
Putative Role of the Lung–Brain Axis in the Pathogenesis of COVID-19-Associated Respiratory Failure: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
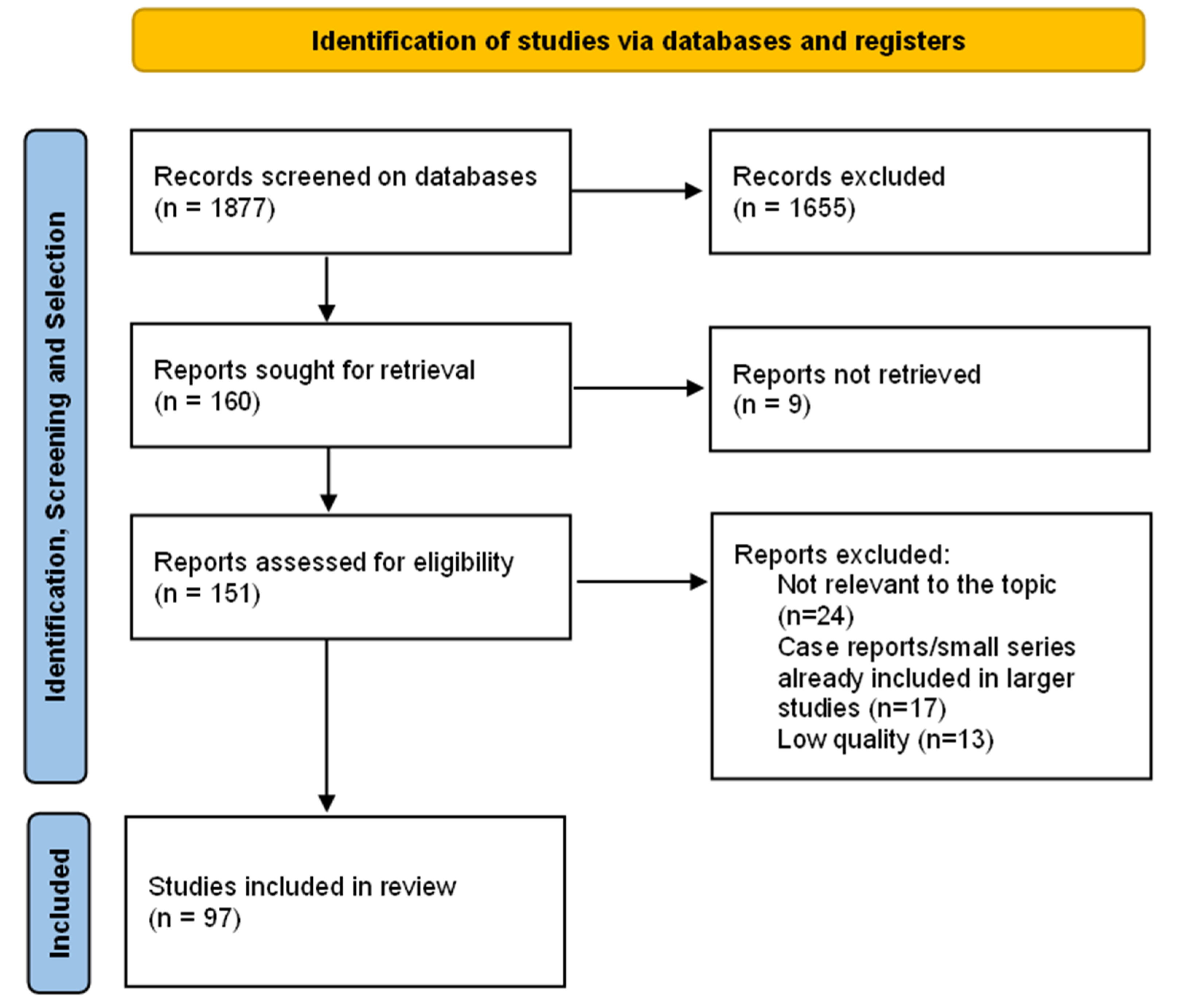
2. Methods
3. Results and Discussion
3.1. Clinical Clues of Brainstem Involvement in COVID-19: Non-Neuro-Specific Symptoms
3.2. Neuro-Specific Symptoms
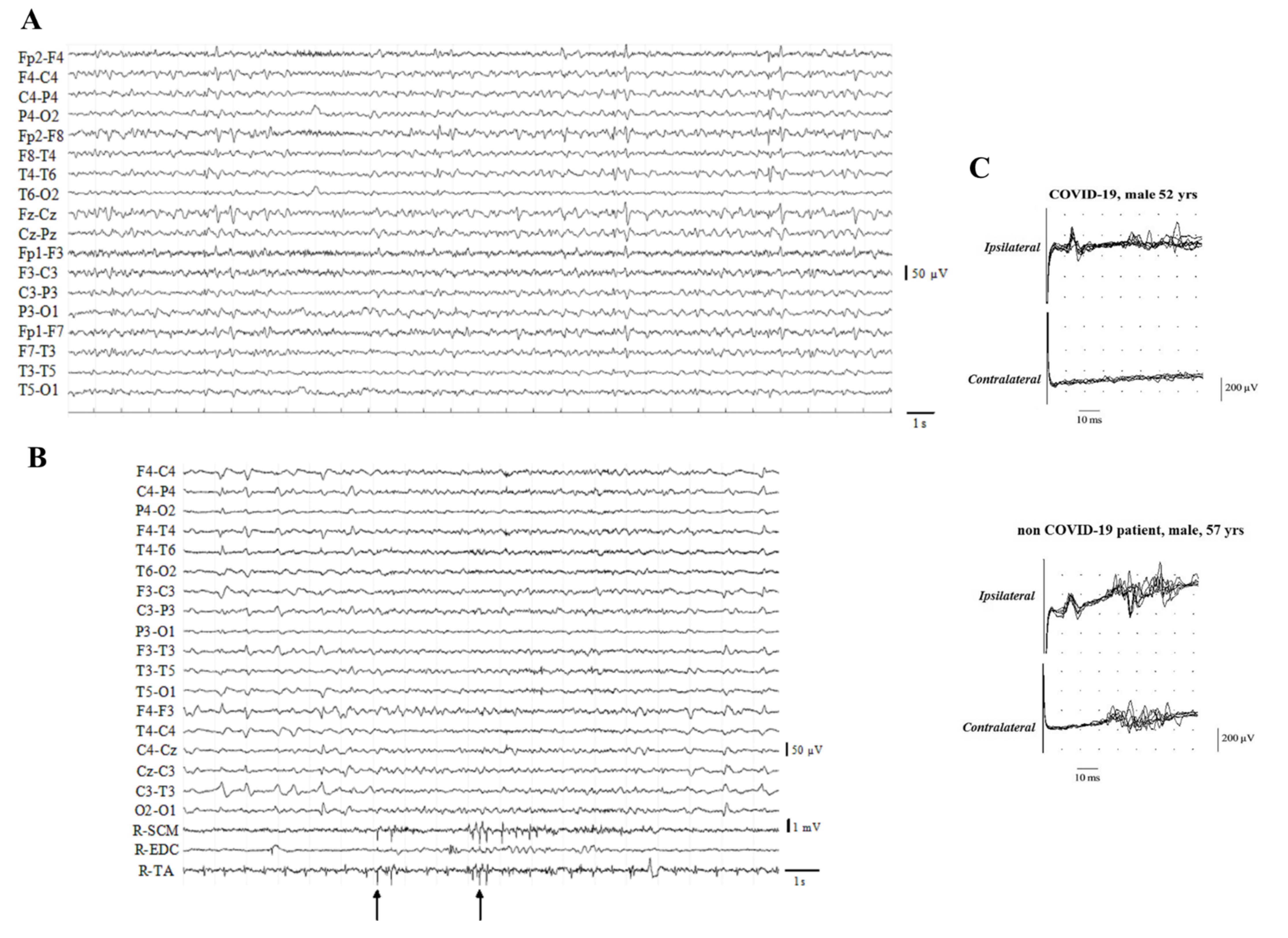
3.3. Neurophysiological Correlates
3.4. Neuroimaging Studies
3.5. Pathogenic Mechanisms
3.6. Clinical and Therapeutic Implications
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Contou, D.; Cally, R.; Sarfati, F.; Desaint, P.; Fraisse, M.; Plantefeve, G. Causes and timing of death in critically ill COVID-19 patients. Crit. Care 2021, 25, 79. [Google Scholar] [CrossRef] [PubMed]
- Elezkurtaj, S.; Greuel, S.; Ihlow, J.; Michaelis, E.G.; Bischoff, P.; Kunze, C.A.; Sinn, B.V.; Gerhold, M.; Hauptmann, K.; Ingold-Heppner, B.; et al. Causes of death and comorbidities in hospitalized patients with COVID-19. Sci. Rep. 2021, 11, 4263. [Google Scholar] [CrossRef]
- Chou, S.H.; Beghi, E.; Helbok, R.; Moro, E.; Sampson, J.; Altamirano, V.; Mainali, S.; Bassetti, C.; Suarez, J.I.; McNett, M.; et al. Global Incidence of Neurological Manifestations Among Patients Hospitalized With COVID-19-A Report for the GCS-NeuroCOVID Consortium and the ENERGY Consortium. JAMA 2021, 4, e2112131. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Varatharaj, A.; Thomas, N.; Ellul, M.A.; Davies, N.W.S.; Pollak, T.A.; Tenorio, E.L.; Sultan, M.; Easton, A.; Breen, G.; Zandi, M.; et al. Neurological and neuropsychiatric complications of COVID-19 in 153 patients: A UK-wide surveillance study. Lancet. Psychiatry 2020, 7, 875–882. [Google Scholar] [CrossRef]
- Liberatore, G.; de Santis, T.; Doneddu, P.E.; Gentile, F.; Albanese, A.; Nobile-Orazio, E. Clinical Reasoning: A case of COVID-19-associated pharyngeal-cervical-brachial variant of Guillain-Barre syndrome. Neurology 2020, 95, 978–983. [Google Scholar] [CrossRef]
- Filosto, M.; Piccinelli, S.C.; Gazzina, S.; Foresti, C.; Frigeni, B.; Servalli, M.C.; Sessa, M.; Cosentino, G.; Marchioni, E.; Ravaglia, S.; et al. Guillain-Barre syndrome and COVID-19: An observational multicentre study from two Italian hotspot regions. J. Neurol. Neurosurg. Psychiatry 2021, 92, 751–756. [Google Scholar] [CrossRef]
- Matschke, J.; Lutgehetmann, M.; Hagel, C.; Sperhake, J.P.; Schroder, A.S.; Edler, C.; Mushumba, H.; Fitzek, A.; Allweiss, L.; Dandri, M.; et al. Neuropathology of patients with COVID-19 in Germany: A post-mortem case series. Lancet. Neurol. 2020, 19, 919–929. [Google Scholar] [CrossRef]
- Mullol, J.; Alobid, I.; Marino-Sanchez, F.; Izquierdo-Dominguez, A.; Marin, C.; Klimek, L.; Wang, D.Y.; Liu, Z. The Loss of Smell and Taste in the COVID-19 Outbreak: A Tale of Many Countries. Curr. Allergy Asthma Rep. 2020, 20, 61. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Chiesa-Estomba, C.M.; de Siati, D.R.; Horoi, M.; le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Izquierdo-Dominguez, A.; Rojas-Lechuga, M.J.; Chiesa-Estomba, C.; Calvo-Henriquez, C.; Ninchritz-Becerra, E.; Soriano-Reixach, M.; Poletti-Serafini, D.; Villarreal, I.M.; Maza-Solano, J.M.; Moreno-Luna, R.; et al. Smell and Taste Dysfunction in COVID-19 Is Associated With Younger Age in Ambulatory Settings: A Multicenter Cross-Sectional Study. J. Investig. Allergol. Clin. Immunol. 2020, 30, 346–357. [Google Scholar] [CrossRef]
- Gomez-Iglesias, P.; Porta-Etessam, J.; Montalvo, T.; Valls-Carbo, A.; Gajate, V.; Matias-Guiu, J.A.; Parejo-Carbonell, B.; Gonzalez-Garcia, N.; Ezpeleta, D.; Lainez, J.M.; et al. An Online Observational Study of Patients with Olfactory and Gustory Alterations Secondary to SARS-CoV-2 Infection. Front. Public Health 2020, 8, 243. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Freidin, M.B.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Ganesh, S.; Varsavsky, T.; Cardoso, M.J.; El-Sayed Moustafa, J.S.; et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat. Med. 2020, 26, 1037–1040. [Google Scholar] [CrossRef]
- Xydakis, M.S.; Dehgani-Mobaraki, P.; Holbrook, E.H.; Geisthoff, U.W.; Bauer, C.; Hautefort, C.; Herman, P.; Manley, G.T.; Lyon, D.M.; Hopkins, C. Smell and taste dysfunction in patients with COVID-19. Lancet. Infect. Dis. 2020, 20, 1015–1016. [Google Scholar] [CrossRef]
- Costa, K.; Carnauba, A.T.L.; Rocha, K.W.; Andrade, K.C.L.; Ferreira, S.M.S.; Menezes, P.L. Olfactory and taste disorders in COVID-19: A systematic review. Braz. J. Otorhinolaryngol. 2020, 86, 781–792. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Beckers, E.; Mustin, V.; Ducarme, M.; Journe, F.; Marchant, A.; Jouffe, L.; Barillari, M.R.; Cammaroto, G.; et al. Prevalence and 6-month recovery of olfactory dysfunction: A multicentre study of 1363 COVID-19 patients. J. Intern. Med. 2021, 290, 451–461. [Google Scholar] [CrossRef]
- Foster, K.J.; Jauregui, E.; Tajudeen, B.; Bishehsari, F.; Mahdavinia, M. Smell loss is a prognostic factor for lower severity of coronavirus disease 2019. Ann. Allergy Asthma Immunol. 2020, 125, 481–483. [Google Scholar] [CrossRef]
- Barreto-Filho, J.A.; Seabra-Garcez, J.D.; Garcez, F.B.; Moreira, T.S.; Drager, L.F. Nondyspnogenic acute hypoxemic respiratory failure in COVID-19 pneumonia. J. Appl. Physiol. 2021, 130, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Nouri-Vaskeh, M.; Sharifi, A.; Khalili, N.; Zand, R.; Sharifi, A. Dyspneic and non-dyspneic (silent) hypoxemia in COVID-19: Possible neurological mechanism. Clin. Neurol. Neurosurg. 2020, 198, 106217. [Google Scholar] [CrossRef] [PubMed]
- Ur, A.; Verma, K. Happy Hypoxemia in COVID-19-A Neural Hypothesis. ACS Chem. Neurosci. 2020, 11, 1865–1867. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Bertran Recasens, B.; Martinez-Llorens, J.M.; Rodriguez-Sevilla, J.J.; Rubio, M.A. Lack of dyspnea in patients with Covid-19: Another neurological conundrum? Eur. J. Neurol. 2020, 27, e40. [Google Scholar] [CrossRef]
- Cavallazzi, R.; Ramirez, J.A. Influenza and Viral Pneumonia. Clin. Chest Med. 2018, 39, 703–721. [Google Scholar] [CrossRef]
- Ewig, S.; Ruiz, M.; Mensa, J.; Marcos, M.A.; Martinez, J.A.; Arancibia, F.; Niederman, M.S.; Torres, A. Severe Community-acquired Pneumonia. Am. J. Respir. Crit. Care Med. 1998, 158, 1102–1108. [Google Scholar] [CrossRef]
- Tsai, P.H.; Lai, W.Y.; Lin, Y.Y.; Luo, Y.H.; Lin, Y.T.; Chen, H.K.; Chen, Y.M.; Lai, Y.C.; Kuo, L.C.; Chen, S.D.; et al. Clinical manifestation and disease progression in COVID-19 infection. J. Chin. Med. Assoc. JCMA 2021, 84, 3–8. [Google Scholar] [CrossRef]
- Gonzalez-Duarte, A.; Norcliffe-Kaufmann, L. Is ‘happy hypoxia’ in COVID-19 a disorder of autonomic interoception? A hypothesis. Clin. Auton. Res. 2020, 30, 331–333. [Google Scholar] [CrossRef]
- Li, Y.C.; Bai, W.Z.; Hashikawa, T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J. Med. Virol. 2020, 92, 552–555. [Google Scholar] [CrossRef]
- Girard, T.D.; Thompson, J.L.; Pandharipande, P.P.; Brummel, N.E.; Jackson, J.C.; Patel, M.B.; Hughes, C.G.; Chandrasekhar, R.; Pun, B.T.; Boehm, L.M.; et al. Clinical phenotypes of delirium during critical illness and severity of subsequent long-term cognitive impairment: A prospective cohort study. Lancet. Respir. Med. 2018, 6, 213–222. [Google Scholar] [CrossRef]
- Lambrecq, V.; Hanin, A.; Munoz-Musat, E.; Chougar, L.; Gassama, S.; Delorme, C.; Cousyn, L.; Borden, A.; Damiano, M.; Frazzini, V.; et al. Association of Clinical, Biological, and Brain Magnetic Resonance Imaging Findings with Electroencephalographic Findings for Patients with COVID-19. JAMA 2021, 4, e211489. [Google Scholar] [CrossRef]
- Lin, L.; Al-Faraj, A.; Ayub, N.; Bravo, P.; Das, S.; Ferlini, L.; Karakis, I.; Lee, J.W.; Mukerji, S.S.; Newey, C.R.; et al. Electroencephalographic Abnormalities are Common in COVID-19 and are Associated with Outcomes. Ann. Neurol. 2021, 89, 872–883. [Google Scholar] [CrossRef] [PubMed]
- Louis, S.; Dhawan, A.; Newey, C.; Nair, D.; Jehi, L.; Hantus, S.; Punia, V. Continuous electroencephalography characteristics and acute symptomatic seizures in COVID-19 patients. Clin. Neurophysiol. 2020, 131, 2651–2656. [Google Scholar] [CrossRef] [PubMed]
- Apartis, E.; Vercueil, L. To jerk or not to jerk: A clinical pathophysiology of myoclonus. Rev. Neurol. 2016, 172, 465–476. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.L.; Murphy, K.A.; Sarna, J.R. Myoclonus and cerebellar ataxia associated with COVID-19: A case report and systematic review. J. Neurol. 2021, 268, 3517–3548. [Google Scholar] [CrossRef]
- Rabano-Suarez, P.; Bermejo-Guerrero, L.; Mendez-Guerrero, A.; Parra-Serrano, J.; Toledo-Alfocea, D.; Sanchez-Tejerina, D.; Santos-Fernandez, T.; Folgueira-Lopez, M.D.; Gutierrez-Gutierrez, J.; Ayuso-Garcia, B.; et al. Generalized myoclonus in COVID-19. Neurology 2020, 95, e767–e772. [Google Scholar] [CrossRef]
- Anand, P.; Zakaria, A.; Benameur, K.; Ong, C.; Putman, M.; O’Shea, S.; Greer, D.; Cervantes-Arslanian, A.M. Myoclonus in Patients With Coronavirus Disease 2019: A Multicenter Case Series. Crit. Care Med. 2020, 48, 1664–1669. [Google Scholar] [CrossRef]
- Grieb, A.; Seitz, T.; Kitzberger, R.; Schmidbauer, M.; Hoepler, W.; Baumgartner, S.; Traugott, M.T.; Pawelka, E.; Karolyi, M.; Strasser, G.; et al. COVID-19-associated myoclonus in a series of five critically ill patients. Wien. Klin. Wochenschr. 2021, 133, 902–908. [Google Scholar] [CrossRef]
- Bocci, T.; Bulfamante, G.; Campiglio, L.; Coppola, S.; Falleni, M.; Chiumello, D.; Priori, A. Brainstem clinical and neurophysiological involvement in COVID-19. J. Neurol. 2021, 268, 3598–3600. [Google Scholar] [CrossRef]
- Manganelli, F.; Vargas, M.; Iovino, A.; Iacovazzo, C.; Santoro, L.; Servillo, G. Brainstem involvement and respiratory failure in COVID-19. Neurol. Sci. 2020, 41, 1663–1665. [Google Scholar] [CrossRef] [PubMed]
- Jeanneret, V.; Winkel, D.; Risman, A.; Shi, H.; Gombolay, G. Post-infectious rhombencephalitis after coronavirus-19 infection: A case report and literature review. J. Neuroimmunol. 2021, 357, 577623. [Google Scholar] [CrossRef] [PubMed]
- Al-Dalahmah, O.; Thakur, K.T.; Nordvig, A.S.; Prust, M.L.; Roth, W.; Lignelli, A.; Uhlemann, A.C.; Miller, E.H.; Kunnath-Velayudhan, S.; Del Portillo, A.; et al. Neuronophagia and microglial nodules in a SARS-CoV-2 patient with cerebellar hemorrhage. Acta Neuropathol. Commun. 2020, 8, 147. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Fernandez, F.; Sandoval Valencia, H.; Barbella-Aponte, R.A.; Collado-Jimenez, R.; Ayo-Martin, O.; Barrena, C.; Molina-Nuevo, J.D.; Garcia-Garcia, J.; Lozano-Setien, E.; Alcahut-Rodriguez, C.; et al. Cerebrovascular disease in patients with COVID-19: Neuroimaging, histological and clinical description. Brain 2020, 143, 3089–3103. [Google Scholar] [CrossRef]
- Antony, A.R.; Haneef, Z. Systematic review of EEG findings in 617 patients diagnosed with COVID-19. Seizure 2020, 83, 234–241. [Google Scholar] [CrossRef]
- Pasini, E.; Bisulli, F.; Volpi, L.; Minardi, I.; Tappata, M.; Muccioli, L.; Pensato, U.; Riguzzi, P.; Tinuper, P.; Michelucci, R. EEG findings in COVID-19 related encephalopathy. Clin. Neurophysiol. 2020, 131, 2265–2267. [Google Scholar] [CrossRef]
- Koutroumanidis, M.; Gratwicke, J.; Sharma, S.; Whelan, A.; Tan, S.V.; Glover, G. Alpha coma EEG pattern in patients with severe COVID-19 related encephalopathy. Clin. Neurophysiol. 2021, 132, 218–225. [Google Scholar] [CrossRef]
- Clark, J.R.; Liotta, E.M.; Reish, N.J.; Shlobin, N.A.; Hoffman, S.C.; Orban, Z.S.; Lim, P.H.; Koralnik, I.J.; Batra, A. Abnormal movements in hospitalized COVID-19 patients: A case series. J. Neurol. Sci. 2021, 423, 117377. [Google Scholar] [CrossRef]
- Muccioli, L.; Rondelli, F.; Ferri, L.; Rossini, G.; Cortelli, P.; Guarino, M. Subcortical myoclonus in COVID-19: Comprehensive evaluation of a patient. Mov. Disord. Clin. Pract. 2020, 7, 971–973. [Google Scholar] [CrossRef]
- Newcombe, V.F.J.; Spindler, L.R.B.; Das, T.; Winzeck, S.; Allinson, K.; Stamatakis, E.A.; Menon, D.K.; Cambridge NeuroCovid Imaging Collaborators. Neuroanatomical substrates of generalized brain dysfunction in COVID-19. Intensive Care Med. 2021, 47, 116–118. [Google Scholar] [CrossRef]
- Groiss, S.J.; Balloff, C.; Elben, S.; Brandenburger, T.; Müttel, T.; Kindgen-Milles, D.; Vollmer, C.; Feldt, T.; Kunstein, A.; Ole Jensen, B.E.; et al. Prolonged Neuropsychological Deficits, Central Nervous System Involvement, and Brain Stem Affection After COVID-19-A Case Series. Front. Neurol. 2020, 11, 574004. [Google Scholar] [CrossRef]
- Niguet, J.P.; Tortuyaux, R.; Garcia, B.; Jourdain, M.; Chaton, L.; Preau, S.; Poissy, J.; Favory, R.; Nseir, S.; Mathieu, D.; et al. Neurophysiological findings and their prognostic value in critical COVID-19 patients: An observational study. Clin. Neurophysiol. 2021, 132, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Coolen, T.; Lolli, V.; Sadeghi, N.; Rovai, A.; Trotta, N.; Taccone, F.S.; Creteur, J.; Henrard, S.; Goffard, J.C.; Dewitte, O.; et al. Early postmortem brain MRI findings in COVID-19 non-survivors. Neurology 2020, 95, e2016–e2027. [Google Scholar] [CrossRef] [PubMed]
- Kremer, S.; Lersy, F.; de Seze, J.; Ferre, J.C.; Maamar, A.; Carsin-Nicol, B.; Collange, O.; Bonneville, F.; Adam, G.; Martin-Blondel, G.; et al. Brain MRI Findings in Severe COVID-19: A Retrospective Observational Study. Radiology 2020, 297, E242–E251. [Google Scholar] [CrossRef]
- Morassi, M.; Palmerini, F.; Nici, S.; Magni, E.; Savelli, G.; Guerra, U.P.; Chieregato, M.; Morbelli, S.; Vogrig, A. SARS-CoV-2-related encephalitis with prominent parkinsonism: Clinical and FDG-PET correlates in two patients. J. Neurol. 2021, 268, 3980–3987. [Google Scholar] [CrossRef]
- Cohen, M.E.; Eichel, R.; Steiner-Birmanns, B.; Janah, A.; Ioshpa, M.; Bar-Shalom, R.; Paul, J.J.; Gaber, H.; Skrahina, V.; Bornstein, N.M.; et al. A case of probable Parkinson’s disease after SARS-CoV-2 infection. Lancet Neurol. 2020, 19, 804–805. [Google Scholar] [CrossRef]
- Méndez-Guerrero, A.; Laespada-García, M.I.; Gómez-Grande, A.; Ruiz-Ortiz, M.; Blanco-Palmero, V.A.; Azcarate-Diaz, F.J.; Rábano-Suárez, P.; Álvarez-Torres, E.; de Fuenmayor-Fernández de la Hoz, C.P.; Vega Pérez, D.; et al. Acute hypokinetic-rigid syndrome following SARS-CoV-2 infection. Neurology 2020, 95, e2109–e2118. [Google Scholar] [CrossRef]
- Faber, I.; Brandão, P.R.P.; Menegatti, F.; de Carvalho Bispo, D.D.; Maluf, F.B.; Cardoso, F. Coronavirus Disease 2019 and Parkinsonism: A Non-post-encephalitic Case. Mov. Disord. 2020, 35, 1721–1722. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, L.A.; Vilensky, J.A. Encephalitis lethargica: 100 years after the epidemic. Brain 2017, 140, 2246–2251. [Google Scholar] [CrossRef]
- Guedj, E.; Campion, J.Y.; Dudouet, P.; Kaphan, E.; Bregeon, F.; Tissot-Dupont, H.; Guis, S.; Barthelemy, F.; Habert, P.; Ceccaldi, M.; et al. 18F-FDG brain PET hypometabolism in patients with long COVID. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2823–2833. [Google Scholar] [CrossRef]
- Guedj, E.; Million, M.; Dudouet, P.; Tissot-Dupont, H.; Bregeon, F.; Cammilleri, S.; Raoult, D. 18F-FDG brain PET hypometabolism in post-SARS-CoV-2 infection: Substrate for persistent/delayed disorders? Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 592–595. [Google Scholar] [CrossRef]
- Bulfamante, G.; Bocci, T.; Falleni, M.; Campiglio, L.; Coppola, S.; Tosi, D.; Chiumello, D.; Priori, A. Brainstem neuropathology in two cases of COVID-19: SARS-CoV-2 trafficking between brain and lung. J. Neurol. 2021, 268, 4486–4491. [Google Scholar] [CrossRef]
- Deigendesch, N.; Sironi, L.; Kutza, M.; Wischnewski, S.; Fuchs, V.; Hench, J.; Frank, A.; Nienhold, R.; Mertz, K.D.; Cathomas, G.; et al. Correlates of critical illness-related encephalopathy predominate postmortem COVID-19 neuropathology. Acta Neuropathol. 2020, 140, 583–586. [Google Scholar] [CrossRef]
- Fabbri, V.P.; Foschini, M.P.; Lazzarotto, T.; Gabrielli, L.; Cenacchi, G.; Gallo, C.; Aspide, R.; Frascaroli, G.; Cortelli, P.; Riefolo, M.; et al. Brain ischemic injury in COVID-19-infected patients: A series of 10 post-mortem cases. Brain Pathol. 2021, 31, 205–210. [Google Scholar] [CrossRef]
- Kantonen, J.; Mahzabin, S.; Mayranpaa, M.I.; Tynninen, O.; Paetau, A.; Andersson, N.; Sajantila, A.; Vapalahti, O.; Carpen, O.; Kekalainen, E.; et al. Neuropathologic features of four autopsied COVID-19 patients. Brain Pathol. 2020, 30, 1012–1016. [Google Scholar] [CrossRef]
- Kirschenbaum, D.; Imbach, L.L.; Rushing, E.J.; Frauenknecht, K.B.M.; Gascho, D.; Ineichen, B.V.; Keller, E.; Kohler, S.; Lichtblau, M.; Reimann, R.R.; et al. Intracerebral endotheliitis and microbleeds are neuropathological features of COVID-19. Neuropathol. Appl. Neurobiol. 2021, 47, 454–459. [Google Scholar] [CrossRef]
- Lee, M.H.; Perl, D.P.; Nair, G.; Li, W.; Maric, D.; Murray, H.; Dodd, S.J.; Koretsky, A.P.; Watts, J.A.; Cheung, V.; et al. Microvascular Injury in the Brains of Patients with Covid-19. N. Engl. J. Med. 2021, 384, 481–483. [Google Scholar] [CrossRef]
- Meinhardt, J.; Radke, J.; Dittmayer, C.; Franz, J.; Thomas, C.; Mothes, R.; Laue, M.; Schneider, J.; Brunink, S.; Greuel, S.; et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat. Neurosci. 2021, 24, 168–175. [Google Scholar] [CrossRef]
- Poloni, T.E.; Medici, V.; Moretti, M.; Visona, S.D.; Cirrincione, A.; Carlos, A.F.; Davin, A.; Gagliardi, S.; Pansarasa, O.; Cereda, C.; et al. COVID-19-related neuropathology and microglial activation in elderly with and without dementia. Brain Pathol. 2021, e12997. [Google Scholar] [CrossRef]
- Schurink, B.; Roos, E.; Radonic, T.; Barbe, E.; Bouman, C.S.C.; de Boer, H.H.; de Bree, G.J.; Bulle, E.B.; Aronica, E.M.; Florquin, S.; et al. Viral presence and immunopathology in patients with lethal COVID-19: A prospective autopsy cohort study. Lancet Microbe 2020, 1, e290–e299. [Google Scholar] [CrossRef]
- Solomon, I.H.; Normandin, E.; Bhattacharyya, S.; Mukerji, S.S.; Keller, K.; Ali, A.S.; Adams, G.; Hornick, J.L.; Padera, R.F., Jr.; Sabeti, P. Neuropathological Features of Covid-19. N. Engl. J. Med. 2020, 383, 989–992. [Google Scholar] [CrossRef] [PubMed]
- Thakur, K.T.; Miller, E.H.; Glendinning, M.D.; Al-Dalahmah, O.; Banu, M.A.; Boehme, A.K.; Boubour, A.L.; Bruce, S.S.; Chong, A.M.; Claassen, J.; et al. COVID-19 neuropathology at Columbia University Irving Medical Center/New York Presbyterian Hospital. Brain 2021, 144, 2696–2708. [Google Scholar] [CrossRef]
- von Weyhern, C.H.; Kaufmann, I.; Neff, F.; Kremer, M. Early evidence of pronounced brain involvement in fatal COVID-19 outcomes. Lancet 2020, 395, e109. [Google Scholar] [CrossRef]
- Hanley, B.; Naresh, K.N.; Roufosse, C.; Nicholson, A.G.; Weir, J.; Cooke, G.S.; Thursz, M.; Manousou, P.; Corbett, R.; Goldin, R.; et al. Histopathological findings and viral tropism in UK patients with severe fatal COVID-19: A post-mortem study. Lancet. Microbe 2020, 1, e245–e253. [Google Scholar] [CrossRef]
- Jensen, M.P.; Le Quesne, J.; Officer-Jones, L.; Teodosio, A.; Thaventhiran, J.; Ficken, C.; Goddard, M.; Smith, C.; Menon, D.; Allinson, K.S.J. Neuropathological findings in two patients with fatal COVID-19. Neuropathol. Appl. Neurobiol. 2021, 47, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Schwabenland, M.; Salie, H.; Tanevski, J.; Killmer, S.; Lago, M.S.; Schlaak, A.E.; Mayer, L.; Matschke, J.; Puschel, K.; Fitzek, A.; et al. Deep spatial profiling of human COVID-19 brains reveals neuroinflammation with distinct microanatomical microglia-T-cell interactions. Immunity 2021, 54, 1594–1610e.11. [Google Scholar] [CrossRef]
- Duarte-Neto, A.N.; Monteiro, R.A.A.; da Silva, L.F.F.; Malheiros, D.; de Oliveira, E.P.; Theodoro-Filho, J.; Pinho, J.R.R.; Gomes-Gouvea, M.S.; Salles, A.P.M.; de Oliveira, I.R.S.; et al. Pulmonary and systemic involvement in COVID-19 patients assessed with ultrasound-guided minimally invasive autopsy. Histopathology 2020, 77, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Bryce, C.; Grimes, Z.; Pujadas, E.; Ahuja, S.; Beasley, M.B.; Albrecht, R.; Hernandez, T.; Stock, A.; Zhao, Z.; AlRasheed, M.R.; et al. Pathophysiology of SARS-CoV-2: The Mount Sinai COVID-19 autopsy experience. Mod. Pathol. 2021, 34, 1456–1467. [Google Scholar] [CrossRef]
- Song, E.; Zhang, C.; Israelow, B.; Lu-Culligan, A.; Prado, A.V.; Skriabine, S.; Lu, P.; Weizman, O.E.; Liu, F.; Dai, Y.; et al. Neuroinvasion of SARS-CoV-2 in human and mouse brain. J. Exp. Med. 2021, 218, e20202135. [Google Scholar] [CrossRef]
- Ge, H.; Pan, Q.; Zhou, Y.; Xu, P.; Zhang, L.; Zhang, J.; Yi, J.; Yang, C.; Zhou, Y.; Liu, L.; et al. Lung Mechanics of Mechanically Ventilated Patients With COVID-19: Analytics With High-Granularity Ventilator Waveform Data. Front. Med. 2020, 7, 541. [Google Scholar] [CrossRef]
- El Beltagi, A.H.; Vattoth, S.; Abdelhady, M.; Ahmed, I.; Paksoy, Y.; Abou Kamar, M.; Alsoub, H.; Almaslamani, M.; Alkhal, A.L.; Own, A.; et al. Spectrum of neuroimaging findings in COVID-19. Br. J. Radiol. 2021, 94, 20200812. [Google Scholar] [CrossRef] [PubMed]
- Kandemirli, S.G.; Dogan, L.; Sarikaya, Z.T.; Kara, S.; Akinci, C.; Kaya, D.; Kaya, Y.; Yildirim, D.; Tuzuner, F.; Yildirim, M.S.; et al. Brain MRI Findings in Patients in the Intensive Care Unit with COVID-19 Infection. Radiology 2020, 297, E232–E235. [Google Scholar] [CrossRef] [PubMed]
- Mahammedi, A.; Saba, L.; Vagal, A.; Leali, M.; Rossi, A.; Gaskill, M.; Sengupta, S.; Zhang, B.; Carriero, A.; Bachir, S.; et al. Imaging of Neurologic Disease in Hospitalized Patients with COVID-19: An Italian Multicenter Retrospective Observational Study. Radiology 2020, 297, E270–E273. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.Y.; Khan, N.; Close, B.J.; Goel, R.K.; Blum, B.; Tavares, A.H.; Kenney, D.; Conway, H.L.; Ewoldt, J.K.; Chitalia, V.C.; et al. SARS-CoV-2 Disrupts Proximal Elements in the JAK-STAT Pathway. J. Virol. 2021, 95, e0086221. [Google Scholar] [CrossRef]
- Hadjadj, J.; Yatim, N.; Barnabei, L.; Corneau, A.; Boussier, J.; Smith, N.; Pere, H.; Charbit, B.; Bondet, V.; Chenevier-Gobeaux, C.; et al. Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science 2020, 369, 718–724. [Google Scholar] [CrossRef]
- Sun, J.; Ye, F.; Wu, A.; Yang, R.; Pan, M.; Sheng, J.; Zhu, W.; Mao, L.; Wang, M.; Xia, Z.; et al. Comparative Transcriptome Analysis Reveals the Intensive Early Stage Responses of Host Cells to SARS-CoV-2 Infection. Front. Microbiol 2020, 11, 593857. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Y.; Li, Y.; Huang, F.; Luo, B.; Yuan, Y.; Xia, B.; Ma, X.; Yang, T.; Yu, F.; et al. The ORF8 protein of SARS-CoV-2 mediates immune evasion through down-regulating MHC-Iota. Proc. Natl. Acad. Sci. USA 2021, 118, e2024202118. [Google Scholar] [CrossRef]
- Cutsforth-Gregory, J.K.; Benarroch, E.E. Nucleus of the solitary tract, medullary reflexes, and clinical implications. Neurology 2017, 88, 1187–1196. [Google Scholar] [CrossRef]
- Lambermont, B.; Davenne, E.; Maclot, F.; Delvenne, P. SARS-CoV-2 in carotid body. Intensive Care Med. 2021, 47, 342–343. [Google Scholar] [CrossRef]
- Bulfamante, G.; Chiumello, D.; Canevini, M.P.; Priori, A.; Mazzanti, M.; Centanni, S.; Felisati, G. First ultrastructural autoptic findings of SARS -Cov-2 in olfactory pathways and brainstem. Minerva Anestesiol. 2020, 86, 678–679. [Google Scholar] [CrossRef]
- Fanou, E.M.; Coutinho, J.M.; Shannon, P.; Kiehl, T.R.; Levi, M.M.; Wilcox, M.E.; Aviv, R.I.; Mandell, D.M. Critical Illness-Associated Cerebral Microbleeds. Stroke 2017, 48, 1085–1087. [Google Scholar] [CrossRef]
- Benghanem, S.; Mazeraud, A.; Azabou, E.; Chhor, V.; Shinotsuka, C.R.; Claassen, J.; Rohaut, B.; Sharshar, T. Brainstem dysfunction in critically ill patients. Crit. Care 2020, 24, 5. [Google Scholar] [CrossRef] [Green Version]
- Dongiovanni, P.; Meroni, M.; Longo, M.; Fracanzani, A.L. MAFLD in COVID-19 patients: An insidious enemy. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 867–872. [Google Scholar] [CrossRef]
- Aladawi, M.; Elfil, M.; Abu-Esheh, B.; Jazar, D.A.; Armouti, A.; Bayoumi, A.; Piccione, E. Guillain Barre Syndrome as a Complication of COVID-19: A Systematic Review (1197). Neurology 2021, 96, 1197. [Google Scholar]
- Gutierrez-Ortiz, C.; Mendez-Guerrero, A.; Rodrigo-Rey, S.; San Pedro-Murillo, E.; Bermejo-Guerrero, L.; Gordo-Manas, R.; de Aragon-Gomez, F.; Benito-Leon, J. Miller Fisher syndrome and polyneuritis cranialis in COVID-19. Neurology 2020, 95, e601–e605. [Google Scholar] [CrossRef] [Green Version]
- Caamano, D.S.J.; Alonso Beato, R. Facial diplegia, a possible atypical variant of Guillain-Barre Syndrome as a rare neurological complication of SARS-CoV-2. J. Clin. Neurosci. 2020, 77, 230–232. [Google Scholar] [CrossRef]
- Frithiof, R.; Rostami, E.; Kumlien, E.; Virhammar, J.; Fallmar, D.; Hultstrom, M.; Lipcsey, M.; Ashton, N.; Blennow, K.; Zetterberg, H.; et al. Critical illness polyneuropathy, myopathy and neuronal biomarkers in COVID-19 patients: A prospective study. Clin. Neurophysiol. 2021, 132, 1733–1740. [Google Scholar] [CrossRef]
- Bocci, T.; Campiglio, L.; Zardoni, M.; Botta, S.; Coppola, S.; Groppo, E.; Chiumello, D.; Priori, A. Critical illness neuropathy in severe COVID-19: A case series. Neurol. Sci. 2021, 42, 4893–4898. [Google Scholar] [CrossRef]
- Bax, F.; Lettieri, C.; Marini, A.; Pellitteri, G.; Surcinelli, A.; Valente, M.; Budai, R.; Patruno, V.; Gigli, G.L. Clinical and neurophysiological characterization of muscular weakness in severe COVID-19. Neurol. Sci. 2021, 42, 2173–2178. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Hoesch, R.E.; Lin, E.; Young, M.; Gottesman, R.F.; Altaweel, L.; Nyquist, P.A.; Stevens, R.D. Acute lung injury in critical neurological illness. Crit. Care Med. 2012, 40, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Sharshar, T.; Porcher, R.; Siami, S.; Rohaut, B.; Bailly-Salin, J.; Hopkinson, N.S.; Clair, B.; Guidoux, C.; Iacobone, E.; Sonneville, R.; et al. Brainstem responses can predict death and delirium in sedated patients in intensive care unit. Crit. Care Med. 2011, 39, 1960–1967. [Google Scholar] [CrossRef] [PubMed]
- Petersen, M.S.; Kristiansen, M.F.; Hanusson, K.D.; Danielsen, M.E.; Bjarni, A.S.; Gaini, S.; Strom, M.; Weihe, P. Long COVID in the Faroe Islands—A longitudinal study among non-hospitalized patients. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Carfi, A.; Bernabei, R.; Landi, F.; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- van den Borst, B.; Peters, J.B.; Brink, M.; Schoon, Y.; Bleeker-Rovers, C.P.; Schers, H.; van Hees, H.W.H.; van Helvoort, H.; van den Boogaard, M.; van der Hoeven, H.; et al. Comprehensive Health Assessment 3 Months After Recovery From Acute Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2021, 73, e1089–e1098. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Li, X.; Geng, D.; Mei, N.; Wu, P.Y.; Huang, C.C.; Jia, T.; Zhao, Y.; Wang, D.; Xiao, A.; et al. Cerebral Micro-Structural Changes in COVID-19 Patients—An MRI-based 3-month Follow-up Study. EClinicalMedicine 2020, 25, 100484. [Google Scholar] [CrossRef] [PubMed]
- Fuglebjerg, N.J.U.; Jensen, T.O.; Hoyer, N.; Ryrso, C.K.; Lindegaard, B.; Harboe, Z.B. Silent hypoxia in patients with SARS CoV-2 infection before hospital discharge. Int. J. Infect. Dis. Infect. Dis. 2020, 99, 100–101. [Google Scholar] [CrossRef]
- Cannistraro, R.J.; Badi, M.; Eidelman, B.H.; Dickson, D.W.; Middlebrooks, E.H.; Meschia, J.F. CNS small vessel disease: A clinical review. Neurology 2019, 92, 1146–1156. [Google Scholar] [CrossRef]
- Yong, S.J. Persistent Brainstem Dysfunction in Long-COVID: A Hypothesis. ACS Chem. Neurosci. 2021, 12, 573–580. [Google Scholar] [CrossRef]
- Hauss-Wegrzyniak, B.; Vraniak, P.D.; Wenk, G.L. LPS-induced neuroinflammatory effects do not recover with time. Neuroreport 2000, 11, 1759–1763. [Google Scholar] [CrossRef]
- Kim, W.G.; Mohney, R.P.; Wilson, B.; Jeohn, G.H.; Liu, B.; Hong, J.S. Regional difference in susceptibility to lipopolysaccharide-induced neurotoxicity in the rat brain: Role of microglia. J. Neurosci. 2000, 20, 6309–6316. [Google Scholar] [CrossRef] [PubMed]
- Azabou, E.; Bao, G.; Bounab, R.; Heming, N.; Annane, D. Vagus Nerve Stimulation: A Potential Adjunct Therapy for COVID-19. Front. Med. 2021, 8, 625836. [Google Scholar] [CrossRef]
- Kohoutova, M.; Horak, J.; Jarkovska, D.; Martinkova, V.; Tegl, V.; Nalos, L.; Vistejnova, L.; Benes, J.; Sviglerova, J.; Kuncova, J.; et al. Vagus Nerve Stimulation Attenuates Multiple Organ Dysfunction in Resuscitated Porcine Progressive Sepsis. Crit. Care Med. 2019, 47, e461–e469. [Google Scholar] [CrossRef] [PubMed]
- Meneses, G.; Bautista, M.; Florentino, A.; Diaz, G.; Acero, G.; Besedovsky, H.; Meneses, D.; Fleury, A.; Del Rey, A.; Gevorkian, G.; et al. Electric stimulation of the vagus nerve reduced mouse neuroinflammation induced by lipopolysaccharide. J. Inflamm. 2016, 13, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staats, P.; Giannakopoulos, G.; Blake, J.; Liebler, E.; Levy, R.M. The Use of Non-invasive Vagus Nerve Stimulation to Treat Respiratory Symptoms Associated with COVID-19: A Theoretical Hypothesis and Early Clinical Experience. Neuromodulation Technol. Neural Interface 2020, 23, 784–788. [Google Scholar] [CrossRef]
- Boezaart, A.P.; Botha, D.A. Treatment of Stage 3 COVID-19 with Transcutaneous Auricular Vagus Nerve Stimulation Drastically Reduces Interleukin-6 Blood Levels: A Report on Two Cases. Neuromodulation 2021, 24, 166–167. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Pathology Pattern | N | NeS | N (%) ICU | Vascular Damage | Inflammatory Response | SARS-CoV-2 Detection | References | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hy | I | T | Hem | BI | MA | MN/N | ||||||
| Inflammatory | 99 | 5/5 | 33 (33) | +/++ | -/+ | - | - | +/++ | +++ (>BT) | ++/+ (>BT) | ++ (CN V, IX, V, BT, OB) | [11,62,69,73,74,76,77] |
| Vascular | 94 | 24/39 (61) | 18/29 (62) | +/++ | +/++ | ++ | +/++ | + | ++ (BT)/NR | -/NR | -/+ | [64,65,66,71,77,79] |
| Inflammatory & Vascular | 120 | 23/83 (28) | 68/120 (57) | ++ | +/++ | +/++ | + | +/++ | +++ (>BT, OB) | ++/+ (BT) | ++ (CN V, BT, OB) | [63,67,68,70,72,75] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gentile, F.; Bocci, T.; Coppola, S.; Pozzi, T.; Modafferi, L.; Priori, A.; Chiumello, D. Putative Role of the Lung–Brain Axis in the Pathogenesis of COVID-19-Associated Respiratory Failure: A Systematic Review. Biomedicines 2022, 10, 729. https://doi.org/10.3390/biomedicines10030729
Gentile F, Bocci T, Coppola S, Pozzi T, Modafferi L, Priori A, Chiumello D. Putative Role of the Lung–Brain Axis in the Pathogenesis of COVID-19-Associated Respiratory Failure: A Systematic Review. Biomedicines. 2022; 10(3):729. https://doi.org/10.3390/biomedicines10030729
Chicago/Turabian StyleGentile, Francesco, Tommaso Bocci, Silvia Coppola, Tommaso Pozzi, Leo Modafferi, Alberto Priori, and Davide Chiumello. 2022. "Putative Role of the Lung–Brain Axis in the Pathogenesis of COVID-19-Associated Respiratory Failure: A Systematic Review" Biomedicines 10, no. 3: 729. https://doi.org/10.3390/biomedicines10030729