
Hepatic Steatosis Is Associated with High White Blood Cell and Platelet Counts

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
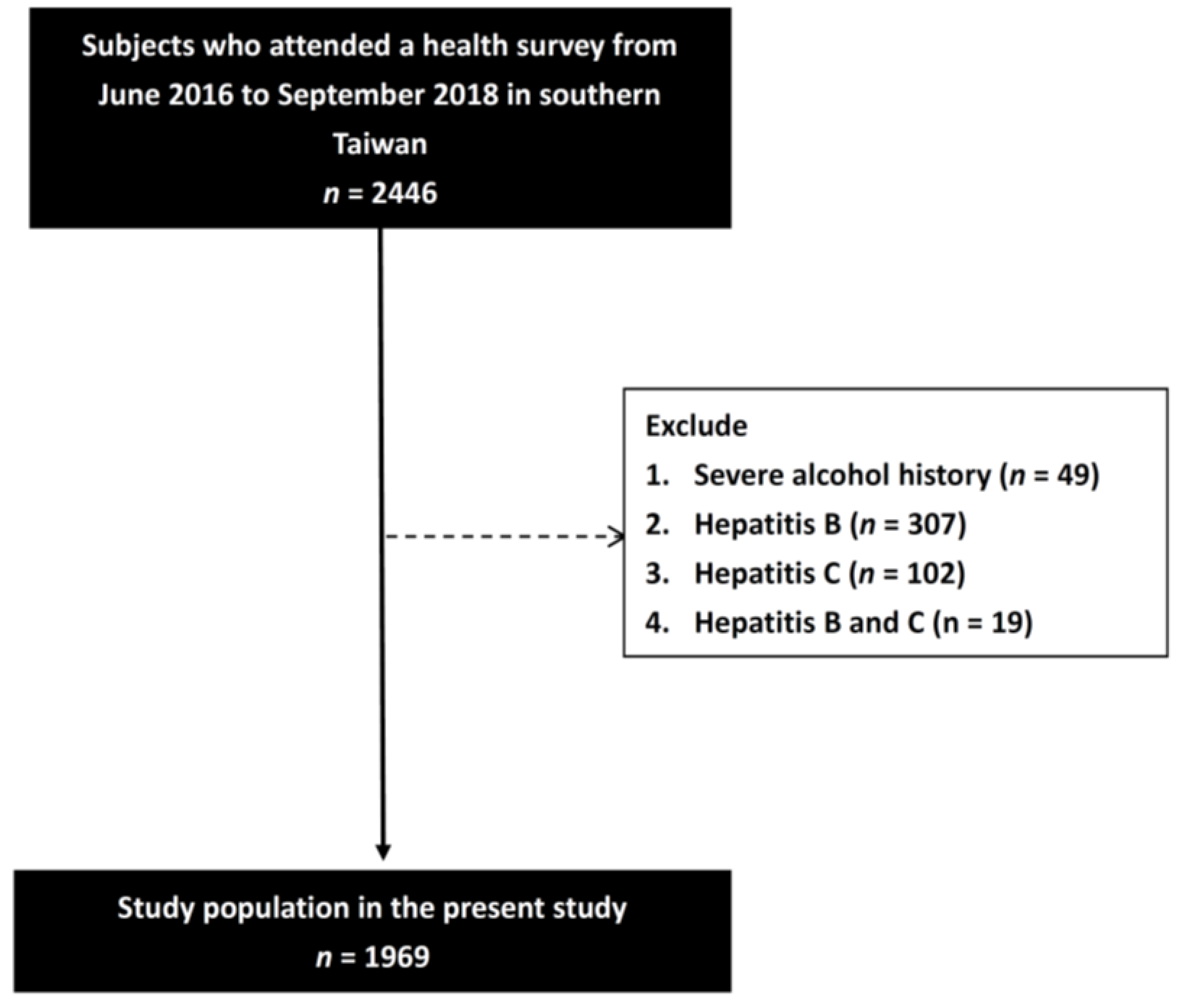
2.1. Participant Recruitment
2.2. Collection of Demographic, Medical, and Laboratory Data
2.3. Assessment of Hepatic Steatosis
2.4. Statistical Analysis
3. Results
3.1. Association between WBC and Platelet Counts with the Severity of Hepatic Steatosis
3.2. Determinants of WBC Count Using Linear Regression Analysis
3.3. Determinants of Platelet Count Using Linear Regression Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wong, W.K.; Chan, W.K. Nonalcoholic Fatty Liver Disease: A Global Perspective. Clin. Ther. 2021, 43, 473–499. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zou, B.; Yeo, Y.H.; Feng, Y.; Xie, X.; Lee, D.H.; Fujii, H.; Wu, Y.; Kam, L.Y.; Ji, F.; et al. Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999–2019: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2019, 4, 389–398. [Google Scholar] [CrossRef]
- Powell, E.E.; Wong, V.W.; Rinella, M. Non-alcoholic fatty liver disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef]
- Yang, R.; Chen, Y.; Chen, X. Value of routine test for identifying colorectal cancer from patients with nonalcoholic fatty liver disease. BMC Gastroenterol. 2020, 20, 180. [Google Scholar] [CrossRef]
- Nseir, W.; Abu-Rahmeh, Z.; Tsipis, A.; Mograbi, J.; Mahamid, M. Relationship between Non-Alcoholic Fatty Liver Disease and Breast Cancer. Isr. Med. Assoc. J. 2017, 19, 242–245. [Google Scholar]
- Dowman, J.K.; Tomlinson, J.W.; Newsome, P.N. Pathogenesis of non-alcoholic fatty liver disease. QJM: Int. J. Med. 2009, 103, 71–83. [Google Scholar] [CrossRef] [Green Version]
- Wainwright, P.; Byrne, C.D. Bidirectional Relationships and Disconnects between NAFLD and Features of the Metabolic Syndrome. Int. J. Mol. Sci. 2016, 17, 367. [Google Scholar] [CrossRef] [Green Version]
- Cobbina, E.; Akhlaghi, F. Non-alcoholic fatty liver disease (NAFLD)—Pathogenesis, classification, and effect on drug metabolizing enzymes and transporters. Drug Metab. Rev. 2017, 49, 197–211. [Google Scholar] [CrossRef]
- Kogiso, T.; Moriyoshi, Y.; Shimizu, S.; Nagahara, H.; Shiratori, K. High-sensitivity C-reactive protein as a serum predictor of nonalcoholic fatty liver disease based on the Akaike Information Criterion scoring system in the general Japanese population. J. Gastroenterol. 2009, 44, 313–321. [Google Scholar] [CrossRef]
- Tilg, H.; Diehl, A.M. Cytokines in alcoholic and nonalcoholic steatohepatitis. N. Engl. J. Med. 2000, 343, 1467–1476. [Google Scholar] [CrossRef]
- Tarantino, G.; Conca, P.; Pasanisi, F.; Ariello, M.; Mastrolia, M.; Arena, A.; Tarantino, M.; Scopacasa, F.; Vecchione, R. Could inflammatory markers help diagnose nonalcoholic steatohepatitis? Eur. J. Gastroenterol. Hepatol. 2009, 21, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Bugianesi, E.; McCullough, A.J.; Marchesini, G. Insulin resistance: A metabolic pathway to chronic liver disease. Hepatology 2005, 42, 987–1000. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of The Liver; European Association for the Study of Diabetes. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. Diabetologia 2016, 59, 1121–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef]
- Cerny, J.; Rosmarin, A.G. Why does my patient have leukocytosis? Hematol. Oncol. Clin. N. Am. 2012, 26, 303–319. [Google Scholar] [CrossRef]
- Sweetnam, P.M.; Thomas, H.F.; Yarnell, J.W.; Baker, I.A.; Elwood, P.C. Total and differential leukocyte counts as predictors of ischemic heart disease: The Caerphilly and Speedwell studies. Am. J. Epidemiol. 1997, 145, 416–421. [Google Scholar] [CrossRef] [Green Version]
- Kasper, P.; Martin, A.; Lang, S.; Kütting, F.; Goeser, T.; Demir, M.; Steffen, H.M. NAFLD and cardiovascular diseases: A clinical review. Clin. Res. Cardiol. 2021, 110, 921–937. [Google Scholar] [CrossRef]
- Hedayati, M.T.; Montazeri, M.; Rashidi, N.; Yousefi-Abdolmaleki, E.; Shafiee, M.A.; Maleki, A.; Farmani, M.; Montazeri, M. White blood cell count and clustered components of metabolic syndrome: A study in western Iran. Casp. J. Intern. Med. 2021, 12, 59–64. [Google Scholar] [CrossRef]
- Kim, D.J.; Noh, J.H.; Lee, B.W.; Choi, Y.H.; Chung, J.H.; Min, Y.K.; Lee, M.S.; Lee, M.K.; Kim, K.W. The associations of total and differential white blood cell counts with obesity, hypertension, dyslipidemia and glucose intolerance in a Korean population. J. Korean Med. Sci. 2008, 23, 193–198. [Google Scholar] [CrossRef]
- Herishanu, Y.; Rogowski, O.; Polliack, A.; Marilus, R. Leukocytosis in obese individuals: Possible link in patients with unexplained persistent neutrophilia. Eur. J. Haematol. 2006, 76, 516–520. [Google Scholar] [CrossRef]
- Rudnicka, E.; Suchta, K.; Grymowicz, M.; Calik-Ksepka, A.; Smolarczyk, K.; Duszewska, A.M.; Smolarczyk, R.; Meczekalski, B. Chronic Low Grade Inflammation in Pathogenesis of PCOS. Int. J. Mol. Sci. 2021, 22, 3789. [Google Scholar] [CrossRef] [PubMed]
- Chung, G.E.; Yim, J.Y.; Kim, D.; Kwak, M.S.; Yang, J.I.; Chung, S.J.; Yang, S.Y.; Kim, J.S. Associations between White Blood Cell Count and the Development of Incidental Nonalcoholic Fatty Liver Disease. Gastroenterol. Res. Pract. 2016, 2016, 7653689. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.D.; Behary, J.; Zekry, A. Non-alcoholic fatty liver disease: A review of epidemiology, risk factors, diagnosis and management. Intern. Med. J. 2020, 50, 1038–1047. [Google Scholar] [CrossRef] [PubMed]
- Neuschwander-Tetri, B.A. Non-alcoholic fatty liver disease. BMC Med. 2017, 15, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Meijden, P.E.J.; Heemskerk, J.W.M. Platelet biology and functions: New concepts and clinical perspectives. Nat. Rev. Cardiol. 2019, 16, 166–179. [Google Scholar] [CrossRef] [PubMed]
- Appleby, N.; Angelov, D. Clinical and laboratory assessment of a patient with thrombocytosis. Br. J. Hosp.Med. 2017, 78, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Alexandrakis, M.G.; Passam, F.H.; Moschandrea, I.A.; Christophoridou, A.V.; Pappa, C.A.; Coulocheri, S.A.; Kyriakou, D.S. Levels of serum cytokines and acute phase proteins in patients with essential and cancer-related thrombocytosis. Am. J. Clin. Oncol. 2003, 26, 135–140. [Google Scholar] [CrossRef]
- Kaushansky, K. Thrombopoiesis. Semin. Hematol. 2015, 52, 4–11. [Google Scholar] [CrossRef]
- Lohsoonthorn, V.; Jiamjarasrungsi, W.; Williams, M.A. Association of Hematological Parameters with Clustered Components of Metabolic Syndrome among Professional and Office Workers in Bangkok, Thailand. Diabetes Metab. Syndr. 2007, 1, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Patti, G.; Di Martino, G.; Ricci, F.; Renda, G.; Gallina, S.; Hamrefors, V.; Melander, O.; Sutton, R.; Engström, G.; De Caterina, R.; et al. Platelet Indices and Risk of Death and Cardiovascular Events: Results from a Large Population-Based Cohort Study. Thromb. Haemost. 2019, 119, 1773–1784. [Google Scholar] [CrossRef]
- Taniguchi, A.; Fukushima, M.; Seino, Y.; Sakai, M.; Yoshii, S.; Nagasaka, S.; Yamauchi, I.; Okumura, T.; Nin, K.; Tokuyama, K.; et al. Platelet count is independently associated with insulin resistance in non-obese Japanese type 2 diabetic patients. Metabolism 2003, 52, 1246–1249. [Google Scholar] [CrossRef]
- Malehmir, M.; Pfister, D.; Gallage, S.; Szydlowska, M.; Inverso, D.; Kotsiliti, E.; Leone, V.; Peiseler, M.; Surewaard, B.G.J.; Rath, D.; et al. Platelet GPIbα is a mediator and potential interventional target for NASH and subsequent liver cancer. Nat. Med. 2019, 25, 641–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrne, C.D.; Targher, G. What’s new in NAFLD pathogenesis, biomarkers and treatment? Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 70–71. [Google Scholar] [CrossRef]
- Pavlovic, N.; Rani, B.; Gerwins, P.; Heindryckx, F. Platelets as Key Factors in Hepatocellular Carcinoma. Cancers 2019, 11, 1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chauhan, A.; Adams, D.H.; Watson, S.P.; Lalor, P.F. Platelets: No longer bystanders in liver disease. Hepatology 2016, 64, 1774–1784. [Google Scholar] [CrossRef]
- Lee, Y.J.; Lee, H.R.; Shim, J.Y.; Moon, B.S.; Lee, J.H.; Kim, J.K. Relationship between white blood cell count and nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 888–894. [Google Scholar] [CrossRef]
- Wang, S.; Zhang, C.; Zhang, G.; Yuan, Z.; Liu, Y.; Ding, L.; Sun, X.; Jia, H.; Xue, F. Association between white blood cell count and non-alcoholic fatty liver disease in urban Han Chinese: A prospective cohort study. BMJ Open 2016, 6, e010342. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.Y.; Cai, J.T.; Song, Z.Y.; Tong, Y.L.; Wang, J.H. The associations among Helicobacter pylori infection, white blood cell count and nonalcoholic fatty liver disease in a large Chinese population. Medicine 2018, 97, e13271. [Google Scholar] [CrossRef]
- Campos, G.M.; Bambha, K.; Vittinghoff, E.; Rabl, C.; Posselt, A.M.; Ciovica, R.; Tiwari, U.; Ferrel, L.; Pabst, M.; Bass, N.M.; et al. A clinical scoring system for predicting nonalcoholic steatohepatitis in morbidly obese patients. Hepatology 2008, 47, 1916–1923. [Google Scholar] [CrossRef]
- Yoneda, M.; Fujii, H.; Sumida, Y.; Hyogo, H.; Itoh, Y.; Ono, M.; Eguchi, Y.; Suzuki, Y.; Aoki, N.; Kanemasa, K.; et al. Platelet count for predicting fibrosis in nonalcoholic fatty liver disease. J. Gastroenterol. 2011, 46, 1300–1306. [Google Scholar] [CrossRef]
- Milovanovic Alempijevic, T.; Stojkovic Lalosevic, M.; Dumic, I.; Jocic, N.; Pavlovic Markovic, A.; Dragasevic, S.; Jovicic, I.; Lukic, S.; Popovic, D.; Milosavljevic, T. Diagnostic Accuracy of Platelet Count and Platelet Indices in Noninvasive Assessment of Fibrosis in Nonalcoholic Fatty Liver Disease Patients. Can. J. Gastroenterol. Hepatol. 2017, 2017, 6070135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, K.C.; Kim, B.S.; Cho, Y.K.; Park, D.I.; Woo, S.; Kim, S.; Wild, S.H.; Byrne, C.D. Predicting incident fatty liver using simple cardio-metabolic risk factors at baseline. BMC Gastroenterol. 2012, 12, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garjani, A.; Safaeiyan, A.; Khoshbaten, M. Association between platelet count as a noninvasive marker and ultrasonographic grading in patients with nonalcoholic Fatty liver disease. Hepat. Mon. 2015, 15, e24449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, W.; Zhao, C.; Shen, C.; Wang, Y. Cytokeratin 18, alanine aminotransferase, platelets and triglycerides predict the presence of nonalcoholic steatohepatitis. PLoS ONE 2013, 8, e82092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef]
- Fan, J.G.; Jia, J.D.; Li, Y.M.; Wang, B.Y.; Lu, L.G.; Shi, J.P.; Chan, L.Y. Guidelines for the diagnosis and management of nonalcoholic fatty liver disease: Update 2010. J. Dig. Dis. 2011, 12, 38–44. [Google Scholar] [CrossRef]
- Farrell, G.C.; Chitturi, S.; Lau, G.K.; Sollano, J.D. Guidelines for the assessment and management of non-alcoholic fatty liver disease in the Asia-Pacific region: Executive summary. J. Gastroenterol. Hepatol. 2007, 22, 775–777. [Google Scholar] [CrossRef]
- Sirota, J.C.; McFann, K.; Targher, G.; Johnson, R.J.; Chonchol, M.; Jalal, D.I. Elevated serum uric acid levels are associated with non-alcoholic fatty liver disease independently of metabolic syndrome features in the United States: Liver ultrasound data from the National Health and Nutrition Examination Survey. Metabolism 2013, 62, 392–399. [Google Scholar] [CrossRef] [Green Version]
- Kuppan, G.; Anjana, R.M.; Deepa, M.; Paramasivam, P.; Chandrakumar, S.; Kaliyaperumal, V.; Mohan, V. Inflammatory markers in relation to nonalcoholic fatty liver disease in urban South Indians. Diabetes Technol. Ther. 2012, 14, 152–158. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Duan, Q.; Wu, R.; Harris, E.N.; Su, Q. Pathophysiological communication between hepatocytes and non-parenchymal cells in liver injury from NAFLD to liver fibrosis. Adv. Drug Deliv. Rev. 2021, 176, 113869. [Google Scholar] [CrossRef] [PubMed]
- Vallianou, N.; Christodoulatos, G.S.; Karampela, I.; Tsilingiris, D.; Magkos, F.; Stratigou, T.; Kounatidis, D.; Dalamaga, M. Understanding the Role of the Gut Microbiome and Microbial Metabolites in Non-Alcoholic Fatty Liver Disease: Current Evidence and Perspectives. Biomolecules 2021, 12, 56. [Google Scholar] [CrossRef] [PubMed]
- Caussy, C.; Tripathi, A.; Humphrey, G.; Bassirian, S.; Singh, S.; Faulkner, C.; Bettencourt, R.; Rizo, E.; Richards, L.; Xu, Z.Z.; et al. A gut microbiome signature for cirrhosis due to nonalcoholic fatty liver disease. Nat. Commun. 2019, 10, 1406. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; de Gottardi, A.; Rescigno, M. The gut-liver axis in liver disease: Pathophysiological basis for therapy. J. Hepatol. 2020, 72, 558–577. [Google Scholar] [CrossRef] [Green Version]
- Stojsavljevic, S.; Gomercic Palcic, M.; Virovic Jukic, L.; Smircic Duvnjak, L.; Duvnjak, M. Adipokines and proinflammatory cytokines, the key mediators in the pathogenesis of nonalcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 18070–18091. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Mehal, W.; Nagy, L.E.; Rotman, Y. Immunological mechanisms and therapeutic targets of fatty liver diseases. Cell. Mol. Immunol. 2021, 18, 73–91. [Google Scholar] [CrossRef]
- Friedman, S.L. Mechanisms of hepatic fibrogenesis. Gastroenterology 2008, 134, 1655–1669. [Google Scholar] [CrossRef] [Green Version]
- Yoneda, M.; Mawatari, H.; Fujita, K.; Iida, H.; Yonemitsu, K.; Kato, S.; Takahashi, H.; Kirikoshi, H.; Inamori, M.; Nozaki, Y.; et al. High-sensitivity C-reactive protein is an independent clinical feature of nonalcoholic steatohepatitis (NASH) and also of the severity of fibrosis in NASH. J. Gastroenterol. 2007, 42, 573–582. [Google Scholar] [CrossRef]
- Ramadori, P.; Klag, T.; Malek, N.P.; Heikenwalder, M. Platelets in chronic liver disease, from bench to bedside. JHEP Rep. 2019, 1, 448–459. [Google Scholar] [CrossRef] [Green Version]
- Ripoche, J. Blood platelets and inflammation: Their relationship with liver and digestive diseases. Clin. Res. Hepatol. Gastroenterol. 2011, 35, 353–357. [Google Scholar] [CrossRef]
- Lisman, T.; Porte, R.J. The role of platelets in liver inflammation and regeneration. Semin. Thromb. Hemost. 2010, 36, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Jesri, A.; Okonofua, E.C.; Egan, B.M. Platelet and white blood cell counts are elevated in patients with the metabolic syndrome. J. Clin. Hypertens. 2005, 7, 705–711; quiz 712–713. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-M.; Lee, J.-W.; Shim, J.-Y.; Lee, Y.-J. Relationship between platelet count and insulin resistance in Korean adolescents: A nationwide population-based study. Metab. Syndr. Relat. Disord. 2018, 16, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Keenan, R.T. The biology of urate. Semin. Arthritis Rheum. 2020, 50, S2–S10. [Google Scholar] [CrossRef]
- Kushiyama, A.; Nakatsu, Y.; Matsunaga, Y.; Yamamotoya, T.; Mori, K.; Ueda, K.; Inoue, Y.; Sakoda, H.; Fujishiro, M.; Ono, H.; et al. Role of Uric Acid Metabolism-Related Inflammation in the Pathogenesis of Metabolic Syndrome Components Such as Atherosclerosis and Nonalcoholic Steatohepatitis. Mediat. Inflamm. 2016, 2016, 8603164. [Google Scholar] [CrossRef]
- Kanbay, M.; Jensen, T.; Solak, Y.; Le, M.; Roncal-Jimenez, C.; Rivard, C.; Lanaspa, M.A.; Nakagawa, T.; Johnson, R.J. Uric acid in metabolic syndrome: From an innocent bystander to a central player. Eur. J. Intern. Med. 2016, 29, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Hsieh, M.C.; Chang, S.J. Metabolic syndrome, diabetes, and hyperuricemia. Curr. Opin. Rheumatol. 2013, 25, 210–216. [Google Scholar] [CrossRef]
- Zhou, Y.; Wei, F.; Fan, Y. High serum uric acid and risk of nonalcoholic fatty liver disease: A systematic review and meta-analysis. Clin. Biochem. 2016, 49, 636–642. [Google Scholar] [CrossRef]
- Darmawan, G.; Hamijoyo, L.; Hasan, I. Association between Serum Uric Acid and Non-Alcoholic Fatty Liver Disease: A Meta-Analysis. Acta Med. Indones 2017, 49, 136–147. [Google Scholar]
- Liu, Z.; Que, S.; Zhou, L.; Zheng, S. Dose-response Relationship of Serum Uric Acid with Metabolic Syndrome and Non-alcoholic Fatty Liver Disease Incidence: A Meta-analysis of Prospective Studies. Sci. Rep. 2015, 5, 14325. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Xu, C.; Ying, L.; Zang, S.; Zhuang, Z.; Lv, H.; Yang, W.; Luo, Y.; Ma, X.; Wang, L.; et al. Relationship of serum uric acid level with non-alcoholic fatty liver disease and its inflammation progression in non-obese adults. Hepatol. Res. 2017, 47, E104–E112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruggiero, C.; Cherubini, A.; Ble, A.; Bos, A.J.; Maggio, M.; Dixit, V.D.; Lauretani, F.; Bandinelli, S.; Senin, U.; Ferrucci, L. Uric acid and inflammatory markers. Eur. Heart J. 2006, 27, 1174–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, P.; Hong, L.; Zhao, Y.; Sun, H.; Li, L. The Association Between Hyperuricemia and Hematological Indicators in a Chinese Adult Population. Medicine 2016, 95, e2822. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Shen, P.; Ma, X.; Yu, X.; Ni, L.; Hao, X.; Wang, W.; Chen, N. White blood cell count and the incidence of hyperuricemia: Insights from a community-based study. Front. Med. 2019, 13, 741–746. [Google Scholar] [CrossRef]
- Tayefi, M.; Hassanian, S.M.; Maftouh, M.; Moohebati, M.; Bahrami, A.; Parizadeh, S.M.; Mahdizadeh, A.; Ghazizadeh, H.; Bazeli, J.; Heidari-Bakavoli, A.; et al. Relationship between platelet count and platelet width distribution and serum uric acid concentrations in patients with untreated essential hypertension. Biofactors 2018, 44, 532–538. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Hepatic Steatosis (−) (n = 1143) | Hepatic Steatosis (+) (n = 826) | p |
|---|---|---|---|
| Age (year) | 54.3 ± 14.2 | 55.7 ± 12.6 | 0.027 |
| Male gender (%) | 35.9 | 42.9 | 0.002 |
| Smoking history (%) | 10.7 | 13.4 | 0.064 |
| Alcohol history (%) | 21.3 | 20.4 | 0.604 |
| DM (%) | 7.0 | 15.3 | <0.001 |
| Hypertension (%) | 20.5 | 31.1 | <0.001 |
| SBP (mmHg) | 128.8 ± 20.0 | 135.7 ±18.7 | <0.001 |
| DBP (mmHg) | 75.7 ± 11.8 | 79.0 ± 10.9 | <0.001 |
| Body height (cm) | 160.2 ± 8.4 | 160.8 ± 9.0 | 0.194 |
| Body weight (kg) | 60.7 ± 10.7 | 69.5 ± 12.7 | <0.001 |
| Body mass index (kg/m2) | 23.6 ± 3.4 | 26.8 ± 3.7 | <0.001 |
| Laboratory parameters | |||
| WBC (×103/μL) | 5.8 ± 1.5 | 6.5 ± 1.8 | <0.001 |
| Hemoglobin (g/dL) | 13.8 ± 1.6 | 14.2 ± 1.7 | <0.001 |
| Platelet (×103/μL) | 261.5 ± 67.8 | 271.0 ± 68.5 | 0.002 |
| Fasting glucose (mg/dL) | 95.1 ± 21.0 | 106.8 ± 32.4 | <0.001 |
| Triglyceride (mg/dL) | 87 (64–125) | 134 (98–188.25) | <0.001 |
| Total cholesterol (mg/dL) | 199.4 ± 37.3 | 202.7 ± 37.7 | 0.059 |
| HDL-cholesterol (mg/dL) | 56.3 ± 13.9 | 48.2 ± 11.2 | <0.001 |
| LDL-cholesterol (mg/dL) | 117.7 ± 32.8 | 123.6 ± 35.3 | <0.001 |
| AST (U/L) | 25.2 ± 8.0 | 29.7 ± 14.2 | <0.001 |
| ALT (U/L) | 20.4 ± 12.9 | 33.0 ± 23.5 | <0.001 |
| Creatinine (mg/dL) | 0.94 ± 0.25 | 0.95 ± 0.28 | 0.381 |
| eGFR (mL/min/1.73 m2) | 89.7 ± 17.2 | 88.8 ± 15.3 | 0.206 |
| Uric acid (mg/dL) | 5.5 ± 1.5 | 6.0 ± 1.5 | <0.001 |
| Variables | Univariable | Multivariable | ||
|---|---|---|---|---|
| Unstandardized Coefficient β (95% CI) | p | Unstandardized Coefficient β (95% CI) | p | |
| Hepatic steatosis | 0.667 (0.522, 0.812) | <0.001 | 0.209 (0.055, 0.364) | 0.008 |
| Age (per 1 year) | −0.013 (−0.019, −0.008) | <0.001 | −0.027 (−0.037, −0.018) | <0.001 |
| Male (vs. female) | 0.469 (0.320, 0.617) | <0.001 | −0.270 (−0.467, −0.073) | 0.007 |
| Smoking history | 1.353 (1.134, 1.573) | <0.001 | 1.004 (0.778, 1.230) | <0.001 |
| Alcohol history | 0.174 (−0.007, 0.354) | 0.059 | - | - |
| DM | 0.682 (0.445, 0.919) | <0.001 | 0.434 (0.160, 0.708) | 0.002 |
| Hypertension | 0.117 (−0.052, 0.286) | 0.175 | - | - |
| SBP (per 1 mmHg) | 0.006 (0.002, 0.009) | 0.002 | 0.004 (−0.001, 0.009) | 0.088 |
| DBP (per 1 mmHg) | 0.014 (0.007, 0.020) | <0.001 | −0.001 (−0.009, 0.007) | 0.827 |
| Laboratory parameters | ||||
| Hemoglobin (per 1 g/dL) | 0.208 (0.163, 0.252) | <0.001 | 0.087 (0.033, 0.140) | 0.001 |
| Fasting glucose (per 1 mg/dL) | 0.010 (0.008, 0.013) | <0.001 | 0.006 (0.003, 0.009) | <0.001 |
| Triglyceride (log per 1 mg/dL) | 1.904 (1.610, 2.197) | <0.001 | 0.775 (0.412, 1.138) | <0.001 |
| Total cholesterol (per 1 mg/dL) | 0 (−0.002, 0.002) | 0.847 | - | - |
| HDL-cholesterol (per 1 mg/dL) | −0.027 (−0.032, −0.021) | <0.001 | −0.009 (−0.015, −0.003) | 0.005 |
| LDL-cholesterol (per 1 mg/dL) | 0.003 (0.001, 0.005) | 0.003 | 0.002 (0, 0.004) | 0.086 |
| AST (per 1 U/L) | 0.013 (0.006, 0.019) | <0.001 | −0.005 (−0.016, 0.006) | 0.343 |
| ALT (per 1 U/L) | 0.016 (0.012, 0.019) | <0.001 | 0.005 (−0.001, 0.012) | 0.122 |
| eGFR (per 1 mL/min/1.73 m2) | 0.006 (0.002, 0.010) | 0.008 | −0.005 (−0.013, 0.003) | 0.203 |
| Uric acid (per 1 mg/dL) | 0.193 (0.146, 0.240) | <0.001 | 0.075 (0.020, 0.129) | 0.007 |
| Variables | Univariable | Multivariable | ||
|---|---|---|---|---|
| Unstandardized Coefficient β (95% CI) | p | Unstandardized Coefficient β (95% CI) | p | |
| Hepatic steatosis | 9.482 (3.382, 15.583) | 0.002 | 12.213 (6.092, 18.334) | <0.001 |
| Age (per 1 year) | −1.580 (−1.792, −1.368) | <0.001 | −1.448 (−1.836, −1.060) | <0.001 |
| Male (vs. female) | −31.035 (−37.073, −24.997) | <0.001 | −20.475 (−28.290, −12.659) | <0.001 |
| Smoking history | 0.415 (−8.980, 9.809) | 0.931 | - | - |
| Alcohol history | −2.313 (−9.768, 5.142) | 0.543 | - | - |
| DM | −20.151 (−29.970, −10.333) | <0.001 | −3.306 (−14.601, 7.990) | 0.566 |
| Hypertension | −19.206 (−26.129, −12.283) | <0.001 | 1.473 (−5.783, 8.729) | 0.691 |
| SBP (per 1 mmHg) | −0.231 (−0.383, −0.079) | 0.003 | 0.154 (−0.003, 0.310) | 0.055 |
| DBP (per 1 mmHg) | 0.258 (−0.003, 0.519) | 0.053 | - | - |
| Laboratory parameters | ||||
| Hemoglobin (per 1 g/dL) | −8.608 (−10.426, −6.790) | <0.001 | −8.251 (−10.410, −6.093) | <0.001 |
| Fasting glucose (per 1 mg/dL) | −0.197 (−0.309, −0.086) | 0.001 | −0.003 (−0.132, 0.126) | 0.968 |
| Triglyceride (log per 1 mg/dL) | 11.627 (−0.954, 24.209) | 0.070 | - | - |
| Total cholesterol (per 1 mg/dL) | 0.097 (0.017, 0.177) | 0.018 | 0.009 (−0.152, 0.171) | 0.911 |
| HDL-cholesterol (per 1 mg/dL) | 0.284 (0.061, 0.507) | 0.013 | −0.179 (−0.449, 0.091) | 0.193 |
| LDL-cholesterol (per 1 mg/dL) | 0.130 (0.041, 0.218) | 0.004 | 0.167 (0.001, 0.334) | 0.049 |
| AST (per 1 U/L) | −0.488 (−0.755, −0.222) | <0.001 | −0.062 (−0.319,0.195) | 0.635 |
| ALT (per 1 U/L) | −0.046 (−0.204, 0.112) | 0.568 | - | - |
| eGFR (per 1 mL/min/1.73 m2) | 1.132 (0.956, 1.309) | <0.001 | 0.333 (0.010, 0.656) | 0.043 |
| Uric acid (per 1 mg/dL) | −4.479 (−6.436, −2.522) | <0.001 | 2.375 (0.154, 4.596) | 0.036 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chao, Y.-L.; Wu, P.-Y.; Huang, J.-C.; Chiu, Y.-W.; Lee, J.-J.; Chen, S.-C.; Chang, J.-M.; Hwang, S.-J.; Chen, H.-C. Hepatic Steatosis Is Associated with High White Blood Cell and Platelet Counts. Biomedicines 2022, 10, 892. https://doi.org/10.3390/biomedicines10040892
Chao Y-L, Wu P-Y, Huang J-C, Chiu Y-W, Lee J-J, Chen S-C, Chang J-M, Hwang S-J, Chen H-C. Hepatic Steatosis Is Associated with High White Blood Cell and Platelet Counts. Biomedicines. 2022; 10(4):892. https://doi.org/10.3390/biomedicines10040892
Chicago/Turabian StyleChao, Yu-Lin, Pei-Yu Wu, Jiun-Chi Huang, Yi-Wen Chiu, Jia-Jung Lee, Szu-Chia Chen, Jer-Ming Chang, Shang-Jyh Hwang, and Hung-Chun Chen. 2022. "Hepatic Steatosis Is Associated with High White Blood Cell and Platelet Counts" Biomedicines 10, no. 4: 892. https://doi.org/10.3390/biomedicines10040892