
Genes Involved in Immune Reinduction May Constitute Biomarkers of Response for Metastatic Melanoma Patients Treated with Targeted Therapy

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives and Endpoints
- -
- Identify changes in immunological markers after administering targeted therapy (BRAF+/−MEK inhibitors in patients with a BRAF mutation) whose mechanisms of action can be correlated with good immune function. In this sense, we will consider immune reinduction.
- -
- Identify early response prediction markers to identify long-term survivors after treatment with targeted therapy.
- -
- Identify prognostic immunological markers of metastatic melanoma.
- -
- Correlate the blood gene expression of immunological markers and their monitoring after the treatments with clinical variables.
- -
- Generate hypotheses to optimise the sequence of treatments (targeted therapy vs. immunotherapy).
2.2. Patients and Study Design
2.3. Ethical Aspects
2.4. Sample Collection
2.5. Gene Expression Analysis
2.6. Statistical and Bioinformatic Analysis
3. Results
3.1. Study Population
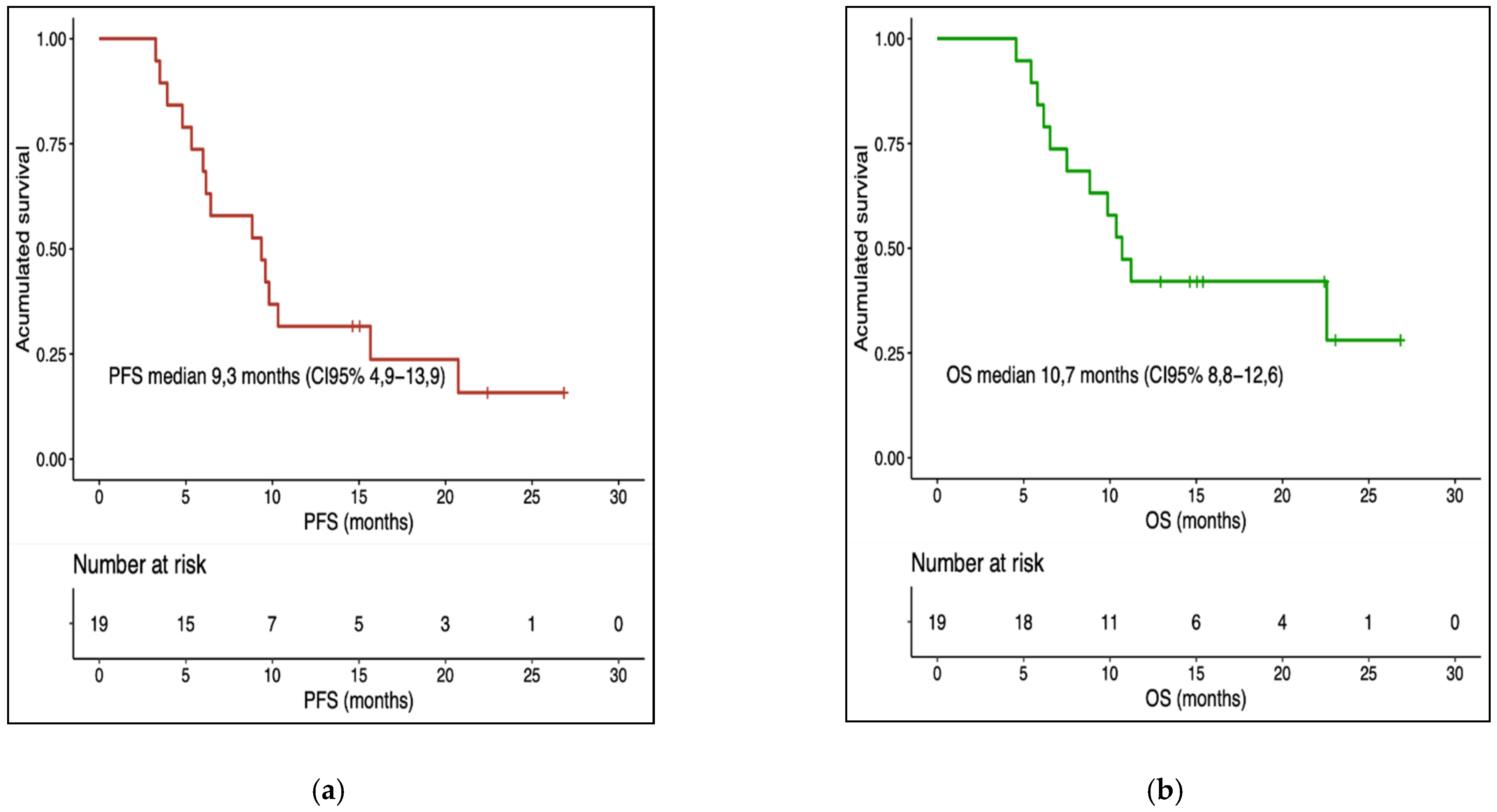
3.2. Treatment Response and Survival
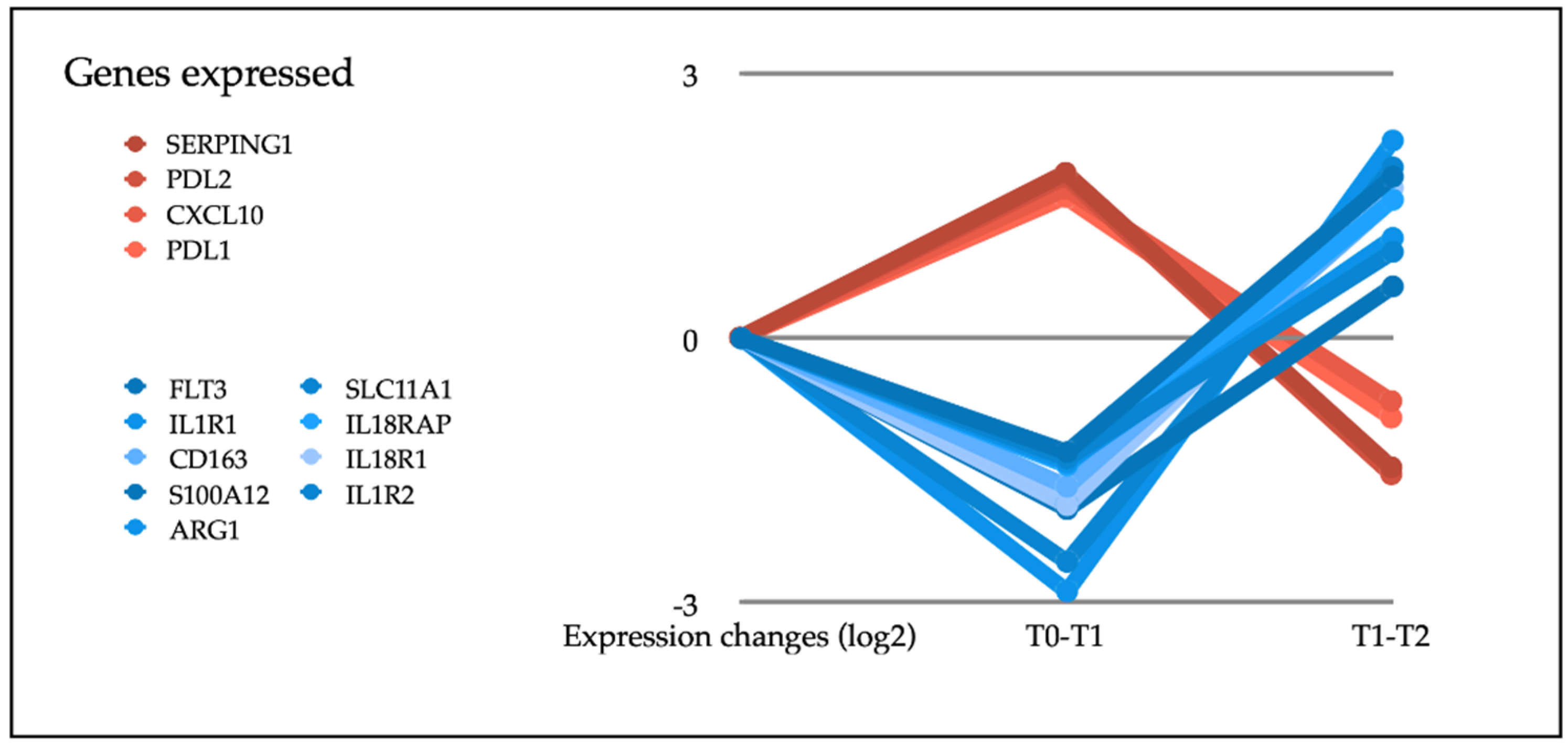
3.3. Gene Expression
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Palucka, A.K.; Coussens, L.M. The Basis of Oncoimmunology. Cell 2016, 164, 1233–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, C.; Thomas, L.; Bondarenko, I.; O’Day, S.; Weber, J.; Garbe, C.; Lebbe, C.; Baurain, J.-F.; Testori, A.; Grob, J.-J.; et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N. Engl. J. Med. 2011, 364, 2517–2526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef]
- Eggermont, A.M.; Chiarion-Sileni, V.; Grob, J.J.; Dummer, R.; Wolchok, J.D.; Schmidt, H.; Hamid, O.; Robert, C.; Ascierto, P.A.; Richards, J.M.; et al. Prolonged Survival in Stage III Melanoma with Ipilimumab Adjuvant Therapy. N. Engl. J. Med. 2016, 375, 1845–1855, Correction in N. Engl. J. Med. 2018, 379, 2185. [Google Scholar] [CrossRef] [Green Version]
- Ascierto, P.A.; Del Vecchio, M.; Mandalá, M.; Gogas, H.; Arance, A.M.; Dalle, S.; Cowey, C.L.; Schenker, M.; Grob, J.-J.; Chiarion-Sileni, V.; et al. Adjuvant nivolumab versus ipilimumab in resected stage IIIB-C and stage IV melanoma (CheckMate 238): 4-year results from a multicentre, double-blind, randomised, controlled, phase 3 trial. Lancet Oncol. 2020, 21, 1465–1477. [Google Scholar] [CrossRef]
- Eggermont, A.M.M.; Blank, C.U.; Mandala, M.; Long, G.V.; Atkinson, V.G.; Dalle, S.; Haydon, A.M.; Meshcheryakov, A.; Khattak, A.; Carlino, M.S.; et al. Longer Follow-Up Confirms Recurrence-Free Survival Benefit of Adjuvant Pembrolizumab in High-Risk Stage III Melanoma: Updated Results From the EORTC 1325-MG/KEYNOTE-054 Trial. J. Clin. Oncol. 2020, 38, 3925–3936. [Google Scholar] [CrossRef]
- Lee, Y.T.; Tan, Y.J.; Oon, C.E. Molecular targeted therapy: Treating cancer with specificity. Eur. J. Pharmacol. 2018, 834, 188–196. [Google Scholar] [CrossRef]
- Davies, H.; Bignell, G.R.; Cox, C.; Stephens, P.; Edkins, S.; Clegg, S.; Teague, J.; Woffendin, H.; Garnett, M.J.; Bottomley, W.; et al. Mutations of the BRAF gene in human cancer. Nature 2002, 417, 949–954. [Google Scholar] [CrossRef]
- Dummer, R.; Ascierto, P.A.; Gogas, H.J.; Arance, A.; Mandala, M.; Liszkay, G.; Garbe, C.; Schadendorf, D.; Krajsova, I.; Gutzmer, R.; et al. Overall survival in patients with BRAF-mutant melanoma receiving encorafenib plus binimetinib versus vemurafenib or encorafenib (COLUMBUS): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1315–1327, Correction in Lancet Oncol. 2018, 19, e509. [Google Scholar] [CrossRef]
- Robert, C.; Karaszewska, B.; Schachter, J.; Rutkowski, P.; Mackiewicz, A.; Stroiakovski, D.; Lichinitser, M.; Dummer, R.; Grange, F.; Mortier, L.; et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N. Engl. J. Med. 2015, 372, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larkin, J.; Ascierto, P.A.; Dréno, B.; Atkinson, V.; Liszkay, G.; Maio, M.; Mandalà, M.; Demidov, L.; Stroyakovskiy, D.; Thomas, L.; et al. Combined vemurafenib and cobimetinib in BRAF-mutated melanoma. N. Engl. J. Med. 2014, 371, 1867–1876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dummer, R.; Hauschild, A.; Santinami, M.; Atkinson, V.; Mandalà, M.; Kirkwood, J.M.; Sileni, V.C.; Larkin, J.; Nyakas, M.; Dutriaux, C.; et al. Five-Year Analysis of Adjuvant Dabrafenib plus Trametinib in Stage III Melanoma. N. Engl. J. Med. 2020, 383, 1139–1148. [Google Scholar] [CrossRef] [PubMed]
- Kuske, M.; Westphal, D.; Wehner, R.; Schmitz, M.; Beissert, S.; Praetorius, C.; Meier, F. Immunomodulatory effects of BRAF and MEK inhibitors: Implications for Melanoma therapy. Pharmacol. Res. 2018, 136, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Dummer, R.; Lebbé, C.; Atkinson, V.; Mandalà, M.; Nathan, P.D.; Arance, A.; Richtig, E.; Yamazaki, N.; Robert, C.; Schadendorf, D.; et al. Combined PD-1, BRAF and MEK inhibition in advanced BRAF-mutant melanoma: Safety run-in and biomarker cohorts of COMBI-i. Nat. Med. 2020, 26, 1557–1563. [Google Scholar] [CrossRef]
- Schwartz, L.H.; Litière, S.; de Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1-Update and clarification: From the RECIST committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef] [Green Version]
- Love, M.I.; Huber, W.; Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef] [Green Version]
- Navas-Delgado, I.; García-Nieto, J.; López-Camacho, E.; Rybinski, M.; Lavado, R.; Guerrero, M.B.; Aldana-Montes, J.F. VIGLA-M: Visual gene expression data analytics. BMC Bioinform. 2019, 20 (Suppl. 4), 150. [Google Scholar] [CrossRef]
- Langfelder, P.; Horvath, S. WGCNA: An R package for weighted correlation network analysis. BMC Bioinform. 2008, 9, 559. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Hu, E.; Xu, S.; Chen, M.; Guo, P.; Dai, Z.; Feng, T.; Zhou, L.; Tang, W.; Zhan, L.; et al. clusterProfiler 4.0: A universal enrichment tool for interpreting omics data. Innovation 2021, 2, 100141. [Google Scholar] [CrossRef]
- Ashburner, M.; Ball, C.A.; Blake, J.A.; Botstein, D.; Butler, H.; Cherry, J.M.; Davis, A.P.; Dolinski, K.; Dwight, S.S.; Eppig, J.T.; et al. Gene ontology: Tool for the unification of biology. The Gene Ontology Consortium. Nat. Genet. 2000, 25, 25–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanehisa, M.; Goto, S. KEGG: Kyoto encyclopedia of genes and genomes. Nucleic Acids Res. 2000, 28, 27–30. [Google Scholar] [CrossRef]
- Gonzalez-Cao, M.; Mayo de Las Casas, C.; Jordana Ariza, N.; Manzano, J.L.; Molina-Vila, M.; Soriano, V.; Puertolas, T.; Balada, A.; Soria, A.; Majem, M.; et al. Early evolution of BRAFV600 status in the blood of melanoma patients correlates with clinical outcome and identifies patients refractory to therapy. Melanoma Res. 2018, 28, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Herbreteau, G.; Charpentier, S.; Vallée, A.; Denis, M.G. Use of circulating tumoral DNA to guide treatment for metastatic melanoma. Pharmacogenomics 2019, 20, 1259–1270. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Cao, M.; Mayo de Las Casas, C.; Oramas, J.; Berciano-Guerrero, M.A.; de la Cruz, L.; Cerezuela, P.; Arance, A.; Muñoz-Couselo, E.; Espinosa, E.; Puertolas, T.; et al. Intermittent BRAF inhibition in advanced BRAF mutated melanoma results of a phase II randomized trial. Nat. Commun. 2021, 12, 7008. [Google Scholar] [CrossRef] [PubMed]
- Louveau, B.; Delyon, J.; De Moura, C.R.; Battistella, M.; Jouenne, F.; Golmard, L.; Sadoux, A.; Podgorniak, M.-P.; Chami, I.; Marco, O.; et al. A targeted genomic alteration analysis predicts survival of melanoma patients under BRAF inhibitors. Oncotarget 2019, 10, 1669–1687. [Google Scholar] [CrossRef] [Green Version]
- Dabrosin, N.; Sloth Juul, K.; Bæhr Georgsen, J.; Andrup, S.; Schmidt, H.; Steiniche, T.; Øllegaard, T.H.; Behrndtz, L.B. Innate immune cell infiltration in melanoma metastases affects survival and is associated with BRAFV600E mutation status. Melanoma Res. 2019, 29, 30–37. [Google Scholar] [CrossRef]
- Kelley, M.C. Immune Responses to BRAF-Targeted Therapy in Melanoma: Is Targeted Therapy Immunotherapy? Crit. Rev. Oncog. 2016, 21, 83–91. [Google Scholar] [CrossRef]
- Young, H.L.; Rowling, E.J.; Bugatti, M.; Giurisato, E.; Luheshi, N.; Arozarena, I.; Acosta, J.C.; Kamarashev, J.; Frederick, D.T.; Cooper, Z.; et al. An adaptive signaling network in melanoma inflammatory niches confers tolerance to MAPK signaling inhibition. J. Exp. Med. 2017, 214, 1691–1710. [Google Scholar] [CrossRef] [Green Version]
- Rulli, E.; Legramandi, L.; Salvati, L.; Mandala, M. The impact of targeted therapies and immunotherapy in melanoma brain metastases: A systematic review and meta-analysis. Cancer 2019, 125, 3776–3789. [Google Scholar] [CrossRef]
- Schaper-Gerhardt, K.; Okoye, S.; Herbst, R.; Ulrich, J.; Terheyden, P.; Pföhler, C.; Utikal, J.S.; Kreuter, A.; Mohr, P.; Dippel, E.; et al. PD-L1 status does not predict the outcome of BRAF inhibitor therapy in metastatic melanoma. Eur. J. Cancer. 2018, 88, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Frederick, D.T.; Piris, A.; Cogdill, A.P.; Cooper, Z.; Lezcano, C.; Ferrone, C.R.; Mitra, D.; Boni, A.; Newton, L.P.; Liu, C.; et al. BRAF inhibition is associated with enhanced melanoma antigen expression and a more favorable tumor microenvironment in patients with metastatic melanoma. Clin. Cancer Res. 2013, 19, 1225–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Mayes, P.A.; Eastman, S.; Shi, H.; Yadavilli, S.; Zhang, T.; Yang, J.; Seestaller-Wehr, L.; Zhang, S.-Y.; Hopson, C.; et al. The BRAF and MEK Inhibitors Dabrafenib and Trametinib: Effects on Immune Function and in Combination with Immunomodulatory Antibodies Targeting PD-1, PD-L1, and CTLA-4. Clin. Cancer Res. 2015, 21, 1639–1651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buderath, P.; Schwich, E.; Jensen, C.; Horn, P.A.; Kimmig, R.; Kasimir-Bauer, S.; Rebmann, V. Soluble Programmed Death Receptor Ligands sPD-L1 and sPD-L2 as Liquid Biopsy Markers for Prognosis and Platinum Response in Epithelial Ovarian Cancer. Front. Oncol. 2019, 9, 1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyo, J.S.; Son, B.K.; Chung, K.H.; Oh, I.H. Clinicopathological significance and prognostic implication of programmed death-1 ligand 2 expression in colorectal cancer. Int. J. Biol. Markers 2019, 34, 276–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, T.V.; Hussmann, D.; Nielsen, A.L. PD-L1 and PD-L2 expression correlated genes in non-small-cell lung cancer. Cancer Commun. 2019, 39, 30. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Zhou, X.; Sun, L.; Mao, Y. Correlation Between PD-L2 Expression and Clinical Outcome in Solid Cancer Patients: A Meta-Analysis. Front. Oncol. 2019, 9, 47. [Google Scholar] [CrossRef] [Green Version]
- Kakavand, H.; Rawson, R.V.; Pupo, G.M.; Yang, J.Y.H.; Menzies, A.; Carlino, M.S.; Kefford, R.; Howle, J.R.; Saw, R.P.; Thompson, J.F.; et al. PD-L1 Expression and Immune Escape in Melanoma Resistance to MAPK Inhibitors. Clin. Cancer Res. 2017, 23, 6054–6061. [Google Scholar] [CrossRef] [Green Version]
- Dufour, J.H.; Dziejman, M.; Liu, M.T.; Leung, J.H.; Lane, T.E.; Luster, A.D. IFN-gamma-inducible protein 10 (IP-10; CXCL10)-deficient mice reveal a role for IP-10 in effector T cell generation and trafficking. J. Immunol. 2002, 168, 3195–3204. [Google Scholar] [CrossRef] [Green Version]
- Bagheri, H.; Pourhanifeh, M.H.; Derakhshan, M.; Mahjoubin-Tehran, M.; Ghasemi, F.; Mousavi, S.; Rafiei, R.; Abbaszadeh-Goudarzi, K.; Mirzaei, H.R.; Mirzaei, H. CXCL-10: A new candidate for melanoma therapy? Cell Oncol. 2020, 43, 353–365. [Google Scholar] [CrossRef]
- Barreira da Silva, R.; Laird, M.E.; Yatim, N.; Fiette, L.; Ingersoll, M.A.; Albert, M.L. Dipeptidylpeptidase 4 inhibition enhances lymphocyte trafficking, improving both naturally occurring tumor immunity and immunotherapy. Nat. Immunol. 2015, 16, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.M.; Norsworthy, P.J.; A’Hern, R.P.; Eisen, T.G.; Gore, M.E.; Porter, C.D. Anti-alphaGal-dependent complement-mediated cytotoxicity in metastatic melanoma. Melanoma Res. 2006, 16, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Massi, D.; Rulli, E.; Cossa, M.; Valeri, B.; Rodolfo, M.; Merelli, B.; De Logu, F.; Nassini, R.; Del Vecchio, M.; Di Guardo, L.; et al. The density and spatial tissue distribution of CD8+ and CD163+ immune cells predict response and outcome in melanoma patients receiving MAPK inhibitors. J. Immunother. Cancer 2019, 7, 308. [Google Scholar] [CrossRef] [PubMed]
- Lowe, M.M.; Boothby, I.; Clancy, S.; Ahn, R.S.; Liao, W.; Nguyen, D.N.; Schumann, K.; Marson, A.; Mahuron, K.; Kingsbury, G.A.; et al. Regulatory T cells use arginase 2 to enhance their metabolic fitness in tissues. JCI Insight 2019, 4, e129756. [Google Scholar] [CrossRef] [Green Version]
- Arlauckas, S.P.; Garren, S.B.; Garris, C.S.; Kohler, R.H.; Oh, J.; Pittet, M.J.; Weissleder, R. Arg1 expression defines immunosuppressive subsets of tumor-associated macrophages. Theranostics 2018, 8, 5842–5854. [Google Scholar] [CrossRef]
- Hajek, E.; Krebs, F.; Bent, R.; Haas, K.; Bast, A.; Steinmetz, I.; Tuettenberg, A.; Grabbe, S.; Bros, M. BRAF inhibitors stimulate inflammasome activation and interleukin 1 beta production in dendritic cells. Oncotarget 2018, 9, 28294–28308. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, M.; Liu, W.; Luo, Y.; Tanaka, A.; Cai, X.; Norris, D.A.; Dinarello, C.A.; Fujita, M. Constitutively active inflammasome in human melanoma cells mediating autoinflammation via caspase-1 processing and secretion of interleukin-1beta. J. Biol. Chem. 2010, 285, 6477–6488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vella, L.J.; Pasam, A.; Dimopoulos, N.; Andrews, M.; Knights, A.; Puaux, A.-L.; Louahed, J.; Chen, W.; Woods, K.; Cebon, J. MEK inhibition, alone or in combination with BRAF inhibition, affects multiple functions of isolated normal human lymphocytes and dendritic cells. Cancer Immunol. Res. 2014, 2, 351–360. [Google Scholar] [CrossRef] [Green Version]
- Zubrilov, I.; Sagi-Assif, O.; Izraely, S.; Meshel, T.; Ben-Menahem, S.; Ginat, R.; Pasmanik-Chor, M.; Nahmias, C.; Couraud, P.-O.; Hoon, D.S.; et al. Vemurafenib resistance selects for highly malignant brain and lung-metastasizing melanoma cells. Cancer Lett. 2015, 361, 86–96. [Google Scholar] [CrossRef]
- Petrelli, F.; Ardito, R.; Merelli, B.; Lonati, V.; Cabiddu, M.; Seghezzi, S.; Barni, S.; Ghidini, A. Prognostic and predictive role of elevated lactate dehydrogenase in patients with melanoma treated with immunotherapy and BRAF inhibitors: A systematic review and meta-analysis. Melanoma Res. 2019, 29, 1–12. [Google Scholar] [CrossRef]
- Nakamura, Y.; Kitano, S.; Takahashi, A.; Namikawa, K.; Tanese, K.; Abe, T.; Funakoshi, T.; Yamamoto, N.; Amagai, M.; Yamazaki, N.; et al. Nivolumab for advanced melanoma: Pretreatment prognostic factors and early outcome markers during therapy. Oncotarget 2016, 7, 77404–77415. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | N = 19 |
|---|---|
| Age at initial diagnosis (mean, range) | 45.7 (20.7–61.9) |
| Age at stage IV diagnosis | 49.9 (23.9–85.4) |
| Male | 36.8% |
| Female | 63.2% |
| PS 0–1 | 78.9% |
| PS 2 | 21.1% |
| Comorbidities | |
| Allergies | 15.8% |
| Other medical conditions | 5.3% |
| Baseline Conditions | N = 19 |
| Previous treatments | |
| Primary tumour resection | 77.8% |
| Metastasectomy | 33.3% |
| Adjuvant | 27.8% |
| Analytics | |
| LDH (mean, range) | 367UI (144–1350) |
| Elevated LDH | 47.1% |
| Lymphocytes (mean, range) | 1485.3 (500–2600) |
| High dNLR | 68.4% |
| Tumour features | N = 19 |
| Initial stage | |
| Stage I-II | 44.4% |
| Stage III | 16.7% |
| Stage IV | 38.9% |
| Ulceration | 38.5 % |
| Primary tumour location | |
| Limbs | 27.8% |
| Trunk | 33.3% |
| Head and neck | 22.2% |
| Special locations * | 16.7% |
| Months Dx primary-M1 (mean, range) | 26.2 (0–106) |
| Number of metastasis | |
| One | 21.1% |
| Two | 26.3% |
| Three or more | 52.6% |
| CNS metastasis | 26.3% |
| M1a-b | 26.3% |
| M1c-d | 73.7% |
| BRAF Mutation | |
| V600E | 94.7% |
| V600K | 5.3% |
| Treatment and response | N = 19 |
| Type of treatment | |
| Vemurafenib-Cobimetinib | 57.9% |
| Dabrafenib-Trametinib | 36.8% |
| iBRAF monotherapy | 5.3% |
| Dose reduction | 52.6 % |
| Toxicity | |
| No toxicity | 5.3% |
| Mild–moderate toxicity (G1–2) | 57.9% |
| Significant toxicity (G3–4) | 36.8% |
| Response to treatments | |
| Disease stabilisation | 21.1% |
| Partial response | 57.9% |
| Complete response | 15.8% |
| Progression | 5.3% |
| Events | |
| Progression | 78.9% |
| Death | 63.2% |
| Survival (median in months, 95% CI) | |
| PFS | 9.3 (4.8–13.9) |
| OS | 10.7 (8.7–12.6) |
| OS (global) | 12.2 (4.9–19.5) |
| Gene.Name | log2Fold Change | Wald Test | p Value | p Adjusted |
|---|---|---|---|---|
| SERPING1 | 1.8682 | 4.3611 | 0.0000 | 0.0020 |
| PDCD1LG2 (PD−L2) | 1.8222 | 5.0262 | 0.0000 | 0.0002 |
| CXCL10 | 1.6894 | 3.8960 | 0.0001 | 0.0084 |
| CD274 (PD−L1) | 1.5948 | 4.5412 | 0.0000 | 0.0011 |
| FLT3 | −1.2846 | −3.4812 | 0.0005 | 0.0320 |
| SLC11A1 | −1.3549 | −3.3898 | 0.0007 | 0.0414 |
| IL1R1 | −1.4037 | −3.7701 | 0.0002 | 0.0114 |
| IL18RAP | −1.4360 | −3.8318 | 0.0001 | 0.0098 |
| CD163 | −1.6765 | −4.2324 | 0.0000 | 0.0030 |
| IL18R1 | −1.8855 | −4.5545 | 0.0000 | 0.0011 |
| S100A12 | −1.9305 | −4.1486 | 0.0000 | 0.0035 |
| IL1R2 | −2.5257 | −4.1305 | 0.0000 | 0.0035 |
| ARG1 | −2.8609 | −5.0351 | 0.0000 | 0.0002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berciano-Guerrero, M.-A.; Lavado-Valenzuela, R.; Moya, A.; delaCruz-Merino, L.; Toscano, F.; Valdivia, J.; Castellón, V.; Henao-Carrasco, F.; Sancho, P.; Onieva-Zafra, J.-L.; et al. Genes Involved in Immune Reinduction May Constitute Biomarkers of Response for Metastatic Melanoma Patients Treated with Targeted Therapy. Biomedicines 2022, 10, 284. https://doi.org/10.3390/biomedicines10020284
Berciano-Guerrero M-A, Lavado-Valenzuela R, Moya A, delaCruz-Merino L, Toscano F, Valdivia J, Castellón V, Henao-Carrasco F, Sancho P, Onieva-Zafra J-L, et al. Genes Involved in Immune Reinduction May Constitute Biomarkers of Response for Metastatic Melanoma Patients Treated with Targeted Therapy. Biomedicines. 2022; 10(2):284. https://doi.org/10.3390/biomedicines10020284
Chicago/Turabian StyleBerciano-Guerrero, Miguel-Angel, Rocío Lavado-Valenzuela, Aurelio Moya, Luis delaCruz-Merino, Fátima Toscano, Javier Valdivia, Victoria Castellón, Fernando Henao-Carrasco, Pilar Sancho, Juan-Luis Onieva-Zafra, and et al. 2022. "Genes Involved in Immune Reinduction May Constitute Biomarkers of Response for Metastatic Melanoma Patients Treated with Targeted Therapy" Biomedicines 10, no. 2: 284. https://doi.org/10.3390/biomedicines10020284