
The Effects of Exercise-Based Interventions on Fluid Overload Symptoms in Patients with Heart Failure: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection, Data Extraction, and Quality Appraisal
2.4. Data Synthesis
3. Results
3.1. Study Selection
3.2. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year (Country) | Allocation | Mean Age, Years | Female, % | Mean BMI, kg/m2 | Mean LVEF, % | NYHA III-IV, % | Muscle Contracted † | Intervention Duration and Frequency | Supervised ‡ | Setting | Follow-Ups | Outcomes (Measures) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alkan, et al., 2017 (Turkey) [32] | IG: 35 CG: 35 | 64.4 (12.8) | 60.7% | NR | NR | 73.2% | Respiratory | 30 min daily for 3 months | No | Home | Baseline and 3 months | 1. Dyspnea (BDI) |
| Beniaminovitz, et al., 2002 (United States) [29] | IG: 20 CG: 9 | 49.36 (3.4) | 28.0% | NR | 19.4 (1.4) | NR | Peripheral | 30 min per session, 3 sessions per week for 3 months | Yes | Hospital | 3 months | 1. Dyspnea (TDI) |
| Bosnak-Guclu, et al., 2011 (Turkey) [35] | IG: 18 CG:18 | 67.7 (9.3) | 20% | 25.9 (3.8) | 34.9 (7. 4) | 33.3% | Respiratory | 30 min daily for 6 weeks | Yes | Home and Rehabilitation center | Baseline and 1.5 months | 1. Dyspnea (MMRC); 2. Fatigue (Turkish FSS); 3. Pain (SF-36 bodily pain dimension) |
| Chen, et al., 2018 (Taiwan, China) [45] | IG: 39 CG:41 | 70.3 (13.5) | 47.5% | NR | 58.6 (15.6) | NR | Respiratory and Peripheral | 35 min per session, 3 sessions per week for 3 months | No | Home | Baseline, 1 2, and 3 months | 1. Fatigue (Chinese PFS) |
| Corvera-Tindel, et al., 2004 (United States) [39] | IG: 42 CG: 37 | 62.6 (10.6) | 1.3% | 29.5 (6.3) | 27 (8.8) | 19% | Peripheral | 10–60 min per session, 5 sessions per week for 3 months | No | Home | 3 months | 1. Dyspnea (DFI) |
| Hossein Pour, et al., 2020 (Iran) [33] | IG: 49 CG: 49 | 56.6 (9.2) | 47.6% | 25.7 (4.7) | 33.1 (5.3) | 61.9% | Respiratory | 30 min daily for 6 weeks | Yes | Home and rehabilitation center | Baseline and 1.5 months | 1. Dyspnea (MMRC); 2. Fatigue (FSS) |
| Jena, et al., 2020 (India) [40] | IG: 20 CG: 20 | NR | 37.5% | NR | NR | NR | Peripheral | 30 min daily for 1 month | Yes | Home and hospital | 1 month | 1. Edema (Edema grading scale) 2. Pain (Numeric pain rating scale) |
| Jin and Lee, 2016 (Korea) [41] | IG: 32 CG: 28 | 58 (12) | 26.8% | NR | 31.2 (6.9) | 12.2% | Peripheral | 50 min per session, 5 sessions per week for 3 months | Yes | Home | Baseline and 3 months | 1. Dyspnea (DFI) |
| Klocek, et al., 2005 (Poland) [31] | IG (A): 14 IG (B): 14 CG: 14 | 55.9 (8.1) | 0% | 27 (3.9) | 33.2 (3.8) | 57.1% | Peripheral | 25 min per session, 3 sessions per week for 6 months | Yes | Rehabilitation center | Baseline and 6 months | 1. Subjective symptoms (SSA-P) |
| Norman, et al., 2020 (United States) [34] | IG: 102 CG: 102 | 60.4 (11.5) | 44.6% | 34.9 (8.2) | 39.9 (13.1) | 36.8% | Peripheral | 150 min per week for 18 months | Yes | Rehabilitation center | Baseline, 6, 12 and 18 months | 1. Fatigue (PROMIS-29) |
| Pozehl, et al., 2008 (United States) [42] | IG: 16 CG: 7 | 66.2 (10.2) | 9.5% | 26.9 (5.6) | 28.4 (7.3) | 61.9% | Peripheral | 60 min per session, 3 sessions per week for 6 months | Yes | Rehabilitation center | Baseline, 3 and 6 months | 1. Dyspnea (Dyspnea Index) 2. Fatigue (PFS) |
| Pozehl, et al., 2010 (United States) [43] | IG: 22 CG: 20 | 59.9 (13.8) | 45.5% | NR | 32.7 (6.1) | 45.2% | Peripheral | 60 min per session, 3 sessions per week for 6 months | Yes | Rehabilitation center | Baseline and 3 months | 1. Dyspnea (DFI) |
| Seo, et al., 2016 (United States) [36] | IG: 18 CG: 18 | 65.9 (12.4) | 28.6% | 31.1 (6.3) | 37.1 (18.6) | 52.3% | Respiratory | 15 min per session, two sessions daily, at least 5 days per week for 2 months | No | Home | Baseline, 2 and 5 months | 1. Dyspnea (Items from KCCQ; Dyspnea with ADL; Dyspnea with physical functioning) |
| Wall, et al., 2010 (United States) [44] | IG: 9 CG: 10 | 69.7 (4.1) | 42.1% | NR | NR | NR | Peripheral | 15 min per session, 3 sessions per week for 12 months | Yes | Home | Baseline, 6 and 12 months | 1. Dyspnea (CHQ Subscale); 2. Fatigue (CHQ Subscale) |
| Weiner, et al., 1999 (Israel) [37] | IG: 10 CG: 10 | 65 (4.4) | 10% | NR | 23.8 (2.2) | NR | Respiratory | 60 min daily, 6 times per week for 3 months | Yes | Hospital | Baseline and 3 months | 1. Dyspnea (Dyspnea Index) |
| Willenheimer, et al., 1998 and 2001 Sweden) [38,46] | IG: 23 CG: 27 | 64 (7.4) | 29% | NR | 35.6 (10.9) | 49.0% | Peripheral | 45 min per session, three sessions per week for 4 months | Yes | Rehabilitation center | Baseline, 4 and 10 months | 1. Dyspnea (DFI) |
| Yu, et al., 2007 (Hong Kong, China) [30] | IG: 79 CG: 79 | 76.2 (7.8) | 50.4% | NR | NR | 37.2% | Peripheral | 60 min per session, 2 sessions per week for 14 weeks | No | Home and hospital | Baseline, 2 and 3.5 months | 1. Dyspnea (CHQ Subscale); 2. Fatigue (CHQ Subscale) |
3.3. Risk of Bias in Studies
3.4. Intervention Effect on Dyspnea
3.5. Intervention Effect on Edema
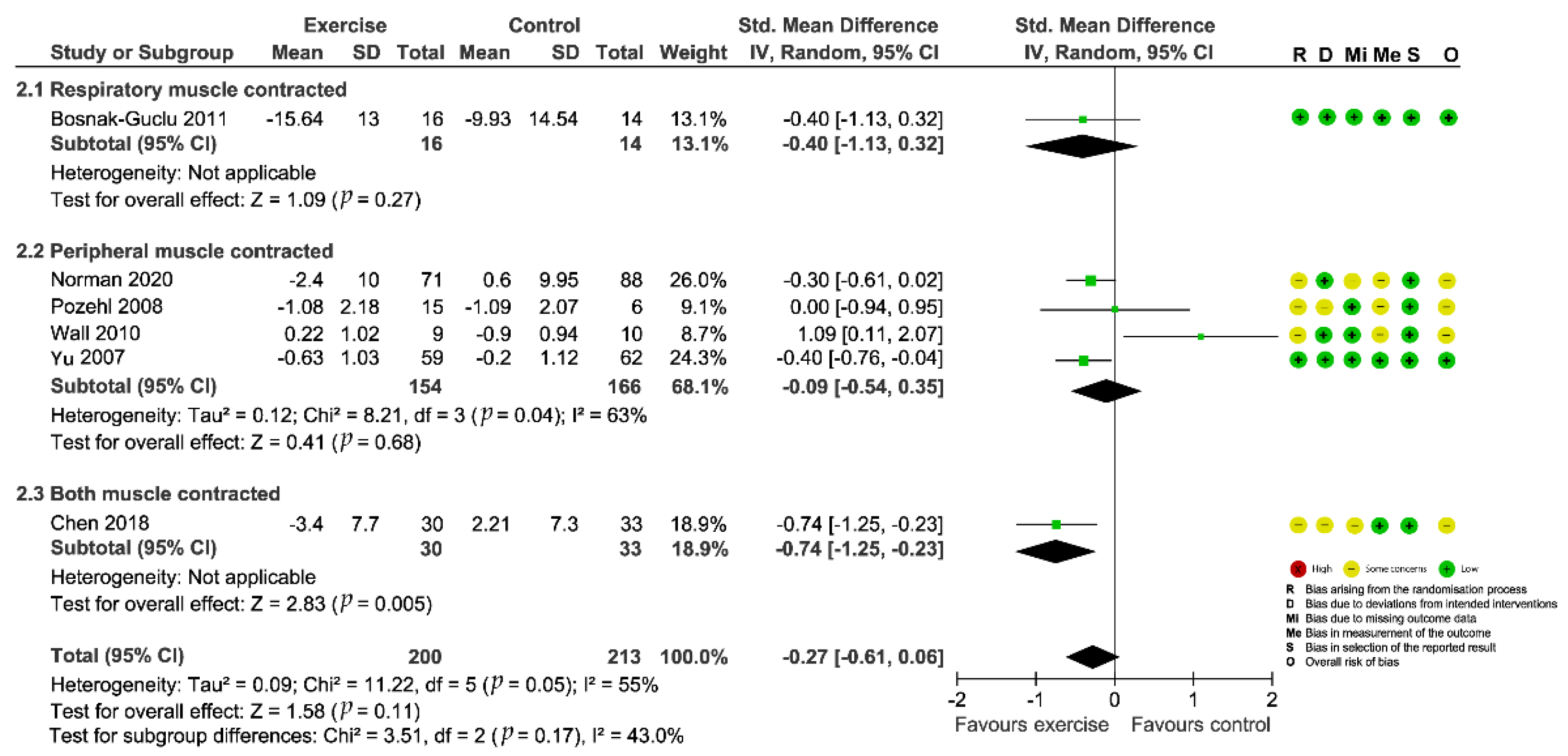
3.6. Intervention Effect on Fatigue
3.7. Intervention Effect on Other Fluid Overload Symptoms
4. Discussion
Limitations of Existing Literature and Strengths of The Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Savarese, G.; Lund, L.H. Global public health burden of heart failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Miller, W.L. Fluid volume overload and congestion in heart failure: Time to reconsider pathophysiology and how volume is assessed. Circ. Heart Fail. 2016, 9, e002922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellicori, P.; Kaur, K.; Clark, A.L. Fluid management in patients with chronic heart failure. Card. Fail. Rev. 2015, 1, 90–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.W.; Jeng, Y.J.; Huang, L.H. Development and testing of a scale to assess fluid overload symptoms. Appl. Nurs. Res. 2015, 28, 206–209. [Google Scholar] [CrossRef] [PubMed]
- Ambrosy, A.P.; Pang, P.S.; Khan, S.; Konstam, M.A.; Fonarow, G.C.; Traver, B.; Maggioni, A.P.; Cook, T.; Swedberg, K.; Burnett, J.C., Jr.; et al. Clinical course and predictive value of congestion during hospitalization in patients admitted for worsening signs and symptoms of heart failure with reduced ejection fraction: Findings from the EVEREST trial. Eur. Heart J. 2013, 34, 835–843. [Google Scholar] [CrossRef] [Green Version]
- Cooper, L.B.; Lippmann, S.J.; DiBello, J.R.; Gorsh, B.; Curtis, L.H.; Sikirica, V.; Hernandez, A.F.; Sprecher, D.L.; Laskey, W.K.; Saini, R.; et al. The burden of congestion in patients hospitalized with acute decompensated heart failure. Am. J. Cardiol. 2019, 124, 545–553. [Google Scholar] [CrossRef]
- Parrinello, G.; Greene, S.J.; Torres, D.; Alderman, M.; Bonventre, J.V.; Di Pasquale, P.; Gargani, L.; Nohria, A.; Fonarow, G.C.; Vaduganathan, M.; et al. Water and sodium in heart failure: A spotlight on congestion. Heart Fail. Rev. 2015, 20, 13–24. [Google Scholar] [CrossRef] [Green Version]
- Liszkowski, M.; Nohria, A. Rubbing salt into wounds: Hypertonic saline to assist with wolume removal in heart failure. Curr. Heart Fail. Rep. 2010, 7, 134–139. [Google Scholar] [CrossRef]
- Jain, A.; Agrawal, N.; Kazory, A. Defining the role of ultrafiltration therapy in acute heart failure: A systematic review and meta-analysis. Heart Fail. Rev. 2016, 21, 611–619. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013, 128, 1810–1852. [Google Scholar] [CrossRef]
- Houston, B.A.; Kalathiya, R.J.; Kim, D.A.; Zakaria, S. Volume overload in heart failure: An evidence-based review of strategies for treatment and prevention. Mayo Clin. Proc. 2015, 90, 1247–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scallan, J.P.; Zawieja, S.D.; Castorena-gonzalez, J.A.; Davis, M.J. Lymphatic pumping: Mechanics, mechanisms and malfunction. J. Physiol. 2016, 20, 5749–5768. [Google Scholar] [CrossRef] [PubMed]
- Aspelund, A.; Robciuc, M.R.; Karaman, S.; Makinen, T.; Alitalo, K. Lymphatic system in cardiovascular medicine. Circ. Res. 2016, 118, 515–530. [Google Scholar] [CrossRef] [PubMed]
- Klaourakis, K.; Vieira, J.; Riley, P. The evolving cardiac lymphatic vasculature in development, repair and regeneration. Nat. Rev. Cardiol. 2021, 18, 368–379. [Google Scholar] [CrossRef]
- Moore, J.E., Jr.; Bertram, C.D. Lymphatic system flows. Annu. Rev. Fluid Mech. 2018, 50, 459–482. [Google Scholar] [CrossRef]
- Itkin, M.; Rockson, S.G.; Burkhoff, D. Pathophysiology of the lymphatic system in patients with heart failure: JACC state-of-the-art review. J. Am. Coll. Cardiol. 2021, 78, 278–290. [Google Scholar] [CrossRef]
- Stücker, O.; Pons-Himbert, C.; Laemmel, E. Towards a better understanding of lymph circulation. Phlebolymphology 2008, 15, 31–36. [Google Scholar]
- The University of Texas MD Anderson Cancer Center. November 2019: Exercise and the Lymphatic System. Available online: https://www.mdanderson.org/publications/focused-on-health/exercise-and-the-lymphatic-system.h20-1592991.html (accessed on 10 April 2022).
- McGeown, J.G.; McHale, N.G.; Thornbury, K.D. The role of external compression and movement in lymph propulsion in the sheep hind limb. J. Physiol. 1987, 387, 83–93. [Google Scholar] [CrossRef]
- Coates, G.; O’Brodovich, H.; Goeree, G. Hindlimb and lung lymph flows during prolonged exercise. J. Appl. Physiol. 1993, 75, 633–638. [Google Scholar] [CrossRef]
- Havas, E.; Parviainen, T.; Vuorela, J.; Toivanen, J.; Nikula, T.; Vihko, V. Lymph flow dynamics in exercising human skeletal muscle as detected by scintography. J. Physiol. 1997, 504, 233–239. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Fu, M.R.; Fang, J.; Zheng, H.; Luo, B. The effectiveness of transitional care interventions for adult people with heart failure on patient-centered health outcomes: A systematic review and meta-analysis including dose-response relationship. Int. J. Nurs. Stud. 2021, 117, 103902. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.R.; Ridner, S.H.; Hu, S.H.; Stewart, B.R.; Cormier, J.N.; Armer, J.M. Psychosocial impact of lymphedema: A systematic review of literature from 2004 to 2011. Psychooncology 2013, 22, 1466–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, version 6.3 (updated February 2022); Cochrane: London, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 11 April 2022).
- Fu, R.; Gartlehner, G.; Grant, M.; Shamliyan, T.; Sedrakyan, A.; Wilt, T.J.; Griffith, L.; Oremus, M.; Raina, P.; Ismaila, A.; et al. Conducting quantitative synthesis when comparing medical interventions: AHRQ and the Effective Health Care Program. J. Clin. Epidemiol. 2011, 64, 1187–1197. [Google Scholar] [CrossRef] [PubMed]
- World Bank Data Team. New Country Classifications by Income Level: 2019–2020. Available online: https://blogs.worldbank.org/opendata/new-country-classifications-income-level-2019-2020 (accessed on 11 April 2022).
- Beniaminovitz, A.; Lang, C.C.; LaManca, J.; Mancini, D.M. Selective low-level leg muscle training alleviates dyspnea in patients with heart failure. J. Am. Coll. Cardiol. 2002, 40, 1602–1608. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.S.; Lee, D.T.; Woo, J. Effects of relaxation therapy on psychologic distress and symptom status in older Chinese patients with heart failure. J. Psychosom. Res. 2007, 62, 427–437. [Google Scholar] [CrossRef]
- Klocek, M.; Kubinyi, A.; Bacior, B.; Kawecka-Jaszcz, K. Effect of physical training on quality of life and oxygen consumption in patients with congestive heart failure. Int. J. Cardiol. 2005, 103, 323–329. [Google Scholar] [CrossRef]
- Alkan, H.; Uysal, H.; Enc, N.; Yigit, Z. Influence of breathing exercise education applied on patients with heart failure on dyspnoea and quality of sleep: A randomized controlled study. Int. J. Med. Res. Health Sci. 2017, 6, 107–113. [Google Scholar]
- Hossein Pour, A.H.; Gholami, M.; Saki, M.; Birjandi, M. The effect of inspiratory muscle training on fatigue and dyspnea in patients with heart failure: A randomized, controlled trial. Jpn. J. Nurs. Sci. 2020, 17, e12290. [Google Scholar] [CrossRef]
- Norman, J.F.; Kupzyk, K.A.; Artinian, N.T.; Keteyian, S.J.; Alonso, W.S.; Bills, S.E.; Pozehl, B.J. The influence of the HEART Camp intervention on hysical function, health-related quality of life, depression, axiety and fatigue in patients with heart failure. Eur. J. Cardiovasc. Nurs. 2020, 19, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Bosnak-Guclu, M.; Arikan, H.; Savci, S.; Inal-Ince, D.; Tulumen, E.; Aytemir, K.; Tokgözoglu, L. Effects of inspiratory muscle training in patients with heart failure. Respir. Med. 2011, 105, 1671–1681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, Y.; Yates, B.; LaFramboise, L.; Pozehl, B.; Norman, J.F.; Hertzog, M. A home-based diaphragmatic breathing retraining in rural patients with heart failure. West. J. Nurs. Res. 2016, 38, 270–291. [Google Scholar] [CrossRef] [PubMed]
- Weiner, P.; Waizman, J.; Magadle, R.; Berar-Yanay, N.; Pelled, B. The effect of specific inspiratory muscle training on the sensation of dyspnea and exercise tolerance in patients with congestive heart failure. Clin. Cardiol. 1999, 22, 727–732. [Google Scholar] [CrossRef]
- Willenheimer, R.; Erhardt, L.; Cline, C.; Rydberg, E.; Israelsson, B. Exercise training in heart failure improves quality of life and exercise capacity. Eur. Heart J. 1998, 19, 774–781. [Google Scholar] [CrossRef] [Green Version]
- Corvera-Tindel, T.; Doering, L.V.; Woo, M.A.; Khan, S.; Dracup, K. Effects of a home walking exercise program on functional status and symptoms in heart failure. Am. Heart J. 2004, 147, 339–346. [Google Scholar] [CrossRef]
- Jena, S.; Das, S.; Pradhan, R. A comparative study between effects of aerobic exercises and conventional treatment on selected outcomes of heart failure clients. Int. J. Res. Pharm. Sci. 2020, 11, 342–346. [Google Scholar] [CrossRef]
- Jin, H.; Lee, H. The effects of reinforced walking exercise on dyspnea-fatigue symptoms, daily activities, walking ability, and health related quality of life in heart failure patients. Korean J. Adult Nurs. 2016, 28, 266–278. [Google Scholar] [CrossRef]
- Pozehl, B.; Duncan, K.; Hertzog, M. The effects of exercise training on fatigue and dyspnea in heart failure. Eur. J. Cardiovasc. Nurs. 2008, 7, 127–132. [Google Scholar] [CrossRef]
- Pozehl, B.; Duncan, K.; Hertzog, M.; Norman, J.F. Heart failure exercise and training camp: Effects of a multicomponent exercise training intervention in patients with heart failure. Heart Lung 2010, 39, S1–S13. [Google Scholar] [CrossRef] [Green Version]
- Wall, H.K.; Ballard, J.; Troped, P.; Njike, V.Y.; Katz, D.L. Impact of home-based, supervised exercise on congestive heart failure. Int. J. Cardiol. 2010, 145, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.M.; Yu, W.C.; Hung, H.F.; Tsai, J.C.; Wu, H.Y.; Chiou, A.F. The effects of baduanjin exercise on fatigue and quality of life in patients with heart failure: A randomized controlled trial. Eur. J. Cardiovasc. Nurs. 2018, 17, 456–466. [Google Scholar] [CrossRef] [PubMed]
- Willenheimer, R.; Rydberg, E.; Cline, C.; Broms, K.; Hillberger, B.; Oberg, L.; Erhardt, L. Effects on quality of life, symptoms and daily activity 6 months after termination of an exercise training programme in heart failure patients. Int. J. Cardiol. 2001, 77, 25–31. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-Bias VISualization (Robvis): An R package and Shiny web app for visualizing Risk-of-Bias assessments. Res. Synth. Methods 2020, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Mustian, K.M.; Alfano, C.M.; Heckler, C.; Kleckner, A.S.; Kleckner, I.R.; Leach, C.R.; Mohr, D.; Palesh, O.G.; Peppone, L.J.; Piper, B.F.; et al. Comparison of pharmaceutical, psychological, and exercise treatments for cancer-related fatigue: A meta-analysis. JAMA Oncol. 2017, 3, 961–968. [Google Scholar] [CrossRef]
- Tomlinson, D.; Diorio, C.; Beyene, J.; Sung, L. Effect of exercise on cancer-related fatigue: A meta-analysis. Am. J. Phys. Med. Rehabil. 2014, 93, 675–686. [Google Scholar] [CrossRef]
- Kessels, E.; Husson, O.; van der Feltz-Cornelis, C.M. The effect of exercise on cancer-related fatigue in cancer survivors: A systematic review and meta-analysis. Neuropsychiatr. Dis. Treat. 2018, 14, 479–494. [Google Scholar] [CrossRef] [Green Version]
- Stout, N.L.; Baima, J.; Swisher, A.K.; Winters-Stone, K.M.; Welsh, J. A systematic review of exercise systematic reviews in the cancer literature (2005–2017). PM&R 2017, 9, S347–S384. [Google Scholar]
- Koshy, A.O.; Gallivan, E.R.; McGinlay, M.; Straw, S.; Drozd, M.; Toms, A.G.; Gierula, J.; Cubbon, R.M.; Kearney, M.T.; Witte, K.K. Prioritizing symptom management in the treatment of chronic heart failure. ESC Heart Fail. 2020, 7, 2193–2207. [Google Scholar] [CrossRef]
- Wu, J.; Kuang, L.; Fu, L. Effects of inspiratory muscle training in chronic heart failure patients: A systematic review and meta-analysis. Congenit. Heart Dis. 2018, 13, 194–202. [Google Scholar] [CrossRef]
- Azambuja, A.C.M.; de Oliveira, L.Z.; Sbruzzi, G. Inspiratory muscle training in patients with heart failure: What is new? Systematic review and meta-analysis. Phys. Ther. 2020, 100, 2099–2109. [Google Scholar] [CrossRef] [PubMed]
- Sadek, Z.; Salami, A.; Joumaa, W.H.; Awada, C.; Ahmaidi, S.; Ramadan, W. Best mode of inspiratory muscle training in heart failure patients: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2018, 25, 1691–1701. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.R.; Axelrod, D.; Guth, A.A.; Cartwright, F.; Qiu, Z.; Goldberg, J.D.; Kim, J.; Scagliola, J.; Kleinman, R.; Haber, J. Proactive approach to lymphedema risk reduction: A prospective study. Ann. Surg. Oncol. 2014, 21, 3481–3489. [Google Scholar] [CrossRef] [PubMed]
- Tabet, J.Y.; Meurin, P.; Driss, A.B.; Weber, H.; Renaud, N.; Grosdemouge, A.; Beauvais, F.; Cohen-Solal, A. Benefits of exercise training in chronic heart failure. Arch. Cardiovasc. Dis. 2009, 102, 721–730. [Google Scholar] [CrossRef] [Green Version]
- Havas, E.; Lehtonen, M.; Vuorela, J.; Parviainen, T.; Vihko, V. Albumin clearance from human skeletal muscle during prolonged steady-state running. Exp. Physiol. 2000, 85, 863–868. [Google Scholar] [CrossRef]
- Fu, M.R.; McTernan, M.L.; Qiu, J.M.; Ko, E.; Yazicioglu, S.; Axelrod, D.; Guth, A.; Fan, Z.; Sang, A.; Miaskowski, C.; et al. The effects of kinect-enhanced lymphatic exercise intervention on lymphatic pain, swelling, and lymph fluid level. Integr. Cancer Ther. 2021, 20, 153473542110267. [Google Scholar] [CrossRef]
- Fu, M.R.; Axelrod, D.; Guth, A.A.; Scagliola, J.; Rampertaap, K.; El-Shammaa, N.; Qiu, J.M.; McTernan, M.L.; Frye, L.; Park, C.S.; et al. A web- and mobile-based intervention for women treated for breast cancer to manage chronic pain and symptoms related to lymphedema: Results of a randomized clinical trial. JMIR Cancer 2022, 8, e29485. [Google Scholar] [CrossRef]
- Mortimer, P.S.; Levick, J.R. Cronic peripheral oedema: The critical role of the lymphatic system. Clin. Med. 2004, 4, 448–453. [Google Scholar] [CrossRef]
- American Heart Association. Heart Failure Signs and Symptoms. Available online: https://www.heart.org/en/health-topics/heart-failure/warning-signs-of-heart-failure#.W09BCtgzZmA (accessed on 11 April 2022).
- Hu, D.; Li, L.; Li, S.; Wu, M.; Ge, N.; Cui, Y.; Lian, Z.; Song, J.; Chen, H. Lymphatic system identification, pathophysiology and therapy in the cardiovascular diseases. J. Mol. Cell. Cardiol. 2019, 133, 99–111. [Google Scholar] [CrossRef]
- Greene, A.K.; Sudduth, C.L. Lower extremity lymphatic function predicted by body mass index: A lymphoscintigraphic study of obesity and lipedema. Int. J. Obes. 2021, 45, 369–373. [Google Scholar] [CrossRef]
- Fu, M.R.; Axelrod, D.; Guth, A.; McTernan, M.L.; Qiu, J.M.; Zhou, Z.; Ko, E.; Magny-Normilus, C.; Scagliola, J.; Wang, Y. The effects of obesity on lymphatic pain and swelling in breast cancer patients. Biomedicines 2021, 9, 818. [Google Scholar] [CrossRef] [PubMed]
- Sevilla-Cazes, J.; Ahmad, F.S.; Bowles, K.H.; Jaskowiak, A.; Gallagher, T.; Goldberg, L.R.; Kangovi, S.; Alexander, M.; Riegel, B.; Barg, F.K.; et al. Heart failure home management challenges and reasons for readmission: A qualitative study to understand the patient’s perspective. J. Gen. Intern. Med. 2018, 33, 1700–1707. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Dyspnea | Fatigue | |||||
|---|---|---|---|---|---|---|
| No. | Regression Coefficient (95% CI) | p Value | No. | Regression Coefficient (95% CI) | p Value | |
| Mean age (years) | 9 | 0.006 (−0.065, 0.076) | 0.85 | 6 | −0.006 (−0.143, 0.131) | 0.91 |
| Male percentage (%) | 9 | −0.001 (−0.033, 0.032) | 0.97 | 6 | 0.006 (−0.051, 0.064) | 0.78 |
| BMI (kg/m2) | 3 | - | - | 3 | - | - |
| LVEF (%) | 6 | 0.050 (−0.121, 0.221) | 0.46 | 4 | - | - |
| NYHA | 8 | −0.003 (−0.020, 0.013) | 0.62 | 5 | - | - |
| Intervention length (weeks) | 9 | 0.033 (0.003, 0.063) | 0.04 | 6 | 0.007 (−0.019, 0.034) | 0.47 |
| Intervention dose a | 9 | −0.004 (−0.033, 0.026) | 0.79 | 6 | 0.007 (−0.031, 0.046) | 0.63 |
| Supervised b | 9 | 0.091 (−0.846, 1.028) | 0.83 | 6 | 0.564 (−0.839, 1.967) | 0.33 |
| Setting | ||||||
| Home-based | 4 | 0.176 (−0.800, 1.152) | 0.68 | 2 | 0.200 (−2.140, 2.540) | 0.80 |
| Mixed settings c | 2 | −0.292 (−1.378, 0.794) | 0.54 | 2 | −0.222 (−2.485, 2.042) | 0.78 |
| Center-based d | 3 | Ref. | - | 2 | Ref. | - |
| Study quality | ||||||
| Low risk of bias | 2 | −0.307 (−1.744, 1.129) | 0.62 | 2 | Ref. | - |
| Some concerns | 6 | 0.105 (−1.203, 1.414) | 0.85 | 4 | 0.276 (−1.161, 1.714) | 0.62 |
| High risk of bias | 1 | Ref. | - | 0 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, M.R.; Li, Y.; Conway, C.; Masone, A.; Fang, J.; Lee, C. The Effects of Exercise-Based Interventions on Fluid Overload Symptoms in Patients with Heart Failure: A Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 1111. https://doi.org/10.3390/biomedicines10051111
Fu MR, Li Y, Conway C, Masone A, Fang J, Lee C. The Effects of Exercise-Based Interventions on Fluid Overload Symptoms in Patients with Heart Failure: A Systematic Review and Meta-Analysis. Biomedicines. 2022; 10(5):1111. https://doi.org/10.3390/biomedicines10051111
Chicago/Turabian StyleFu, Mei Rosemary, Yuan Li, Catherine Conway, Alessandra Masone, Jinbo Fang, and Christopher Lee. 2022. "The Effects of Exercise-Based Interventions on Fluid Overload Symptoms in Patients with Heart Failure: A Systematic Review and Meta-Analysis" Biomedicines 10, no. 5: 1111. https://doi.org/10.3390/biomedicines10051111