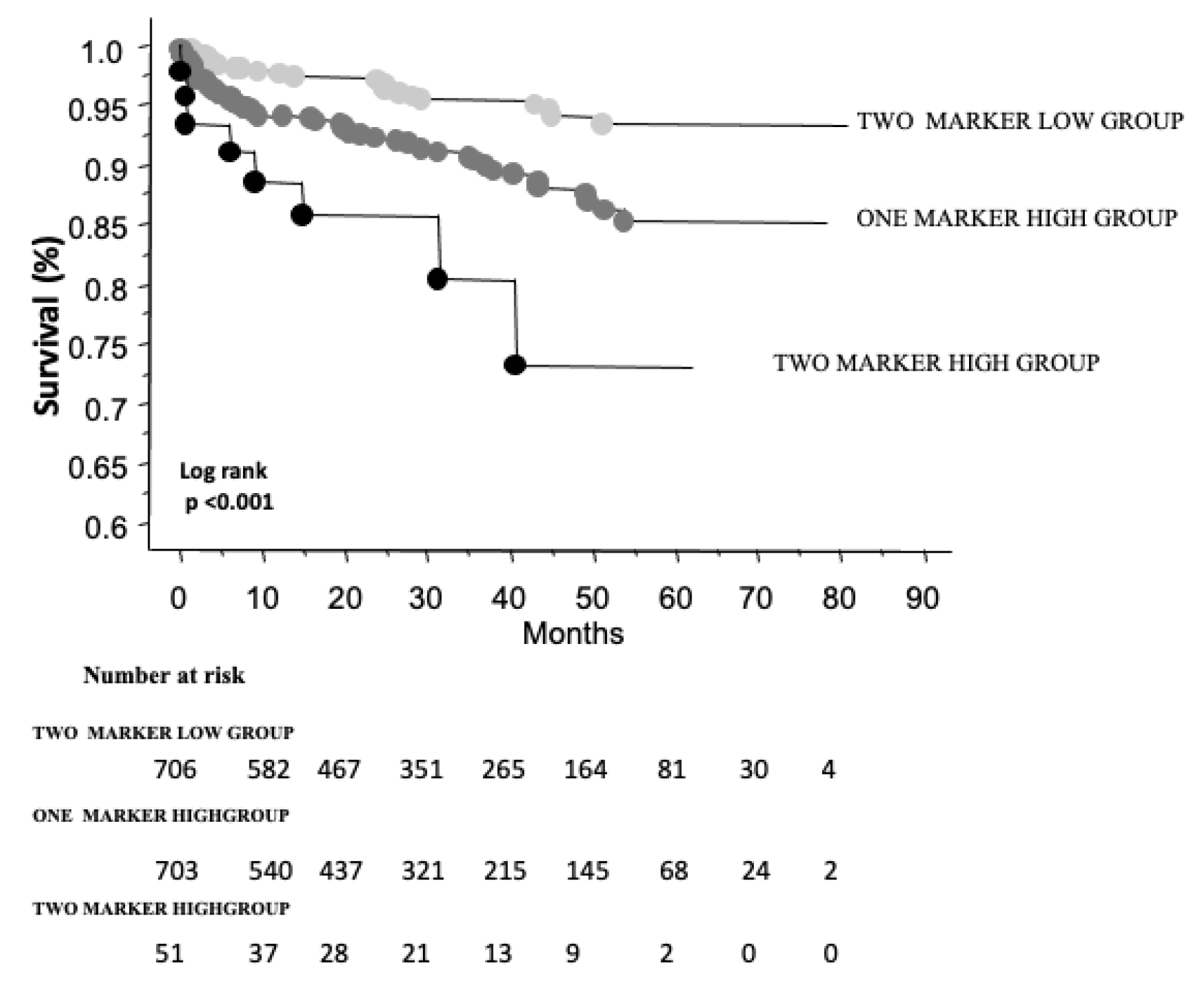
3.4. Follow-Up
4. Discussion
5. Study Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ross, R. Atherosclerosis is an inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Alon, L.; Corica, B.; Raparelli, V.; Cangemi, R.; Basili, S.; Proietti, M.; Romiti, G.F. Risk of cardiovascular events in patients with non-alcoholic fatty liver disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2021, 29, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Wu, W.; Wen, W.; Xu, F.; Han, D.; Lyu, J.; Huang, Y. Association of NAFLD with cardiovascular disease and all-cause mortality: A large-scale prospective cohort study based on UK Biobank. Ther. Adv. Chronic Dis. 2022, 13, 20406223221122478. [Google Scholar] [CrossRef] [PubMed]
- Kahan, T.; Forslund, L.; Held, C.; Björkander, I.; Billing, E.; Eriksson, S.V.; Näsman, P.; Rehnqvist, N.; Hjemdahl, P. Risk prediction in stable angina pectoris. Eur. J. Clin. Investig. 2012, 43, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Baratta, F.; Pastori, D.; Angelico, F.; Balla, A.; Paganini, A.M.; Cocomello, N.; Ferro, D.; Violi, F.; Sanyal, A.J.; Del Ben, M. Nonalcoholic Fatty Liver Disease and Fibrosis Associated With Increased Risk of Cardiovascular Events in a Prospective Study. Clin. Gastroenterol. Hepatol. 2020, 18, 2324–2331.e4. [Google Scholar] [CrossRef]
- Bäck, M.; Yurdagul, A., Jr.; Tabas, I.; Öörni, K.; Kovanen, P.T. Inflammation and its resolution in atherosclerosis: Mediators and therapeutic opportunities. Nat. Rev. Cardiol. 2019, 16, 389–406. [Google Scholar] [CrossRef]
- Stahl, E.P.; Dhindsa, D.S.; Lee, S.K.; Sandesara, P.B.; Chalasani, N.P.; Sperling, L.S. Nonalcoholic Fatty Liver Disease and the Heart: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 948–963. [Google Scholar] [CrossRef]
- Ma, J.; Li, H. The Role of Gut Microbiota in Atherosclerosis and Hypertension. Front. Pharmacol. 2018, 9, 1082. [Google Scholar] [CrossRef]
- Brouwers, M.C.; Simons, N.; Stehouwer, C.D.; Koek, G.H.; Schaper, N.; Isaacs, A. Relationship Between Nonalcoholic Fatty Liver Disease Susceptibility Genes and Coronary Artery Disease. Hepatol. Commun. 2019, 3, 587–596. [Google Scholar] [CrossRef]
- Balta, S. Mean Platelet Volume, Neutrophil–Lymphocyte Ratio, and Long-Term Major Cardiovascular Events. Angiology 2018, 70, 289–290. [Google Scholar] [CrossRef]
- Balta, S.; Celik, T.; Mikhailidis, D.P.; Ozturk, C.; Demirkol, S.; Aparci, M.; Iyisoy, A. The Relation Between Atherosclerosis and the Neutrophil–Lymphocyte Ratio. Clin. Appl. Thromb. 2015, 22, 405–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Turco, S.; Basta, G.; De Caterina, A.R.; Sbrana, S.; Paradossi, U.; Taddei, A.; Trianni, G.; Ravani, M.; Palmieri, C.; Berti, S.; et al. Different inflammatory profile in young and elderly STEMI patients undergoing primary percutaneous coronary intervention (PPCI): Its influence on no-reflow and mortality. Int. J. Cardiol. 2019, 290, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Del Turco, S.; Bastiani, L.; Minichilli, F.; Landi, P.; Basta, G.; Pingitore, A.; Vassalle, C. Interaction of Uric Acid and Neutrophil-to-Lymphocyte Ratio for Cardiometabolic Risk Stratification and Prognosis in Coronary Artery Disease Patients. Antioxidants 2022, 11, 2163. [Google Scholar] [CrossRef]
- Lucijanic, M.; Cicic, D.; Stoos-Veic, T.; Pejsa, V.; Lucijanic, J.; Dzankic, A.F.; Glasnovic, J.V.; Soric, E.; Skelin, M.; Kusec, R. Elevated Neutrophil–to–Lymphocyte-ratio and Platelet–to–Lymphocyte Ratio in Myelofibrosis: Inflammatory Biomarkers or Representatives of Myeloproliferation Itself? Anticancer Res. 2018, 38, 3157–3163. [Google Scholar] [CrossRef]
- Krečak, I.; Holik, H.; Perić, M.M.; Zekanović, I.; Coha, B.; Krečak, M.V.; Gverić-Krečak, V.; Lucijanić, M. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as prognostic biomarkers in polycythemia vera. Int. J. Lab. Hematol. 2022, 44, e145–e148. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Morrow, D.A.; de Lemos, J.A.; Gibson, C.M.; Murphy, S.A.; Rifai, N.; McCabe, C.; Antman, E.M.; Cannon, C.P.; Braunwald, E. Multimarker Approach to Risk Stratification in Non-ST Elevation Acute Coronary Syndromes. Circulation 2002, 105, 1760–1763. [Google Scholar] [CrossRef] [Green Version]
- Goriki, Y.; Tanaka, A.; Nishihira, K.; Kawaguchi, A.; Natsuaki, M.; Watanabe, N.; Ashikaga, K.; Kuriyama, N.; Shibata, Y.; Node, K. A Novel Predictive Model for In-Hospital Mortality Based on a Combination of Multiple Blood Variables in Patients with ST-Segment-Elevation Myocardial Infarction. J. Clin. Med. 2020, 9, 852. [Google Scholar] [CrossRef] [Green Version]
- Goriki, Y.; Yoshioka, G.; Natsuaki, M.; Shinzato, K.; Nishihira, K.; Kuriyama, N.; Shimomura, M.; Inoue, Y.; Nishikido, T.; Kaneko, T.; et al. Simple risk-score model for in-hospital major bleeding based on multiple blood variables in patients with acute myocardial infarction. Int. J. Cardiol. 2021, 346, 1–7. [Google Scholar] [CrossRef]
- Traxler, D.; Zimmermann, M.; Simader, E.; Veraar, C.M.; Moser, B.; Mueller, T.; Mildner, M.; Dannenberg, V.; Lainscak, M.; Jug, B.; et al. The inflammatory markers sST2, HSP27 and hsCRP as a prognostic biomarker panel in chronic heart failure patients. Clin. Chim. Acta 2020, 510, 507–514. [Google Scholar] [CrossRef]
- Vassalle, C. New biomarkers and traditional cardiovascular risk scores: Any crystal ball for current effective advice and future exact prediction? Clin. Chem. Lab. Med. 2018, 56, 1803–1805. [Google Scholar] [CrossRef]
- Vassalle, C.; Chatzianagnostou, K.; Vannucci, A.; Guiducci, L.; Battaglia, D.; Maffei, S.; Arvia, C.; Landi, P.; Carpeggiani, C. Gender differences for uric acid as predictor of hard events in patients referred for coronary angiography. Biomarkers Med. 2016, 10, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Michelucci, E.; Rocchiccioli, S.; Gaggini, M.; Ndreu, R.; Berti, S.; Vassalle, C. Ceramides and Cardiovascular Risk Factors, Inflammatory Parameters and Left Ventricular Function in AMI Patients. Biomedicines 2022, 10, 429. [Google Scholar] [CrossRef]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Zhou, R.; Li, H.; Zhao, X.; Sun, Y.; Fan, Y.; Zhang, S. Alterations of Gut Microbiome and Serum Metabolome in Coronary Artery Disease Patients Complicated With Non-alcoholic Fatty Liver Disease Are Associated With Adverse Cardiovascular Outcomes. Front. Cardiovasc. Med. 2022, 8, 805812. [Google Scholar] [CrossRef] [PubMed]
- Arslan, U.; Yenerçağ, M. Relationship between non-alcoholic fatty liver disease and coronary heart disease. World J. Clin. Cases 2020, 8, 4688–4699. [Google Scholar] [CrossRef] [PubMed]
- Toh, J.Z.K.; Pan, X.-H.; Tay, P.W.L.; Ng, C.H.; Yong, J.N.; Xiao, J.; Koh, J.H.; Tan, E.Y.; Tan, E.X.X.; Dan, Y.Y.; et al. A Meta-Analysis on the Global Prevalence, Risk factors and Screening of Coronary Heart Disease in Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2021, 20, 2462–2473.e10. [Google Scholar] [CrossRef]
- Bae, Y.S.; Ko, Y.S.; Yun, J.M.; Eo, A.Y.; Kim, H. Association and Prediction of Subclinical Atherosclerosis by Nonalcoholic Fatty Liver Disease in Asymptomatic Patients. Can. J. Gastroenterol. Hepatol. 2020, 2020, 8820445. [Google Scholar] [CrossRef]
- Wu, S.; Wu, F.; Ding, Y.; Hou, J.; Bi, J.; Zhang, Z. Association of non-alcoholic fatty liver disease with major adverse cardiovascular events: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 33386. [Google Scholar] [CrossRef] [Green Version]
- Hsu, P.; Wang, Y.; Lin, C.; Wang, Y.; Ding, Y.; Liou, T.; Huang, S.; Lu, T.; Chan, W.; Lin, S.; et al. The association of the steatosis severity in fatty liver disease with coronary plaque pattern in general population. Liver Int. 2020, 41, 81–90. [Google Scholar] [CrossRef]
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef]
- Mantovani, A.; Csermely, A.; Petracca, G.; Beatrice, G.; Corey, K.E.; Simon, T.G.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: An updated systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 903–913. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhong, G.-C.; Tan, H.-Y.; Hao, F.-B.; Hu, J.-J. Nonalcoholic fatty liver disease and mortality from all causes, cardiovascular disease, and cancer: A meta-analysis. Sci. Rep. 2019, 9, 11124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saokaew, S.; Kanchanasurakit, S.; Thawichai, K.; Duangprom, P.; Wannasri, M.; Khankham, S.; Kositamongkol, C.; Chaiyakunapruk, N.; Phisalprapa, P. Association of non-alcoholic fatty liver disease and all-cause mortality in hospitalized cardiovascular disease patients: A systematic review and meta-analysis. Medicine 2021, 100, e24557. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Ghany, M.G.; Morgan, T.R.; Panel, A.H.C.G.; Marks, K.M.; Wyles, D.L.; Aronsohn, A.I.; Bhattacharya, D.; Broder, T.; Falade-Nwulia, O.O.; Feld, J.J.; et al. Hepatitis C Guidance 2019 Update: American Association for the Study of Liver Diseases–Infectious Diseases Society of America Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection. Hepatology 2019, 71, 686–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guidelines for the Screening Care and Treatment of Persons with Chronic Hepatitis C Infection: Updated Version; World Health Organization: Geneva, Switzerland, 2016. Available online: https://pubmed.ncbi.nlm.nih.gov/27227200/ (accessed on 1 December 2022).
- Hagström, H.; Talbäck, M.; Andreasson, A.; Walldius, G.; Hammar, N. Repeated FIB-4 measurements can help identify individuals at risk of severe liver disease. J. Hepatol. 2020, 73, 1023–1029. [Google Scholar] [CrossRef]
- Berzigotti, A.; Tsochatzis, E.; Boursier, J.; Castera, L.; Cazzagon, N.; Friedrich-Rust, M.; Petta, S.; Thiele, M. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis—2021 update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef]
- Yan, Z.; Liu, Y.; Li, W.; Zhao, X.; Lin, W.; Zhang, J.; Yu, S.; Ma, J.; Wang, J.; Yu, P.; et al. Liver fibrosis scores and prognosis in patients with cardiovascular diseases: A system-atic review and meta-analysis. Eur. J. Clin. Invest. 2022, 52, e13855. [Google Scholar] [CrossRef]
- Majnarić, L.T.; Guljaš, S.; Bosnić, Z.; Šerić, V.; Wittlinger, T. Neutrophil-to-Lymphocyte Ratio as a Cardiovascular Risk Marker May Be Less Efficient in Women Than in Men. Biomolecules 2021, 11, 528. [Google Scholar] [CrossRef]
- Ikeda, U.; Ikeda, M.; Oohara, T.; Kano, S.; Yaginuma, T. Mitogenic action of interleukin-1α on vascular smooth muscle cells mediated by PDGF. Atherosclerosis 1990, 84, 183–188. [Google Scholar] [CrossRef]
- Simpson, E.; Cantor, H. Regulation of the immune response by subclasses of T lymphocytes. II. The effect of adult thymectomy upon humoral and cellular responses in mice. Eur. J. Immunol. 1975, 5, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Moghanjoughi, P.H.; Neshat, S.; Rezaei, A.; Heshmat-Ghahdarijani, K. Is the Neutrophil-to-Lymphocyte Ratio an Exceptional Indicator for Metabolic Syndrome Disease and Outcomes? Endocr. Pract. 2022, 28, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Mannarino, M.R.; Bianconi, V.; Gigante, B.; Strawbridge, R.J.; Savonen, K.; Kurl, S.; Giral, P.; Smit, A.; Eriksson, P.; Tremoli, E.; et al. Neutrophil to lymphocyte ratio is not related to carotid atherosclerosis progression and cardiovascular events in the primary prevention of cardiovascular disease: Results from the IMPROVE study. BioFactors 2021, 48, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Dentali, F.; Nigro, O.; Squizzato, A.; Gianni, M.; Zuretti, F.; Grandi, A.M.; Guasti, L. Impact of neutrophils to lymphocytes ratio on major clinical outcomes in patients with acute coronary syndromes: A systematic review and meta-analysis of the literature. Int. J. Cardiol. 2018, 266, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Chen, M.-H.; Li, S.; Guo, Y.-L.; Zhu, C.-G.; Xu, R.-X.; Zhang, Y.; Sun, J.; Qing, P.; Liu, G.; et al. Usefulness of the Neutrophil-to-Lymphocyte Ratio in Predicting the Severity of Coronary Artery Disease: A Gensini Score Assessment. J. Atheroscler. Thromb. 2014, 21, 1271–1282. [Google Scholar] [CrossRef] [Green Version]
- Ding, R.; Zhou, X.; Huang, D.; Wang, Y.; Li, X.; Yan, L.; Lu, W.; Yang, Z.; Zhang, Z. Predictive Performances of Blood Parameter Ratios for Liver Inflammation and Advanced Liver Fibrosis in Chronic Hepatitis B Infection. BioMed Res. Int. 2021, 2021, 6644855. [Google Scholar] [CrossRef]
- Chen, L.-Z.; Jing, X.-B.; Wu, C.-F.; Zeng, Y.-C.; Xie, Y.-C.; Wang, M.-Q.; Chen, W.-X.; Hu, X.; Zhou, Y.-N.; Cai, X.-B. Nonalcoholic Fatty Liver Disease-Associated Liver Fibrosis Is Linked with the Severity of Coronary Artery Disease Mediated by Systemic Inflammation. Dis. Markers 2021, 2021, 6591784. [Google Scholar] [CrossRef]
- Arbel, Y.; Shacham, Y.; Ziv-Baran, T.; Perl, M.L.; Finkelstein, A.; Halkin, A.; Revivo, M.; Milwidsky, A.; Berliner, S.; Herz, I.; et al. Higher Neutrophil/Lymphocyte Ratio Is Related to Lower Ejection Fraction and Higher Long-term All-Cause Mortality in ST-Elevation Myocardial Infarction Patients. Can. J. Cardiol. 2014, 30, 1177–1182. [Google Scholar] [CrossRef]
- Kotani, K. Neutrophil/Lymphocyte Ratio and the Oxidative Stress Burden. Can. J. Cardiol. 2015, 31, 365.e9. [Google Scholar] [CrossRef]
- Pilotto, A.; Gallina, P.; Panza, F.; Copetti, M.; Cella, A.; Cruz-Jentoft, A.; Daragjati, J.; Ferrucci, L.; Maggi, S.; Mattace-Raso, F.; et al. Relation of Statin Use and Mortality in Community-Dwelling Frail Older Patients With Coronary Artery Disease. Am. J. Cardiol. 2016, 118, 1624–1630. [Google Scholar] [CrossRef]
- Hwang, I.-C.; Jeon, J.-Y.; Kim, Y.; Kim, H.M.; Yoon, Y.E.; Lee, S.-P.; Kim, H.-K.; Sohn, D.-W.; Sung, J.; Kim, Y.-J. Statin therapy is associated with lower all-cause mortality in patients with non-obstructive coronary artery disease. Atherosclerosis 2015, 239, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, T.; Iwade, K.; Hirata, N.; Yamashita, M.; Ikegami, H.; Tanaka, N.; Aosaki, M.; Kasanuki, H. Improvement of arterial stiffness by the antioxidant and anti-inflammatory effects of short-term statin therapy in patients with hypercholesterolemia. Hear. Vessel. 2005, 20, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Dobrucki, L.W.; Kalinowski, L.; Dobrucki, I.T.; Malinski, T. Statin-stimulated nitric oxide release from endothelium. J. Pharmacol. Exp. Ther. 2001, 7, 622–627. [Google Scholar]
- Tutor, A.W.; Lavie, C.J.; Kachur, S.; Milani, R.V.; Ventura, H.O. Updates on obesity and the obesity paradox in cardiovascular diseases. Prog. Cardiovasc. Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Ha, E.E.; Bauer, R.C. Emerging Roles for Adipose Tissue in Cardiovascular Disease. Arter. Thromb. Vasc. Biol. 2018, 38, e137–e144. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | FIB-4 | NLR | ||||
|---|---|---|---|---|---|---|
| ≤3.25 | >3.25 | p | ≤2.04 | >2.04 | p | |
| n = 1385 | n = 75 | n = 730 | n = 730 | |||
| Age (years) | 68 ± 10 | 74 ± 9 | <0.001 | 67 ± 9 | 69 ± 10 | <0.001 |
| Age (<69 years) | 700 (50) | 55 (73) | <0.001 | 336 (46) | 419 (57) | <0.001 |
| Male sex | 1097 (79) | 54 (72) | ns | 582 (51) | 569 (49) | ns |
| Body mass index (kg/m2) (n = 1429) | 27 ± 4 | 27 ± 4 | ns | 28 ± 4 | 27 ± 4 | 0.014 |
| Obesity | 306 (22) | 20 (27) | ns | 173 (24) | 153 (24) | ns |
| Hypertension | 831 (60) | 42 (56) | ns | 442 (61) | 431 (59) | ns |
| Diabetes | 431 (31) | 31 (41) | ns | 225 (31) | 237(32) | ns |
| Dyslipidemia/lipid-lowering drugs | 1172 (85) | 56 (75) | 0.022 | 638 (87) | 590 (81) | <0.001 |
| Smoking habit (current/former smokers) | 646 (47) | 30 (40) | ns | 341 (47) | 335 (46) | ns |
| LVEF (%) (n = 1448) | 52 ± 11 | 48 ± 12 | <0.001 | 53 ± 10 | 50 ± 4 | <0.0001 |
| LVEF (<50%) | 368 (26) | 29 (39) | <0.22 | 154 (21) | 243 (33) | <0.001 |
| Multivessel disease | 847 (61) | 54 (72) | ns | 434 (59) | 467 (64) | ns |
| FIB-4 | - | - | - | 1.54 ± 0.76 | 1.88 ± 1.85 | <0.001 |
| FIB-4 (>3.25) | - | - | - | 24 (3) | 51 (7) | 0.0014 |
| NLR | 2.57 ± 2.4 | 4.9 ± 5.39 | <0.001 | - | - | - |
| NLR (>2.04) | 679 (49) | 51 (68) | 0.0014 | - | - | - |
| Parameter | Mortality | ||
|---|---|---|---|
| Hazard Ratio | 95% CI | p | |
| Age (years) | 1.08 | 1.05–1.11 | <0.001 |
| Age (<69 years) | 3.7 | 2.3–6.1 | <0.001 |
| Male sex | 0.96 | 0.6–1.6 | ns |
| Body mass index (kg/m2) (n = 1429) | 0.87 | 0.8–0.9 | <0.001 |
| Obesity | 0.46 | 0.24–0.86 | 0.015 |
| Hypertension | 0.85 | 0.6–1.3 | ns |
| Diabetes | 1.13 | 0.7–1.7 | ns |
| Dyslipidemia/lipid-lowering drugs | 0.35 | 0.22–0.53 | <0.001 |
| Smoking habit (current/former smokers) | 1.1 | 0.7–1.7 | ns |
| LVEF (n = 1448) | 0.96 | 0.94–0.97 | <0.001 |
| LVEF (<50%) | 2.4 | 1.6–3.7 | <0.001 |
| Multivessel disease | 1.4 | 1–2.1 | ns |
| FIB-4 | 1.13 | 1.05–1.22 | 0.0011 |
| FIB-4 (>3.25) | 2.35 | 1.22–4.52 | 0.011 |
| NLR | 1.1 | 1.1–1.2 | <0.001 |
| NLR (>2.04) | 2.4 | 1.6–3.8 | <0.001 |
| One marker high group | 2.4 | 1.5–3.7 | <0.001 |
| Two marker high group | 5 | 2.3–11 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaggini, M.; Minichilli, F.; Gorini, F.; Del Turco, S.; Landi, P.; Pingitore, A.; Vassalle, C. FIB-4 Index and Neutrophil-to-Lymphocyte-Ratio as Death Predictor in Coronary Artery Disease Patients. Biomedicines 2023, 11, 76. https://doi.org/10.3390/biomedicines11010076
Gaggini M, Minichilli F, Gorini F, Del Turco S, Landi P, Pingitore A, Vassalle C. FIB-4 Index and Neutrophil-to-Lymphocyte-Ratio as Death Predictor in Coronary Artery Disease Patients. Biomedicines. 2023; 11(1):76. https://doi.org/10.3390/biomedicines11010076
Chicago/Turabian StyleGaggini, Melania, Fabrizio Minichilli, Francesca Gorini, Serena Del Turco, Patrizia Landi, Alessandro Pingitore, and Cristina Vassalle. 2023. "FIB-4 Index and Neutrophil-to-Lymphocyte-Ratio as Death Predictor in Coronary Artery Disease Patients" Biomedicines 11, no. 1: 76. https://doi.org/10.3390/biomedicines11010076