
Change in PD-L1 and CD8 Expression after Chemoradiotherapy for Esophageal Squamous Cell Carcinoma

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
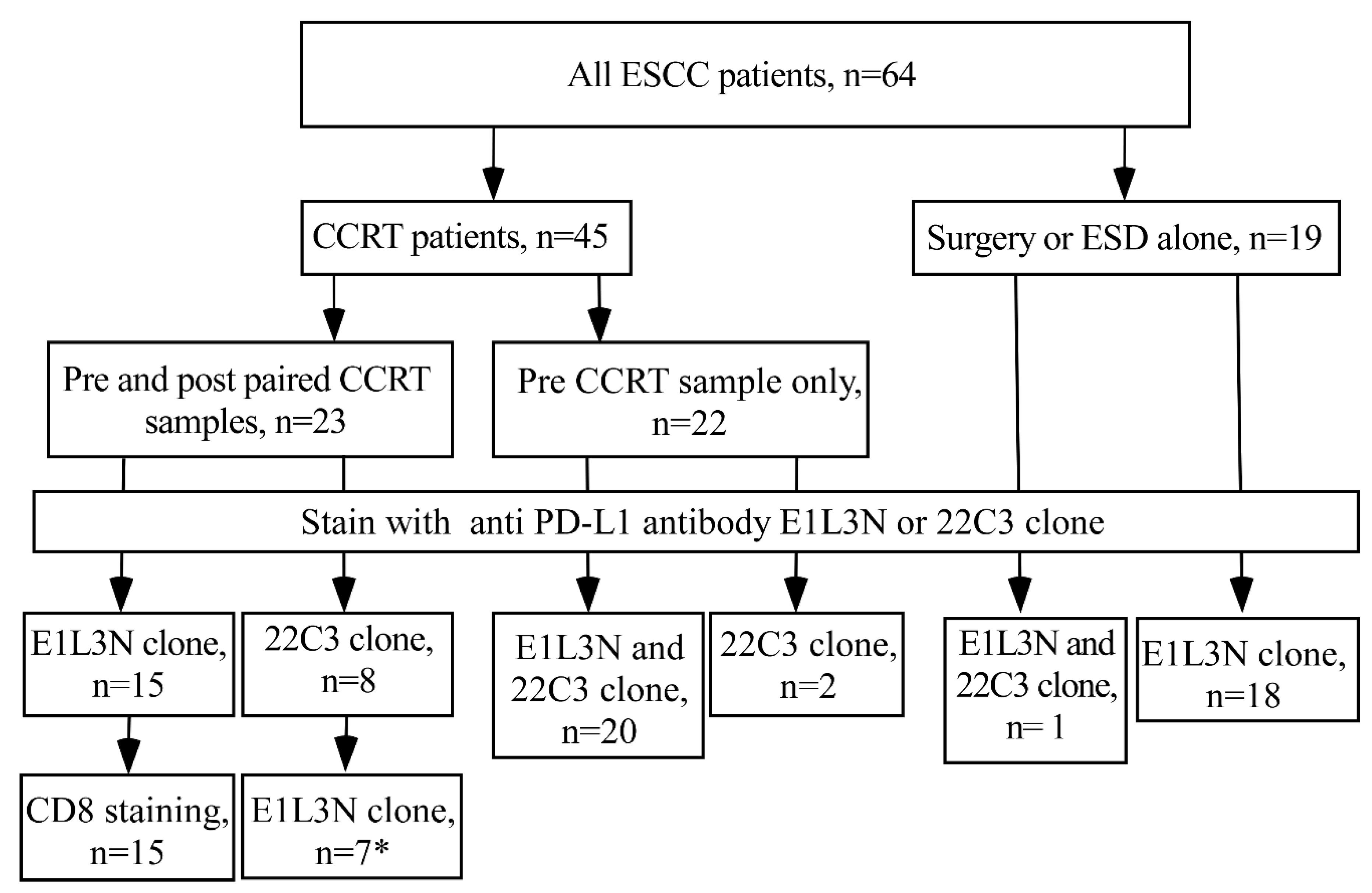
2.1. Patients and Specimens
2.2. Immunohistochemistry Staining for PD-L1 and CD8
2.3. Evaluation of PD-L1 and CD8
2.4. Quality Control for PD-L1 of E1L3N Clone
2.5. Statistical Analysis
3. Results
3.1. Study Subjects
3.2. Down Regulation of PD-L1 in ESCC after CCRT Treatment
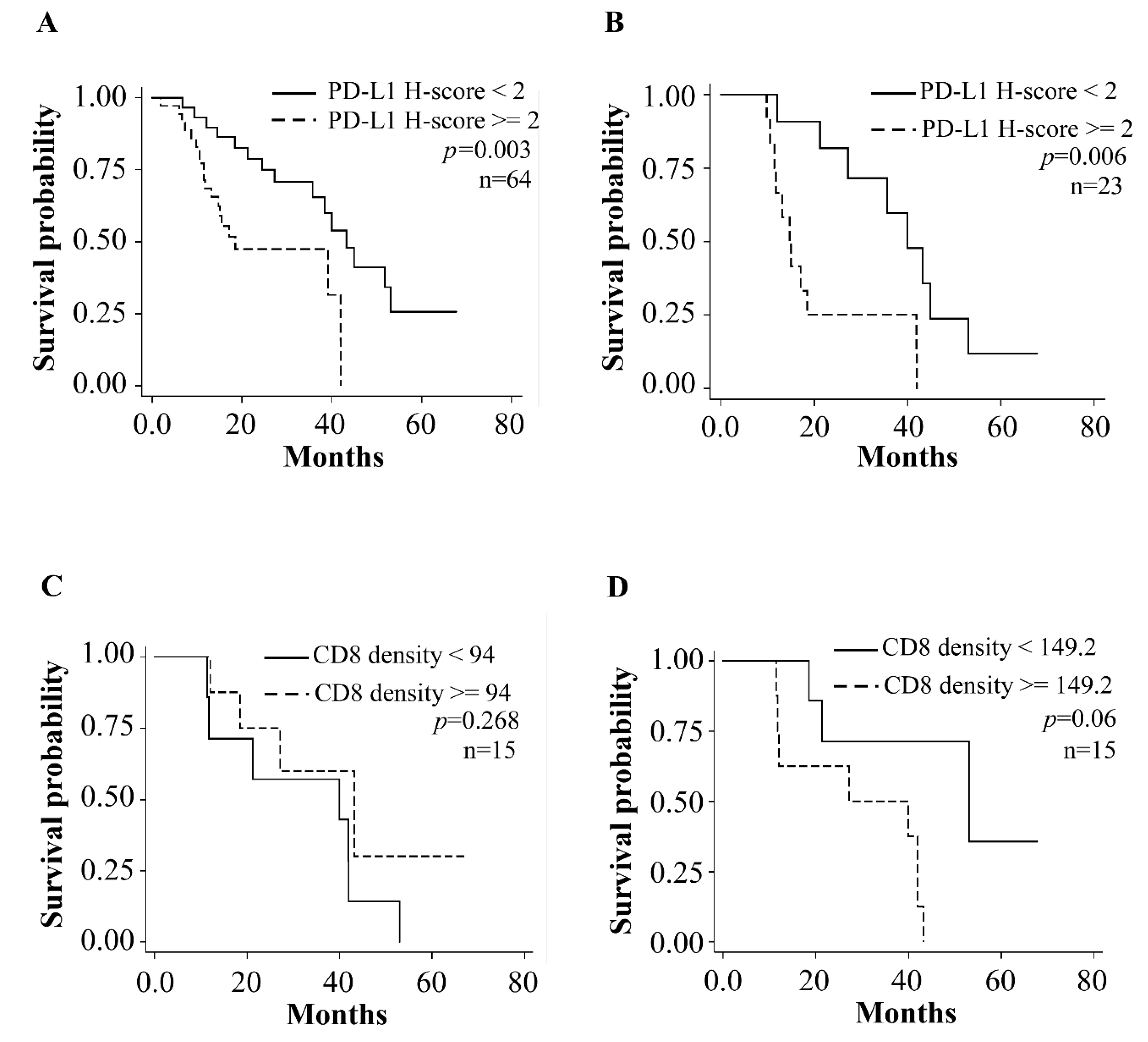
3.3. Prognostic Relevance of Tumor PD-L1 Expression in ESCC Patients
3.4. CD8 Positive Cells in Tumor Specimens before and after CCRT
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ribas, A.; Wolchok, J.D. Cancer immunotherapy using checkpoint blockade. Science 2018, 359, 1350–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Food and Drug Administration. FDA Approves Pembrolizumab for Esophageal or GEJ Carcinoma. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-pembrolizumab-esophageal-or-gej-carcinoma (accessed on 5 December 2021).
- Mimura, K.; Yamada, L.; Ujiie, D.; Hayase, S.; Tada, T.; Hanayama, H.; Min, A.K.T.; Shibata, M.; Momma, T.; Saze, Z.; et al. Immunotherapy for esophageal squamous cell carcinoma: A review. Fukushima J. Med. Sci. 2018, 64, 46–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farinha, H.T.; Digklia, A.; Schizas, D.; Demartines, N.; Schafer, M.; Mantziari, S. Immunotherapy for Esophageal Cancer: State-of-the Art in 2021. Cancers 2022, 14, 554. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Cho, B.C.; Takahashi, M.; Okada, M.; Lin, C.Y.; Chin, K.; Kadowaki, S.; Ahn, M.J.; Hamamoto, Y.; Doki, Y.; et al. Nivolumab versus chemotherapy in patients with advanced oesophageal squamous cell carcinoma refractory or intolerant to previous chemotherapy (ATTRACTION-3): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 1506–1517. [Google Scholar] [CrossRef]
- Kojima, T.; Shah, M.A.; Muro, K.; Francois, E.; Adenis, A.; Hsu, C.H.; Doi, T.; Moriwaki, T.; Kim, S.B.; Lee, S.H.; et al. Randomized Phase III KEYNOTE-181 Study of Pembrolizumab Versus Chemotherapy in Advanced Esophageal Cancer. J. Clin. Oncol. 2020, 38, 4138–4148. [Google Scholar] [CrossRef]
- Kelly, R.J.; Ajani, J.A.; Kuzdzal, J.; Zander, T.; Van Cutsem, E.; Piessen, G.; Mendez, G.; Feliciano, J.; Motoyama, S.; Lievre, A.; et al. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. N. Engl. J. Med. 2021, 384, 1191–1203. [Google Scholar] [CrossRef]
- Rong, L.; Liu, Y.; Hui, Z.; Zhao, Z.; Zhang, Y.; Wang, B.; Yuan, Y.; Li, W.; Guo, L.; Ying, J.; et al. PD-L1 expression and its clinicopathological correlation in advanced esophageal squamous cell carcinoma in a Chinese population. Diagn. Pathol. 2019, 14, 6. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Feng, F.; Wang, F.; Liu, Z.; Liu, S.; Xu, G.; Zheng, G.; Guo, M.; Lian, X.; Zhang, H. PD-L1 Expression On tumor Cells Was Associated With Unfavorable Prognosis In Esophageal Squamous Cell Carcinoma. J. Cancer 2018, 9, 2224–2231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, C.; Zhu, Y.; Tang, S.; Zhang, G.; Lin, Q.; Xu, Y.; Shang, J. High PD-L1 expression is associated with a favorable prognosis in patients with esophageal squamous cell carcinoma undergoing postoperative adjuvant radiotherapy. Oncol. Lett. 2019, 17, 1626–1634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.; Cheng, G.; Zhang, F.; Zhang, N.; Li, D.; Jin, J.; Wu, J.; Ying, L.; Mao, W.; Su, D. Prognostic significance of programmed death-1 and programmed death-ligand 1 expression in patients with esophageal squamous cell carcinoma. Oncotarget 2016, 7, 30772–30780. [Google Scholar] [CrossRef] [PubMed]
- Qu, H.X.; Zhao, L.P.; Zhan, S.H.; Geng, C.X.; Xu, L.; Xin, Y.N.; Jiang, X.J. Clinicopathological and prognostic significance of programmed cell death ligand 1 (PD-L1) expression in patients with esophageal squamous cell carcinoma: A meta-analysis. J. Thorac. Dis. 2016, 8, 3197–3204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, W.; Wang, P.; Li, N.; Shao, F.; Zhang, H.; Yang, Z.; Li, R.; Gao, Y.; He, J. Prognostic value of PD-L1 in esophageal squamous cell carcinoma: A meta-analysis. Oncotarget 2018, 9, 13920–13933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, H.; Li, Y.; Li, S.; Liu, G. Prognostic Function of Programmed Cell Death-Ligand 1 in Esophageal Squamous Cell Carcinoma Patients Without Preoperative Therapy: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 693886. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.C.; Wu, C.T.; Wang, C.P.; Lou, P.J.; Ko, J.Y.; Chang, Y.L. The differences of immunologic and TP53 mutant phenotypes between synchronous and metachronous head and neck cancer and esophageal cancer. Oral Oncol. 2020, 111, 104945. [Google Scholar] [CrossRef] [PubMed]
- Ito, N.; Tsujimoto, H.; Horiguchi, H.; Shimazaki, H.; Miyazaki, H.; Saitoh, D.; Kishi, Y.; Ueno, H. Clinical Significance of Programmed Death Ligand-1 Expression in Esophageal Squamous Cell Carcinoma. J. Surg. Res. 2020, 251, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, B.; Jung, H.A.; La Choi, Y.; Sun, J.M. Nivolumab for esophageal squamous cell carcinoma and the predictive role of PD-L1 or CD8 expression in its therapeutic effect. Cancer Immunol. Immunother. 2021, 70, 1203–1211. [Google Scholar] [CrossRef] [PubMed]
- Kovaleva, O.V.; Rashidova, M.A.; Samoilova, D.V.; Podlesnaya, P.A.; Mochalnikova, V.V.; Gratchev, A. Immunosuppressive Phenotype of Esophagus Tumors Stroma. Anal. Cell Pathol. 2020, 2020, 5424780. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Li, M.; Mu, D.; Kong, L.; Zhang, J.; Zhao, F.; Li, Z.; Liu, X.; Bo, C.; Yu, J. CD8+/FOXP3+ ratio and PD-L1 expression associated with survival in pT3N0M0 stage esophageal squamous cell cancer. Oncotarget 2016, 7, 71455–71465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, S.; Yang, H.; Zhang, J.; Wang, J.; Liang, Z.; Liu, S.; Li, Y.; Pan, Y.; Zhao, L.; Xi, M. Changes in Indoleamine 2,3-Dioxygenase 1 Expression and CD8+ Tumor-Infiltrating Lymphocytes after Neoadjuvant Chemoradiation Therapy and Prognostic Significance in Esophageal Squamous Cell Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 286–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowe, A.R.; Yue, W. Semi-quantitative Determination of Protein Expression using Immunohistochemistry Staining and Analysis: An Integrated Protocol. Bio Protoc. 2019, 9, 3465. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, K.M.; Sun, H.; Liao, X.; Hua, P.; Callea, M.; Greenfield, E.A.; Hodi, F.S.; Sharpe, A.H.; Signoretti, S.; Rodig, S.J.; et al. PD-L1 Antibodies to Its Cytoplasmic Domain Most Clearly Delineate Cell Membranes in Immunohistochemical Staining of Tumor Cells. Cancer Immunol. Res. 2015, 3, 1308–1315. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.; Bo, Y.; Wang, K.; Liu, Y.; Tang, X.; Zhao, Y.; Zhao, E.; Yuan, L. Concurrent neoadjuvant chemoradiotherapy could improve survival outcomes for patients with esophageal cancer: A meta-analysis based on random clinical trials. Oncotarget 2017, 8, 20410–20417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, K.; Miyata, H.; Sugimura, K.; Kanemura, T.; Hamada-Uematsu, M.; Mizote, Y.; Yamasaki, M.; Wada, H.; Nakajima, K.; Takiguchi, S.; et al. Negative influence of programmed death-1-ligands on the survival of esophageal cancer patients treated with chemotherapy. Cancer Sci. 2016, 107, 726–733. [Google Scholar] [CrossRef]
- Lim, S.H.; Hong, M.; Ahn, S.; Choi, Y.L.; Kim, K.M.; Oh, D.; Ahn, Y.C.; Jung, S.H.; Ahn, M.J.; Park, K.; et al. Changes in tumour expression of programmed death-ligand 1 after neoadjuvant concurrent chemoradiotherapy in patients with squamous oesophageal cancer. Eur. J. Cancer 2016, 52, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Joung, J.G.; Min, Y.W.; Nam, J.Y.; Ryu, D.; Oh, D.; Park, W.Y.; Lee, S.H.; Choi, Y.; Ahn, J.S.; et al. Paired whole exome and transcriptome analyses for the Immunogenomic changes during concurrent chemoradiotherapy in esophageal squamous cell carcinoma. J. Immunother. Cancer 2019, 7, 128. [Google Scholar] [CrossRef] [PubMed]
- Rimm, D.L.; Han, G.; Taube, J.M.; Yi, E.S.; Bridge, J.A.; Flieder, D.B.; Homer, R.; West, W.W.; Wu, H.; Roden, A.C.; et al. A Prospective, Multi-institutional, Pathologist-Based Assessment of 4 Immunohistochemistry Assays for PD-L1 Expression in Non-Small Cell Lung Cancer. JAMA Oncol. 2017, 3, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Yoh, K.; Matsumoto, S.; Furuya, N.; Nishino, K.; Miyamoto, S.; Oizumi, S.; Okamoto, N.; Itani, H.; Kuyama, S.; Nakamura, A.; et al. Comprehensive assessment of PD-L1 expression, tumor mutational burden and oncogenic driver alterations in non-small cell lung cancer patients treated with immune checkpoint inhibitors. Lung Cancer 2021, 159, 128–134. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean ± SD or No. (%) | |
|---|---|---|
| Gender | ||
| Male | 61 | (95.3) |
| Female | 3 | (4.6) |
| Age (years) (Mean) | 56.08 | ±8.17 |
| Pathologic status | ||
| Stage I | 10 | (15.6) |
| Stage II | 14 | (21.8) |
| Stage III | 36 | (56.2) |
| Stage IV | 4 | (6.2) |
| Tumor differentiation | ||
| Grade 1 (Well) | 5 | (7.8) |
| Grade 2 (Moderate) | 49 | (76.5) |
| Grade 3 (Poor) | 6 | (9.3) |
| Missing | 4 | (6.2) |
| Treatment | ||
| ESD only | 5 | (7.8) |
| OP only | 14 | (21.9) |
| CCRT | 25 | (39.1) |
| CCRT then OP | 20 | (31.2) |
| CCRT Response All CCRT cases (N = 45) | ||
| Complete response | 7 | (15.6) |
| Partial response | 32 | (71.1) |
| Stable disease | 5 | (11.1) |
| Progressive disease | 1 | (2.2) |
| With paired specimens before and after CCRT (N = 23) | ||
| Partial response | 22 | (95.6) |
| Stable disease | 1 | (4.4) |
| Variables | No. | Adjusted HR | 95% CI | p Value |
|---|---|---|---|---|
| Pre-CCRT PD-L1 H score | ||||
| H-score Median <2 | 29 | 1 | ||
| H-score Median ≥2 | 35 | 2.81 | 1.20–6.62 | 0.02 |
| Gender | ||||
| Male | 61 | 1 | ||
| Female | 3 | 0.72 | 0.09–5.55 | 0.76 |
| Age | 64 | 1.07 | 1.10–1.12 | 0.01 |
| Stage | ||||
| Stage I and II | 24 | 1 | ||
| Stage III and IV | 40 | 2.34 | 0.67–8.16 | 0.18 |
| Treatment | ||||
| With OP or ESD | 19 | 1 | ||
| With CCRT | 45 | 0.39 | 0.10–1.52 | 0.17 |
| Variables | Total No. 23 | PD-L1 Adjusted HR (95% CI) | p Value | |
|---|---|---|---|---|
| Pre-CCRT | PD-L1 H score † | |||
| Lower than median | 11 | 1 | ||
| Equal and higher than median | 12 | 3.46 (1.13–10.54) | 0.03 | |
| Gender | ||||
| Male | 22 | 1 | ||
| Female | 1 | 2.59 × 10−17 (0) | 1.00 | |
| Age | 23 | 1.04 (0.98–1.11) | 0.2 | |
| Post-CCRT | PD-L1 H score † | |||
| Lower than median | 14 | 1 | ||
| Equal and higher than median | 9 | 1.31 (0.50–3.45) | 0.58 | |
| Gender | ||||
| Male | 22 | 1 | ||
| Female | 1 | 6.50 × 10−17 (0) | 1.000 | |
| Age | 23 | 1.06 (0.99–1.14) | 0.099 |
| Total No. 15 | CD8 Adjusted HR (95% CI) | p Value | ||
|---|---|---|---|---|
| Pre-CCRT | CD8 density † | |||
| Lower than median | 7 | 1 | ||
| Equal and higher than median | 8 | 0.66 (0.18–2.35) | 0.52 | |
| Gender | ||||
| Male | 14 | 1 | ||
| Female | 1 | 2.45 × 10−17 (0) | 1.00 | |
| Age | 15 | 1.10 (0.99–1.21) | 0.07 | |
| Post-CCRT | CD8 density ‡ | |||
| Lower than median | 7 | 1 | ||
| Equal and higher than median | 8 | 4.89 (0.96–24.92) | 0.06 | |
| Gender | ||||
| Male | 14 | 1 | ||
| Female | 1 | 2.20 × 10−17 (0) | 1.00 | |
| Age | 15 | 1.11 (1.01–1.22) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, W.-C.; Wu, C.-C.; Chen, Y.-H.; Lee, J.-Y.; Wang, Y.-K.; Wu, N.-S.; Wu, M.-T.; Wu, I.-C. Change in PD-L1 and CD8 Expression after Chemoradiotherapy for Esophageal Squamous Cell Carcinoma. Biomedicines 2022, 10, 1888. https://doi.org/10.3390/biomedicines10081888
Chen W-C, Wu C-C, Chen Y-H, Lee J-Y, Wang Y-K, Wu N-S, Wu M-T, Wu I-C. Change in PD-L1 and CD8 Expression after Chemoradiotherapy for Esophageal Squamous Cell Carcinoma. Biomedicines. 2022; 10(8):1888. https://doi.org/10.3390/biomedicines10081888
Chicago/Turabian StyleChen, Wei-Chung, Chun-Chieh Wu, Yi-Hsun Chen, Jui-Ying Lee, Yao-Kuang Wang, Nian-Siou Wu, Ming-Tsang Wu, and I-Chen Wu. 2022. "Change in PD-L1 and CD8 Expression after Chemoradiotherapy for Esophageal Squamous Cell Carcinoma" Biomedicines 10, no. 8: 1888. https://doi.org/10.3390/biomedicines10081888