
Extracorporeal Carbon Dioxide Removal: From Pathophysiology to Clinical Applications; Focus on Combined Continuous Renal Replacement Therapy

 , , and
, , and
Abstract
:1. Introduction
2. Carbon Dioxide and Acid–Base Balance
3. ECCO2R: Principles
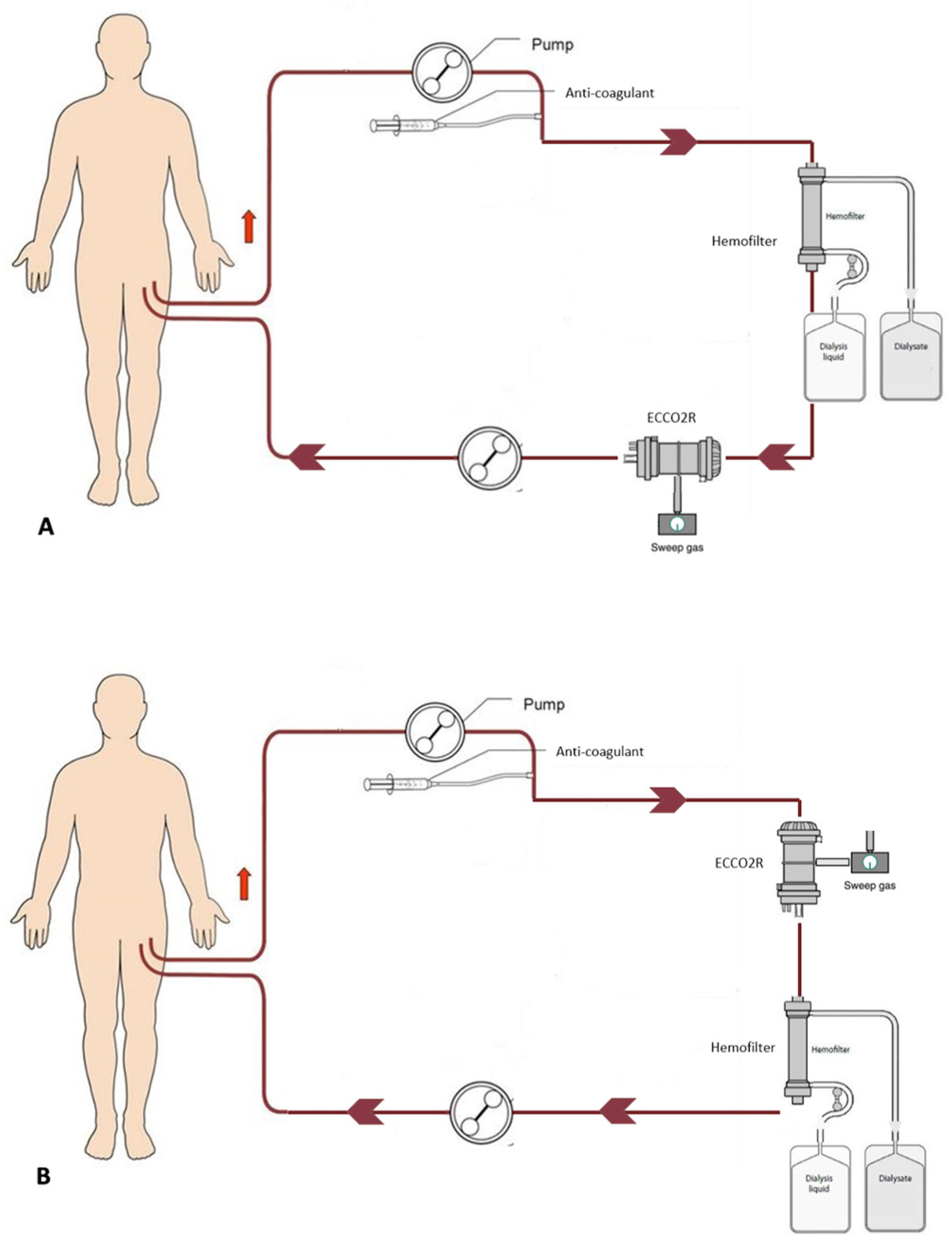
3.1. Principles and Systems
3.2. Anticoagulation
3.3. Complications
4. ECCO2R: Clinical Applications
4.1. ECCO2R in COPD
4.2. ECCO2R in ARDS
5. Respiratory and Renal Failure: A Dangerous Interconnection
6. Experiences with ECCO2R Integrated into CRRT Platforms
Experiences with ECCO2R Integrated into CRRT Platform in COVID-19 Patients
7. Critical Considerations
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roussos, C.; Koutsoukou, A. Respiratory Failure. Eur. Respir. J. Suppl. 2003, 47, 3s–14s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shekar, K.; Mullany, D.V.; Thomson, B.; Ziegenfuss, M.; Platts, D.G.; Fraser, J.F. Extracorporeal Life Support Devices and Strategies for Management of Acute Cardiorespiratory Failure in Adult Patients: A Comprehensive Review. Crit. Care 2014, 18, 219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camporota, L.; Barrett, N. Current Applications for the Use of Extracorporeal Carbon Dioxide Removal in Critically Ill Patients. BioMed Res. Int. 2016, 2016, 9781695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, J.; Cooper, J.S. Physiology, Carbon Dioxide Transport; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Ronco, C.; Bellomo, R.; Kellum, J.A.; Ricci, Z. Critical Care Nephrology; Elsevier Health Sciences: Amsterdam, The Netherlands, 2019; ISBN 9780323449427. [Google Scholar]
- Boyle MBChB, A.J.; McNamee FCICM, J.J.; McAuley, D.F.; Boyle, A.J.; McNamee, J.J.; Boyle, A.J.; Sklar, M.C.; McNamee, J.J.; Brodie, D.; Slutsky, A.S.; et al. Extracorporeal Carbon Dioxide Removal for Lowering the Risk of Mechanical Ventilation: Research Questions and Clinical Potential for the Future. Lancet Respir. Med. 2018, 6, 874–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- May, A.G.; Omecinski, K.S.; Frankowski, B.J.; Federspiel, W.J. Effect of Hematocrit on the CO2 Removal Rate of Artificial Lungs. ASAIO J. 2020, 66, 1161–1165. [Google Scholar] [CrossRef]
- Yu, T.Z.; Tatum, R.T.; Saxena, A.; Ahmad, D.; Yost, C.C.; Maynes, E.J.; O’Malley, T.J.; Massey, H.T.; Swol, J.; Whitson, B.A.; et al. Utilization and Outcomes of Extracorporeal CO2 Removal (ECCO2R): Systematic Review and Meta-Analysis of Arterio-Venous and Veno-Venous ECCO2R Approaches. Artif. Organs 2022, 46, 763–774. [Google Scholar] [CrossRef]
- Giraud, R.; Banfi, C.; Assouline, B.; de Charrière, A.; Cecconi, M.; Bendjelid, K. The Use of Extracorporeal CO2 Removal in Acute Respiratory Failure. Ann. Intensive Care 2021, 11, 43. [Google Scholar] [CrossRef]
- Morales-Quinteros, L.; Del Sorbo, L.; Artigas, A. Extracorporeal Carbon Dioxide Removal for Acute Hypercapnic Respiratory Failure. Ann. Intensive Care 2019, 9, 79. [Google Scholar] [CrossRef]
- Terragni, P.P.; Birocco, A.; Faggiano, C.; Ranieri, V.M. Extracorporeal CO2; Removal. In Cardiorenal Syndromes in Critical Care; Karger Publishers: Basel, Switzerland, 2010; Volume 165, pp. 185–196. ISBN 978-3-8055-9472-1. [Google Scholar]
- Terragni, P.; Maiolo, G.; Ranieri, V.M. Role and Potentials of Low-Flow CO(2) Removal System in Mechanical Ventilation. Curr. Opin. Crit. Care 2012, 18, 93–98. [Google Scholar] [CrossRef]
- Del Sorbo, L.; Cypel, M.; Fan, E. Extracorporeal Life Support for Adults with Severe Acute Respiratory Failure. Lancet Respir. Med. 2014, 2, 154–164. [Google Scholar] [CrossRef]
- Ficial, B.; Vasques, F.; Zhang, J.; Whebell, S.; Slattery, M.; Lamas, T.; Daly, K.; Agnew, N.; Camporota, L. Physiological Basis of Extracorporeal Membrane Oxygenation and Extracorporeal Carbon Dioxide Removal in Respiratory Failure. Membranes 2021, 11, 225. [Google Scholar] [CrossRef]
- Barrett, N.A.; Hart, N.; Camporota, L. In Vivo Carbon Dioxide Clearance of a Low-Flow Extracorporeal Carbon Dioxide Removal Circuit in Patients with Acute Exacerbations of Chronic Obstructive Pulmonary Disease. Perfusion 2020, 35, 436–441. [Google Scholar] [CrossRef]
- Arazawa, D.T.; Kimmel, J.D.; Finn, M.C.; Federspiel, W.J. Acidic Sweep Gas with Carbonic Anhydrase Coated Hollow Fiber Membranes Synergistically Accelerates CO2 Removal from Blood. Acta Biomater. 2015, 25, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Menajovsky, L.B. Heparin-Induced Thrombocytopenia: Clinical Manifestations and Management Strategies. Am. J. Med. 2005, 118 (Suppl. 8A), 21S–30S. [Google Scholar] [CrossRef]
- Tolwani, A.; Wille, K.M. Advances in Continuous Renal Replacement Therapy: Citrate Anticoagulation Update. Blood Purif. 2012, 34, 88–93. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; Laupland, K.B.; Boiteau, P.J.E.; Godinez-Luna, T. Is Regional Citrate Superior to Systemic Heparin Anticoagulation for Continuous Renal Replacement Therapy? A Prospective Observational Study in an Adult Regional Critical Care System. J. Crit. Care 2005, 20, 155–161. [Google Scholar] [CrossRef]
- Sharma, A.S.; Weerwind, P.W.; Bekers, O.; Wouters, E.M.; Maessen, J.G. Carbon Dioxide Dialysis in a Swine Model Utilizing Systemic and Regional Anticoagulation. Intensive Care Med. Exp. 2016, 4, 2. [Google Scholar] [CrossRef] [Green Version]
- Sklar, M.C.; Beloncle, F.; Katsios, C.M.; Brochard, L.; Friedrich, J.O. Extracorporeal Carbon Dioxide Removal in Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review. Intensive Care Med. 2015, 41, 1752–1762. [Google Scholar] [CrossRef]
- Cove, M.E.; MacLaren, G.; Federspiel, W.J.; Kellum, J.A. Bench to Bedside Review: Extracorporeal Carbon Dioxide Removal, Past Present and Future. Crit. Care 2012, 16, 232. [Google Scholar] [CrossRef] [Green Version]
- Azzi, M.; Aboab, J.; Alviset, S.; Ushmorova, D.; Ferreira, L.; Ioos, V.; Memain, N.; Issoufaly, T.; Lermuzeaux, M.; Laine, L.; et al. Extracorporeal CO2removal in Acute Exacerbation of COPD Unresponsive to Non-Invasive Ventilation. BMJ Open Respir. Res. 2021, 8, e001089. [Google Scholar] [CrossRef]
- Ricard, J.D.; Dreyfuss, D.; Saumon, G. Ventilator-Induced Lung Injury. Eur. Respir. J. Suppl. 2003, 42, 2s–9s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, E.; Brodie, D.; Slutsky, A.S. Acute Respiratory Distress Syndrome. JAMA 2018, 319, 698. [Google Scholar] [CrossRef] [PubMed]
- Tiruvoipati, R.; Pilcher, D.; Buscher, H.; Botha, J.; Bailey, M. Effects of Hypercapnia and Hypercapnic Acidosis on Hospital Mortality in Mechanically Ventilated Patients*. Crit. Care Med. 2017, 45, e649–e656. [Google Scholar] [CrossRef] [PubMed]
- İnal, V.; Efe, S. Extracorporeal Carbon Dioxide Removal (Ecco2r) in Copd and Ards Patients with Severe Hypercapnic Respiratory Failure. a Retrospective Case-Control Study. Turk. J. Med. Sci. 2021, 51, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- Dave, C.; Wharton, S.; Mukherjee, R.; Faqihi, B.M.; Stockley, R.A.; Turner, A.M. Development and Relevance of Hypercapnia in COPD. Can. Respir. J. 2021, 2021, 6623093. [Google Scholar] [CrossRef]
- Brochard, L.; Mancebo, J.; Wysocki, M.; Lofaso, F.; Conti, G.; Rauss, A.; Simonneau, G.; Benito, S.; Gasparetto, A.; Lemaire, F.; et al. Noninvasive Ventilation for Acute Exacerbations of Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 1995, 333, 817–822. [Google Scholar] [CrossRef]
- del Sorbo, L.; Pisani, L.; Filippini, C.; Fanelli, V.; Fasano, L.; Terragni, P.; Dell’Amore, A.; Urbino, R.; Mascia, L.; Evangelista, A.; et al. Extracorporeal Co2 Removal in Hypercapnic Patients at Risk of Noninvasive Ventilation Failure: A Matched Cohort Study with Historical Control. Crit. Care Med. 2015, 43, 120–127. [Google Scholar] [CrossRef]
- Morelli, A.; D’Egidio, A.; Orecchioni, A.; Alessandri, F.; Mascia, L.; Ranieri, V.M. Extracorporeal Co2 Removal in Hypercapnic Patients Who Fail Noninvasive Ventilation and Refuse Endotracheal Intubation: A Case Series. Intensive Care Med. Exp. 2015, 3, A824. [Google Scholar] [CrossRef] [Green Version]
- Braune, S.; Sieweke, A.; Brettner, F.; Staudinger, T.; Joannidis, M.; Verbrugge, S.; Frings, D.; Nierhaus, A.; Wegscheider, K.; Kluge, S. The Feasibility and Safety of Extracorporeal Carbon Dioxide Removal to Avoid Intubation in Patients with COPD Unresponsive to Noninvasive Ventilation for Acute Hypercapnic Respiratory Failure (ECLAIR Study): Multicentre Case–Control Study. Intensive Care Med. 2016, 42, 1437–1444. [Google Scholar] [CrossRef]
- Combes, A.; Auzinger, G.; Capellier, G.; du Cheyron, D.; Clement, I.; Consales, G.; Dabrowski, W.; de Bels, D.; de Molina Ortiz, F.J.G.; Gottschalk, A.; et al. ECCO2R Therapy in the ICU: Consensus of a European Round Table Meeting. Crit. Care 2020, 24, 490. [Google Scholar] [CrossRef]
- Sloane, P.J.; Gee, M.H.; Gottlieb, J.E.; Albertine, K.H.; Peters, S.P.; Robert Burns, J.; Machiedo, G.; Fish, J.E. A Multicenter Registry of Patients with Acute Respiratory Distress Syndrome. Am. Rev. Respir. Dis. 1992, 146, 419–426. [Google Scholar] [CrossRef]
- Zilberberg, M.D.; Epstein, S.K.; Ep-Stein, S.K. Acute Lung Injury in the Medical ICU Comorbid Conditions, Age, Etiology, and Hospital Outcome. Am. J. Respir. Crit. Care Med. 1998, 157, 1159–1164. [Google Scholar] [CrossRef] [Green Version]
- Yndrome, S.; Etwork, N. The new england journal of medicine ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome a bstract background traditional approaches to mechanical. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar]
- Terragni, P.P.; Rosboch, G.; Tealdi, A.; Corno, E.; Menaldo, E.; Davini, O.; Gandini, G.; Herrmann, P.; Mascia, L.; Quintel, M.; et al. Tidal Hyperinflation during Low Tidal Volume Ventilation in Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2007, 175, 160–166. [Google Scholar] [CrossRef]
- Bellani, G.; Guerra, L.; Musch, G.; Zanella, A.; Patroniti, N.; Mauri, T.; Messa, C.; Pesenti, A. Lung Regional Metabolic Activity and Gas Volume Changes Induced by Tidal Ventilation in Patients with Acute Lung Injury. Am. J. Respir. Crit. Care Med. 2011, 183, 1193–1199. [Google Scholar] [CrossRef] [Green Version]
- Rozencwajg, S.; Guihot, A.; Franchineau, G.; Lescroat, M.; Bréchot, N.; Hékimian, G.; Lebreton, G.; Autran, B.; Luyt, C.E.; Combes, A.; et al. Ultra-Protective Ventilation Reduces Biotrauma in Patients on Venovenous Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. Crit. Care Med. 2019, 47, 1505–1512. [Google Scholar] [CrossRef]
- Fanelli, V.; Costamagna, A.; Ranieri, V.M. Extracorporeal Support for Severe Acute Respiratory Failure. Semin. Respir. Crit. Care Med. 2014, 35, 519–527. [Google Scholar] [CrossRef]
- Almanza-Hurtado, A.; Polanco Guerra, C.; Martínez-Ávila, M.C.; Borré-Naranjo, D.; Rodríguez-Yanez, T.; Dueñas-Castell, C. Hypercapnia from Physiology to Practice. Int. J. Clin. Pract. 2022, 2022, 2635616. [Google Scholar] [CrossRef]
- Nin, N.; Muriel, A.; Peñuelas, O.; Brochard, L.; Lorente, J.A.; Ferguson, N.D.; Raymondos, K.; Ríos, F.; Violi, D.A.; Thille, A.W.; et al. Severe Hypercapnia and Outcome of Mechanically Ventilated Patients with Moderate or Severe Acute Respiratory Distress Syndrome. Intensive Care Med. 2017, 43, 200–208. [Google Scholar] [CrossRef]
- Combes, A.; Fanelli, V.; Pham, T.; Ranieri, V.M.; Goligher, E.C.; Brodie, D.; Pesenti, A.; Beale, R.; Brochard, L.; Chiche, J.D.; et al. Feasibility and Safety of Extracorporeal CO2 Removal to Enhance Protective Ventilation in Acute Respiratory Distress Syndrome: The SUPERNOVA Study. Intensive Care Med. 2019, 45, 592–600. [Google Scholar] [CrossRef] [Green Version]
- McNamee, J.J.; Gillies, M.A.; Barrett, N.A.; Perkins, G.D.; Tunnicliffe, W.; Young, D.; Bentley, A.; Harrison, D.A.; Brodie, D.; Boyle, A.J.; et al. Effect of Lower Tidal Volume Ventilation Facilitated by Extracorporeal Carbon Dioxide Removal vs Standard Care Ventilation on 90-Day Mortality in Patients with Acute Hypoxemic Respiratory Failure: The REST Randomized Clinical Trial. JAMA J. Am. Med. Assoc. 2021, 326, 1013–1023. [Google Scholar] [CrossRef] [PubMed]
- Akkanti, B.; Jagpal, S.; Darwish, R.; Saavedra Romero, R.; Scott, L.K.; Dinh, K.; Hussain, S.; Radbel, J.; Saad, M.A.; Enfield, K.B.; et al. Physiologic Improvement in Respiratory Acidosis Using Extracorporeal Co 2 Removal With Hemolung Respiratory Assist System in the Management of Severe Respiratory Failure From Coronavirus Disease 2019. Crit. Care Explor. 2021, 3, e0372. [Google Scholar] [CrossRef] [PubMed]
- Husain-Syed, F.; Slutsky, A.S.; Ronco, C. Lung–Kidney Cross-Talk in the Critically Ill Patient. Am. J. Respir. Crit. Care Med. 2016, 194, 402–414. [Google Scholar] [CrossRef] [PubMed]
- van den Akker, J.P.; Egal, M.; Groeneveld, J.A. Invasive Mechanical Ventilation as a Risk Factor for Acute Kidney Injury in the Critically Ill: A Systematic Review and Meta-Analysis. Crit. Care 2013, 17, R98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, P.T. The Kidney in Respiratory Failure and Mechanical Ventilation. Cardiorenal Syndr. Crit. Care 2010, 165, 159–165. [Google Scholar]
- Kuiper, J.W.; Groeneveld, A.B.J.; Slutsky, A.S.; Plötz, F.B. Mechanical Ventilation and Acute Renal Failure. Crit. Care Med. 2005, 33, 1408–1415. [Google Scholar] [CrossRef]
- Alge, J.; Dolan, K.; Angelo, J.; Thadani, S.; Virk, M.; Akcan Arikan, A. Two to Tango: Kidney-Lung Interaction in Acute Kidney Injury and Acute Respiratory Distress Syndrome. Front. Pediatr. 2021, 9, 1046. [Google Scholar] [CrossRef]
- Mehta, R.L.; Pascual, M.T.; Gruta, C.G.; Zhuang, S.; Chertow, G.M. Refining Predictive Models in Critically Ill Patients with Acute Renal Failure. J. Am. Soc. Nephrol. 2002, 13, 1350–1357. [Google Scholar] [CrossRef] [Green Version]
- Uchino, S. Acute Renal Failure in Critically Ill Patients—A Multinational, Multicenter Study. JAMA 2005, 294, 813. [Google Scholar] [CrossRef] [Green Version]
- Consales, G.; Zamidei, L.; Turani, F.; Atzeni, D.; Isoni, P.; Boscolo, G.; Saggioro, D.; Resta, M.V.; Ronco, C. Combined Renal-Pulmonary Extracorporeal Support with Low Blood Flow Techniques : A Retrospective Observational Study (CICERO Study). Blood Purif. 2022, 51, 299–308. [Google Scholar] [CrossRef]
- De Bels, D.; Pierrakos, C.; Spapen, H.D.; Honore, P.M. A Double Catheter Approach for Extracorporeal CO 2 Removal Integrated within a Continuous Renal Replacement Circuit. J. Transl. Int. Med. 2018, 6, 157–158. [Google Scholar] [CrossRef] [Green Version]
- Terragni, P.P.; Del Sorbo, L.; Mascia, L.; Urbino, R.; Martin, E.L.; Birocco, A.; Faggiano, C.; Quintel, M.; Gattinoni, L.; Ranieri, V.M. Tidal Volume Lower than 6 Ml/Kg Enhances Lung Protection: Role of Extracorporeal Carbon Dioxide Removal. Anesthesiology 2009, 111, 826–835. [Google Scholar] [CrossRef]
- Forster, C.; Schriewer, J.; John, S.; Eckardt, K.U.; Willam, C. Low-Flow CO2 Removal Integrated into a Renal-Replacement Circuit Can Reduce Acidosis and Decrease Vasopressor Requirements. Crit. Care 2013, 17, R154. [Google Scholar] [CrossRef] [Green Version]
- Quintard, J.M.; Barbot, O.; Thevenot, F.; de Matteis, O.; Benayoun, L.; Leibinger, F. Partial Extracorporeal Carbon Dioxide Removal Using a Standard Continuous Renal Replacement Therapy Device: A Preliminary Study. ASAIO J. 2014, 60, 564–569. [Google Scholar] [CrossRef]
- Allardet-Servent, J.; Castanier, M.; Signouret, T.; Soundaravelou, R.; Lepidi, A.; Seghboyan, J.M. Safety and Efficacy of Combined Extracorporeal Co2 Removal and Renal Replacement Therapy in Patients with Acute Respiratory Distress Syndrome and Acute Kidney Injury: The Pulmonary and Renal Support in Acute Respiratory Distress Syndrome Study. Crit. Care Med. 2015, 43, 2570–2581. [Google Scholar] [CrossRef] [Green Version]
- Fanelli, V.; Cantaluppi, V.; Alessandri, F.; Costamagna, A.; Cappello, P.; Brazzi, L.; Pugliese, F.; Biancone, L.; Terragni, P.; Marco Ranieri, V. Extracorporeal CO2 Removal May Improve Renal Function of Patients with Acute Respiratory Distress Syndrome and Acute Kidney Injury: An Open-Label, Interventional Clinical Trial. Am. J. Respir. Crit. Care Med. 2018, 198, 687–690. [Google Scholar] [CrossRef]
- Schmidt, M.; Jaber, S.; Zogheib, E.; Godet, T.; Capellier, G.; Combes, A. Feasibility and Safety of Low-Flow Extracorporeal CO2 Removal Managed with a Renal Replacement Platform to Enhance Lung-Protective Ventilation of Patients with Mild-to-Moderate ARDS. Crit. Care 2018, 22, 122. [Google Scholar] [CrossRef] [Green Version]
- Nentwich, J.; Wichmann, D.; Kluge, S.; Lindau, S.; Mutlak, H.; John, S. Low-Flow CO2 Removal in Combination with Renal Replacement Therapy Effectively Reduces Ventilation Requirements in Hypercapnic Patients: A Pilot Study. Ann. Intensive Care 2019, 9, 3. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA J. Am. Med. Assoc. 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Gacitúa, I.; Frías, A.; Sanhueza, M.E.; Bustamante, S.; Cornejo, R.; Salas, A.; Guajardo, X.; Torres, K.; Figueroa, E.; Eduardo, C.; et al. Extracorporeal CO2 Removal and Renal Replacement Therapy in Acute Severe Respiratory Failure in COVID-19 Pneumonia: Case Report. Semin. Dial. 2021, 34, 257–262. [Google Scholar] [CrossRef]
- Husain-Syed, F.; Birk, H.W.; Wilhelm, J.; Ronco, C.; Ranieri, V.M.; Karle, B.; Kuhnert, S.; Tello, K.; Hecker, M.; Morty, R.E.; et al. Extracorporeal Carbon Dioxide Removal Using a Renal Replacement Therapy Platform to Enhance Lung-Protective Ventilation in Hypercapnic Patients With Coronavirus Disease 2019-Associated Acute Respiratory Distress Syndrome. Front. Med. 2020, 7, 757. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Chen, H.; Zhao, H.; Zhang, H.; He, H.; Cheng, W.; Wang, C.; Jiang, W.; Ma, J.; Qin, Y.; et al. ECCO2R in 12 COVID-19 ARDS Patients With Extremely Low Compliance and Refractory Hypercapnia. Front. Med. 2021, 8, 654658. [Google Scholar] [CrossRef] [PubMed]
- Alessandri, F.; Tonetti, T.; Pistidda, L.; Busani, S.; Borrazzo, C.; Fanelli, V.; Polzoni, M.; Piazza, O.; Lorini, L.; Cattaneo, S.; et al. Extracorporeal CO2 Removal During Renal Replacement Therapy to Allow Lung-Protective Ventilation in Patients with COVID-19–Associated Acute Respiratory Distress Syndrome. ASAIO J. 2023, 69, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Chonghaile, M.N.; Higgins, B.; Laffey, J.G. Permissive Hypercapnia: Role in Protective Lung Ventilatory Strategies. Curr Opin Crit. Care 2005, 11, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Bein, T.; Weber-Carstens, S.; Goldmann, A.; Müller, T.; Staudinger, T.; Brederlau, J.; Muellenbach, R.; Dembinski, R.; Graf, B.M.; Wewalka, M.; et al. Lower Tidal Volume Strategy (≈3 Ml/Kg) Combined with Extracorporeal CO2 Removal versus ‘Conventional’ Protective Ventilation (6 Ml/Kg) in Severe ARDS. Intensive Care Med. 2013, 39, 847–856. [Google Scholar] [CrossRef] [Green Version]
- Granholm, A.; Alhazzani, W.; Derde, L.P.G.; Angus, D.C.; Zampieri, F.G.; Hammond, N.E.; Sweeney, R.M.; Myatra, S.N.; Azoulay, E.; Rowan, K.; et al. Randomised Clinical Trials in Critical Care: Past, Present and Future. Intensive Care Med. 2022, 48, 164–178. [Google Scholar] [CrossRef]
- Ronco, C.; Ratanarat, R.; Bellomo, R.; Salvatori, G.; Petras, D.; de Cal, M.; Nalasso, F.; Bonello, M.; Brendolan, A. Multiple Organ Support Therapy for the Critically Ill Patient in Intensive Care. J. Organ. Dysfunct. 2005, 1, 57–68. [Google Scholar] [CrossRef]


{kind=link}
| Study, Ref | Study Design | Patients, n | Patient Characteristics (%) | Patients with Renal Failure, n (%) | PaCO2 (mmHg)/ pH Baseline | PaCO2 (mmHg)/ pH End | Main Outcomes | AE |
|---|---|---|---|---|---|---|---|---|
| Terragni 2009 [39] | Prospective cohort study | 32 | Pneumonia (34) Sepsis (50) Trauma (16) | 0 | 73.6 ± 11 7.2 ± 0.02 | 47.2 ± 8.6 7.38 ± 0.04 | Reduction in TV in patients with initial high Pplat | Membrane clotting in three pts |
| Forster 2013 [56] | Pilot study | 10 | H1N1 pneumonia (30) Bacterial pneumonia (50) aeCOPD (20) | AKI: 10 (100) | 69 ± 10.5 7.18 ± 0.8 | 53.6 ± 13.5 7.29 ± 0.07 | Seven pts weaning from MV Two pts died in ICU | System clotting in two pts |
| Quintard 2014 [57] | Retrospective single-center study | 16 | ARDS with Pneumonia (56) Shock (19) Other (25) | AKI: 16 (100) | 77.4 ± 13.4 7.17 ± 0.1 | 47.4 ± 9.7 7.40 ± 0.07 | Reduction in TV Seven pts (43%) died in ICU | None |
| Allardet-Servent 2015 [58] | Prospective observational study | 11 | ARDS with Pneumonia (27) Urinary infection (36) Peritonitis (18) Other (18) | AKI: 11 (100) | 47 ± 11 7.28 ± 0.12 | 37 ± 4 7.42 ± 4.8 | PaCO2 reduction during LPV High mortality in ICU (82%) | Hemofilter clotting in one pt |
| Fanelli 2018 [59] | Prospective cohort study—propensity score matching | 13 ECCO2R–CRRT Vs 13 CRRT standalone | ARDS, not specified | AKI: 26 (100) | NA | NA (reported as stable) | In ECCO2R–CRRT group: uLPV reduced inflammatory and apoptosis marker | None |
| Schmidt 2018 [60] | Prospective observational study | 20 | Mild/Moderate ARDS Pneumonia (80) Other (20) | 0 | 43 ± 8 7.39 ± 0.1 | 53 ± 9 7.32 ± 0.1 | Limited PaCO2 increase during LPV 28-day mortality 15%. | Membrane clotting in ten pts Two cases hemoptysis |
| Nentwich 2019 [61] | Multicenter observational pilot study | 20 | ARDS (65) arCOPD (35) | AKI: 14 (70) CIHD: 6 (30) | 68.3 ± 11.8 7.18 ± 0.09 | 53.2 ± 14.7 7.22 ± 0.08 | Improvement of ventilatory parameters and reduction in norepinephrine | Circuit clotting in five pts |
| Consales 2021 [53] | Retrospective single-center observational study | 22 | ARDS (36) aeCOPD (64) | AKI: 18 (82) CKD: 4 (18) | 73.8 ± 11.3 7.20 ± 0.02 | 43.5 ± 4 7.40 ± 0.02 | Shift to LPV in 62% of MV pts 21 pts recover from AKI Mortality 27% | None |
| Study, Ref | ECCO2R Device | CRRT Platform | CRRT Modality | ECCO2R Position * | Circuit Duration (h) | Anticoagulant | Blood Flow (mL/min) | Membrane Oxigenator Area (m2) | Sweep Gas Flow (L/min) | CO2 Removal (mL/min) |
|---|---|---|---|---|---|---|---|---|---|---|
| Terragni, 2009 [39] | Decap®, Hemodec | Hemofilter MedicaD200, Medolla, Ita | NA | Pre | 144 (84–168) | Heparin | 191–422 | 0.33 | 8 | NA |
| Forster 2013 [56] | D902 Liliput 2 ECMO; Sorin Group | bm11/14; Edwards-Lifescience, Irvine | CVVHD | Post | 24 | Heparin | 378 ± 85.3 | 0.67 | 5.2 ± 0.98 | NA |
| Quintard 2014, [57] | HILITE 2400 LT, MEDOS | Multifiltrate, Fresenius MedicalCare | CVVHD/ CVVH | Pre | 5.9 ± 3.8 days | Heparin | 400–500 | 0.65 | 10 | NA |
| Allardet-Servent 2015 [58] | HILITE 2400 LT, MEDOS | PrismaFlex v6.0 monitor Baxter Gambro | CVVHF | Pre: 7 pts Post: 5 pts | 72 | Heparin | Pre: 432 ± 25 Post: 382 ± 29 | 0.65 | 8 | Pre: 91 ± 49 Post: 72 ± 59 |
| Fanelli 2018 [59] | NA | Diapact; B. Braun Avitum | NA | Pre | NA | Heparin 6 pts Citrate 7 pts | 276 ± 53 | NA | 8.1 ± 0.5 | NA |
| Schmidt 2018 [60] | Prismalung™, Baxter Gambro | PrismaFlex v6.0 Baxter Gambro | Not applied | NA | 31 ± 22 | Heparin | 421 ± 40 | 0.32 | 10 ± 0.3 | 51 ± 26 |
| Nentwich 2019 [61] | Prismalung™, Baxter Gambro | PrismaFlex v6.0 Baxter Gambro | CVVHF | Post | 95.8 ± 47.7 | Heparin | 400–500 | 0.32 | NA | 43.4 ± 14.1 |
| Consales 2021 [53] | Prismalung™, Baxter Gambro | PrismaFlex v6.0 Baxter Gambro | CVVHDF | NA | 82.9 ± 31.2 | Heparin | 217 ± 88.2 | 0.32 | 6.4 ± 4.9 | NA |
| Study, Ref | Study Design | Patients, n | Patients with Renal Failure, n (%) | PaCO2 (mmHg)/ pH Baseline | PaCO2 (mmHg)/ pH End | Main Outcomes | AE (%) |
|---|---|---|---|---|---|---|---|
| Husain-Syed 2020 [64] | Single-center, prospective | 4 | 1 (25) | 60.7 ± 5.4 7.33 ± 0.07 | 47 ± 3.7 7.42 ± 0.05 | TV and Pplat reduction, no effect on hemodynamics | None |
| Ding 2021 [65] | Single-center, prospective | 12 | 0 | 64.5 (56–88.75) 7.33 (7.22–7.41) | 66.4 (44.3–95.9) NA | TV and Pplat reduction, 28-day mortality 67% | None |
| Alessandri 2022 [66] | Multicenter retrospective study | 27 | AKI: 27 (100) | 68.1 ± 11.2 7.30 ± 0.08 | NA (stable) 7.39 ± 0.08 | TV reduction. Renal function improvement 28-day mortality 63%. | Circuit clotting in four pts |
| Study, Ref | ECCO2R Device | CRRT Platform | CRRT Modality | ECCO2R Position * | Circuit Duration (h) | Anticoagulant | Blood Flow (mL/min) | Membrane Oxigenator Area (m2) | Sweep Gas Flow (L/min) | CO2 Removal (mL/min) |
|---|---|---|---|---|---|---|---|---|---|---|
| Husain-Syed 2020 [64] | MultiECCO2R; Eurosets | Multifiltrate, Fresenius Medical Care | Hemoperfusion (3 pts) CVVHD (1 pt) | Post | 5.5 days | Heparin + Regional Citrate | 350 ± 87 | 1.35 | 5.4 ± 1 | NA |
| Ding 2021 [65] | QUADROX-I pediatric HMO30000, MAQUET | Prismaflex platform, Gambro-Baxter | SCUF (with UF = 0) | Pre | 24 h | Heparin | 342.5 ± 49 | 0.8 | 10 | 45.91 ± 7.70 |
| Alessandri 2022 [66] | OMNI blood purification System, B.Braun Avitum | OMNI blood purification system | CVVHDF (15 pts) CVVHD (6 pts) CVVH (6 pts) | Pre | >48 h | Heparin | 186–393 | 1.81 | 9–11 | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cappadona, F.; Costa, E.; Mallia, L.; Sangregorio, F.; Nescis, L.; Zanetti, V.; Russo, E.; Bianzina, S.; Viazzi, F.; Esposito, P. Extracorporeal Carbon Dioxide Removal: From Pathophysiology to Clinical Applications; Focus on Combined Continuous Renal Replacement Therapy. Biomedicines 2023, 11, 142. https://doi.org/10.3390/biomedicines11010142
Cappadona F, Costa E, Mallia L, Sangregorio F, Nescis L, Zanetti V, Russo E, Bianzina S, Viazzi F, Esposito P. Extracorporeal Carbon Dioxide Removal: From Pathophysiology to Clinical Applications; Focus on Combined Continuous Renal Replacement Therapy. Biomedicines. 2023; 11(1):142. https://doi.org/10.3390/biomedicines11010142
Chicago/Turabian StyleCappadona, Francesca, Elisa Costa, Laura Mallia, Filippo Sangregorio, Lorenzo Nescis, Valentina Zanetti, Elisa Russo, Stefania Bianzina, Francesca Viazzi, and Pasquale Esposito. 2023. "Extracorporeal Carbon Dioxide Removal: From Pathophysiology to Clinical Applications; Focus on Combined Continuous Renal Replacement Therapy" Biomedicines 11, no. 1: 142. https://doi.org/10.3390/biomedicines11010142