
Adjuvant Chemoradiotherapy Associated with Improved Overall Survival in Resected Esophageal Squamous Cell Carcinoma after Neoadjuvant Chemoradiotherapy in Intensity-Modulated Radiotherapy Era

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
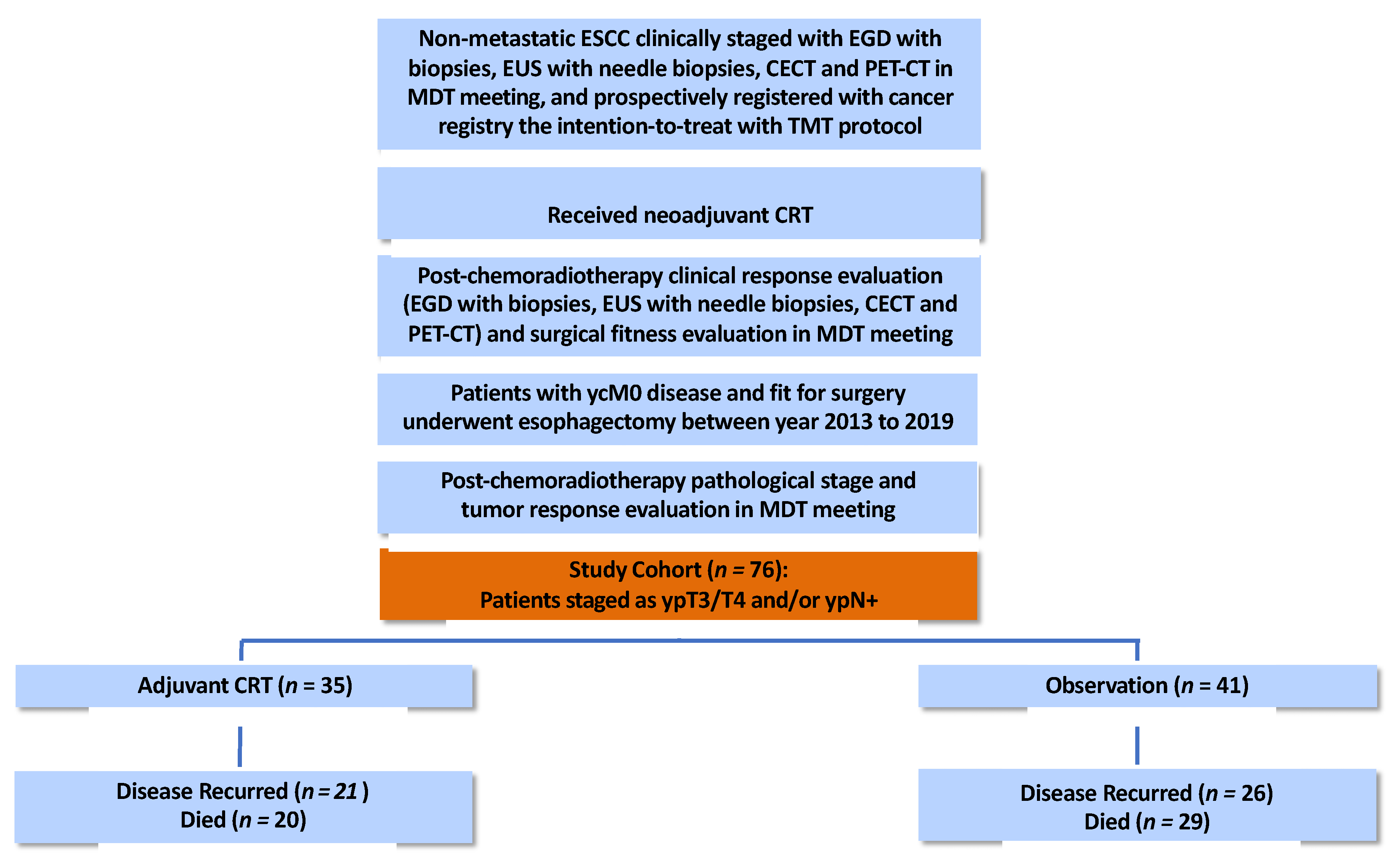
2.1. Study Participants
2.2. Treatment Protocols
2.3. Post-Treatment Surveillance
2.4. Statistical Analyses
3. Results
3.1. Patient and Treatment Characteristics
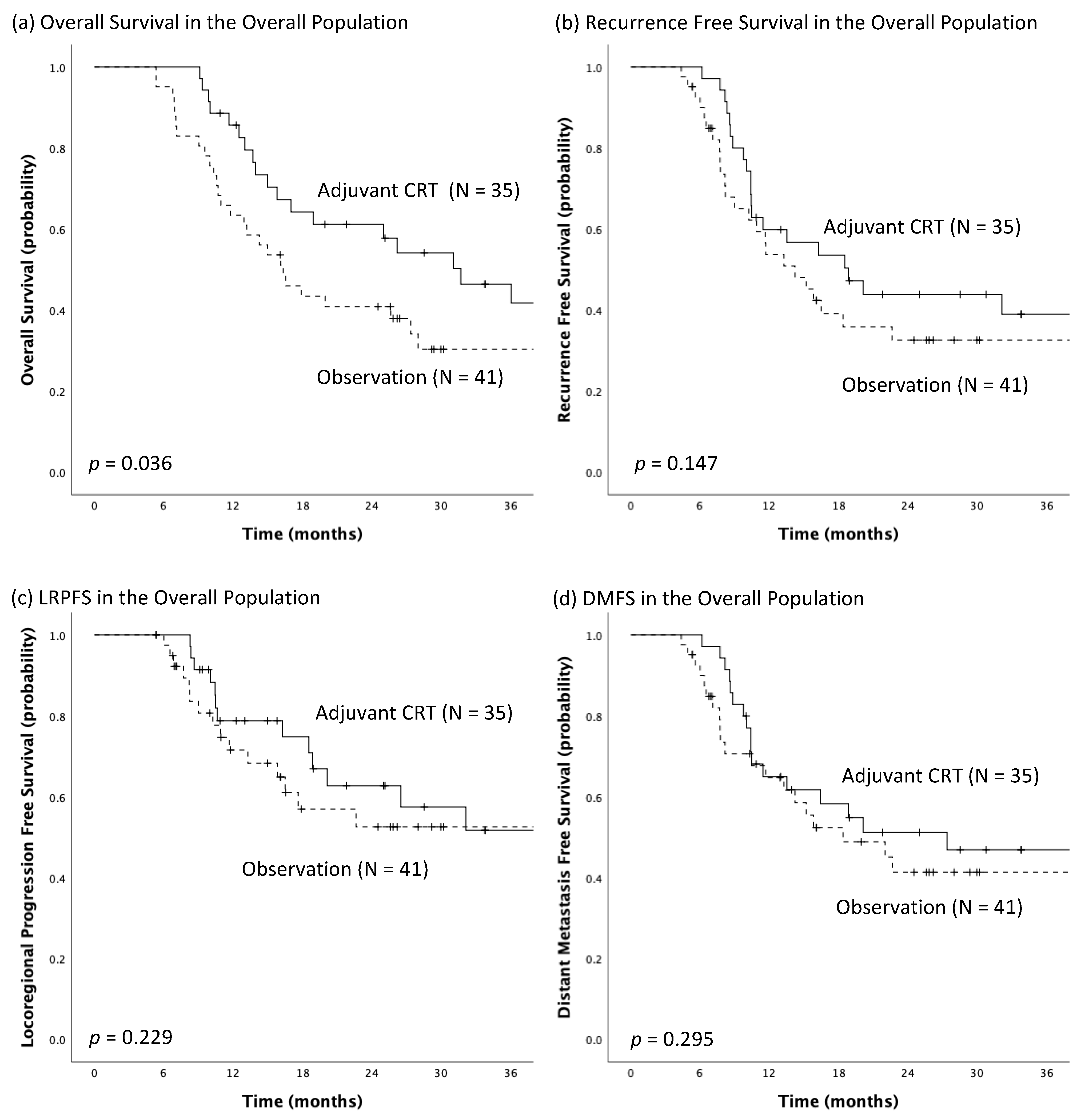
3.2. Survival Analyses
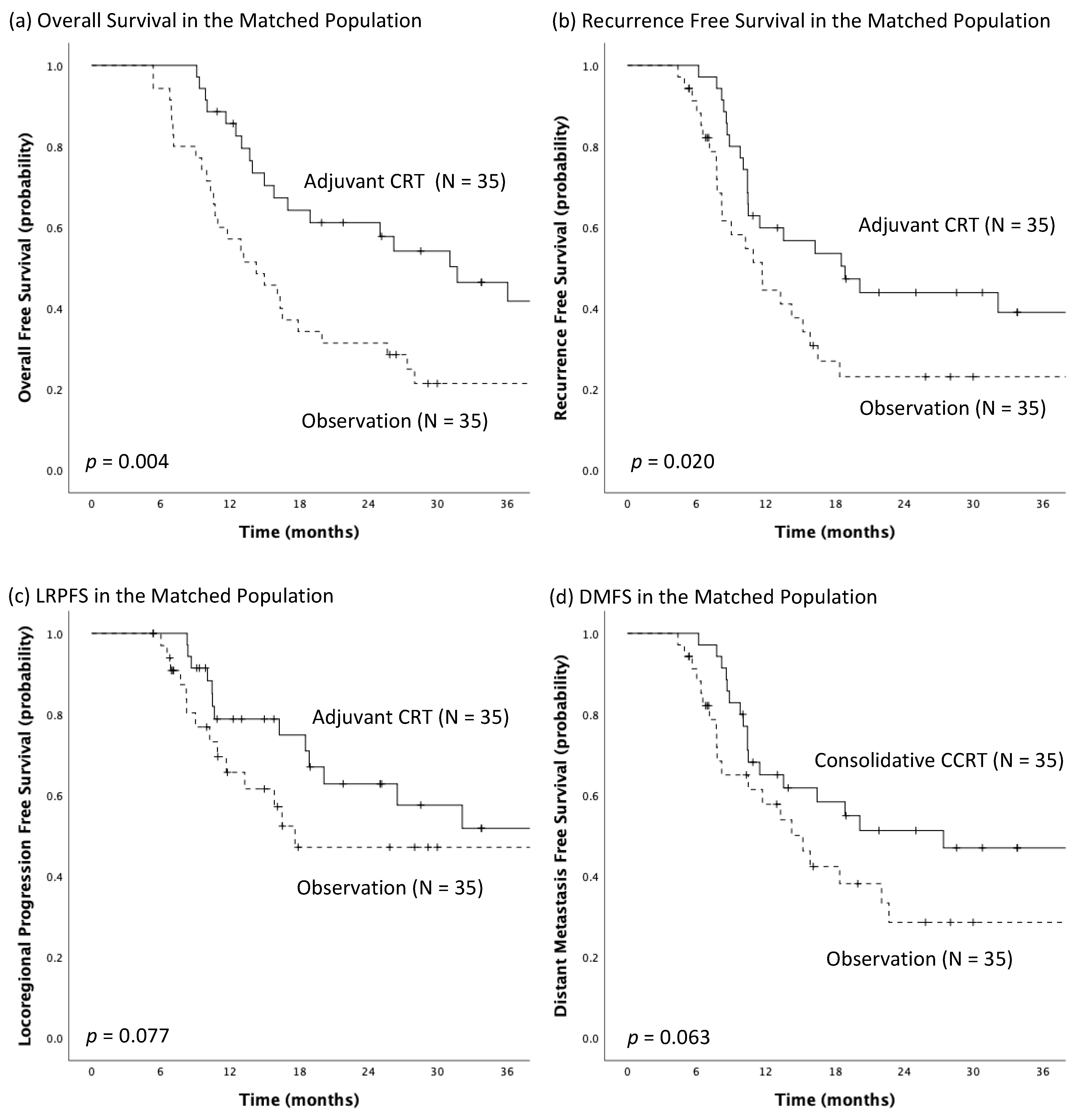
3.3. Propensity Score Matching Analyses
3.4. Univariable and Multivariable Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Arnold, M.; Soerjomataram, I.; Ferlay, J.; Forman, D. Global incidence of oesophageal cancer by histological subtype in 2012. Gut 2015, 64, 381–387. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, M.; Tachimori, Y.; Oyama, T.; Toh, Y.; Matsubara, H.; Ueno, M.; Kono, K.; Uno, T.; Ishihara, R.; Muro, K.; et al. Comprehensive registry of esophageal cancer in Japan, 2013. Esophagus 2021, 18, 1–24. [Google Scholar] [CrossRef]
- Lai, W.W.; Lin, C.N.; Chang, C.C.; Wang, J.D. Lifetime risks, expected years of life lost, and cost-per-life year of esophageal cancer in Taiwan. Sci. Rep. 2020, 10, 3722. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, J.; van Lanschot, J.J.B.; Hulshof, M.C.C.M.; van Hagen, P.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; van Laarhoven, H.W.M.; Nieuwenhuijzen, G.A.P.; Hospers, G.A.P.; Bonenkamp, J.J.; et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): Long-term results of a randomised controlled trial. Lancet Oncol. 2015, 16, 1090–1098. [Google Scholar] [CrossRef]
- van Hagen, P.; Hulshof, M.C.C.M.; van Lanschot, J.J.B.; Steyerberg, E.W.; Henegouwen, M.I.v.B.; Wijnhoven, B.P.L.; Richel, D.J.; Nieuwenhuijzen, G.A.P.; Hospers, G.A.P.; Bonenkamp, J.J.; et al. Preoperative Chemoradiotherapy for Esophageal or Junctional Cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar] [CrossRef] [Green Version]
- Shah, M.A.; Kennedy, E.B.; Catenacci, D.V.; Deighton, D.C.; Goodman, K.A.; Malhotra, N.K.; Willett, C.; Stiles, B.; Sharma, P.; Tang, L.; et al. Treatment of Locally Advanced Esophageal Carcinoma: ASCO Guideline. J. Clin. Oncol. 2020, 38, 2677–2694. [Google Scholar] [CrossRef]
- Rice, T.W.; Lerut, T.E.; Orringer, M.B.; Chen, L.Q.; Hofstetter, W.L.; Smithers, B.M.; Rusch, V.W.; van Lanschot, J.; Chen, K.N.; Davies, A.R.; et al. Worldwide Esophageal Cancer Collaboration: Neoadjuvant pathologic staging data. Dis. Esophagus 2016, 29, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.J.; Ajani, J.A.; Kuzdzal, J.; Zander, T.; Van Cutsem, E.; Piessen, G.; Mendez, G.; Feliciano, J.; Motoyama, S.; Lièvre, A.; et al. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. N. Engl. J. Med. 2021, 384, 1191–1203. [Google Scholar] [CrossRef]
- Shah, M.A.; Hofstetter, W.L.; Kennedy, E.B. Immunotherapy in Patients With Locally Advanced Esophageal Carcinoma: ASCO Treatment of Locally Advanced Esophageal Carcinoma Guideline Rapid Recommendation Update. J. Clin. Oncol. 2021, 39, 3182–3184. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Samarasinghe, Y.; Lee, M.H.; Thiru, L.; Shargall, Y.; Finley, C.; Hanna, W.; Levine, O.; Juergens, R.; Agzarian, J. Role of Adjuvant Therapy in Esophageal Cancer Patients After Neoadjuvant Therapy and Esophagectomy: A Systematic Review and Meta-analysis. Ann. Surg. 2022, 275, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.H.; Hung, T.M.; Chang, Y.C.; Hsieh, C.H.; Shih, M.C.; Huang, S.M.; Yang, C.K.; Chang, C.F.; Chan, S.C.; Yap, W.K. Prognostic Value of Lymph Node-to-Primary Tumor Standardized Uptake Value Ratio in Esophageal Squamous Cell Carcinoma Treated with Definitive Chemoradiotherapy. Cancers 2020, 12, 607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yap, W.K.; Chang, Y.C.; Hsieh, C.H.; Chao, Y.K.; Chen, C.C.; Shih, M.C.; Hung, T.M. Favorable versus unfavorable prognostic groups by post-chemoradiation FDG-PET imaging in node-positive esophageal squamous cell carcinoma patients treated with definitive chemoradiotherapy. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Yap, W.K.; Chang, Y.C.; Tseng, C.K.; Hsieh, C.H.; Chao, Y.K.; Su, P.J.; Hou, M.M.; Yang, C.K.; Pai, P.C.; Lin, C.R.; et al. Predictive value of nodal maximum standardized uptake value of pretreatment [18F]fluorodeoxyglucose positron emission tomography imaging in patients with esophageal cancer. Dis. Esophagus 2017, 30, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Clark, T.G.; Bradburn, M.J.; Love, S.B.; Altman, D.G. Survival Analysis Part I: Basic concepts and first analyses. Br. J. Cancer 2003, 89, 232–238. [Google Scholar] [CrossRef] [Green Version]
- Semenkovich, T.R.; Subramanian, M.; Yan, Y.; Hofstetter, W.L.; Correa, A.M.; Cassivi, S.D.; Inra, M.L.; Stiles, B.M.; Altorki, N.K.; Chang, A.C.; et al. Adjuvant Therapy for Node-Positive Esophageal Cancer After Induction and Surgery: A Multisite Study. Ann. Thorac. Surg. 2019, 108, 828–836. [Google Scholar] [CrossRef]
- Agarwal, G.G. Statistics for surgeons-understanding survival analysis. Indian J. Surg. Oncol. 2012, 3, 208–214. [Google Scholar] [CrossRef] [Green Version]
- Blum Murphy, M.; Xiao, L.; Patel, V.R.; Maru, D.M.; Correa, A.M.; F, G.A.; Liao, Z.; Komaki, R.; Lin, S.H.; Skinner, H.D.; et al. Pathological complete response in patients with esophageal cancer after the trimodality approach: The association with baseline variables and survival-The University of Texas MD Anderson Cancer Center experience. Cancer 2017, 123, 4106–4113. [Google Scholar] [CrossRef]
- Depypere, L.P.; Vervloet, G.; Lerut, T.; Moons, J.; De Hertogh, G.; Sagaert, X.; Coosemans, W.; Van Veer, H.; Nafteux, P.R. ypT0N+: The unusual patient with pathological complete tumor response but with residual lymph node disease after neoadjuvant chemoradiation for esophageal cancer, what’s up? J. Thorac. Dis. 2018, 10, 2771–2778. [Google Scholar] [CrossRef]
- Ardalan, B.; Spector, S.A.; Livingstone, A.S.; Franceschi, D.; Mezentsev, D.; Lima, M.; Bowen-Wells, C.P.; Sparling, L.; Avisar, E.; Sapp, M.; et al. Neoadjuvant, surgery and adjuvant chemotherapy without radiation for esophageal cancer. Jpn. J. Clin. Oncol. 2007, 37, 590–596. [Google Scholar] [CrossRef]
- Huang, Z.; Li, S.; Yang, X.; Lu, F.; Huang, M.; Zhang, S.; Xiong, Y.; Zhang, P.; Si, J.; Ma, Y.; et al. Long-term survival of patients with locally advanced esophageal squamous cell carcinoma receiving esophagectomy following neoadjuvant chemotherapy: A cohort study. Cancer Manag. Res. 2019, 11, 1299–1308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruhstaller, T.; Thuss-Patience, P.; Hayoz, S.; Schacher, S.; Knorrenschild, J.R.; Schnider, A.; Plasswilm, L.; Budach, W.; Eisterer, W.; Hawle, H.; et al. Neoadjuvant chemotherapy followed by chemoradiation and surgery with and without cetuximab in patients with resectable esophageal cancer: A randomized, open-label, phase III trial (SAKK 75/08). Ann. Oncol. 2018, 29, 1386–1393. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.M.; Hsu, F.M.; Lin, C.C.; Hsu, C.H.; Cheng, J.C.; Lee, J.M. Do We Need to Add Postoperative Radiotherapy in Patients Undergoing Trimodality Therapy for Esophageal Squamous Cell Carcinoma with Positive Lymph Nodes Disease? Dig. Surg. 2018, 35, 104–110. [Google Scholar] [CrossRef]
- Saeed, N.A.; Mellon, E.A.; Meredith, K.L.; Hoffe, S.E.; Shridhar, R.; Frakes, J.; Fontaine, J.P.; Pimiento, J.M.; Kothari, N.; Almhanna, K. Adjuvant chemotherapy and outcomes in esophageal carcinoma. J. Gastrointest Oncol. 2017, 8, 816–824. [Google Scholar] [CrossRef] [Green Version]
- Mokdad, A.A.; Yopp, A.C.; Polanco, P.M.; Mansour, J.C.; Reznik, S.I.; Heitjan, D.F.; Choti, M.A.; Minter, R.R.; Wang, S.C.; Porembka, M.R. Adjuvant Chemotherapy vs Postoperative Observation Following Preoperative Chemoradiotherapy and Resection in Gastroesophageal Cancer: A Propensity Score-Matched Analysis. JAMA Oncol. 2018, 4, 31–38. [Google Scholar] [CrossRef]
- Luc, G.; Vendrely, V.; Terrebonne, E.; Chiche, L.; Collet, D. Neoadjuvant chemoradiotherapy improves histological results compared with perioperative chemotherapy in locally advanced esophageal adenocarcinoma. Ann. Surg. Oncol. 2015, 22, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Hoeppner, J.; Zirlik, K.; Brunner, T.; Bronsert, P.; Kulemann, B.; Sick, O.; Marjanovic, G.; Hopt, U.T.; Makowiec, F. Multimodal treatment of locally advanced esophageal adenocarcinoma: Which regimen should we choose? Outcome analysis of perioperative chemotherapy versus neoadjuvant chemoradiation in 105 patients. J. Surg. Oncol. 2014, 109, 287–293. [Google Scholar] [CrossRef]
- Hsu, H.Y.; Chao, Y.K.; Hsieh, C.H.; Wen, Y.W.; Chang, H.K.; Tseng, C.K.; Liu, Y.H. Postoperative Adjuvant Therapy Improves Survival in Pathologic Nonresponders after Neoadjuvant Chemoradiation for Esophageal Squamous Cell Carcinoma: A Propensity-Matched Analysis. Ann. Thorac. Surg. 2016, 102, 1687–1693. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Adjuvant CRT (n = 35) | Observation (n = 41) | p-Value |
|---|---|---|---|
| Age, years | 0.357 | ||
| Median (IQR) | 51.0 (46.0–56.0) | 54.0 (51.5–62.0) | |
| Male Sex, n (%) | 35 (100%) | 40 (97.6%) | 1.000 |
| ECOG Performance Status, n (%) | 0.327 | ||
| 0 | 7 (20.0%) | 4 (9.8%) | |
| 1 | 28 (80.0%) | 37 (90.2%) | |
| Initial Tumor Length, cm | 1.000 | ||
| Median (IQR) | 6.0 (5.0–7.2) | 5.3 (4.0–7.1) | |
| Tumor Location, n (%) | 0.991 | ||
| Upper | 6 (17.1%) | 7 (17.1%) | |
| Middle | 15 (42.9%) | 17 (41.5%) | |
| Lower | 14 (40.0%) | 17 (41.5%) | |
| Pretreatment Clinical Stage | 0.200 | ||
| II | 1 (2.9%) | 2 (4.9%) | |
| III | 30 (85.7%) | 28 (68.3%) | |
| IVA | 4 (11.4%) | 11 (26.8%) | |
| Neoadjuvant Chemotherapy | 0.800 | ||
| Carboplatin */Paclitaxel | 26 (74.3%) | 29 (70.7%) | |
| Cisplatin/5-FU | 9 (25.7%) | 12 (29.3%) | |
| Number of Cycles of Neoadjuvant Chemotherapy, Median (IQR) | |||
| Carboplatin */Paclitaxel | 6.0 (5.0–6.0) | 5.0 (5.0–6.0) | 0.684 |
| Cisplatin/5-FU | 2.0 (2.0–2.5) | 2.0 (2.0–2.0) | 1.000 |
| Neoadjuvant RT dose, cGy | |||
| Median (IQR) | 4500 (4500–4500) | 4500 (4320–4500) | 0.456 |
| ypT classification, n (%) | 0.020 | ||
| 0 | 2 (5.7%) | 7 (17.1%) | |
| 1 | 1 (2.9%) | 5 (12.2%) | |
| 2 | 1 (2.9%) | 6 (14.6%) | |
| 3 | 31 (88.6%) | 23 (56.1%) | |
| ypN classification, n (%) | 0.391 | ||
| 0 | 16 (45.7%) | 19 (46.3%) | |
| 1 | 12 (34.3%) | 19 (46.3%) | |
| 2 | 5 (14.3%) | 2 (4.9%) | |
| 3 | 2 (5.7%) | 1 (2.4%) | |
| ypStage, n (%) | 0.763 | ||
| II | 16 (45.7%) | 19 (46.3%) | |
| III | 17 (48.6%) | 21 (51.2%) | |
| IVA | 2 (5.7%) | 1 (2.4%) | |
| Resection margin, n (%) | 0.206 | ||
| R0 | 27 (77.1%) | 37 (90.2%) | |
| R1 | 8 (22.9%) | 4 (9.8%) | |
| Number of Lymph Nodes Resected | 1.000 | ||
| Median (IQR) | 25 (20–33) | 28 (17–35) | |
| Number of Positive Lymph Nodes | 0.140 | ||
| Median (IQR) | 1 (0–2) | 1 (0–1) | |
| Mandard Tumor Regression Grade, n (%) | 0.234 | ||
| 1–2 (i.e., good pathologic response) | 9 (25.7%) | 16 (39%) | |
| 3–4 (i.e., poor pathologic response) | 26 (74.3%) | 25 (61%) | |
| Time to Adjuvant CRT after Surgery, months | |||
| Median (IQR) | 1.6 (1.2–2.4) | ||
| Adjuvant RT dose, cGy | |||
| Median (IQR) | 2000 (2000–2340) | ||
| Number of Cycles of adjuvant Chemotherapy #, Median (IQR) | |||
| Carboplatin */Paclitaxel | 3.0 (2.3–4.0) | ||
| Cisplatin/5-FU | 2.0 (1.0–2.0) |
| OS | RFS | ||||
|---|---|---|---|---|---|
| Clinical Characteristics | N | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Adjuvant Treatment | 0.40 (0.21, 0.74) | 0.003 | 0.52 (0.28, 0.95) | 0.035 | |
| Observation (ref) | 41 | ||||
| Adjuvant CRT | 35 | ||||
| Resection Margin | 2.18 (1.04, 4.58) | 0.040 | 2.88 (1.38, 6.02) | 0.005 | |
| R0 (ref) | 64 | ||||
| R1 | 12 | ||||
| Mandard Tumor Regression Grade | 2.77 (1.29, 5.92) | 0.009 | 2.22 (1.06, 4.64) | 0.035 | |
| 1–2 (ref) | 25 | ||||
| 3–4 | 51 | ||||
| No. of Positive Lymph Nodes | 76 | 1.33 (1.14, 1.53) | 0.001 | 1.16 (1.00, 1.34) | 0.058 |
| No. of Lymph Nodes Resected | 76 | 0.97 (0.94, 0.99) | 0.041 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yap, W.-K.; Shih, M.-C.; Chang, Y.-C.; Lin, C.-H.; Huang, S.-M.; Tsai, T.-Y.; Chang, C.-F.; Hsu, C.-C.; Tseng, C.-K.; Chen, M.-F.; et al. Adjuvant Chemoradiotherapy Associated with Improved Overall Survival in Resected Esophageal Squamous Cell Carcinoma after Neoadjuvant Chemoradiotherapy in Intensity-Modulated Radiotherapy Era. Biomedicines 2022, 10, 2989. https://doi.org/10.3390/biomedicines10112989
Yap W-K, Shih M-C, Chang Y-C, Lin C-H, Huang S-M, Tsai T-Y, Chang C-F, Hsu C-C, Tseng C-K, Chen M-F, et al. Adjuvant Chemoradiotherapy Associated with Improved Overall Survival in Resected Esophageal Squamous Cell Carcinoma after Neoadjuvant Chemoradiotherapy in Intensity-Modulated Radiotherapy Era. Biomedicines. 2022; 10(11):2989. https://doi.org/10.3390/biomedicines10112989
Chicago/Turabian StyleYap, Wing-Keen, Ming-Chieh Shih, Yu-Chen Chang, Chia-Hsin Lin, Shih-Ming Huang, Tsung-You Tsai, Ching-Fu Chang, Chih-Chung Hsu, Chen-Kan Tseng, Miao-Fen Chen, and et al. 2022. "Adjuvant Chemoradiotherapy Associated with Improved Overall Survival in Resected Esophageal Squamous Cell Carcinoma after Neoadjuvant Chemoradiotherapy in Intensity-Modulated Radiotherapy Era" Biomedicines 10, no. 11: 2989. https://doi.org/10.3390/biomedicines10112989