
Urinary Exosomal Tissue TIMP and Angiopoietin-1 Are Preoperative Novel Biomarkers of Well-Differentiated Thyroid Cancer
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Exosome Collection
2.3. Tryptic Digestion
2.4. MRM Q1/Q3 Ion Pair Selection Using Direct Infusion
2.5. LC-MRM/MS Analysis of Urinary Exosomes Digests
2.6. MRM Data Analysis
2.7. Thyroglobulin and Anti-Thyroglobulin Antibody
2.8. Reagents and Chemicals
2.9. Statistical Analysis
3. Results
Characteristics of Study Population

{kind=link}
{kind=link}
| Variable | LNs Metas | p-Value | |
|---|---|---|---|
| Yes (n = 8) | No (n = 13) | ||
| Pre-op exosome expression | |||
| UEx Thyroglobulin | 1.08 (0.67–1.62) | 2.21 (0.91–4.13) | 0.33 b |
| UEx Galectin-3 | 0.69 (0.57–2.39) | 1.28 (0.72–2.28) | 0.46 b |
| UEx Transketolase | 1.64 (0.45–13.36) | 0.51 (0.19–1.27) | 0.14 b |
| UEx Calprotectin A8 | 10.10 (1.42–27.68) | 42.00 (3.05–71.60) | 0.17 b |
| UEx Calprotectin A9(2) * | 38.28 (17.24–252.80) | 22.08 (4.88–67.58) | 0.49 b |
| UEx Calprotectin A9(13) * | 19.68 (7.54–87.20) | 5.20 (5.12–16.08) | 0.14 b |
| UEx Annexin-2 | 55.20 (25.60–165.60) | 40.81 (19.90–119.59) | 0.49 b |
| UEx Afamin | 0.60 (0.25–0.80) | 0.31 (0.00–0.70) | 0.58 b |
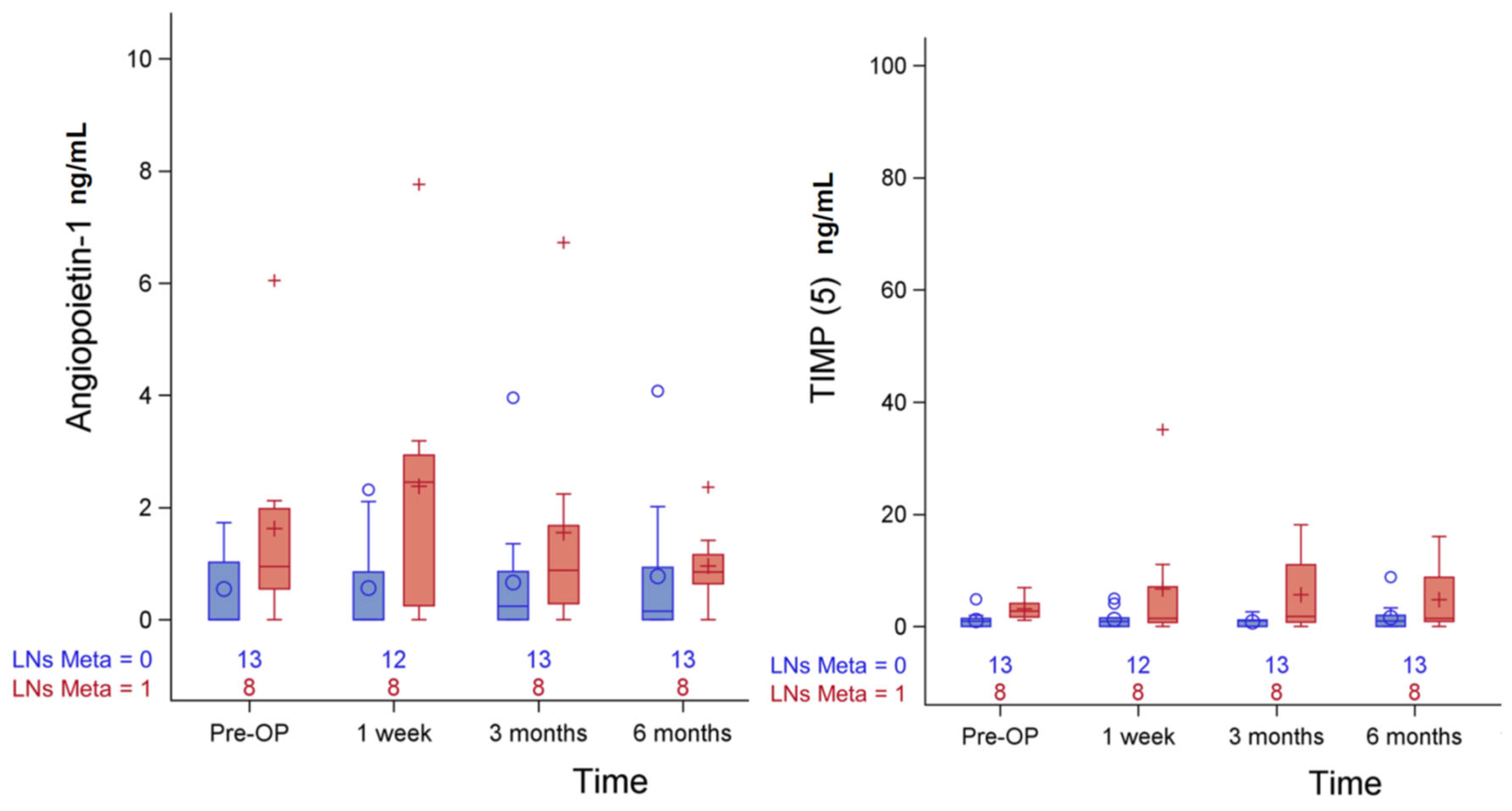
| UEx Angiopoietin-1 | 0.95 (0.55–1.98) | 0.00 (0.00–1.02) | 0.09 b |
| UEx Keratin-19 | 0.79 (0.56–1.45) | 0.69 (0.53–1.54) | 1.00 b |
| UEx TIMP (5) * | 2.73 (1.67–4.11) | 0.95 (0.00–1.42) | 0.01 b |
| UEx TIMP (14) * | 1.63 (0.33–6.38) | 0.68 (0.19–1.26) | 0.31 b |
| UEx Keratin 8 (8) * | 0.48 (0.23–1.07) | 0.42 (0.23–0.80) | 0.61 b |
| UEx Keratin 8 (17) * | 1.34 ± 0.92 | 0.94 ± 0.63 | 0.25 a |
| Demography | |||
| Gender | 0.79 c | ||
| Male | 1 (33.33%) | 2 (66.67%) | |
| Female | 7 (38.89%) | 11 (61.11%) | |
| Age (Year) | 49.75 ± 13.77 | 52.23 ± 7.95 | 0.60 a |
| Hypertension | 0.62 c | ||
| Yes | 2 (50.00%) | 2 (50.00%) | |
| No | 6 (35.29%) | 11 (64.71%) | |
| Diabetes (type 2) | 1.00 c | ||
| Yes | 2 (40.00%) | 3 (60.00%) | |
| No | 6 (37.50%) | 10 (62.50%) | |
| Clinical parameters | |||
| TNM stage | 0.04 c | ||
| I | 5 (27.78%) | 13 (72.22%) | |
| II | 3 (100.00%) | 0 (0.00%) | |
| Tumor size (cm) | 1.30 (0.65–1.60) | 1.4 (0.9–1.7) | 0.69 b |
| Tumor multifocality | 0.13 c | ||
| Yes | 2 (100.00%) | 0 (0.00%) | |
| No | 6 (31.58%) | 13 (68.42%) | |
| Extrathyroid invasion | 1 (16.67%) | 5 (83.33%) | 0.34 c |
| I-131 treatment | 0.08 c | ||
| No | 1 (16.67%) | 5 (83.33%) | |
| 1 time | 4 (33.33%) | 8 (66.67%) | |
| 2 times | 3 (100.00%) | 0 (0.00%) | |
| I-131 cumulative dose | 87.5 (30–300 mCi) | 18.4 (0–30 mCi) | 0.02 b |
| ATA (IU/mL) | 0.39 c | ||
| <3 | 3 (27.27%) | 8 (72.73%) | |
| ≥3 | 5 (50.00%) | 5 (50.00%) | |
| TPO Ab (IU/mL) | 0.63 c | ||
| <3 | 5 (33.33%) | 10 (66.67%) | |
| ≥3 | 3 (50.00%) | 3 (50.00%) | |
| Post-operative TSH (IU/mL) | 36.46 (1.25–78.85) | 23.30 (0.96–111.00) | 0.97 b |
| Peptide No. | Sequence | Molecular Weight (Dalton) | Representative Protein |
|---|---|---|---|
| 13 | LGHPDTLNQGEFK | 1455.59 | CalprotectinA9 |
| 10 | IIALDGDTK | 945.08 | Transketolase |
| 15 | GNDVAFHFNPR | 1273.37 | Galectin-3 |
| 9 | AALEDTLAETEAR | 1389.48 | Keratin 19 |
| 4 | QSSLILHGADFSTK | 1503.68 | Angiopoietin-1 |
| 6 | IALDFQR | 862 | Galectin-3 |
| 5 | FVGTPEVNQTTLYQR | 1752.95 | Tissue inhibitor of metalloproteinase |
| 8 | LSELEAALQR | 1129.28 | Keratin 8 |
| 1 | ALNSIIDVYHK | 1272.47 | CalprotectinA8 |
| 14 | GFQALGDAADIR | 1233.35 | Tissue inhibitor of metalloproteinase |
| 12 | VIFDANAPVAVR | 1271.48 | Thyroglobulin |
| 17 | ASLEAAIADAEQR | 1344.44 | Keratin 8 |
| 11 | FLAVQSVISGR | 1176.38 | Thyroglobulin |
| 16 | AEDGSVIDYELIDQDAR | 1908.99 | Annexin II |
| 3 | FLVNLVK | 832.05 | Afamin |
| 2 | NIETIINTFHQYSVK | 1807.04 | CalprotectinA9 |
| 7 | GVDEVTIVNILTNR | 1542.75 | Annexin II |
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzaferri, E.L.; Jhiang, S.M. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J. Med. 1994, 97, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid Cancer: What is new and what has changed? Cancer 2017, 123, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Kalluri, R.; LeBleu, V.S. The biology, function, and biomedical applications of exosomes. Science 2020, 367, eaau6977. [Google Scholar] [CrossRef]
- Soung, Y.H.; Nguyen, T.; Cao, H.; Lee, J.; Chung, J. Emerging roles of exosomes in cancer invasion and metastasis. BMB Rep. 2016, 49, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.Y.; Wang, C.Y.; Chen, K.Y.; Huang, L.T. Urinary exosomal thyroglobulin in thyroid cancer patients With Post-ablative Therapy: A New Biomarker in Thyroid Cancer. Front. Endocrinol. 2020, 11, 382. [Google Scholar] [CrossRef]
- Suh, S.; Kim, K.W. Diabetes and cancer: Cancer should be screened in routine diabetes assessment. Diabetes Metab. J. 2019, 43, 733–743. [Google Scholar] [CrossRef]
- Cabanillas, M.E.; McFadden, D.G.; Durante, C. Thyroid cancer. Lancet 2016, 388, 2783–2795. [Google Scholar] [CrossRef]
- Ling, Q.J.A.; Deora, A.; Febbraio, M.; Simantov, R.; Silverstein, R.L.; Hempstead, B.; Mark, W.H.; Hajjar, K.A. Annexin II regulates fibrin homeostasis and neoangiogenesis in vivo. J. Clin. Investig. 2004, 113, 38–48. [Google Scholar] [CrossRef] [Green Version]
- Feng, X.; Liu, H.; Zhang, Z.; Gu, Y.; Qiu, H.; He, Z. Annexin A2 contributes to cisplatin resistance by activation of JNK-p53 pathway in non-small cell lung cancer cells. J. Exp. Clin. Cancer Res. 2017, 36, 123. [Google Scholar] [CrossRef]
- Mahdi, A.F.; Malacrida, B.; Nolan, J.; McCumiskey, M.E.; Merrigan, A.B.; Lal, A.; Tormey, S.; Lowery, A.J.; McGourty, K.; Kiely, P.A. Expression of annexin A2 promotes cancer progression in estrogen receptor negative breast cancers. Cells 2020, 9, 1582. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.S.; Li, H.; Li, Y.; Zhu, H.; Jin, Y.-H. Identification of natural compounds targeting Annexin A2 with an anti-cancer effect. Protein Cell 2018, 9, 568–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shabani, F.; Farasat, A.; Mahdavi, M.; Gheibi, N. Calprotectin (S100A8/S100A9): A key protein between inflammation and cancer. Inflamm. Res. 2018, 67, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Khammanivong, A.; Sorenson, B.S.; Ross, K.F.; Dickerson, E.B.; Hasina, R.; Lingen, M.W.; Herzberg, M.C. Involvement of calprotectin (S100A8/A9) in molecular pathways associated with HNSCC. Oncotarget 2016, 7, 14029–14047. [Google Scholar] [CrossRef] [Green Version]
- Anjali Arora Patil, V.; Kundu, P.; Kondaiah, P.; Hegde, A.S.; Arivazhagan, A.; Santosh, V.; Pal, D.; Somasundaram, K. Serum biomarkers identification by iTRAQ and verification by MRM: S100A8/S100A9 levels predict tumor-stroma involvement and prognosis in Glioblastoma. Sci. Rep. 2019, 9, 2749. [Google Scholar]
- Lee, J.S.; Lee, N.R.; Kashif, A.; Yang, S.J.; Nam, A.R.; Song, I.C.; Gong, S.J.; Hong, M.H.; Kim, G.; Seok, P.R.; et al. S100A8 and S100A9 promote apoptosis of chronic eosinophilic leukemia cells. Front. Immunol. 2020, 11, 1258. [Google Scholar] [CrossRef]
- Mondet, J.; Chevalier, S.; Mossuz, P. Pathogenic Roles of S100A8 and S100A9 proteins in acute myeloid and lymphoid leukemia: Clinical and therapeutic impacts. Molecules 2021, 26, 1323. [Google Scholar] [CrossRef]
- Lim, S.Y.; Yuzhalin, A.E.; Gordon-Weeks, A.N.; Muschel, R.J. Tumor-infiltrating monocytes/macrophages promote tumor invasion and migration by upregulating S100A8 and S100A9 expression in cancer cells. Oncogene 2016, 35, 5735. [Google Scholar] [CrossRef] [Green Version]
- Guo, D.; Xu, Q.; Pabla, S.; Koomen, J.; Biddinger, P.; Sharma, A.; Pabla, S.; Pacholczyk, R.; Chang, C.C.; Friedrich, K.; et al. Cytokeratin-8 in anaplastic thyroid carcinoma: More than a simple structural cytoskeletal protein. Int. J. Mol. Sci. 2018, 19, 577. [Google Scholar] [CrossRef] [Green Version]
- Melmer, A.; Fineder, L.; Lamina, C.; Kollerits, B.; Dieplinger, B.; Braicu, I.; Sehouli, J.; Cadron, I.; Vergote, I.; Mahner, S.; et al. Plasma concentrations of the vitamin E-binding protein afamin are associated with overall and progression-free survival and platinum sensitivity in serous ovarian cancer—A study by the OVCAD consortium. Gynecol. Oncol. 2013, 128, 38–43. [Google Scholar] [CrossRef]
- Niedźwiecki, S.; Stepień, T.; Kopeć, K.; Kuzdak, K.; Komorowski, J.; Krupiński, R.; Stepień, H. Angiopoietin 1 (Ang-1), angiopoietin 2 (Ang-2) and Tie-2 (a receptor tyrosine kinase) concentrations in peripheral blood of patients with thyroid cancers. Cytokine 2006, 36, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.E.; Kim, K.S.; Park, S.J.; Jung, S.N.; Chang, J.W.; Yi, S.; Jung, M.G.; Kim, J.M.; Koo, B.S. High expression of angiopoietin-1 is associated with lymph node metastasis and invasiveness of papillary thyroid carcinoma. World J. Surg. 2017, 41, 3128–3138. [Google Scholar] [CrossRef] [PubMed]
- Brew, K.; Dinakarprandian, D.; Nagase, H. Tissue inhibitors of metalloproteinases: Evolution, structure and function. Biochim. Biophys. Acta 2000, 1477, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.I.; Lassalle, S.; Long-Mira, E.; Hofman, V.; Zangari, J.; Bénaim, G.; Bozec, A.; Guevara, N.; Haudebourg, J.; Birtwisle-Peyrottes, I.; et al. In papillary thyroid carcinoma, TIMP-1 expression correlates with BRAF (V600E) mutation status and together with hypoxia-related proteins predicts aggressive behavior. Virchows Arch. 2013, 463, 437–444. [Google Scholar] [CrossRef]
- Zhang, W.J.; Song, B.; Yang, T. MMP-2, MMP-9, TIMP-1, and TIMP-2 in the peripheral blood of patients with differentiated thyroid carcinoma. Cancer Manag. Res. 2019, 11, 10675–10681. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Guo, Z.; Liu, X.; Yang, L.; Jing, Z.; Cai, M.; Zheng, Z.; Shao, C.; Zhang, Y.; Sun, H.; et al. Noninvasive urinary protein signatures associated with colorectal cancer diagnosis and metastasis. Nat. Commun. 2022, 13, 2757. [Google Scholar] [CrossRef]
- Gasparri, R.; Sedda, G.; Caminiti, V.; Maisonneuve, P.; Prisciandaro, E.; Spaggiari, L. Urinary Biomarkers for Early Diagnosis of Lung Cancer. J. Clin. Med. 2021, 10, 1723. [Google Scholar] [CrossRef]


| Variable | Total |
|---|---|
| (n = 21) | |
| Female/Male | 18/3 (85.71/14.29%) |
| Age (year) | 51.29 ± 10.29 |
| Hypertension | 4 (19.05%) |
| Diabetes (type 2) | 5 (23.81%) |
| TNM stage | |
| I | 18 (85.71%) |
| II | 3 (14.29%) |
| Tumor size (cm) | 1.40 (0.9–1.6) |
| Tumor multifocality | 2 (9.52%) |
| Extrathyroid invasion | 6 (28.57%) |
| I-131 treatment | |
| No | 6 (28.57%) |
| 1 time | 12 (57.14%) |
| 2 times | 3 (14.29%) |
| I-131 cumulative dose (mCi) | (0–300) |
| 30 | 11 (52.38%) |
| 60 | 1 (0.47%) |
| 120 | 1 (0.47%) |
| 130 | 1 (0.47%) |
| 300 | 1 (0.47%) |
| ATA, ≥3 (IU/mL) | 10 (47.62%) |
| TPO Ab, ≥3 (IU/mL) | 6 (28.57) |
| Post-operative TSH (IU/mL) | 23.30 (1.00–82.30) |
| MACIS | 6.24 (5.64–6.85) |
| ≥7 | 5 (23.81%) |
| LNs Metastasis | 8 (38.10%) |
| Variable | MACIS | p-Value | |
|---|---|---|---|
| <7 (n = 16) | ≥7 (n = 5) | ||
| Pre-op exosome expression | |||
| UEx Thyroglobulin | 1.35 (0.62–3.91) | 1.87 (1.18–1.88) | 0.73 b |
| UEx Galectin-3 | 0.76 (0.59–1.55) | 1.90 (1.60–2.84) | 0.12 b |
| UEx Transketolase | 0.52 (0.27–2.17) | 1.62 (0.95–23.84) | 0.30 b |
| UEx Calprotectin A8 | 24.10 (1.42–61.80) | 37.81 (17.56–62.35) | 0.30 b |
| UEx Calprotectin A9(2) * | 26.31 (5.96–70.39) | 31.77 (30.03–241.96) | 0.39 b |
| UEx Calprotectin A9(13) * | 5.55 (5.14–62.39) | 17.07 (9.46–22.29) | 0.54 b |
| UEx Annexin-2 | 43.81 (20.47–194.20) | 45.60 (28.48–58.62) | 0.84 b |
| UEx Afamin | 0.60 (0.00–0.81) | 0.00 (0.00–0.49) | 0.35 b |
| UEx Angiopoietin-1 | 0.57 (0.00–1.38) | 0.56 (0.00–1.32) | 1.00 b |
| UEx Keratin-19 | 0.79 (0.53–1.39) | 0.69 (0.57–1.67) | 1.00 b |
| UEx TIMP (5) * | 1.31 (0.94–1.95) | 1.93 (0.00–3.49) | 0.84 b |
| UEx TIMP (14) * | 0.68 (0.21–1.20) | 4.48 (1.48–8.28) | 0.12 b |
| UEx Keratin 8 (8) * | 0.45 (0.34–0.67) | 0.23 (0.11–1.60) | 0.74 b |
| UEx Keratin 8 (17) * | 0.99 ± 0.64 | 1.40 ± 1.09 | 0.31 a |
| Demography | |||
| Gender | 1.00 c | ||
| Male | 14 (77.78%) | 4 (22.22%) | |
| Female | 2 (66.67%) | 1 (33.33%) | |
| Age | 47.94 ± 7.38 | 62 ± 11.68 | 0.004 a |
| Hypertension | 0.23 c | ||
| Yes | 2 (50.00%) | 2 (50.00%) | |
| No | 14 (82.35%) | 3 (17.65%) | |
| Diabetes (type 2) | 0.004 c | ||
| Yes | 1 (20.00%) | 4 (80.00%) | |
| No | 15 (93.75%) | 1 (6.25%) | |
| Clinical parameters | |||
| TNM stage | 0.008 c | ||
| I | 16 (88.89) | 2 (11.11) | |
| II | 0 (0.00) | 3 (100.00) | |
| Tumor size | 1.45 (0.85–1.65) | 1.1 (1.0–1.5) | 0.90 b |
| Tumor multifocality | 0.048 c | ||
| Yes | 0 (0.00%) | 2 (100.00%) | |
| No | 16 (84.21%) | 3 (15.79%) | |
| Extrathyroid invasion | 5 (83.33%) | 1 (16.67) | 0.85 c |
| I-131 treatment | 0.21 c | ||
| No | 5 (83.33%) | 1 (16.67%) | |
| 1 time | 10 (83.33%) | 2 (16.67%) | |
| 2 times | 1 (33.33%) | 2 (66.67%) | |
| I-131 cumulative dose | 30.6 (0–130 mCi) | 84 (30–300 mCi) | 0.32 b |
| ATA (IU/mL) | 0.45 c | ||
| <3 | 9 (81.82%) | 2 (18.18%) | |
| ≥3 | 7 (70.00%) | 3 (30.00%) | |
| TPO Ab (IU/mL) | 0.45 c | ||
| <3 | 12 (80.00%) | 3 (20.00%) | |
| ≥3 | 4 (66.67%) | 2 (33.33%) | |
| Post-operative TSH (IU/mL) | 4.55 (0.98–78.85) | 71.28 (23.30–111.00) | 0.49 b |
| Variable | MACIS ≥ 7 a | LNs Metas b | ||
|---|---|---|---|---|
| aOR (95% CI) | p-Value | aOR (95% CI) | p-Value | |
| Pre-op exosome expression | ||||
| UEx Thyroglobulin | 1.02 (0.57–1.81) | 0.95 | 0.95 (0.77–1.16) | 0.60 |
| UEx Galectin-3 | 1.53 (0.48–4.88) | 0.47 | 0.98 (0.64–1.49) | 0.91 |
| UEx Transketolase c | NA | - | 1.13 (0.92–1.38) | 0.25 |
| UEx Calprotectin A8 | 1.00 (0.99–1.01) | 0.74 | 0.99 (0.98–1.01) | 0.38 |
| UEx Calprotectin A9(2) * | 1.01 (0.99–1.02) | 0.51 | 1.01 (1.00–1.02) | 0.25 |
| UEx Calprotectin A9(13) * | 1.01 (0.97–1.05) | 0.68 | 1.01 (0.99–1.03) | 0.34 |
| UEx Annexin-2 | 1.00 (0.99–1.01) | 0.99 | 1.00 (1.00–1.00) | 0.92 |
| UEx Afamin | 1.23 (0.28–5.49) | 0.78 | 0.81 (0.40–1.67) | 0.57 |
| UEx Angiopoietin-1 | 1.41 (0.28–7.08) | 0.68 | 3.09 (0.99–9.60) | 0.052 |
| UEx Keratin-19 c | NA | - | 0.85 (0.38–1.89) | 0.70 |
| UEx TIMP (5) * | 2.84 (0.47–17.16) | 0.26 | 2.24 (0.97–5.15) | 0.058 |
| UEx TIMP (14) * | 1.15 (0.86–1.52) | 0.35 | 1.03 (0.90–1.18) | 0.67 |
| UEx Keratin 8 (8) * | 1.16 (0.20–6.60) | 0.87 | 0.90 (0.30–2.72) | 0.85 |
| UEx Keratin 8 (17) * | 8.57 (0.28–260.23) | 0.22 | 2.16 (0.56–8.38) | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.-Y.; Shih, S.-R.; Chen, K.-Y.; Huang, P.-J. Urinary Exosomal Tissue TIMP and Angiopoietin-1 Are Preoperative Novel Biomarkers of Well-Differentiated Thyroid Cancer. Biomedicines 2023, 11, 24. https://doi.org/10.3390/biomedicines11010024
Wang C-Y, Shih S-R, Chen K-Y, Huang P-J. Urinary Exosomal Tissue TIMP and Angiopoietin-1 Are Preoperative Novel Biomarkers of Well-Differentiated Thyroid Cancer. Biomedicines. 2023; 11(1):24. https://doi.org/10.3390/biomedicines11010024
Chicago/Turabian StyleWang, Chih-Yuan, Shyang-Rong Shih, Kuen-Yuan Chen, and Pei-Jie Huang. 2023. "Urinary Exosomal Tissue TIMP and Angiopoietin-1 Are Preoperative Novel Biomarkers of Well-Differentiated Thyroid Cancer" Biomedicines 11, no. 1: 24. https://doi.org/10.3390/biomedicines11010024