
Automated Detection of Broncho-Arterial Pairs Using CT Scans Employing Different Approaches to Classify Lung Diseases
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Method
2.1. Prior Work
2.2. Research Contribution
- The anomalies and alteration of BA information in a chest CT scan dataset, such as abnormal bronchial dilatation, distortion of the bronchial tree, lack of tapering, mucus plugging, air bronchogram, and airway wall thickening, are briefly explained with respect to the different lung diseases.
- Several image preprocessing and lung segmentation steps, including total variation denoising, dynamic intensity adjustment, Otsu thresholding, largest contour detection, inverting image, flood fill operation, inner hole filling, and bitwise_AND, are introduced.
- In the segmented lung regions, BA information is enhanced and highlighted using four approaches: Hessian-based approach, region-growing algorithm-based approach, clustering approach, and color-coding approach.
- Lung diseases are classified for the four processed datasets (Hessian, region growing, clustering, and color) using two deep learning models. The first is a CNN model having 14 layers, and the second is a CNN-based model with LSTM and an attention mechanism, having 16 layers.
2.3. Dataset
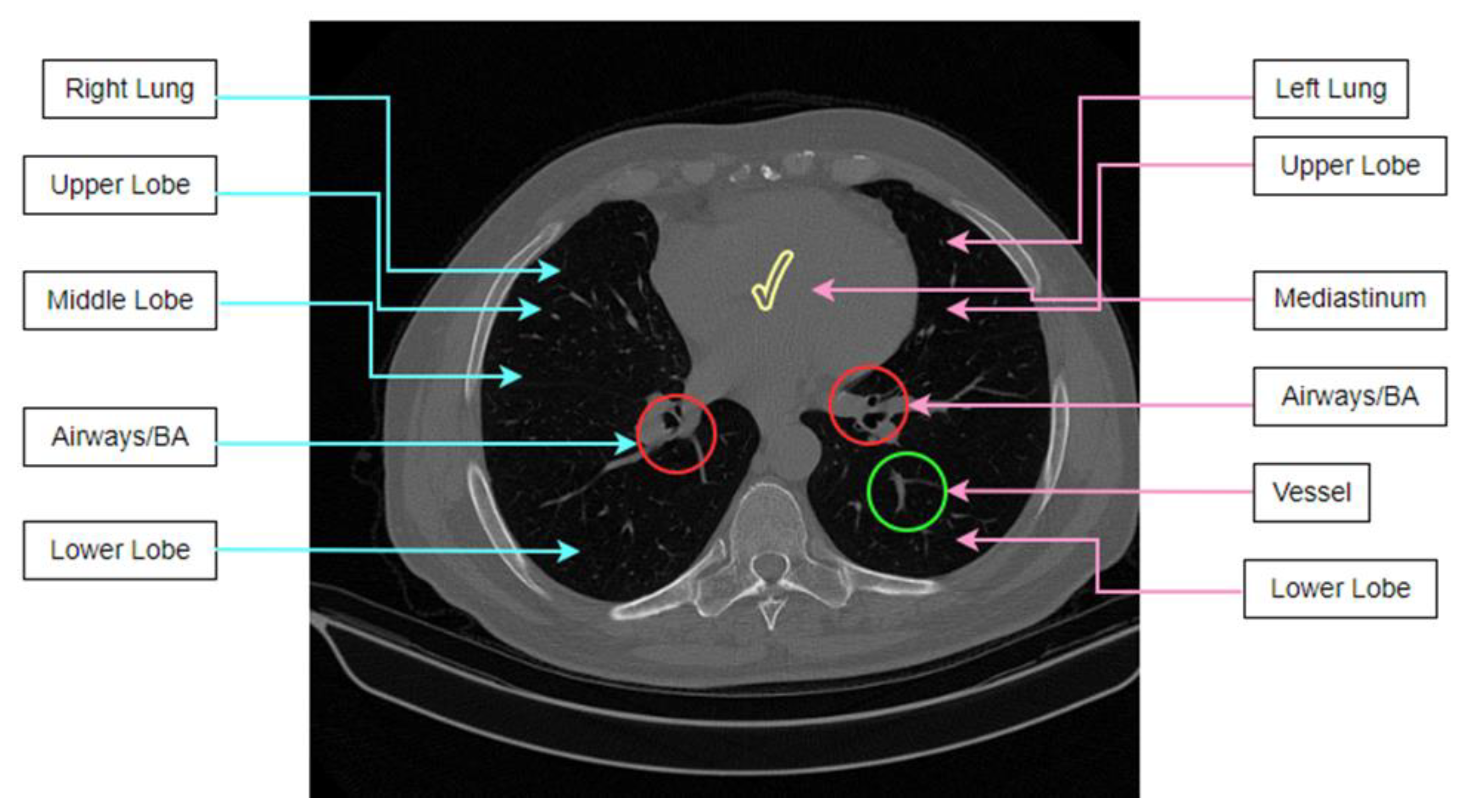
2.4. Anatomical Features of Lung CT Scans
2.4.1. Anomalies Related to Lung Disease
Bronchial Dilatation
Distortion of the Bronchial Tree
Lack of Bronchial Tapering
Airway Wall Thickening
Air Bronchogram
Mucus Plugging
2.5. Methodology
2.5.1. Lung Segmentation
Total Variation Denoising Method
Dynamic Brightness and Contrast Adjustment
Otsu Threshold Algorithm
Largest Contour Detection
Inverting the Image
Flood Fill Operation
Inner Hole Filling
Extracting Lung
2.5.2. Detection of BA from the Lungs
Hessian-Based Method
Region-Growing Method
Clustering Approach
Color-Coding Approach
2.6. Classification Using Deep Learning
2.6.1. CNN-Based Classification
2.6.2. CNN + LSTM + Attention Mechanism-Based Classification
2.6.3. Dataset Split and Training Strategy
3. Results
3.1. Developing the CNN Model Employing Ablation Study
3.2. Classification Performance of CNN Model
3.3. Classification Performance of CNN with LSTM and Attention Mechanism Model
3.4. Performance Comparison of the CNN + LSTM + Attention Mechanism Model with the Segmented CT Scan and Highlighted CT Scan
3.5. Stability Analysis of the Proposed CNN + LSTM + Attention Mechanism Model in Terms of Complexity
3.6. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Han, B.K.; Rigsby, C.K.; Hlavacek, A.; Leipsic, J.; Nicol, E.D.; Siegel, M.J.; Bardo, D.; Abbara, S.; Ghoshhajra, B.; Lesser, J.R.; et al. Computed Tomography Imaging in Patients with Congenital Heart Disease Part I: Rationale and Utility. An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT): Endorsed by the Society of Pediatric Radiology (SPR) and the North American Society of Cardiac Imaging (NASCI). J. Cardiovasc. Comput. Tomogr. 2015, 9, 475–492. [Google Scholar] [CrossRef]
- Park, H.S.; Kim, Y., II; Kim, H.Y.; Zo, J.I.; Lee, J.H.; Lee, J.S. Bronchial Artery and Systemic Artery Embolization in the Management of Primary Lung Cancer Patients with Hemoptysis. Cardiovasc. Intervent. Radiol. 2007, 30, 638–643. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.P.; Naidich, D.P. Computer-Aided Diagnosis and the Evaluation of Lung Disease. J. Thorac. Imaging 2004, 19, 136–155. [Google Scholar] [CrossRef] [PubMed]
- Kwee, T.C.; Kwee, R.M. Chest Ct in COVID-19: What the Radiologist Needs to Know. Radiographics 2020, 40, 1848–1865. [Google Scholar] [CrossRef] [PubMed]
- Pizzutto, S.J.; Hare, K.M.; Upham, J.W. Bronchiectasis in Children: Current Concepts in Immunology and Microbiology. Front. Pediatr. 2017, 5, 123. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Bracken, J.; Lam, A.; Francis, K.L.; Ramanauskas, F.; Chang, A.B.; Robinson, P.; McCallum, P.; Wurzel, D.F. Refining Diagnostic Criteria for Paediatric Bronchiectasis Using Low-Dose CT Scan. Respir. Med. 2021, 187, 106547. [Google Scholar] [CrossRef]
- Kuo, W.; de Bruijne, M.; Petersen, J.; Nasserinejad, K.; Ozturk, H.; Chen, Y.; Perez-Rovira, A.; Tiddens, H.A.W.M. Diagnosis of Bronchiectasis and Airway Wall Thickening in Children with Cystic Fibrosis: Objective Airway-Artery Quantification. Eur. Radiol. 2017, 27, 4680–4689. [Google Scholar] [CrossRef] [Green Version]
- Matsuoka, S.; Uchiyama, K.; Shima, H.; Ueno, N.; Oish, S.; Nojiri, Y. Bronchoarterial Ratio and Bronchial Wall Thickness on High-Resolution CT in Asymptomatic Subjects: Correlation with Age and Smoking. Am. J. Roentgenol. 2003, 180, 513–518. [Google Scholar] [CrossRef]
- Lynch, D.A.; Hay, T.; Newell, J.D.; Divgi, V.D.; Fan, L.L. Pediatric Diffuse Lung Disease: Diagnosis and Classification Using High-Resolution CT. Am. J. Roentgenol. 1999, 173, 713–718. [Google Scholar] [CrossRef] [Green Version]
- Ambrosetti, M.C.; Battocchio, G.; Zamboni, G.A.; Fava, C.; Tacconelli, E.; Mansueto, G. Rapid Onset of Bronchiectasis in COVID-19 Pneumonia: Two Cases Studied with CT. Radiol. Case Reports 2020, 15, 2098–2103. [Google Scholar] [CrossRef]
- Kapur, N.; Masel, J.P.; Watson, D.; Masters, I.B.; Chang, A.B. Bronchoarterial Ratio on High-Resolution CT Scan of the Chest in Children without Pulmonary Pathology: Need to Redefine Bronchial Dilatation. Chest 2011, 139, 1445–1450. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.B.; Zacharasiewicz, A.; Goyal, V.; Boyd, J.; Alexopoulou, E.; Aliberti, S.; Bell, L.; Bush, A.; Claydon, A.; Constant, C.; et al. Task Force Report: European Respiratory Society Statement for Defining Respiratory Exacerbations in Children and Adolescents with Bronchiectasis for Clinical Trials. Eur. Respir. J. 2022, 60, 2200300. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Tang, H.; McGonigle, D.; He, Z.; Zhang, C.; Wang, Y.P.; Deng, H.-W.; Bober, R.; Zhou, W. A New Approach to Extracting Coronary Arteries and Detecting Stenosis in Invasive Coronary Angiograms. arXiv 2021, arXiv:2101.09848. [Google Scholar]
- Chang, A.B.; Masel, J.P.; Boyce, N.C.; Wheaton, G.; Torzillo, P.J. Non-CF Bronchiectasis: Clinical and HRCT Evaluation. Pediatr. Pulmonol. 2003, 35, 477–483. [Google Scholar] [CrossRef]
- Bhalla, M.; Turcios, N.; Aponte, V.; Jenkins, M.; Leitman, B.S.; McCauley, D.I.; Naidich, D.P. Cystic Fibrosis: Scoring System with Thin-Section CT. Radiology 1991, 179, 783–788. [Google Scholar] [CrossRef]
- Bedi, P.; Chalmers, J.D.; Goeminne, P.C.; Mai, C.; Saravanamuthu, P.; Velu, P.P.; Cartlidge, M.K.; Loebinger, M.R.; Jacob, J.; Kamal, F.; et al. The BRICS (Bronchiectasis Radiologically Indexed CT Score): A Multicenter Study Score for Use in Idiopathic and Postinfective Bronchiectasis. Chest 2018, 153, 1177–1186. [Google Scholar] [CrossRef] [Green Version]
- Prasad, M.; Sowmya, A.; Wilson, P. Automatic Detection of Bronchial Dilatation in HRCT Lung Images. J. Digit. Imaging 2008, 21, 148–163. [Google Scholar] [CrossRef]
- Barral, M.; Sirol, M.; El Hajjam, M.; Zhang, N.; Petit, A.; Cornelis, F.H. Bronchial Artery Embolization Performed in COVID-19 Patients: Tolerance and Outcomes. Cardiovasc. Intervent. Radiol. 2020, 43, 1949–1951. [Google Scholar] [CrossRef]
- Nardelli, P.; Jimenez-Carretero, D.; Bermejo-Pelaez, D.; Washko, G.R.; Rahaghi, F.N.; Ledesma-Carbayo, M.J.; San Jose Estepar, R. Pulmonary Artery-Vein Classification in CT Images Using Deep Learning. IEEE Trans. Med. Imaging 2018, 37, 2428–2440. [Google Scholar] [CrossRef]
- Zhou, C.; Chan, H.P.; Sahiner, B.; Hadjiiski, L.M.; Chughtai, A.; Patel, S.; Wei, J.; Ge, J.; Cascade, P.N.; Kazerooni, E.A. Automatic Multiscale Enhancement and Segmentation of Pulmonary Vessels in CT Pulmonary Angiography Images for CAD Applications. Med. Phys. 2007, 34, 4567–4577. [Google Scholar] [CrossRef] [Green Version]
- Hefeda, M.M. CT Chest Findings in Patients Infected with COVID-19: Review of Literature. Egypt. J. Radiol. Nucl. Med. 2020, 51, 239. [Google Scholar] [CrossRef]
- Gu, Q.; Qi, S.; Yue, Y.; Shen, J.; Zhang, B.; Sun, W.; Qian, W.; Islam, M.S.; Saha, S.C.; Wu, J. Structural and Functional Alterations of the Tracheobronchial Tree after Left Upper Pulmonary Lobectomy for Lung Cancer. Biomed. Eng. Online 2019, 18, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Large COVID-19 CT Scan Slice Dataset|Kaggle. Available online: https://www.kaggle.com/datasets/maedemaftouni/large-covid19-ct-slice-dataset (accessed on 26 November 2022).
- Kuo, W.; Perez-Rovira, A.; Tiddens, H.; de Bruijne, M.; Akesson, L.; Bertolo, S.; Brody, A.S.; de Boeck, K.; de Jong, P.A.; Fleck, R.J.; et al. Airway Tapering: An Objective Image Biomarker for Bronchiectasis. Eur. Radiol. 2020, 30, 2703–2711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charbonnier, J.P.; Pompe, E.; Moore, C.; Humphries, S.; van Ginneken, B.; Make, B.; Regan, E.; Crapo, J.D.; van Rikxoort, E.M.; Lynch, D.A. Airway Wall Thickening on CT: Relation to Smoking Status and Severity of COPD. Respir. Med. 2019, 146, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 Pneumonia. Invest. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef]
- Qu, H.; Zhang, W.; Yang, J.; Jia, S.; Wang, G. The Value of the Air Bronchogram Sign on CT Image in the Identification of Different Solitary Pulmonary Consolidation Lesions. Medicine 2018, 97, e11985. [Google Scholar] [CrossRef] [PubMed]
- Liu: A Observational Autopsy Report of COVID-19 and—Google Scholar. Available online: https://scholar.google.com/scholar_lookup?journal=J+Forensic+Med&title=A+observational+autopsy+report+of+COVID-19+and+at+follow-up&author=XX+Liu&author=Q+Guoqiang&author=Y+Wang&volume=36&publication_year=2020&pages=19-21& (accessed on 12 October 2022).
- Kim, V.; Dolliver, W.R.; Nath, H.P.; Grumley, S.A.; Terry, N.; Ahmed, A.; Yen, A.; Jacobs, K.; Kligerman, S.; Diaz, A.A.; et al. Mucus Plugging on Computed Tomography and Chronic Bronchitis in Chronic Obstructive Pulmonary Disease. Respir. Res. 2021, 22, 110. [Google Scholar] [CrossRef]
- Carotti, M.; Salaffi, F.; Sarzi-Puttini, P.; Agostini, A.; Borgheresi, A.; Minorati, D.; Galli, M.; Marotto, D.; Giovagnoni, A. Chest CT Features of Coronavirus Disease 2019 (COVID-19) Pneumonia: Key Points for Radiologists. Radiol. Medica 2020, 125, 636–646. [Google Scholar] [CrossRef]
- Duran, J.; Coll, B.; Sbert, C. Chambolle’s Projection Algorithm for Total Variation Denoising. Image Process. Line 2013, 3, 311–331. [Google Scholar] [CrossRef] [Green Version]
- Yousefi, J. Image Binarization Using Otsu Thresholding Algorithm. Ont. Can. Univ. Guelph 2011. [Google Scholar] [CrossRef]
- Manders, E.M.M.; Strackee, J.; Aten, J.A. Largest Contour Segmentation: A Tool for the Localization of Spots in Confocal Images. Cytom. J. Int. Soc. Anal. Cytol. 1996, 23, 15–21. [Google Scholar] [CrossRef]
- Rafid, A.R.H.; Azam, S.; Montaha, S.; Karim, A.; Fahim, K.U.; Hasan, M.Z. An Effective Ensemble Machine Learning Approach to Classify Breast Cancer Based on Feature Selection and Lesion Segmentation Using Preprocessed Mammograms. Biology 2022, 11, 1654. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.; Tiwari, U.K.; Kumar, S.; Tomer, V.; Kalra, J. Comparison and Performance Evaluation of Boundary Fill and Flood Fill Algorithm. Int. J. Innov. Technol. Explor. Eng. 2020, 8, 9–13. [Google Scholar] [CrossRef]
- BahadarKhan, K.; Khaliq, A.A.; Shahid, M. A Morphological Hessian Based Approach for Retinal Blood Vessels Segmentation and Denoising Using Region Based Otsu Thresholding. PLoS ONE 2016, 11, e0158996. [Google Scholar] [CrossRef] [Green Version]
- Tang, J. A Color Image Segmentation Algorithm Based on Region Growing. In Proceedings of the 2010 2nd International Conference on Computer Engineering and Technology, Chengdu, China, 16–19 April 2010. [Google Scholar]
- Burney, S.A.; Tariq, H. K-Means Cluster Analysis for Image Segmentation. Int. J. Comput. Appl. 2014, 96. [Google Scholar]
- Lei, X.; Pan, H.; Huang, X. A Dilated CNN Model for Image Classification. IEEE Access 2019, 7, 124087–124095. [Google Scholar] [CrossRef]
- Van Rikxoort, E.M.; Van Ginneken, B. Automated Segmentation of Pulmonary Structures in Thoracic Computed Tomography Scans: A Review. Phys. Med. Biol. 2013, 58, R187. [Google Scholar] [CrossRef]
- Vallabhaneni, R.B.; Rajesh, V. Brain Tumour Detection Using Mean Shift Clustering and GLCM Features with Edge Adaptive Total Variation Denoising Technique. Alex. Eng. J. 2018, 57, 2387–2392. [Google Scholar] [CrossRef]
- Dutta, S.; Dey, G.; Chakraborty, S.; Roy, P.; Dey, N.; Ray, R. Adaptive Thresholding: A Comparative Study. In Proceedings of the 2014 International Conference on Control, Instrumentation, Communication and Computational Technologies (ICCICCT), Kanyakumari District, India, 10–11 July 2014. [Google Scholar] [CrossRef]
- Salima, A.; Herdiyeni, Y.; Douady, S. Leaf Vein Segmentation of Medicinal Plant Using Hessian Matrix. In Proceedings of the 2015 International Conference on Advanced Computer Science and Information Systems (ICACSIS), Depok Indonesia, Indonesian, 10–11 October 2015. [Google Scholar] [CrossRef]
- Khalid, N.E.A.; Ibrahim, S.; Manaf, M.; Ngah, U.K. Seed-Based Region Growing Study for Brain Abnormalities Segmentation. In Proceedings of the 2010 International Symposium on Information Technology, Kuala Lumpur, Malaysia, 15–17 June 2010. [Google Scholar] [CrossRef]
- Pérez, J.M.M.; Pascau, J. Image Processing with ImageJ. Packt Publishing Ltd.: Birmingham, UK, 2013. [Google Scholar]
- Tatiraju, S.; Mehta, A. Image Segmentation Using K-Means Clustering, EM and Normalized Cuts. Dep. EECS 2008, 1, 1–7. [Google Scholar]
- Montaha, S.; Azam, S.; Rakibul Haque Rafid, A.K.M.; Islam, S.; Ghosh, P.; Jonkman, M. A Shallow Deep Learning Approach to Classify Skin Cancer Using Down-Scaling Method to Minimize Time and Space Complexity. PLoS ONE 2022, 17, e0269826. [Google Scholar] [CrossRef]
- Montaha, S.; Azam, S.; Rafid, A.R.H.; Hasan, M.Z.; Karim, A.; Islam, A. TimeDistributed-CNN-LSTM: A Hybrid Approach Combining CNN and LSTM to Classify Brain Tumor on 3D MRI Scans Performing Ablation Study. IEEE Access 2022, 10, 60039–60059. [Google Scholar] [CrossRef]
- Islam, M.Z.; Islam, M.M.; Asraf, A. A Combined Deep CNN-LSTM Network for the Detection of Novel Coronavirus (COVID-19) Using X-Ray Images. Inform. Med. Unlocked 2020, 20, 100412. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Jin, K.; Zhou, D.; Kubota, N.; Ju, Z. Attention Mechanism-Based CNN for Facial Expression Recognition. Neurocomputing 2020, 411, 340–350. [Google Scholar] [CrossRef]
- Aditi, M.K.; Poovammal, E. Image Classification Using a Hybrid Lstm-Cnn Deep Neural Network. Int. J. Eng. Adv. Technol. 2019, 8, 1342–1348. [Google Scholar] [CrossRef]
- Hamdi, S.; Oussalah, M.; Moussaoui, A.; Saidi, M. Attention-Based Hybrid CNN-LSTM and Spectral Data Augmentation for COVID-19 Diagnosis from Cough Sound. J. Intell. Inf. Syst. 2022, 59, 367–389. [Google Scholar] [CrossRef]
- Hirra, I.; Ahmad, M.; Hussain, A.; Ashraf, M.U.; Saeed, I.A.; Qadri, S.F.; Alghamdi, A.M.; Alfakeeh, A.S. Breast Cancer Classification from Histopathological Images Using Patch-Based Deep Learning Modeling. IEEE Access 2021, 9, 24273–24287. [Google Scholar] [CrossRef]
- Wei, L.; Ding, K.; Hu, H. Automatic Skin Cancer Detection in Dermoscopy Images Based on Ensemble Lightweight Deep Learning Network. IEEE Access 2020, 8, 99633–99647. [Google Scholar] [CrossRef]
- Yaqub, M.; Feng, J.; Sultan Zia, M.; Arshid, K.; Jia, K.; Ur Rehman, Z.; Mehmood, A. State-of-the-Art CNN Optimizer for Brain Tumor Segmentation in Magnetic Resonance Images. Brain Sci. 2020, 10, 427. [Google Scholar] [CrossRef]
- Montaha, S.; Azam, S.; Rakibul Haque Rafid, A.K.M.; Ghosh, P.; Hasan, M.Z.; Jonkman, M.; De Boer, F. BreastNet18: A High Accuracy Fine-Tuned VGG16 Model Evaluated Using Ablation Study for Diagnosing Breast Cancer from Enhanced Mammography Images. Biology 2021, 10, 1347. [Google Scholar] [CrossRef]
































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Description |
|---|---|
| Total amount of CT scans | 17,104 |
| Dimension | 512 × 512 |
| Images type | CT scan |
| Colour Grading | Gray scale |
| Non-COVID | 6983 |
| COVID | 7593 |
| CAP | 2618 |
| Ablation Study 1: Changing Kernel Size | ||||
| Configuration | Kernel Size | Epoch × Training Time | Test Accuracy | Finding |
| 1 | 4 | 100 × 161 s | 81.25% | Previous accuracy |
| 2 | 3 | 100 × 135 s | 83.68% | Highest accuracy |
| 3 | 2 | 100 × 135 s | 78.54% | Accuracy dropped |
| 4 | 5 | 100 × 170 s | 80.71% | Accuracy dropped |
| Ablation Study 2: Changing the Loss Function | ||||
| Configuration | Loss Function | Epoch × Training Time | Test Accuracy | Finding |
| 1 | Categorical Cross-entropy | 100 × 135 s | 83.68% | Highest accuracy |
| 2 | Mean Squared Error | 100 × 135 s | 78.15% | Accuracy dropped |
| 3 | Mean absolute error | 100 × 135 s | 79.55% | Accuracy dropped |
| Ablation Study 3: Changing the Type of Pooling Layer | ||||
| Configuration | Type of Pooling Layer | Epochs × Training Time | Test Accuracy | Findings |
| 1 | Max | 100 × 135 s | 83.83% | Highest accuracy |
| 2 | Average | 100 × 135 s | 83.68% | Previous accuracy |
| Ablation Study 4: Changing the Activation Function | ||||
| Configuration | Activation Function | Epochs × Training Time | Test Accuracy | Findings |
| 1 | Tanh | 100 × 135 s | 79.74% | Accuracy dropped |
| 2 | ReLU | 100 × 135 s | 83.83% | Previous accuracy |
| 3 | PReLU | 100 × 135 s | 84.52% | Highest accuracy |
| 4 | Leaky ReLU | 100 × 135 s | 83.33% | Improved accuracy |
| Ablation Study 5: Changing Optimizer | ||||
| Configuration | Optimizer | Epochs × Training Time | Test Accuracy | Findings |
| 1 | Adam | 100 × 135 s | 84.52% | Previous accuracy |
| 2 | Nadam | 100 × 135 s | 85.28% | Highest dropped |
| 3 | SGD | 100 × 135 s | 79.28% | Accuracy dropped |
| 4 | Adamax | 100 × 135 s | 84.27% | Accuracy dropped |
| 5 | RMSprop | 100 × 135 s | 83.95% | Accuracy dropped |
| Ablation Study 6: Learning Rate | ||||
| Configuration | Learning Rate | Epochs × Training Time | Test Accuracy | Findings |
| 1 | 0.0001 | 100 × 135 s | 85.42% | Improved accuracy |
| 2 | 0.001 | 100 × 135 s | 85.28% | Previous accuracy |
| 3 | 0.008 | 100 × 135 s | 84.85% | Accuracy dropped |
| 4 | 0.0008 | 100 × 135 s | 85.69% | Highest accuracy |
| Measure | Hessian | Region Growing | Color-Coding | Clustering |
|---|---|---|---|---|
| Training accuracy | 94.65% | 92.57% | 95.41% | 97.76% |
| Validation accuracy | 88.52% | 86.82% | 94.85% | 96.12% |
| Test accuracy | 88.78% | 87.14% | 92.36% | 95.84% |
| Recall | 89.68% | 89.87% | 94.72% | 97.15% |
| Specificity | 93.37% | 91.31% | 97.18% | 98.88% |
| Precision | 87.79% | 86.79% | 90.66% | 94.79% |
| F1 score | 88.71% | 86.83% | 92.75% | 96.06% |
| Class | Hessian | Region Growing | Color-Coding | Clustering |
|---|---|---|---|---|
| Non-COVID | 85.37% | 86.87% | 91.86% | 94.61% |
| COVID | 87.61% | 86.15% | 92.14% | 95.34% |
| CAP | 89.38% | 88.87% | 93.27% | 96.38% |
| Overall accuracy | 88.78% | 87.14% | 92.36% | 95.84% |
| Measure | Hessian | Region Growing | Color-Coding | Clustering |
|---|---|---|---|---|
| Training accuracy | 95.90% | 93.21% | 97.52% | 98.68% |
| Validation accuracy | 88.95% | 87.58% | 96.47% | 96.83% |
| Test accuracy | 89.61% | 88.28% | 94.61% | 97.12% |
| Recall | 91.46% | 90.32% | 96.44% | 98.26% |
| Specificity | 94.88% | 92.68% | 98.73% | 99.02% |
| Precision | 88.92% | 87.85% | 92.22% | 99.02% |
| F1 score (F1) | 89.58% | 88.43% | 94.97% | 97.57% |
| Class | Hessian | Region Growing | Color-Coding | Clustering |
|---|---|---|---|---|
| Non-COVID | 88.67% | 87.43% | 93.86% | 96.61% |
| COVID | 88.24% | 86.54% | 94.62% | 97.09 % |
| CAP | 90.27% | 89.51% | 95.71% | 99.23% |
| Over all accuracy | 89.56% | 88.28% | 94.61% | 97.12% |
| Measure | Segmented Lung CT Scan | Color-Coding | Clustering |
|---|---|---|---|
| Training accuracy | 92.45% | 97.52% | 98.68% |
| Validation accuracy | 89.39% | 96.47% | 96.83% |
| Test accuracy | 87.69% | 94.61% | 97.12% |
| Recall | 89.44% | 96.44% | 98.26% |
| Specificity | 93.73% | 98.73% | 99.02% |
| Precision | 83.09% | 92.22% | 99.02% |
| F1 score (F1) | 87.83% | 94.97% | 97.57% |
| Dataset | K-Fold Configurations | Accuracy (%) | Per Epoch Training Time (Second) | Total Training Time (Hour) | RAM Usage |
|---|---|---|---|---|---|
| Color coding | 3 fold | 94.48 | 130–135 | 3.5–3.75 | 62% |
| 5 fold | 94.55 | 130–135 | 3.5–3.75 | 61% | |
| 7 fold | 94.51 | 130–135 | 3.5–3.75 | 62% | |
| 10 fold | 94.59 | 130–135 | 3.5–3.75 | 63% | |
| 13 fold | 94.63 | 130–135 | 3.5–3.75 | 62% | |
| 15 fold | 94.65 | 130–135 | 3.5–3.75 | 62% | |
| 17 fold | 94.58 | 130–135 | 3.5–3.75 | 61% | |
| 20 fold | 94.63 | 130–135 | 3.5–3.75 | 63% | |
| Clustering | 3 fold | 96.95 | 130–135 | 3.5–3.75 | 63% |
| 5 fold | 97.04 | 130–135 | 3.5–3.75 | 64% | |
| 7 fold | 97.02 | 130–135 | 3.5–3.75 | 63% | |
| 10 fold | 97.18 | 130–135 | 3.5–3.75 | 65% | |
| 13 fold | 97.20 | 130–135 | 3.5–3.75 | 64% | |
| 15 fold | 96.98 | 130–135 | 3.5–3.75 | 63% | |
| 17 fold | 97.06 | 130–135 | 3.5–3.75 | 63% | |
| 20 fold | 97.11 | 130–135 | 3.5–3.75 | 65% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azam, S.; Rafid, A.K.M.R.H.; Montaha, S.; Karim, A.; Jonkman, M.; De Boer, F. Automated Detection of Broncho-Arterial Pairs Using CT Scans Employing Different Approaches to Classify Lung Diseases. Biomedicines 2023, 11, 133. https://doi.org/10.3390/biomedicines11010133
Azam S, Rafid AKMRH, Montaha S, Karim A, Jonkman M, De Boer F. Automated Detection of Broncho-Arterial Pairs Using CT Scans Employing Different Approaches to Classify Lung Diseases. Biomedicines. 2023; 11(1):133. https://doi.org/10.3390/biomedicines11010133
Chicago/Turabian StyleAzam, Sami, A.K.M. Rakibul Haque Rafid, Sidratul Montaha, Asif Karim, Mirjam Jonkman, and Friso De Boer. 2023. "Automated Detection of Broncho-Arterial Pairs Using CT Scans Employing Different Approaches to Classify Lung Diseases" Biomedicines 11, no. 1: 133. https://doi.org/10.3390/biomedicines11010133