
The Interplay between Vitamin D, Exposure of Anticholinergic Antipsychotics and Cognition in Schizophrenia

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants and Neuropsychological Assessment
2.2. Quantification of Vitamin D Levels and Anticholinergic Drug Exposure
2.3. Statistical Analysis
- (1)
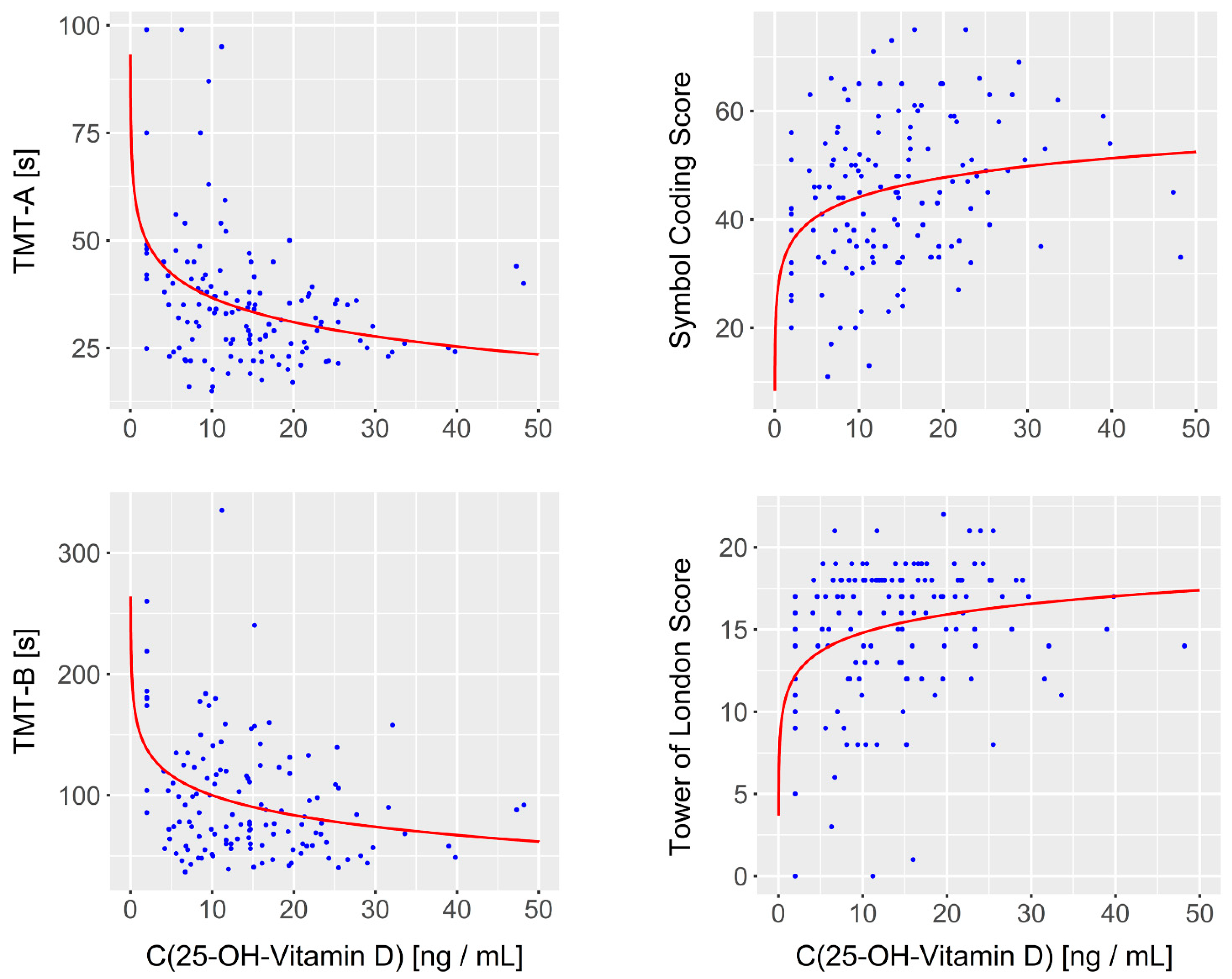
- In the first regression analysis, we assessed the impact of vitamin D on cognition. Thereto, for each of the 10 cognitive items, we separately calculated a bivariate regression model with the respective item as the dependent variable and the 25-OH-vitamin D concentration as the independent variable, yielding 10 regression models in total.
- (2)
- In the second analysis, we investigated the influence of anticholinergic drug exposure on cognition. As in the first analysis, we calculated separate bivariate regression models for each cognitive item, which served as the dependent variable, and the adjusted anticholinergic drug concentration served as the independent variable.
- (3)
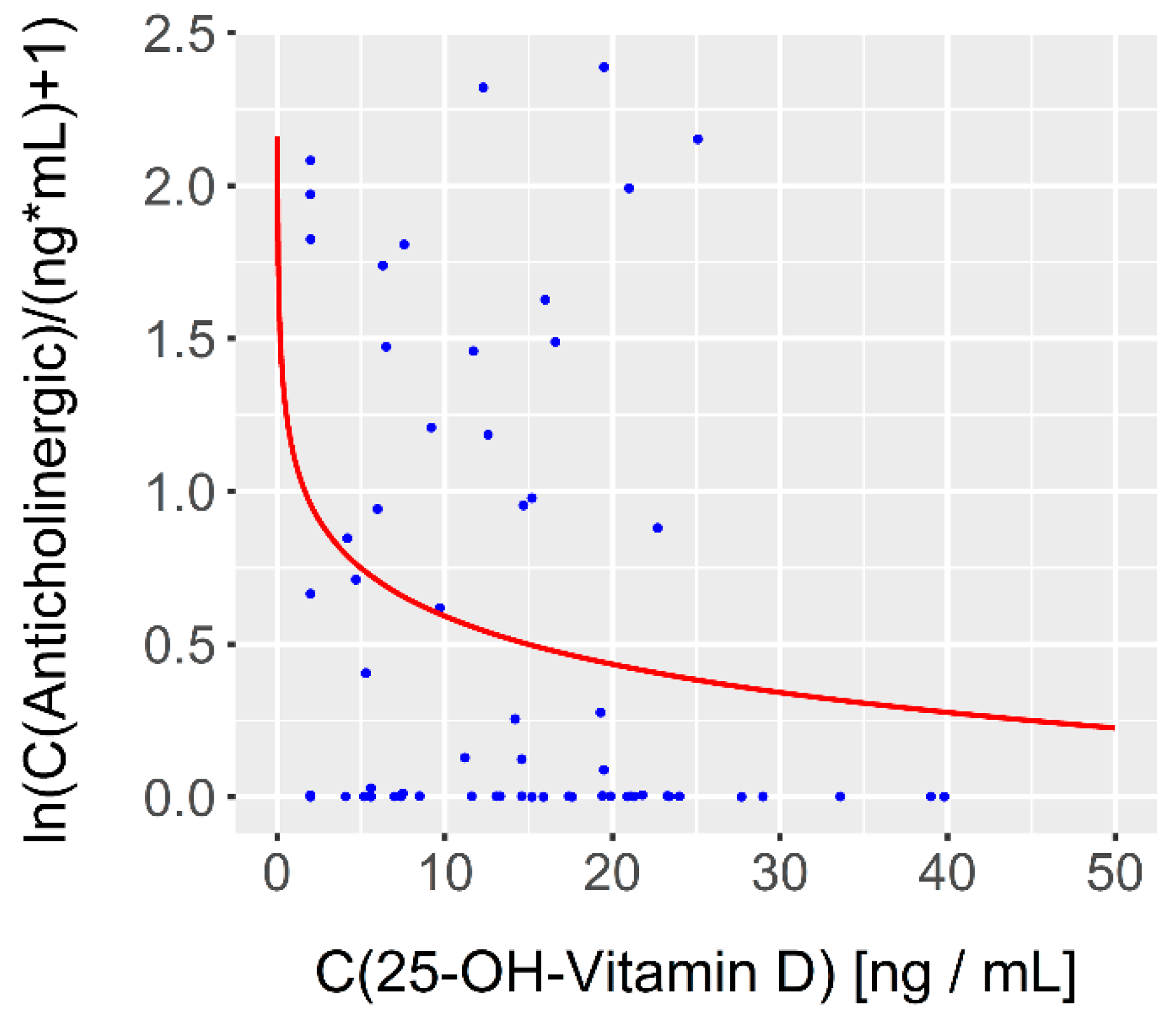
- In the third analysis, we assessed the relationship between vitamin D levels (independent variable) and anticholinergic drug exposure (dependent variable) in a single bivariate regression model. To control for potential confounders, we conducted two additional sub-analyses. In the first one, we added the number of cigarettes per day as a second independent variable to the regression model. In the second one, we removed the two patients receiving a co-treatment with the CYP1A2-inhibitor fluvoxamine.
- (4)
- In a stepwise forward regression analysis, we used one of the three following cognitive items as the dependent variables in separate sub-analyses: TMT-A, TMT-B and the Tower of London. The remaining two cognitive items, the number of cigarettes per day as well as the log-transformed vitamin D and anticholinergic levels served as the independent variables. The independent variables with the most significant impact on the respective dependent variable were sequentially added to the model until no further significant improvement of model fit could be achieved.
- (5)
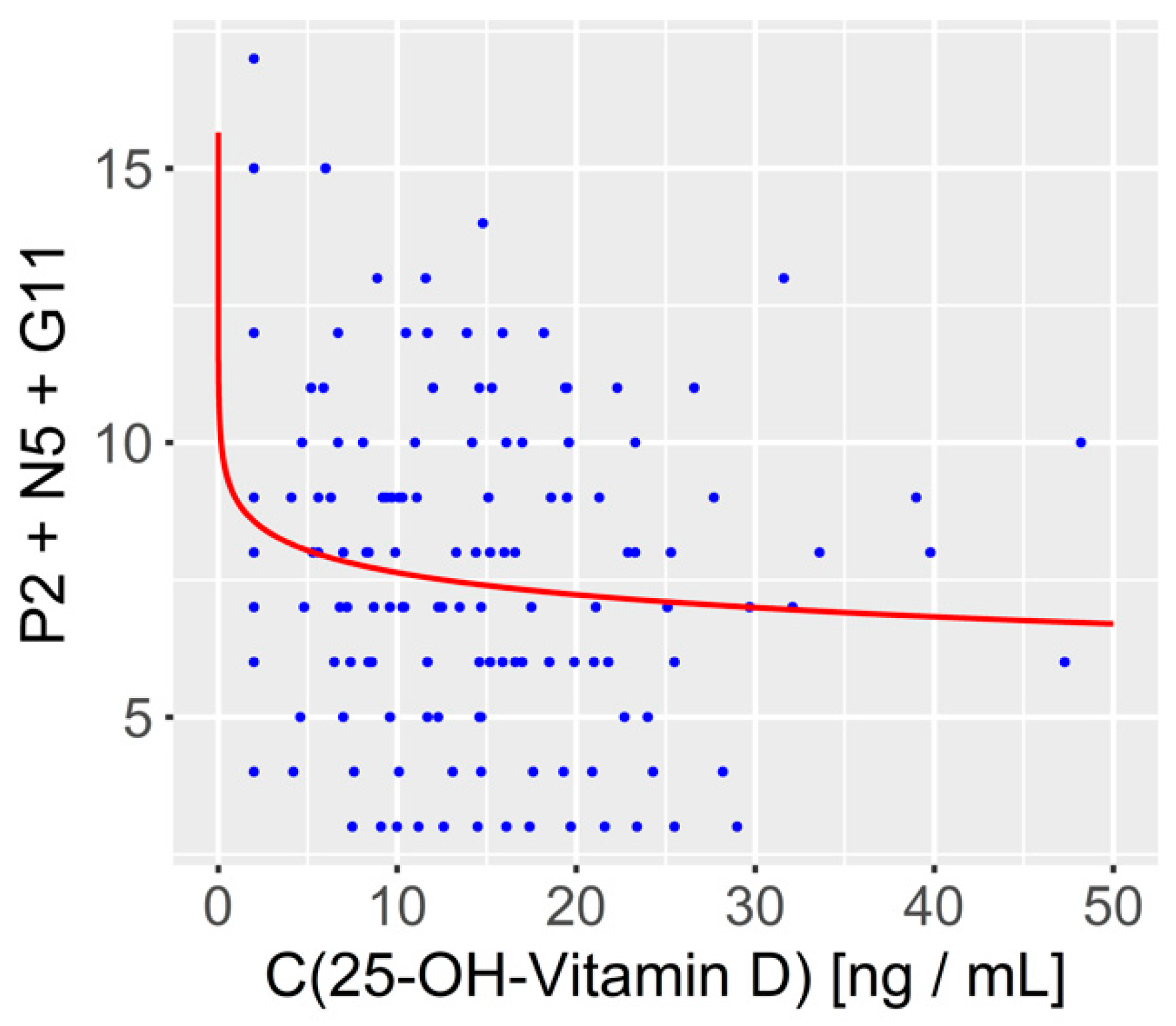
- As a further exploratory analysis, we assessed the impact of vitamin D on an alternative measure of cognition derived from a five-factor model of the positive and negative syndrome scale (PANSS) [45,46]. This five-factor model includes a “positive”, “negative”, “cognitive”, “emotional/depressed” and “excited” factor, with the cognitive factor being composed of item 2 of the positive symptom subscale, item 5 o the negative symptom subscale and item 11 of the general psychopathology subscale (P2N5G11).
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kahn, R.S.; Sommer, I.E.; Murray, R.M.; Meyer-Lindenberg, A.; Weinberger, D.R.; Cannon, T.D.; O’Donovan, M.; Correll, C.U.; Kane, J.M.; van Os, J.; et al. Schizophrenia. Nat. Rev. Dis. Primers 2015, 1, 15067. [Google Scholar] [CrossRef]
- Jauhar, S.; Johnstone, M.; McKenna, P.J. Schizophrenia. Lancet 2022, 399, 473–486. [Google Scholar] [CrossRef]
- Fett, A.K.; Viechtbauer, W.; Dominguez, M.D.; Penn, D.L.; van Os, J.; Krabbendam, L. The relationship between neurocognition and social cognition with functional outcomes in schizophrenia: A meta-analysis. Neurosci. Biobehav. Rev. 2011, 35, 573–588. [Google Scholar] [CrossRef] [Green Version]
- Heinrichs, R.W.; Zakzanis, K.K. Neurocognitive deficit in schizophrenia: A quantitative review of the evidence. Neuropsychology 1998, 12, 426–445. [Google Scholar] [CrossRef] [PubMed]
- Barch, D.M.; Ceaser, A. Cognition in schizophrenia: Core psychological and neural mechanisms. Trends Cogn. Sci. 2012, 16, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Kimoto, S.; Makinodan, M.; Kishimoto, T. Neurobiology and treatment of social cognition in schizophrenia: Bridging the bed-bench gap. Neurobiol. Dis. 2019, 131, 104315. [Google Scholar] [CrossRef] [PubMed]
- Rund, B.R. A review of longitudinal studies of cognitive functions in schizophrenia patients. Schizophr. Bull. 1998, 24, 425–435. [Google Scholar] [CrossRef]
- Tregellas, J.R.; Smucny, J.; Harris, J.G.; Olincy, A.; Maharajh, K.; Kronberg, E.; Eichman, L.C.; Lyons, E.; Freedman, R. Intrinsic hippocampal activity as a biomarker for cognition and symptoms in schizophrenia. Am. J. Psychiatry 2014, 171, 549–556. [Google Scholar] [CrossRef]
- Gaebler, A.J.; Mathiak, K.; Koten, J.W., Jr.; Konig, A.A.; Koush, Y.; Weyer, D.; Depner, C.; Matentzoglu, S.; Edgar, J.C.; Willmes, K.; et al. Auditory mismatch impairments are characterized by core neural dysfunctions in schizophrenia. Brain 2015, 138, 1410–1423. [Google Scholar] [CrossRef]
- Gaebler, A.J.; Zweerings, J.; Koten, J.W.; Konig, A.A.; Turetsky, B.I.; Zvyagintsev, M.; Mathiak, K. Impaired Subcortical Detection of Auditory Changes in Schizophrenia but Not in Major Depression. Schizophr. Bull. 2020, 46, 193–201. [Google Scholar] [CrossRef]
- Javitt, D.C. When doors of perception close: Bottom-up models of disrupted cognition in schizophrenia. Annu. Rev. Clin. Psychol. 2009, 5, 249–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Javitt, D.C.; Sweet, R.A. Auditory dysfunction in schizophrenia: Integrating clinical and basic features. Nat. Rev. Neurosci. 2015, 16, 535–550. [Google Scholar] [CrossRef] [PubMed]
- Nyatega, C.O.; Qiang, L.; Adamu, M.J.; Younis, A.; Kawuwa, H.B. Altered Dynamic Functional Connectivity of Cuneus in Schizophrenia Patients: A Resting-State fMRI Study. Appl. Sci. 2021, 11, 11392. [Google Scholar] [CrossRef]
- Shafee, R.; Nanda, P.; Padmanabhan, J.L.; Tandon, N.; Alliey-Rodriguez, N.; Kalapurakkel, S.; Weiner, D.J.; Gur, R.E.; Keefe, R.S.E.; Hill, S.K.; et al. Polygenic risk for schizophrenia and measured domains of cognition in individuals with psychosis and controls. Transl. Psychiatry 2018, 8, 78. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, A.; Kar, S.K.; Shukla, R. Cognitive Deficits in Schizophrenia: Understanding the Biological Correlates and Remediation Strategies. Clin. Psychopharmacol. Neurosci. Off. Sci. J. Korean Coll. Neuropsychopharmacol. 2018, 16, 7–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgiou, R.; Lamnisos, D.; Giannakou, K. Anticholinergic Burden and Cognitive Performance in Patients With Schizophrenia: A Systematic Literature Review. Front. Psychiatry 2021, 12, 779607. [Google Scholar] [CrossRef]
- Belvederi Murri, M.; Respino, M.; Masotti, M.; Innamorati, M.; Mondelli, V.; Pariante, C.; Amore, M. Vitamin D and psychosis: Mini meta-analysis. Schizophr. Res. 2013, 150, 235–239. [Google Scholar] [CrossRef]
- Fan, X.; Wang, J.; Song, M.; Giovannucci, E.L.; Ma, H.; Jin, G.; Hu, Z.; Shen, H.; Hang, D. Vitamin D status and risk of all-cause and cause-specific mortality in a large cohort: Results from the UK Biobank. J. Clin. Endocrinol. Metab. 2020, 105, e3606–e3619. [Google Scholar] [CrossRef]
- Bruins, J.; Jörg, F.; van den Heuvel, E.R.; Bartels-Velthuis, A.A.; Corpeleijn, E.; Muskiet, F.A.J.; Pijnenborg, G.H.M.; Bruggeman, R. The relation of vitamin D, metabolic risk and negative symptom severity in people with psychotic disorders. Schizophr. Res. 2018, 195, 513–518. [Google Scholar] [CrossRef]
- Yee, J.Y.; See, Y.M.; Abdul Rashid, N.A.; Neelamekam, S.; Lee, J. Association between serum levels of bioavailable vitamin D and negative symptoms in first-episode psychosis. Psychiatry Res. 2016, 243, 390–394. [Google Scholar] [CrossRef] [Green Version]
- Cieslak, K.; Feingold, J.; Antonius, D.; Walsh-Messinger, J.; Dracxler, R.; Rosedale, M.; Aujero, N.; Keefe, D.; Goetz, D.; Goetz, R.; et al. Low vitamin D levels predict clinical features of schizophrenia. Schizophr. Res. 2014, 159, 543–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGrath, J.J.; Eyles, D.W.; Pedersen, C.B.; Anderson, C.; Ko, P.; Burne, T.H.; Norgaard-Pedersen, B.; Hougaard, D.M.; Mortensen, P.B. Neonatal vitamin D status and risk of schizophrenia: A population-based case-control study. Arch. Gen. Psychiatry 2010, 67, 889–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eyles, D.W.; Trzaskowski, M.; Vinkhuyzen, A.A.E.; Mattheisen, M.; Meier, S.; Gooch, H.; Anggono, V.; Cui, X.; Tan, M.C.; Burne, T.H.J.; et al. The association between neonatal vitamin D status and risk of schizophrenia. Sci. Rep. 2018, 8, 17692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, X.; McGrath, J.J.; Burne, T.H.J.; Eyles, D.W. Vitamin D and schizophrenia: 20 years on. Mol. Psychiatry 2021, 26, 2708–2720. [Google Scholar] [CrossRef]
- Groves, N.J.; Kesby, J.P.; Eyles, D.W.; McGrath, J.J.; Mackay-Sim, A.; Burne, T.H. Adult vitamin D deficiency leads to behavioural and brain neurochemical alterations in C57BL/6J and BALB/c mice. Behav. Brain Res. 2013, 241, 120–131. [Google Scholar] [CrossRef] [Green Version]
- Kasatkina, L.A.; Tarasenko, A.S.; Krupko, O.O.; Kuchmerovska, T.M.; Lisakovska, O.O.; Trikash, I.O. Vitamin D deficiency induces the excitation/inhibition brain imbalance and the proinflammatory shift. Int. J. Biochem. Cell Biol. 2020, 119, 105665. [Google Scholar] [CrossRef]
- Byrne, J.H.; Voogt, M.; Turner, K.M.; Eyles, D.W.; McGrath, J.J.; Burne, T.H. The impact of adult vitamin D deficiency on behaviour and brain function in male Sprague-Dawley rats. PLoS ONE 2013, 8, e71593. [Google Scholar] [CrossRef]
- Taghizadeh, M.; Talaei, S.A.; Salami, M. Vitamin D deficiency impairs spatial learning in adult rats. Iran. Biomed. J. 2013, 17, 42–48. [Google Scholar] [CrossRef]
- Roy, N.M.; Al-Harthi, L.; Sampat, N.; Al-Mujaini, R.; Mahadevan, S.; Al Adawi, S.; Essa, M.M.; Al Subhi, L.; Al-Balushi, B.; Qoronfleh, M.W. Impact of vitamin D on neurocognitive function in dementia, depression, schizophrenia and ADHD. Front. Biosci. 2021, 26, 566–611. [Google Scholar] [CrossRef]
- Gaebler, A.J.; Finner-Prével, M.; Lammertz, S.; Schaffrath, S.; Eisner, P.; Stöhr, F.; Röcher, E.; Winkler, L.; Kaleta, P.; Lenzen, L.; et al. The negative impact of vitamin D on antipsychotic drug exposure may counteract its potential benefits in schizophrenia. Br. J. Clin. Pharmacol. 2022. [Google Scholar] [CrossRef]
- Wang, Z.; Schuetz, E.G.; Xu, Y.; Thummel, K.E. Interplay between vitamin D and the drug metabolizing enzyme CYP3A4. J. Steroid Biochem. Mol. Biol. 2013, 136, 54–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindh, J.D.; Andersson, M.L.; Eliasson, E.; Björkhem-Bergman, L. Seasonal variation in blood drug concentrations and a potential relationship to vitamin D. Drug Metab. Dispos. Biol. Fate Chem. 2011, 39, 933–937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, J.B. Effects of vitamin D supplementation in atorvastatin-treated patients: A new drug interaction with an unexpected consequence. Clin. Pharmacol. Ther. 2009, 85, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Keefe, R.S.; Goldberg, T.E.; Harvey, P.D.; Gold, J.M.; Poe, M.P.; Coughenour, L. The Brief Assessment of Cognition in Schizophrenia: Reliability, sensitivity, and comparison with a standard neurocognitive battery. Schizophr. Res. 2004, 68, 283–297. [Google Scholar] [CrossRef]
- Arbuthnott, K.; Frank, J. Trail making test, part B as a measure of executive control: Validation using a set-switching paradigm. J. Clin. Exp. Neuropsychol. 2000, 22, 518–528. [Google Scholar] [CrossRef]
- Corrigan, J.D.; Hinkeldey, N.S. Relationships between parts A and B of the Trail Making Test. J. Clin. Psychol. 1987, 43, 402–409. [Google Scholar] [CrossRef]
- Hiemke, C.; Bergemann, N.; Clement, H.W.; Conca, A.; Deckert, J.; Domschke, K.; Eckermann, G.; Egberts, K.; Gerlach, M.; Greiner, C.; et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017. Pharmacopsychiatry 2018, 51, e1. [Google Scholar] [CrossRef] [Green Version]
- Saar, E.; Beyer, J.; Gerostamoulos, D.; Drummer, O.H. The analysis of antipsychotic drugs in human matrices using LC-MS(/MS). Drug Test. Anal. 2012, 4, 376–394. [Google Scholar] [CrossRef]
- Arneson, W.L.; Arneson, D.L. Current Methods for Routine Clinical Laboratory Testing of Vitamin D Levels. Lab. Med. 2013, 44, e38–e42. [Google Scholar] [CrossRef]
- Administration UFaD. Drug Development and Drug Interactions: Table of Substrates, Inhibitors and Inducers. 2020. Available online: https://www.fda.gov/drugs/drug-interactions-labeling/drug-development-and-drug-interactions-table-substrates-inhibitors-and-inducers (accessed on 10 January 2022).
- Besnard, J.; Ruda, G.F.; Setola, V.; Abecassis, K.; Rodriguiz, R.M.; Huang, X.-P.; Norval, S.; Sassano, M.F.; Shin, A.I.; Webster, L.A.; et al. Automated design of ligands to polypharmacological profiles. Nature 2012, 492, 215–220. [Google Scholar] [CrossRef]
- Ban, T.A. Fifty years chlorpromazine: A historical perspective. Neuropsychiatr. Dis. Treat. 2007, 3, 495–500. [Google Scholar] [PubMed]
- Davis, J.M. Dose equivalence of the antipsychotic drugs. In Catecholamines and Schizophrenia; Elsevier: Amsterdam, The Netherlands, 1975; pp. 65–73. [Google Scholar]
- Wishart, D.S.; Knox, C.; Guo, A.C.; Shrivastava, S.; Hassanali, M.; Stothard, P.; Chang, Z.; Woolsey, J. DrugBank: A comprehensive resource for in silico drug discovery and exploration. Nucleic Acids Res. 2006, 34, D668–D672. [Google Scholar] [CrossRef] [PubMed]
- Wallwork, R.S.; Fortgang, R.; Hashimoto, R.; Weinberger, D.R.; Dickinson, D. Searching for a consensus five-factor model of the Positive and Negative Syndrome Scale for schizophrenia. Schizophr. Res. 2012, 137, 246–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, H.Y.; Zhao, J.M.; Wang, K.Q.; Su, X.R.; Pan, Y.F.; Guo, J.M.; Jiang, L.; Wang, Y.H.; Liu, H.Y.; Sun, S.G.; et al. High-frequency neuronavigated rTMS effect on clinical symptoms and cognitive dysfunction: A pilot double-blind, randomized controlled study in Veterans with schizophrenia. Transl. Psychiatry 2020, 10, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickinson, D.; Ramsey, M.E.; Gold, J.M. Overlooking the obvious: A meta-analytic comparison of digit symbol coding tasks and other cognitive measures in schizophrenia. Arch. Gen. Psychiatry 2007, 64, 532–542. [Google Scholar] [CrossRef] [PubMed]
- Leeson, V.C.; Barnes, T.R.; Harrison, M.; Matheson, E.; Harrison, I.; Mutsatsa, S.H.; Ron, M.A.; Joyce, E.M. The relationship between IQ, memory, executive function, and processing speed in recent-onset psychosis: 1-year stability and clinical outcome. Schizophr. Bull. 2010, 36, 400–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, K.A.; Keefe, R.S.; Lieberman, J.A.; Calikoglu, A.S.; Lansing, K.M.; Perkins, D.O. Relationship of low vitamin D status with positive, negative and cognitive symptom domains in people with first-episode schizophrenia. Early Interv. Psychiatry 2015, 9, 397–405. [Google Scholar] [CrossRef]
- Nerhus, M.; Berg, A.O.; Simonsen, C.; Haram, M.; Haatveit, B.; Dahl, S.R.; Gurholt, T.P.; Bjella, T.D.; Ueland, T.; Andreassen, O.A.; et al. Vitamin D Deficiency Associated With Cognitive Functioning in Psychotic Disorders. J. Clin. Psychiatry 2017, 78, e750–e757. [Google Scholar] [CrossRef]
- Krivoy, A.; Onn, R.; Vilner, Y.; Hochman, E.; Weizman, S.; Paz, A.; Hess, S.; Sagy, R.; Kimhi-Nesher, S.; Kalter, E.; et al. Vitamin D Supplementation in Chronic Schizophrenia Patients Treated with Clozapine: A Randomized, Double-Blind, Placebo-controlled Clinical Trial. EBioMedicine 2017, 26, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Julayanont, P.; Tangwongchai, S.; Hemrungrojn, S.; Tunvirachaisakul, C.; Phanthumchinda, K.; Hongsawat, J.; Suwichanarakul, P.; Thanasirorat, S.; Nasreddine, Z.S. The Montreal Cognitive Assessment-Basic: A Screening Tool for Mild Cognitive Impairment in Illiterate and Low-Educated Elderly Adults. J. Am. Geriatr. Soc. 2015, 63, 2550–2554. [Google Scholar] [CrossRef]
- Gurholt, T.P.; Nerhus, M.; Osnes, K.; Berg, A.O.; Andreassen, O.A.; Melle, I.; Agartz, I. Hippocampus volume reduction in psychosis spectrum could be ameliorated by vitamin D. Schizophr. Res. 2018, 199, 433–435. [Google Scholar] [CrossRef] [PubMed]
- Drocourt, L.; Ourlin, J.C.; Pascussi, J.M.; Maurel, P.; Vilarem, M.J. Expression of CYP3A4, CYP2B6, and CYP2C9 is regulated by the vitamin D receptor pathway in primary human hepatocytes. J. Biol. Chem. 2002, 277, 25125–25132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmiedlin-Ren, P.; Thummel, K.E.; Fisher, J.M.; Paine, M.F.; Lown, K.S.; Watkins, P.B. Expression of enzymatically active CYP3A4 by Caco-2 cells grown on extracellular matrix-coated permeable supports in the presence of 1alpha,25-dihydroxyvitamin D3. Mol. Pharmacol. 1997, 51, 741–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thummel, K.E.; Brimer, C.; Yasuda, K.; Thottassery, J.; Senn, T.; Lin, Y.; Ishizuka, H.; Kharasch, E.; Schuetz, J.; Schuetz, E. Transcriptional control of intestinal cytochrome P-4503A by 1alpha,25-dihydroxy vitamin D3. Mol. Pharmacol. 2001, 60, 1399–1406. [Google Scholar] [CrossRef]
- Thirumaran, R.K.; Lamba, J.K.; Kim, R.B.; Urquhart, B.L.; Gregor, J.C.; Chande, N.; Fan, Y.; Qi, A.; Cheng, C.; Thummel, K.E.; et al. Intestinal CYP3A4 and midazolam disposition in vivo associate with VDR polymorphisms and show seasonal variation. Biochem. Pharmacol. 2012, 84, 104–112. [Google Scholar] [CrossRef] [Green Version]
- Chow, E.C.; Durk, M.R.; Cummins, C.L.; Pang, K.S. 1Alpha,25-dihydroxyvitamin D3 up-regulates P-glycoprotein via the vitamin D receptor and not farnesoid X receptor in both fxr(-/-) and fxr(+/+) mice and increased renal and brain efflux of digoxin in mice in vivo. J. Pharmacol. Exp. Ther. 2011, 337, 846–859. [Google Scholar] [CrossRef] [Green Version]
- Latimer, C.S.; Brewer, L.D.; Searcy, J.L.; Chen, K.-C.; Popović, J.; Kraner, S.D.; Thibault, O.; Blalock, E.M.; Landfield, P.W.; Porter, N.M. Vitamin D prevents cognitive decline and enhances hippocampal synaptic function in aging rats. Proc. Natl. Acad. Sci. USA 2014, 111, E4359–E4366. [Google Scholar] [CrossRef] [Green Version]
- Becker, A.; Eyles, D.W.; McGrath, J.J.; Grecksch, G. Transient prenatal vitamin D deficiency is associated with subtle alterations in learning and memory functions in adult rats. Behav. Brain Res. 2005, 161, 306–312. [Google Scholar] [CrossRef]
- Ribeiro-Santos, A.; Lucio Teixeira, A.; Salgado, J.V. Evidence for an immune role on cognition in schizophrenia: A systematic review. Curr. Neuropharmacol. 2014, 12, 273–280. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, M.; Tóth, F.; Polyák, H.; Szabó, Á.; Mándi, Y.; Vécsei, L. Immune Influencers in Action: Metabolites and Enzymes of the Tryptophan-Kynurenine Metabolic Pathway. Biomedicines 2021, 9, 734. [Google Scholar] [CrossRef]
- Tanaka, M.; Vécsei, L. Editorial of Special Issue “Crosstalk between Depression, Anxiety, and Dementia: Comorbidity in Behavioral Neurology and Neuropsychiatry”. Biomedicines 2021, 9, 517. [Google Scholar] [CrossRef] [PubMed]
- North, H.F.; Bruggemann, J.; Cropley, V.; Swaminathan, V.; Sundram, S.; Lenroot, R.; Pereira, A.M.; Zalesky, A.; Bousman, C.; Pantelis, C.; et al. Increased peripheral inflammation in schizophrenia is associated with worse cognitive performance and related cortical thickness reductions. Eur. Arch Psychiatry Clin. Neurosci. 2021, 271, 595–607. [Google Scholar] [CrossRef] [PubMed]
- Yin, K.; Agrawal, D.K. Vitamin D and inflammatory diseases. J. Inflamm. Res. 2014, 7, 69–87. [Google Scholar] [CrossRef] [Green Version]
- Avan, R.; Sahebnasagh, A.; Hashemi, J.; Monajati, M.; Faramarzi, F.; Henney, N.C.; Montecucco, F.; Jamialahmadi, T.; Sahebkar, A. Update on Statin Treatment in Patients with Neuropsychiatric Disorders. Life 2021, 11, 1365. [Google Scholar] [CrossRef] [PubMed]
- Wonodi, I.; Schwarcz, R. Cortical kynurenine pathway metabolism: A novel target for cognitive enhancement in Schizophrenia. Schizophr. Bull. 2010, 36, 211–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koola, M.M. Kynurenine pathway and cognitive impairments in schizophrenia: Pharmacogenetics of galantamine and memantine. Schizophr. Res. Cogn. 2016, 4, 4–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulivieri, M.; Wierońska, J.M.; Lionetto, L.; Martinello, K.; Cieslik, P.; Chocyk, A.; Curto, M.; Di Menna, L.; Iacovelli, L.; Traficante, A.; et al. The Trace Kynurenine, Cinnabarinic Acid, Displays Potent Antipsychotic-Like Activity in Mice and Its Levels Are Reduced in the Prefrontal Cortex of Individuals Affected by Schizophrenia. Schizophr. Bull. 2020, 46, 1471–1481. [Google Scholar] [CrossRef]
- Correia, B.S.B.; Nani, J.V.; Waladares Ricardo, R.; Stanisic, D.; Costa, T.B.B.C.; Hayashi, M.A.F.; Tasic, L. Effects of Psychostimulants and Antipsychotics on Serum Lipids in an Animal Model for Schizophrenia. Biomedicines 2021, 9, 235. [Google Scholar] [CrossRef]
- Rog, J.; Błażewicz, A.; Juchnowicz, D.; Ludwiczuk, A.; Stelmach, E.; Kozioł, M.; Karakula, M.; Niziński, P.; Karakula-Juchnowicz, H. The Role of GPR120 Receptor in Essential Fatty Acids Metabolism in Schizophrenia. Biomedicines 2020, 8, 243. [Google Scholar] [CrossRef]
- Komatsu, H.; Watanabe, E.; Fukuchi, M. Psychiatric Neural Networks and Precision Therapeutics by Machine Learning. Biomedicines 2021, 9, 403. [Google Scholar] [CrossRef]
- Kraus, M.S.; Keefe, R.S.E. Cognition as an outcome measure in schizophrenia. Br. J. Psychiatry 2007, 191, s46–s51. [Google Scholar] [CrossRef] [PubMed]
- US. Army. Army Individual Test Battery. In Manual of Directions and Scoring; War Department, Adjunct General’s Office: Washington, DC, USA, 1944. [Google Scholar]
- Tombaugh, T.N. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef]
- Laere, E.; Tee, S.F.; Tang, P.Y. Assessment of Cognition in Schizophrenia Using Trail Making Test: A Meta-Analysis. Psychiatry Investig. 2018, 15, 945–955. [Google Scholar] [CrossRef] [PubMed]
- Nuechterlein, K.H.; Green, M.F. MATRICS Consensus Cognitive Battery Manual; MATRICS Assessment Inc.: Los Angeles, CA, USA, 2006. [Google Scholar]
- Morello, M.; Landel, V.; Lacassagne, E.; Baranger, K.; Annweiler, C.; Féron, F.; Millet, P. Vitamin D Improves Neurogenesis and Cognition in a Mouse Model of Alzheimer’s Disease. Mol. Neurobiol. 2018, 55, 6463–6479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, K.M.; Young, J.W.; McGrath, J.J.; Eyles, D.W.; Burne, T.H.J. Cognitive performance and response inhibition in developmentally vitamin D (DVD)-deficient rats. Behav. Brain Res. 2013, 242, 47–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salazar de Pablo, G.; Woods, S.W.; Drymonitou, G.; de Diego, H.; Fusar-Poli, P. Prevalence of Individuals at Clinical High-Risk of Psychosis in the General Population and Clinical Samples: Systematic Review and Meta-Analysis. Brain Sci. 2021, 11, 1544. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Mean | Std |
|---|---|---|
| Biometrics | ||
| Age [Years] | 33.1 | 11.4 |
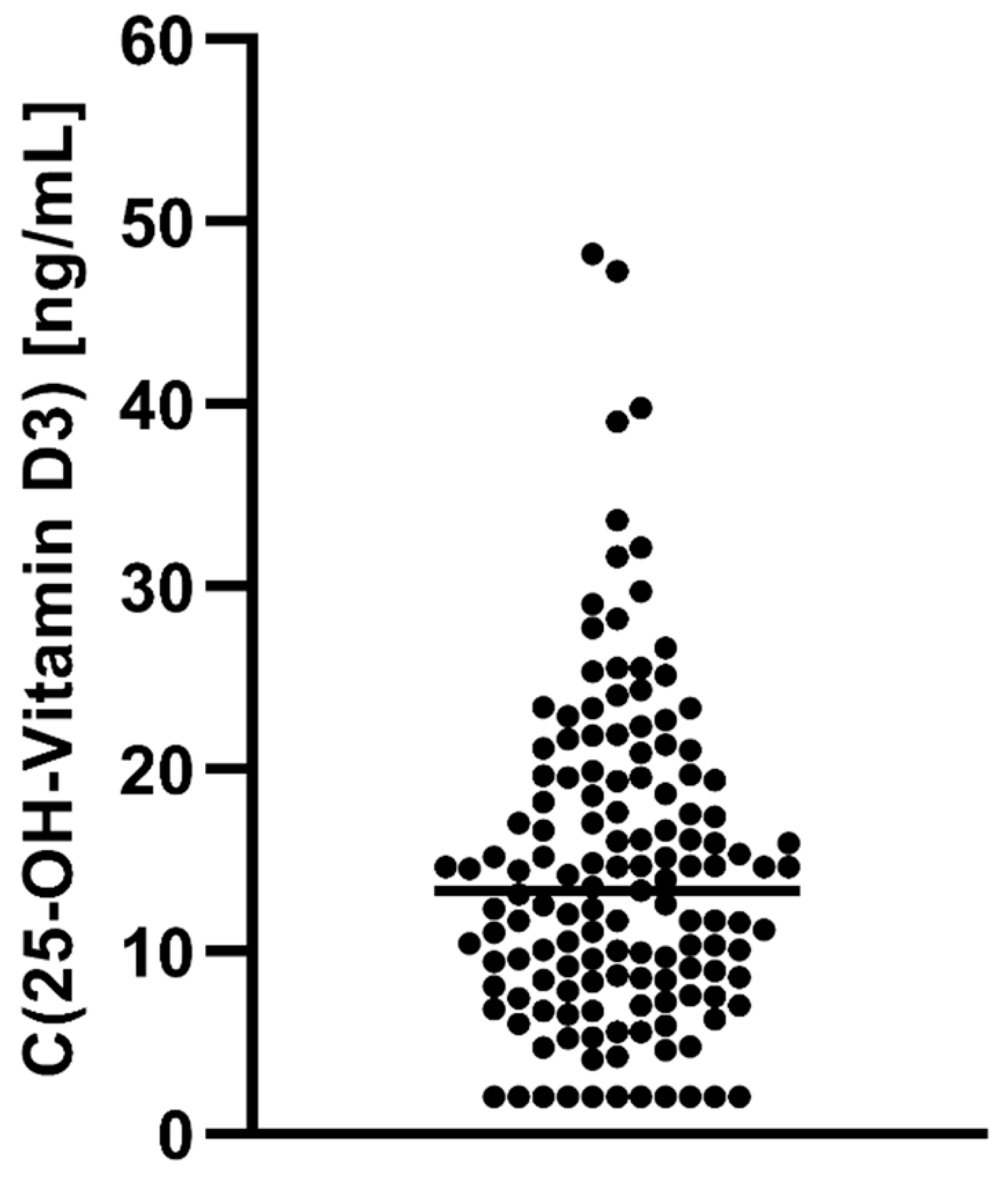
| C (25-OH-Vitamin D3) [ng/mL] | 14.5 | 8.9 |
| Duration of disease | 4.9 | 7.1 |
| Cognitive Performance | ||
| TMT-A [s] | 35.3 | 15.3 |
| TMT-B [s] | 95.9 | 49.6 |
| BACS—Verbal Memory | 37.8 | 12.5 |
| BACS—Working Memory: Correct Answers | 17.6 | 4.4 |
| BACS—Working Memory: Longest Sequence | 6.3 | 1.6 |
| BACS—Motor Speed | 64.0 | 17.6 |
| BACS—Fluent Speech Category | 18.1 | 5.2 |
| BACS—Fluent Speech Letter | 20.1 | 7.9 |
| BACS—Symbol Coding | 44.9 | 13.5 |
| BACS—Tower of London | 15.0 | 4.2 |
| Positive and Negative Syndrome Scale (PANSS) | ||
| Positive Symptoms | 16.1 | 6.9 |
| Negative Symptoms | 17.8 | 6.6 |
| Global Symptoms | 32.8 | 10.9 |
| N | % | |
| Gender | ||
| Female | 40 | 28.4 |
| Male | 101 | 71.6 |
| C(25-OH-Vitamin D) a | C(Anticholinergic) a | ||
|---|---|---|---|
| TMT−A (in s) | Pearson’s r | ** −0.373 | 0.169 |
| p-value | <0.001 | 0.097 | |
| N | 133 | 61 | |
| TMT−B (in s) | Pearson’s r | ** −0.336 | 0.174 |
| p-value | <0.001 | 0.092 | |
| N | 130 | 60 | |
| Verbal Memory | Pearson’s r | 0.175 | −0.124 |
| p-value | 0.020 | 0.173 | |
| N | 139 | 60 | |
| Working Memory Correct Answers | Pearson’s r | 0.131 | −0.048 |
| p-value | 0.062 | 0.358 | |
| N | 139 | 60 | |
| Working Memory Longest Sequence | Pearson’s r | 0.204 | −0.022 |
| p-value | 0.008 | 0.434 | |
| N | 139 | 60 | |
| Motor Speed | Pearson’s r | 0.107 | −0.122 |
| p-value | 0.108 | 0.184 | |
| N | 136 | 57 | |
| Fluent Speech Category | Pearson’s r | 0.195 | 0.001 |
| p-value | 0.011 | 0.496 | |
| N | 137 | 59 | |
| Fluent Speech Letter | Pearson’s r | 0.136 | −0.044 |
| p-value | 0.056 | 0.370 | |
| N | 138 | 59 | |
| Symbol Coding | Pearson’s r | ** 0.280 | −0.070 |
| p-value | <0.001 | 0.299 | |
| N | 139 | 59 | |
| Tower of London | Pearson’s r | ** 0.274 | −0.103 |
| p-value | <0.001 | 0.220 | |
| N | 137 | 59 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaebler, A.J.; Finner-Prével, M.; Sudar, F.P.; Langer, F.H.; Keskin, F.; Gebel, A.; Zweerings, J.; Mathiak, K. The Interplay between Vitamin D, Exposure of Anticholinergic Antipsychotics and Cognition in Schizophrenia. Biomedicines 2022, 10, 1096. https://doi.org/10.3390/biomedicines10051096
Gaebler AJ, Finner-Prével M, Sudar FP, Langer FH, Keskin F, Gebel A, Zweerings J, Mathiak K. The Interplay between Vitamin D, Exposure of Anticholinergic Antipsychotics and Cognition in Schizophrenia. Biomedicines. 2022; 10(5):1096. https://doi.org/10.3390/biomedicines10051096
Chicago/Turabian StyleGaebler, Arnim Johannes, Michelle Finner-Prével, Federico Pacheco Sudar, Felizia Hannah Langer, Fatih Keskin, Annika Gebel, Jana Zweerings, and Klaus Mathiak. 2022. "The Interplay between Vitamin D, Exposure of Anticholinergic Antipsychotics and Cognition in Schizophrenia" Biomedicines 10, no. 5: 1096. https://doi.org/10.3390/biomedicines10051096