
Effectiveness and Safety Profiles of Biological Therapies in Inflammatory Bowel Disease: Real Life Data from an Active Pharmacovigilance Project


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Data Analyses
3. Results
3.1. Study Population
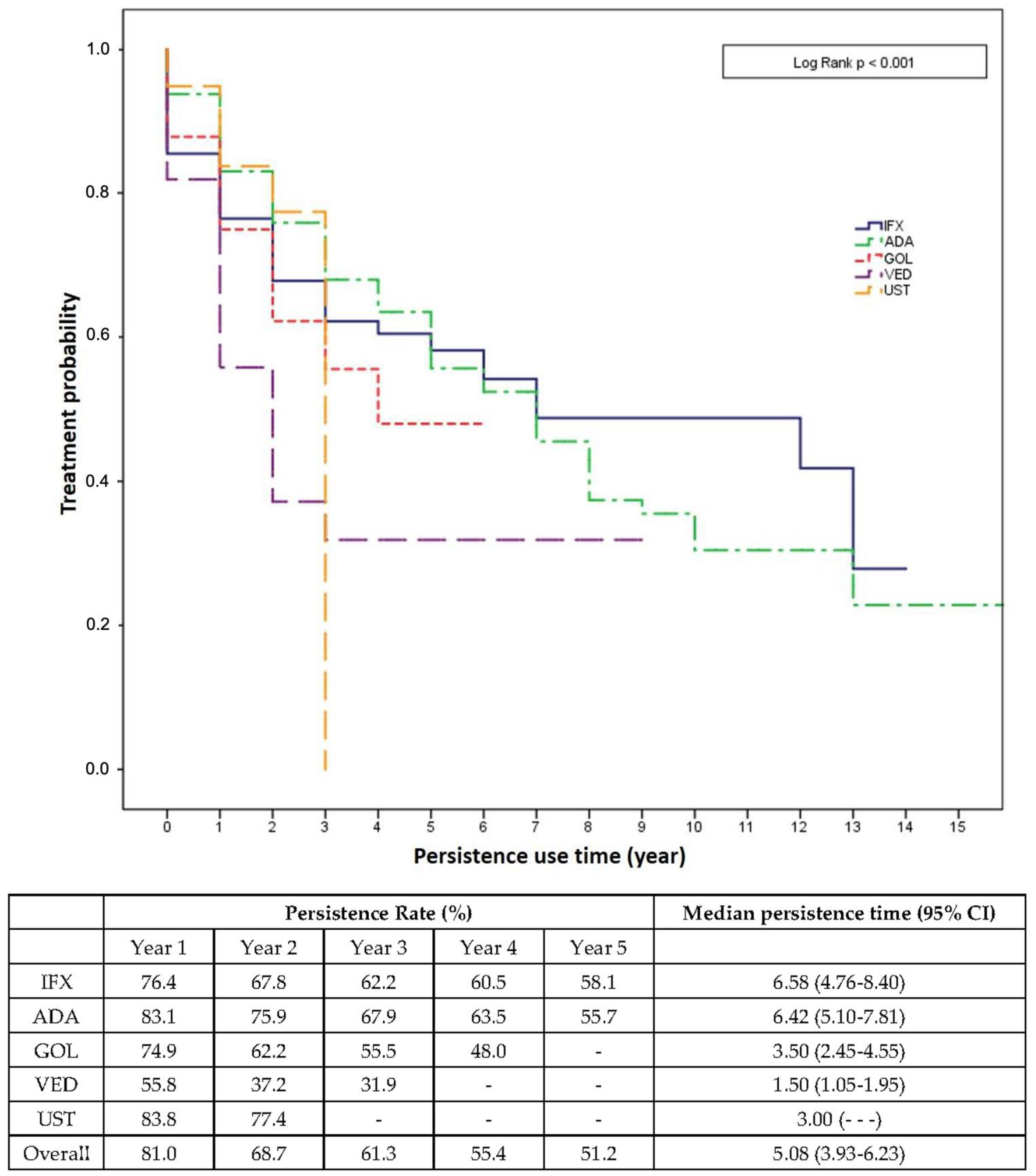
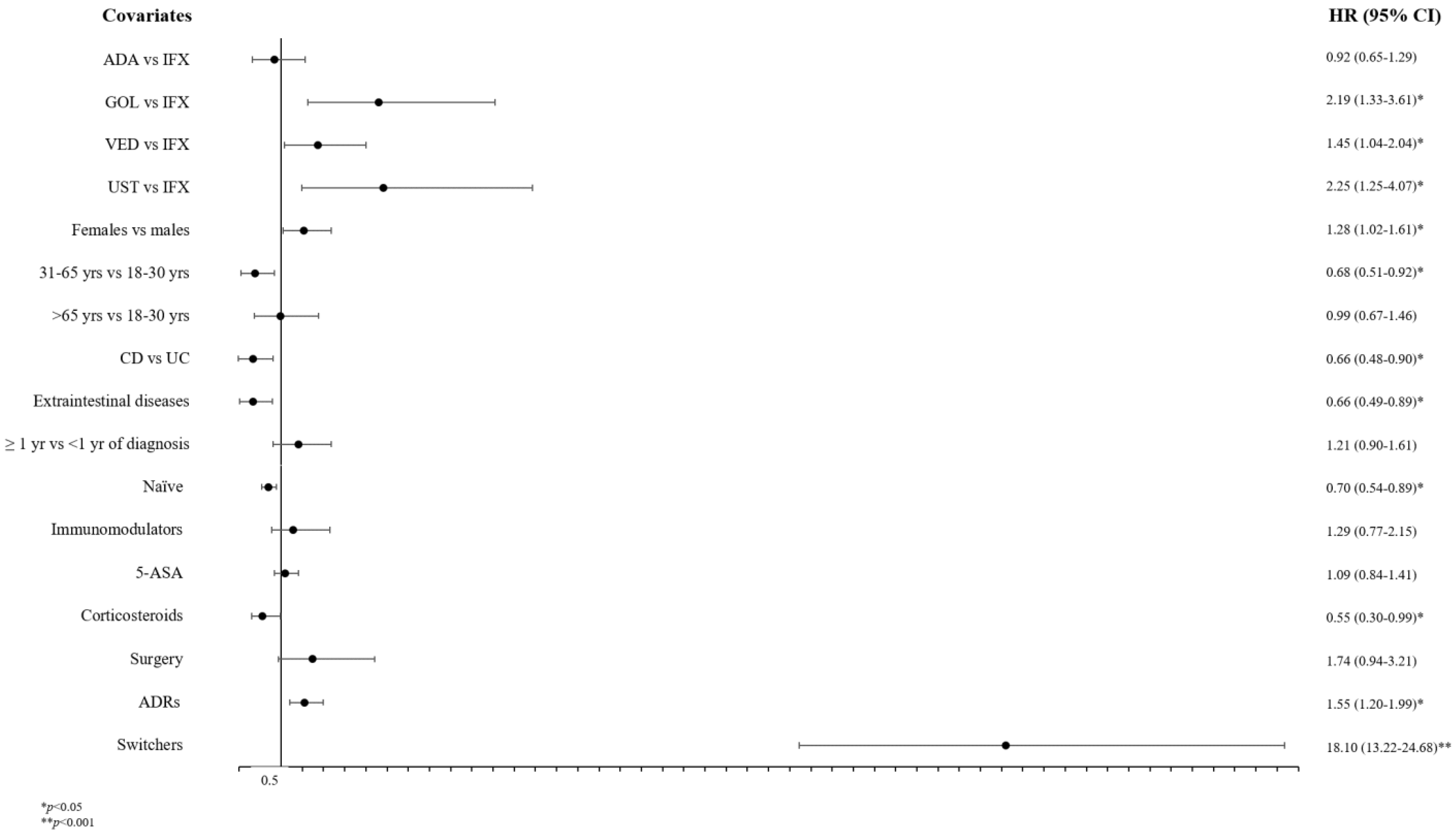
3.2. Persistence of Treatment
3.3. Description of Adverse Drug Reactions
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guan, Q. A Comprehensive Review and Update on the Pathogenesis of Inflammatory Bowel Disease. J. Immunol. Res 2019, 2019, 7247238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Bawardy, B.; Shivashankar, R.; Proctor, D.D. Novel and Emerging Therapies for Inflammatory Bowel Disease. Front. Pharm. 2021, 12, 651415. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, G.G. The Global Burden of IBD: From 2015 to 2025. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Gönczi, L.; Lakatos, P.L.; Burisch, J. The Burden of Inflammatory Bowel Disease in Europe in 2020. J. Crohn’s Colitis 2021, 15, 1573–1587. [Google Scholar] [CrossRef] [PubMed]
- Crocetti, E.; Bergamaschi, W.; Russo, A.G. Population-Based Incidence and Prevalence of Inflammatory Bowel Diseases in Milan (Northern Italy), and Estimates for Italy. Eur. J. Gastroenterol. Hepatol. 2021, 33, e383–e389. [Google Scholar] [CrossRef] [PubMed]
- Gionchetti, P.; Rizzello, F.; Annese, V.; Armuzzi, A.; Biancone, L.; Castiglione, F.; Comberlato, M.; Cottone, M.; Danese, S.; Daperno, M.; et al. Use of Corticosteroids and Immunosuppressive Drugs in Inflammatory Bowel Disease: Clinical Practice Guidelines of the Italian Group for the Study of Inflammatory Bowel Disease. Dig. Liver Dis. 2017, 49, 604–617. [Google Scholar] [CrossRef] [Green Version]
- Biancone, L.; Annese, V.; Ardizzone, S.; Armuzzi, A.; Calabrese, E.; Caprioli, F.; Castiglione, F.; Comberlato, M.; Cottone, M.; Danese, S.; et al. Safety of Treatments for Inflammatory Bowel Disease: Clinical Practice Guidelines of the Italian Group for the Study of Inflammatory Bowel Disease (IG-IBD). Dig. Liver Dis. 2017, 49, 338–358. [Google Scholar] [CrossRef] [PubMed]
- Hurd, L.B.; Lichtenstein, G.R. Therapeutic Potential of Infliximab in Inflammatory Bowel Disease. Gastroenterol. Nurs. 1999, 22, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, C.; Grunert, P.C.; Stallmach, A. An Update for Pharmacologists on New Treatment Options for Inflammatory Bowel Disease: The Clinicians’ Perspective. Front. Pharm. 2021, 12, 655054. [Google Scholar] [CrossRef]
- Holdam, A.S.K.; Bager, P.; Dahlerup, J.F. Biological Therapy Increases the Health-Related Quality of Life in Patients with Inflammatory Bowel Disease in a Clinical Setting. Scand. J. Gastroenterol. 2016, 51, 706–711. [Google Scholar] [CrossRef]
- Gupta, A.; Yu, A.; Peyrin-Biroulet, L.; Ananthakrishnan, A.N. Treat to Target: The Role of Histologic Healing in Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2021, 19, 1800–1813. [Google Scholar] [CrossRef] [PubMed]
- Samaan, M.; Campbell, S.; Cunningham, G.; Tamilarasan, A.G.; Irving, P.M.; McCartney, S. Biologic Therapies for Crohn’s Disease: Optimising the Old and Maximising the New. F1000Research 2019, 8, 1210. [Google Scholar] [CrossRef] [PubMed]
- Moreno, L.O.; Fernández-Tomé, S.; Abalo, R. Biological Treatments in Inflammatory Bowel Disease: A Complex Mix of Mechanisms and Actions. Biologics 2021, 1, 189–210. [Google Scholar] [CrossRef]
- Macaluso, F.S.; Maida, M.; Grova, M.; Crispino, F.; Teresi, G.; Orlando, A.; Orlando, A. Head-to-Head Comparison of Biological Drugs for Inflammatory Bowel Disease: From Randomized Controlled Trials to Real-World Experience. Ther. Adv. Gastroenterol. 2021, 14, 175628482110106. [Google Scholar] [CrossRef] [PubMed]
- Click, B.; Regueiro, M. A Practical Guide to the Safety and Monitoring of New IBD Therapies. Inflamm. Bowel Dis. 2019, 25, 831–842. [Google Scholar] [CrossRef] [PubMed]
- Holmer, A.; Singh, S. Overall and Comparative Safety of Biologic and Immunosuppressive Therapy in Inflammatory Bowel Diseases. Expert Rev. Clin. Immunol. 2019, 15, 969–979. [Google Scholar] [CrossRef]
- Pantic, I.; Jevtic, D.; Nordstrom, C.W.; Madrid, C.; Milovanovic, T.; Dumic, I. Clinical Manifestations of Leukocytoclastic Vasculitis, Treatment, and Outcome in Patients with Ulcerative Colitis: A Systematic Review of the Literature. J. Clin. Med. 2022, 11, 739. [Google Scholar] [CrossRef]
- Roberti, R.; Iannone, L.F.; Palleria, C.; De Sarro, C.; Spagnuolo, R.; Barbieri, M.A.; Vero, A.; Manti, A.; Pisana, V.; Fries, W.; et al. Safety Profiles of Biologic Agents for Inflammatory Bowel Diseases: A Prospective Pharmacovigilance Study in Southern Italy. Curr. Med. Res. Opin. 2020, 36, 1457–1463. [Google Scholar] [CrossRef]
- Barbieri, M.A.; Cicala, G.; Cutroneo, P.M.; Gerratana, E.; Palleria, C.; De Sarro, C.; Vero, A.; Iannone, L.; Manti, A.; Russo, E.; et al. Safety Profile of Biologics Used in Rheumatology: An Italian Prospective Pharmacovigilance Study. J. Clin. Med. 2020, 9, 1227. [Google Scholar] [CrossRef]
- Satsangi, J. The Montreal Classification of Inflammatory Bowel Disease: Controversies, Consensus, and Implications. Gut 2006, 55, 749–753. [Google Scholar] [CrossRef]
- Fine, S.; Papamichael, K.; Cheifetz, A.S. Etiology and Management of Lack or Loss of Response to Anti-Tumor Necrosis Factor Therapy in Patients With Inflammatory Bowel Disease. Gastroenterol. Hepatol. 2019, 15, 656–665. [Google Scholar]
- European Medicines Agency Guideline on Good Pharmacovigilance Practices (GVP) Annex I—Definitions (Rev 4). Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-good-pharmacovigilance-practices-annex-i-definitions-rev-4_en.pdf (accessed on 31 October 2022).
- Olivera, P.; Thiriet, L.; Luc, A.; Baumann, C.; Danese, S.; Peyrin-Biroulet, L. Treatment Persistence for Infliximab Versus Adalimumab in Crohn’s Disease. Inflamm. Bowel Dis. 2017, 23, 976–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, Y.S.; Han, M.; Park, S.; Cheon, J.H. Biologic Use Patterns and Predictors for Non-Persistence and Switching of Biologics in Patients with Inflammatory Bowel Disease: A Nationwide Population-Based Study. Dig. Dis. Sci. 2020, 65, 1436–1444. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Hartzema, A.G.; Xiao, H.; Wei, Y.J.; Chaudhry, N.; Ewelukwa, O.; Glover, S.C.; Zimmermann, E.M. Real-World Pattern of Biologic Use in Patients with Inflammatory Bowel Disease: Treatment Persistence, Switching, and Importance of Concurrent Immunosuppressive Therapy. Inflamm. Bowel Dis. 2019, 25, 1417–1427. [Google Scholar] [CrossRef]
- Mahlich, J.; May, M.; Feig, C.; Straub, V.; Schmelz, R. Persistence with Biologic Therapy and Associated Costs of Patients with Inflammatory Bowel Disease: A German Retrospective Claims Data Analysis. J. Crohn’s Colitis 360 2021, 3, otab011. [Google Scholar] [CrossRef]
- Yokoyama, K.; Yamazaki, K.; Katafuchi, M.; Ferchichi, S. A Retrospective Claims Database Study on Drug Utilization in Japanese Patients with Crohn’s Disease Treated with Adalimumab or Infliximab. Adv. Ther. 2016, 33, 1947–1963. [Google Scholar] [CrossRef] [Green Version]
- Mevius, A.; Brandes, A.; Hardtstock, F.; Wilke, T.; Ratsch, B.A.; Orzechowski, H.D.; Fuchs, A.; Deiters, B.; Bokemeyer, B. Persistence with Biologic Treatment in Patients with Inflammatory Bowel Disease: A German Claims Data Analysis. Digestion 2021, 102, 216–226. [Google Scholar] [CrossRef]
- Stallmach, A.; Langbein, C.; Atreya, R.; Bruns, T.; Dignass, A.; Ende, K.; Hampe, J.; Hartmann, F.; Neurath, M.F.; Maul, J.; et al. Vedolizumab Provides Clinical Benefit over 1 Year in Patients with Active Inflammatory Bowel Disease—A Prospective Multicenter Observational Study. Aliment. Pharmacol. Ther. 2016, 44, 1199–1212. [Google Scholar] [CrossRef]
- Chien, T.H.; Puig, A.; Khuong, T.; Kouhkamari, M.H.; Che, S.; Huang, T.H.-W. An Australian Real-World Study of Treatment Persistence of Ustekinumab in Crohn’s Disease. Biologics 2021, 15, 237–245. [Google Scholar] [CrossRef]
- Viola, A.; Muscianisi, M.; Macaluso, F.S.; Ventimiglia, M.; Cappello, M.; Privitera, A.C.; Magnano, A.; Pluchino, D.; Magrì, G.; Ferracane, C.; et al. Ustekinumab in Crohn’s Disease: Real-world Outcomes from the Sicilian Network for Inflammatory Bowel Diseases. JGH Open 2021, 5, 364–370. [Google Scholar] [CrossRef]
- Parikh, A.; Fox, I.; Leach, T.; Xu, J.; Scholz, C.; Patella, M.; Feagan, B.G. Long-Term Clinical Experience with Vedolizumab in Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2013, 19, 1691–1699. [Google Scholar] [CrossRef] [PubMed]
- Sands, B.E.; Sandborn, W.J.; van Assche, G.; Lukas, M.; Xu, J.; James, A.; Abhyankar, B.; Lasch, K. Vedolizumab as Induction and Maintenance Therapy for Crohn’s Disease in Patients Naïve to or Who Have Failed Tumor Necrosis Factor Antagonist Therapy. Inflamm. Bowel Dis. 2017, 23, 97–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandborn, W.J.; Feagan, B.G.; Danese, S.; O’Brien, C.D.; Ott, E.; Marano, C.; Baker, T.; Zhou, Y.; Volger, S.; Tikhonov, I.; et al. Safety of Ustekinumab in Inflammatory Bowel Disease: Pooled Safety Analysis of Results from Phase 2/3 Studies. Inflamm. Bowel Dis. 2021, 27, 994–1007. [Google Scholar] [CrossRef] [PubMed]
- Sandborn, W.J.; Feagan, B.G.; Marano, C.; Zhang, H.; Strauss, R.; Johanns, J.; Adedokun, O.J.; Guzzo, C.; Colombel, J.-F.; Reinisch, W.; et al. Subcutaneous Golimumab Induces Clinical Response and Remission in Patients With Moderate-to-Severe Ulcerative Colitis. Gastroenterology 2014, 146, 85–95. [Google Scholar] [CrossRef]
- Ko, Y.; Paramsothy, S.; Yau, Y.; Leong, R.W. Superior Treatment Persistence with Ustekinumab in Crohn’s Disease and Vedolizumab in Ulcerative Colitis Compared with Anti-TNF Biological Agents: Real-world Registry Data from the Persistence Australian National IBD Cohort (PANIC) Study. Aliment. Pharmacol. Ther. 2021, 54, 292–301. [Google Scholar] [CrossRef]
- Sah, J.; Teeple, A.; Muser, E.; Gutierrez, C.; Dassopoulos, T. Treatment Persistence and Maintenance Dose Titration among Ulcerative Colitis Patients on Biologics: A Pooled Study of Three United States Claim Databases. Curr. Med. Res. Opin. 2022, 38, 1093–1101. [Google Scholar] [CrossRef]
- Lie, M.R.K.L.; Kreijne, J.E.; Van Der Woude, C.J. Sex Is Associated with Adalimumab Side Effects and Drug Survival in Patients with Crohn’s Disease. Inflamm. Bowel Dis. 2017, 23, 75–81. [Google Scholar] [CrossRef] [Green Version]
- Lopez, A.; Billioud, V.; Peyrin-Biroulet, C.; Peyrin-Biroulet, L. Adherence to Anti-TNF Therapy in Inflammatory Bowel Diseases: A Systematic Review. Inflamm. Bowel Dis. 2013, 19, 1528–1533. [Google Scholar] [CrossRef]
- Greuter, T.; Manser, C.; Pittet, V.; Vavricka, S.R.; Biedermann, L. Gender Differences in Inflammatory Bowel Disease. Digestion 2020, 101, 98–104. [Google Scholar] [CrossRef]
- Bucci, C.; Zingone, F.; Tammaro, S.; Iovino, P.; Santonicola, A.; Ciacci, C. Factors Predicting the Adherence to the Therapy of Italian IBD Patients. Gastroenterol. Res. Pract. 2017, 2017, 719345. [Google Scholar] [CrossRef] [Green Version]
- Roblin, X.; Genin, C.; Nancey, S.; Williet, N.; Veyrard, P.; Boschetti, G.; Phelip, J.-M.; Berger, A.-E.; Killian, M.; Waeckel, L.; et al. Swapping Versus Dose Optimization in Patients Losing Response to Adalimumab With Adequate Drug Levels. Inflamm. Bowel Dis. 2022, 28, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Sall Jensen, M.; Knudsen, T.; Kelsen, J.; Coskun, M.; Kjellberg, J.; Burisch, J. Trends in the Use of Biologicals and Their Treatment Outcomes among Patients with Inflammatory Bowel Diseases—A Danish Nationwide Cohort Study. Aliment. Pharmacol. Ther. 2022, 55, 541–557. [Google Scholar] [CrossRef] [PubMed]
- Perrig, K.; Krupka, N.; Bruno, S.; Jordi, U.; Rossel, J.; Biedermann, L.; Greuter, T.; Schreiner, P.; Vavricka, S.R.; Juillerat, P.; et al. Effectiveness of Golimumab in Patients with Ulcerative Colitis: Results of a Real-Life Study in Switzerland. Ther. Adv. Gastroenterol. 2022, 15, 17562848221074188. [Google Scholar] [CrossRef] [PubMed]
- Taxonera, C.; Rodríguez, C.; Bertoletti, F.; Menchén, L.; Arribas, J.; Sierra, M.; Arias, L.; Martínez-montiel, P.; Juan, A.; Acosta, M.B.; et al. Clinical Outcomes of Golimumab as First, Second or Third Anti-TNF Agent in Patients with Moderate-to-Severe Ulcerative Colitis. Inflamm. Bowel Dis. 2017, 23, 1394–1402. [Google Scholar] [CrossRef] [PubMed]
- Iborra, M.; García-Morales, N.; Rubio, S.; Bertoletti, F.; Calvo, M.; Taxonera, C.; Boscá-Watts, M.M.; Sierra, M.; Mancenido, N.; Beltrán, B.; et al. Real-Life Experience with 4 Years of Golimumab Persistence in Ulcerative Colitis Patients. Sci. Rep. 2020, 10, 17774. [Google Scholar] [CrossRef]
- Viola, A.; Pugliese, D.; Renna, S.; Furfaro, F.; Caprioli, F.; D’Incà, R.; Bossa, F.; Mazza, S.; Costantino, G.; Fantini, M.C.; et al. Outcome in Ulcerative Colitis after Switch from Adalimumab/Golimumab to Infliximab: A Multicenter Retrospective Study. Dig. Liver Dis. 2019, 51, 510–515. [Google Scholar] [CrossRef]
- Irving, P.M.; de Lusignan, S.; Tang, D.; Nijher, M.; Barrett, K. Risk of Common Infections in People with Inflammatory Bowel Disease in Primary Care: A Population-Based Cohort Study. BMJ Open Gastroenterol. 2021, 8, e000573. [Google Scholar] [CrossRef]
- Helwig, U.; Mross, M.; Schubert, S.; Hartmann, H.; Brandes, A.; Stein, D.; Kempf, C.; Knop, J.; Campbell-Hill, S.; Ehehalt, R. Real-World Clinical Effectiveness and Safety of Vedolizumab and Anti-Tumor Necrosis Factor Alpha Treatment in Ulcerative Colitis and Crohn’s Disease Patients: A German Retrospective Chart Review. BMC Gastroenterol. 2020, 20, 211. [Google Scholar] [CrossRef]
- Singh, S.; Facciorusso, A.; Dulai, P.S.; Jairath, V.; Sandborn, W.J. Comparative Risk of Serious Infections with Biologic and/or Immunosuppressive Therapy in Patients with Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2020, 18, 69–81. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Xiong, B.; Li, X.; Xu, T.; Yu, M. Meta-Analysis: Serious Adverse Events in Crohn’s Disease Patients Treated with TNF-Alpha Inhibitors. Hepatogastroenterology 2013, 60, 1333–1342. [Google Scholar] [CrossRef]
- Cheng, D.; Kochar, B.D.; Cai, T.; Ananthakrishnan, A.N. Risk of Infections With Ustekinumab and Tofacitinib Compared to Tumor Necrosis Factor α Antagonists in Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2022, 20, 2366–2372. [Google Scholar] [CrossRef] [PubMed]
- Wheat, C.L.; Ko, C.W.; Clark-Snustad, K.; Grembowski, D.; Thornton, T.A.; Devine, B. Inflammatory Bowel Disease (IBD) Pharmacotherapy and the Risk of Serious Infection: A Systematic Review and Network Meta-Analysis. BMC Gastroenterol. 2017, 17, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahier, J.F.; Magro, F.; Abreu, C.; Armuzzi, A.; Ben-Horin, S.; Chowers, Y.; Cottone, M.; de Ridder, L.; Doherty, G.; Ehehalt, R.; et al. Second European Evidence-Based Consensus on the Prevention, Diagnosis and Management of Opportunistic Infections in Inflammatory Bowel Disease. J. Crohn’s Colitis 2014, 8, 443–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camilleri, M. Leaky Gut: Mechanisms, Measurement and Clinical Implications in Humans. Gut 2019, 68, 1516–1526. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Sun, Y.; Shao, X.; Zhou, Y.; Yu, Y.; Kuai, X.; Zhou, C. Leaky Gut in IBD: Intestinal Barrier–Gut Microbiota Interaction. J. Microbiol. Biotechnol. 2022, 32, 825–834. [Google Scholar] [CrossRef]
- Lambert, J.L.W.; de Schepper, S.; Speeckaert, R. Cutaneous Manifestations in Biological-Treated Inflammatory Bowel Disease Patients: A Narrative Review. J. Clin. Med. 2021, 10, 1040. [Google Scholar] [CrossRef]
- Neri, B.; Scribano, M.L.; Armuzzi, A.; Castiglione, F.; D’Incà, R.; Orlando, A.; Festa, S.; Riegler, G.; Fries, W.; Meucci, G.; et al. Incident Colorectal Cancer in Inflammatory Bowel Disease. Cancers 2022, 14, 721. [Google Scholar] [CrossRef]
- Biancone, L.; Armuzzi, A.; Scribano, M.L.; Castiglione, F.; D’incà, R.; Orlando, A.; Papi, C.; Daperno, M.; Vecchi, M.; Riegler, G.; et al. Cancer Risk in Inflammatory Bowel Disease: A 6-Year Prospective Multicenter Nested Case–Control IG-IBD Study. Inflamm. Bowel Dis. 2019, 26, 450–459. [Google Scholar] [CrossRef]
- Greuter, T.; König, O. Malignancies in Inflammatory Bowel Disease. Digestion 2020, 101, 136–145. [Google Scholar] [CrossRef]
- Annese, V.; Beaugerie, L.; Egan, L.; Biancone, L.; Bolling, C.; Brandts, C.; Dierickx, D.; Dummer, R.; Fiorino, G.; Gornet, J.M.; et al. European Evidence-Based Consensus: Inflammatory Bowel Disease and Malignancies. J. Crohn’s Colitis 2015, 9, 945–965. [Google Scholar] [CrossRef] [Green Version]
- Beaugerie, L.; Itzkowitz, S.H. Cancers Complicating Inflammatory Bowel Disease. N. Engl. J. Med. 2015, 372, 1441–1452. [Google Scholar] [CrossRef] [PubMed]
- Vedamurthy, A.; Gangasani, N.; Ananthakrishnan, A.N. Vedolizumab or Tumor Necrosis Factor Antagonist Use and Risk of New or Recurrent Cancer in Patients with Inflammatory Bowel Disease with Prior Malignancy: A Retrospective Cohort Study. Clin. Gastroenterol. Hepatol. 2022, 20, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Heien, H.C.; Sangaralingham, L.; Shah, N.D.; Sandborn, W.J. Risk of Malignancy with Vedolizumab Versus Tumor Necrosis Factor-α Antagonists in Patients with Inflammatory Bowel Diseases. Dig. Dis. Sci. 2022, 67, 2510–2516. [Google Scholar] [CrossRef] [PubMed]
- Lasa, J.S.; Olivera, P.A.; Danese, S.; Peyrin-Biroulet, L. Efficacy and Safety of Biologics and Small Molecule Drugs for Patients with Moderate-to-Severe Ulcerative Colitis: A Systematic Review and Network Meta-Analysis. Lancet Gastroenterol. Hepatol. 2022, 7, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Peyrin-Biroulet, L.; Arkkila, P.; Armuzzi, A.; Danese, S.; Guardiola, J.; Jahnsen, J.; Lees, C.; Louis, E.; Lukáš, M.; Reinisch, W.; et al. Comparative Efficacy and Safety of Infliximab and Vedolizumab Therapy in Patients with Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. BMC Gastroenterol. 2022, 22, 291. [Google Scholar] [CrossRef]
- Yu, B.; Zhao, L.; Jin, S.; He, H.; Zhang, J.; Wang, X. Model-Based Meta-Analysis on the Efficacy of Biologics and Small Targeted Molecules for Crohn’s Disease. Front. Immunol. 2022, 13, 828219. [Google Scholar] [CrossRef]
- Singh, S.; Murad, M.H.; Fumery, M.; Sedano, R.; Jairath, V.; Panaccione, R.; Sandborn, W.J.; Ma, C. Comparative Efficacy and Safety of Biologic Therapies for Moderate-to-Severe Crohn’s Disease: A Systematic Review and Network Meta-Analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 1002–1014. [Google Scholar] [CrossRef]
- Barbieri, M.A.; Sorbara, E.E.; Cicala, G.; Santoro, V.; Cutroneo, P.M.; Franchina, T.; Spina, E. Adverse Drug Reactions with HER2-Positive Breast Cancer Treatment: An Analysis from the Italian Pharmacovigilance Database. Drugs Real World Outcomes 2022, 9, 91–107. [Google Scholar] [CrossRef]
- Barbieri, M.A.; Sorbara, E.E.; Battaglia, A.; Cicala, G.; Rizzo, V.; Spina, E.; Cutroneo, P.M. Adverse Drug Reactions with Drugs Used in Multiple Sclerosis: An Analysis from the Italian Pharmacovigilance Database. Front. Pharmacol. 2022, 13, 808370. [Google Scholar] [CrossRef]
- Scavone, C.; Sportiello, L.; Sullo, M.G.; Ferrajolo, C.; Ruggiero, R.; Sessa, M.; Berrino, P.M.; di Mauro, G.; Berrino, L.; Rossi, F.; et al. Safety Profile of Anticancer and Immune-Modulating Biotech Drugs Used in a Real World Setting in Campania Region (Italy): BIO-Cam Observational Study. Front. Pharmacol. 2017, 8, 607. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | CD (n = 392) | UC (n = 283) | p Value * | Total (n = 675) |
|---|---|---|---|---|
| Sex, n (%) | ||||
| Females | 158 (40.3) | 122 (43.1) | 0.466 | 280 (41.5) |
| Males | 234 (59.7) | 161 (56.9) | 395 (58.5) | |
| Median age (Q1–Q3) | 42.5 (28–57) | 45 (31–60) | 0.009 | 44 (29–58) |
| Median age at diagnosis (Q1–Q3) | 28 (20–41.8) | 34 (24–47) | <0.001 | 31 (21–44) |
| Naïve, n (%) | 265 (67.6) | 164 (58.0) | 0.013 | 429 (63.6) |
| Disease duration, median (Q1–Q3) | 8 (3–16) | 7 (2–14) | 0.184 | 8 (3–15) |
| Surgery, n (%) | 142 (36.2) | 12 (4.2) | <0.001 | 154 (22.8) |
| Smoking, n (%) | ||||
| Smoker | 121 (30.9) | 24 (8.5) | <0.001 | 145 (21.5) |
| Ex-smoker | 48 (12.2) | 58 (20.5) | 106 (15.7) | |
| Non-smoker | 223 (56.9) | 201 (71.0) | 424 (62.8) | |
| BMI, median (Q1–Q3) | 23 (20.9–26.3) | 24.1 (21.7–27.1) | 0.131 | 24 (21.3–26.4) |
| Comorbidities, median (Q1–Q3) | 0 (0–1) | 1 (0–2) | 0.490 | 1 (0–2) |
| Comorbidities, n (%) | ||||
| Anxiety–depressive disorders | 20 (5.1) | 8 (2.8) | 0.144 | 28 (4.1) |
| Cardiovascular disease | 25 (6.4) | 31 (11.0) | 0.033 | 56 (8.3) |
| Chronic kidney disease | 3 (0.8) | 11 (3.9) | 0.005 | 14 (2.1) |
| Chronic pulmonary disease | 10 (2.6) | 5 (1.8) | 0.495 | 15 (2.2) |
| Diabetes | 10 (2.6) | 22 (7.8) | 0.002 | 32 (4.7) |
| Dyslipidemia | 10 (2.6) | 16 (5.7) | 0.039 | 26 (3.9) |
| Hepatitis | 9 (2.3) | 12 (4.2) | 0.151 | 21 (3.1) |
| Hypertension | 48 (12.2) | 43 (15.2) | 0.268 | 91 (13.5) |
| Malignancies | 19 (4.8) | 8 (2.8) | 0.186 | 27 (4.0) |
| Osteoporosis | 13 (3.3) | 8 (2.8) | 0.718 | 21 (3.1) |
| Thyroid disorders | 18 (4.6) | 22 (7.8) | 0.084 | 40 (5.9) |
| Extraintestinal manifestations, n (%) | 80 (20.4) | 38 (13.4) | 0.024 | 118 (17.5) |
| Arthropathies | 48 (12.2) | 25 (8.8) | 0.159 | 73 (10.8) |
| Erythema nodosum | 11 (2.8) | 5 (1.8) | 0.381 | 16 (2.4) |
| Psoriasis | 18 (4.6) | 7 (2.5) | 0.150 | 25 (3.7) |
| Pyoderma gangrenosum | 3 (0.8) | 2 (0.7) | 0.930 | 5 (0.7) |
| Uveitis | 14 (3.6) | - | 14 (2.1) | |
| Concurrent non-biologics, median (Q1–Q3) | 1 (0–1) | 1 (0–1) | 0.658 | 1 (0–1) |
| Concurrent non-biologics, n (%) | ||||
| Mesalazine | 114 (29.1) | 207 (73.1) | <0.001 | 321 (47.6) |
| Azathioprine | 9 (2.3) | 8 (2.8) | 0.664 | 17 (2.5) |
| Corticosteroids | 9 (2.3) | 6 (2.1) | 0.878 | 15 (2.2) |
| Mercaptopurine | 4 (1.0) | 1 (0.4) | 0.319 | 5 (0.7) |
| Sulfasalazine | 8 (2.0) | 5 (1.8) | 0.798 | 13 (1.9) |
| Methotrexate | 2 (0.5) | 5 (1.8) | 0.112 | 7 (1.0) |
| Switched, n (%) | 127 (32.4) | 96 (33.9) | 0.740 | 223 (33.0) |
| Characteristic | IFX (n = 225) | ADA (n = 269) | GOL (n = 17) | VED (n = 145) | UST (n = 19) |
|---|---|---|---|---|---|
| Sex, n (%) | |||||
| Females | 84 (37.3) | 115 (42.8) | 10 (58.8) | 60 (41.4) | 11 (57.9) |
| Males | 141 (62.7) | 154 (57.2) | 7 (41.2) | 85 (58.6) | 8 (42.1) |
| Median age (Q1–Q3) | 38 (27–51) | 41 (28–55) | 49 (39–59) | 62 (44.5–71.5) | 38 (27–59) |
| Median age at diagnosis (Q1–Q3) | 29 (20–40) | 27 (20–40) | 34 (24–37.5) | 44 (25.5–63.0) | 24 (15–37) |
| Naïve, n (%) | 209 (92.9) | 210 (78.1) | - | 7 (4.8) | 3 (15.8) |
| Diagnosis, n (%) | |||||
| Crohn’s disease | 73 (32.4) | 249 (92.6) | - | 52 (35.9) | 17 (89.5) |
| Ulcerative colitis | 152 (67.6) | 20 (7.4) | 17 (100) | 93 (64.1) | 2 (10.5) |
| Disease duration, median (Q1–Q3) | 6 (2–13) | 8 (3–15) | 14 (5–24.5) | 10 (4–19.5) | 11 (7–17) |
| Surgery, n (%) | 21 (9.3) | 101 (37.5) | 1 (5.9) | 21 (14.5) | 10 (52.6) |
| Smoking, n (%) | |||||
| Smoker | 33 (14.7) | 79 (29.4) | 3 (17.6) | 26 (17.9) | 4 (21.1) |
| Ex-smoker | 31 (13.8) | 35 (13.0) | 4 (23.5) | 35 (24.1) | 1 (5.3) |
| Non-smoker | 161 (71.6) | 155 (57.6) | 10 (58.8) | 84 (57.9) | 14 (73.7) |
| BMI, median (Q1–Q3) | 24 (21.6–26.6) | 23.5 (20.9–26.4) | 27.3 (13.7–31.6) | 23.9 (22.7–31.8) | 23.1 (20.9–26.1) |
| Comorbidities, median (Q1–Q3) | 0 (0–1) | 0 (0–1) | 0 (0–1.0) | 1 (0–2) | 0 (0–1) |
| Comorbidities, n (%) | |||||
| Anxiety–depressive disorders | 6 (2.7) | 14 (5.2) | 1 (5.9) | 7 (4.8) | - |
| Cardiovascular disease | 18 (8.0) | 15 (5.6) | - | 23 (15.9) | - |
| Chronic kidney disease | 1 (0.5) | 3 (1.1) | - | 10 (6.9) | - |
| Chronic pulmonary disease | 5 (2.2) | 7 (2.6) | - | 3 (2.1) | - |
| Diabetes | 7 (3.1) | 5 (1.9) | 3 (17.6) | 16 (11.0) | 1 (5.3) |
| Dyslipidemia | 9 (4.0) | 6 (2.2) | - | 11 (7.4) | - |
| Hepatitis | 6 (2.8) | 5 (1.9) | 1 (5.9) | 9 (6.2) | - |
| Hypertension | 26 (11.6) | 23 (8.6) | - | 42 (29.0) | - |
| Malignancies | - | 7 (2.6) | - | 20 (13.8) | - |
| Osteoporosis | 5 (2.2) | 4 (1.5) | - | 10 (6.9) | 2 (10.5) |
| Thyroid disorders | 17 (7.6) | 12 (4.8) | 1 (5.9) | 9 (6.2) | - |
| Extraintestinal manifestations, n (%) | 38 (16.9) | 58 (21.6) | 3 (17.6) | 13 (9.0) | 6 (31.6) |
| Arthropathies | 22 (10.1) | 38 (14.1) | 2 (11.8) | 6 (4.1) | 4 (21.1) |
| Erythema nodosum | 7 (3.2) | 5 (1.9) | 1 (5.9) | 3 (2.1) | - |
| Psoriasis | 5 (2.3) | 12 (4.5) | - | 4 (2.8) | 4 (21.1) |
| Pyoderma gangrenosum | 2 (0.9) | 3 (1.1) | - | - | - |
| Uveitis | 2 (0.9) | 9 (3.3) | 1 (5.9) | 1 (0.7) | 1 (5.3) |
| Concurrent non-biologics, median (Q1–Q3) | 1 (0–1) | 0 (0–1) | 1 (0–1) | 1 (0–1) | 0 (0–0) |
| Concurrent non-biologics, n (%) | |||||
| Mesalazine | 126 (57.8) | 92 (34.2) | 12 (70.6) | 86 (59.3) | 2 (10.5) |
| Azathioprine | 7 (3.2) | 6 (2.2) | 1 (5.9) | 2 (1.4) | - |
| Corticosteroids | 8 (3.7) | 3 (1.1) | - | 3 (2.1) | 1 (5.3) |
| Mercaptopurine | 1 (0.5) | 3 (1.1) | - | 1 (0.7) | - |
| Sulfasalazine | 5 (2.3) | 6 (2.2) | 1 (5.9) | 1 (0.7) | - |
| Methotrexate | 3 (1.4) | 3 (1.1) | - | - | - |
| Switched, n (%) | 75 (33.3) | 93 (34.6) | 7 (41.2) | 44 (30.4) | - |
| Switch from | Switch to | ||||||
| IFX | ADA | GOL | |||||
| IFX | 2 (9) | 6 (9) | |||||
| ADA | 19 (5) | 2 | |||||
| GOL | 6 | - | |||||
| Swap from | Swap to | ||||||
| IFX | ADA | VED | GOL | UST | |||
| IFX | 29 (15) | 3 (2) | |||||
| ADA | 4 (4) | 44 (15) | |||||
| VED | 15 (3) | 4 | 5 | 13 (4) | |||
| GOL | 1 | - | |||||
| Drug (n. Treatments) | Total Years of Treatment | Number of Total Failures (PF + SF) | Failure/10 yrs | Total Number of ADRs | ADRs/10 yrs |
|---|---|---|---|---|---|
| IFX (277) | 710.8 | 54 | 0.8 | 95 | 1.3 |
| ADA (292) | 890 | 80 | 0.9 | 84 | 0.9 |
| GOL (50) | 61.3 | 22 | 3.6 | 7 | 1.1 |
| VED (215) | 336 | 60 | 1.8 | 40 | 1.2 |
| UST (118) | 90.3 | 11 | 1.2 | 23 | 2.5 |
| Type of ADR, n (Incidence per 10 Years of Treatment) | IFX | p Value * | ADA | p Value * | GOL | p Value * | VED | p Value * | UST | p Value * |
|---|---|---|---|---|---|---|---|---|---|---|
| SADRs # | 17 (0.2) | 0.258 | 22 (0.3) | 0.666 | 4 (0.7) | 0.926 | 19 (0.6) | 0.461 | 9 (1.0) | 0.989 |
| Infections | 22 (0.3) | 0.958 | 26 (0.3) | 0.431 | 4 (0.7) | 0.972 | 13 (0.4) | 0.259 | 10 (1.1) | 0.794 |
| Pneumonia | - | - | 4 (0.04) | 0.127 | - | - | 2 (0.1) | 0.703 | 1 (0.1) | - |
| Infusion/injection-related reaction | 36 (0.5) | <0.001 | 3 (0.03) | 0.001 | - | - | 1 (0.03) | - | 2 (0.2) | 0.125 |
| Skin reaction | 10 (0.1) | 0.703 | 24 (0.3) | <0.001 | 1 (0.2) | - | - | - | 3 (0.3) | 0.391 |
| Joint disease | 7 (0.1) | 0.025 | 3 (0.03) | 0.670 | - | - | 2 (0.1) | 0.623 | - | - |
| Perianal disease | 4 (0.1) | 0.592 | 3 (0.03) | 0.807 | - | - | 3 (0.1) | 0.707 | 1 (0.1) | - |
| Malignancies | 2 (0.03) | 0.220 | 3 (0.03) | 0.451 | 1 (0.2) | - | 8 (0.2) | 0.002 | - | - |
| Blood disorders | 2 (0.03) | 0.817 | 3 (0.03) | 0.302 | - | - | 1 (0.03) | - | - | - |
| Others | 11 (0.2) | 0.607 | 15 (0.2) | 0.537 | 1 (0.2) | - | 10 (0.3) | 0.911 | 6 (0.7) | 0.749 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbieri, M.A.; Viola, A.; Cicala, G.; Spina, E.; Fries, W. Effectiveness and Safety Profiles of Biological Therapies in Inflammatory Bowel Disease: Real Life Data from an Active Pharmacovigilance Project. Biomedicines 2022, 10, 3280. https://doi.org/10.3390/biomedicines10123280
Barbieri MA, Viola A, Cicala G, Spina E, Fries W. Effectiveness and Safety Profiles of Biological Therapies in Inflammatory Bowel Disease: Real Life Data from an Active Pharmacovigilance Project. Biomedicines. 2022; 10(12):3280. https://doi.org/10.3390/biomedicines10123280
Chicago/Turabian StyleBarbieri, Maria Antonietta, Anna Viola, Giuseppe Cicala, Edoardo Spina, and Walter Fries. 2022. "Effectiveness and Safety Profiles of Biological Therapies in Inflammatory Bowel Disease: Real Life Data from an Active Pharmacovigilance Project" Biomedicines 10, no. 12: 3280. https://doi.org/10.3390/biomedicines10123280