
Ten Years of KPC-Kp Bloodstream Infections Experience: Impact of Early Appropriate Empirical Therapy on Mortality

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Study
- to evaluate the impact of ceftazidime/avibactam in empirical therapy, either monotherapy or combination therapy, on mortality.
- to evaluate the impact of nephrotoxicity on mortality in a subgroup of patients treated with colistin or aminoglycoside as a part of combination regimens.
2.2. Inclusion Criteria and Definitions
2.3. Data Collection
2.4. Microbiological Methods
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Overall Population
3.2. Mortality
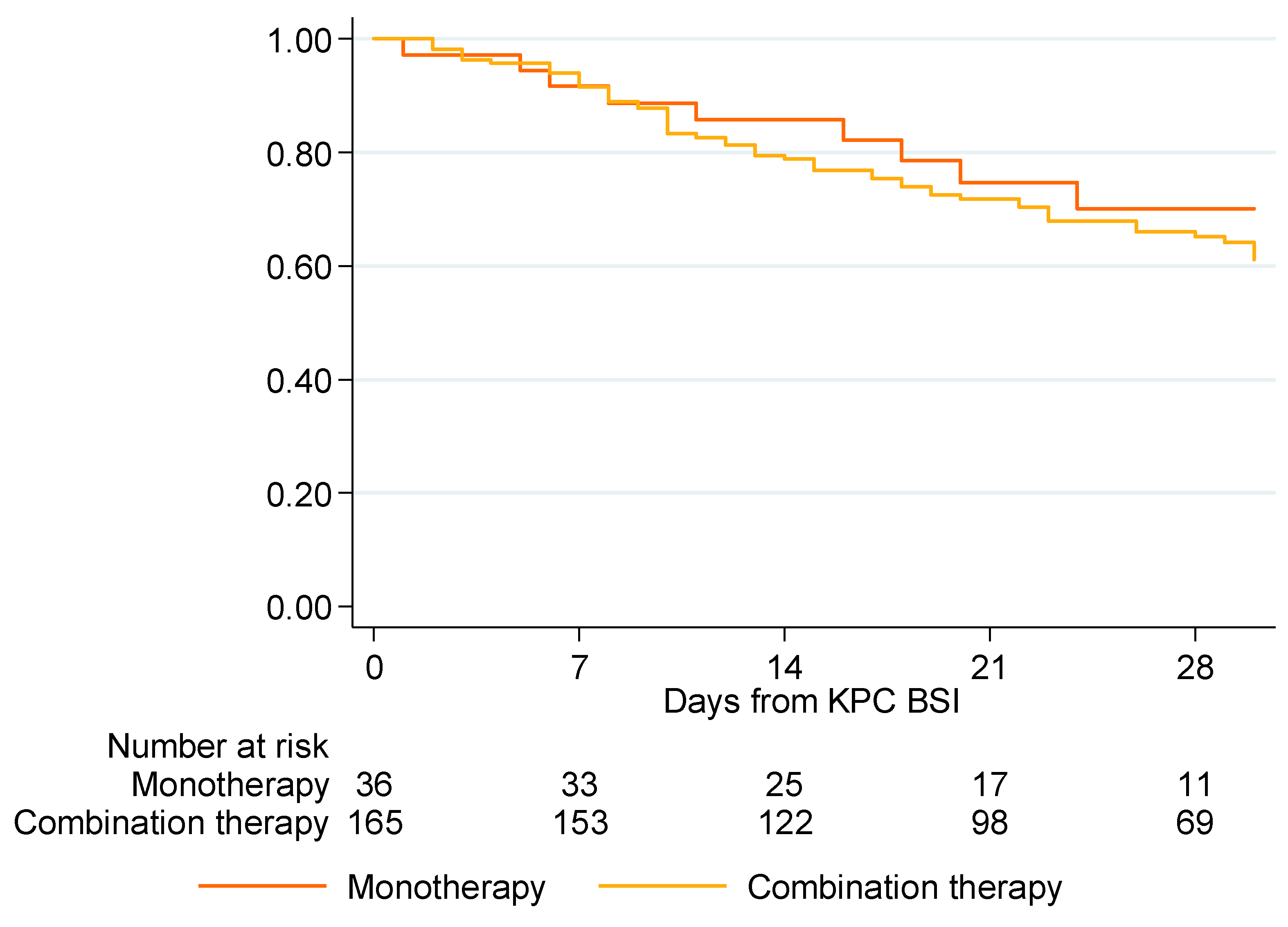
3.2.1. Impact of Appropriate Empirical Therapy, Either Monotherapy or Combination Therapy, on Mortality in Patients with Nosocomial-Onset KPC-Kp BSI
3.2.2. Crude and Adjusted Effects of Predictors of Mortality
3.2.3. Survival from Nephrotoxicity in Colistin- or Aminoglycoside-Treated Subgroup Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yigit, H.; Queenan, A.M.; Anderson, G.J.; Domenech-Sanchez, A.; Biddle, J.W.; Steward, C.D.; Alberti, S.; Bush, K.; Tenover, F.C. Novel carbapenem-hydrolyzing β-lactamase KPC-1 from a carbapenem-resistant strain of Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2001, 45, 1151–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fontana, C.; Favaro, M.; Sarmati, L.; Natoli, S.; Altieri, A.; Bossa, M.C.; Minelli, S.; Leonardis, F.; Favalli, C. Emergence of KPC-producing Klebsiella pneumoniae in Italy. BMC Res. Notes 2010, 3, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wendt, C.; Schütt, S.; Dalpke, A.H.; Konrad, M.; Mieth, M.; Trierweiler-Hauke, B.; Weigand, M.A.; Zimmermann, S.; Biehler, K.; Jonas, D. First outbreak of Klebsiella pneumoniae carbapenemase (KPC)-producing K. pneumoniae in Germany. Eur. J. Clin. Microbiol. 2010, 29, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Kontopoulou, K.; Protonotariou, E.; Vasilakos, K.; Kriti, M.; Koteli, A.; Antoniadou, E.; Sofianou, D. Hospital outbreak caused by Klebsiella pneumoniae producing KPC-2 beta-lactamase resistant to colistin. J. Hosp. Infect. 2010, 76, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Data from the ECDC Surveillance Atlas—Antimicrobial Resistance. Available online: https://atlas.ecdc.europa.eu/public/index.aspx (accessed on 1 November 2022).
- Tumbarello, M.; Viale, P.; Viscoli, C.; Trecarichi, E.M.; Tumietto, F.; Marchese, A.; Spanu, T.; Ambretti, S.; Ginocchio, F.; Cristini, F.; et al. Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae: Importance of combination therapy. Clin. Infect. Dis. 2012, 55, 943–950. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, E.B.; Tam, V.H. Detection and treatment options for Klebsiella pneumoniae carbapenemases (KPCs): An emerging cause of multidrug-resist- ant infection. J. Antimicrob. Chemother. 2010, 65, 1119–1125. [Google Scholar] [CrossRef] [Green Version]
- Daikos, G.L.; Markogiannakis, A. Carbapenemase-producing Klebsiella pneumoniae: (When) might we still consider treating with carbapenems? Clin. Microbiol. Infect. 2011, 17, 1135–1141. [Google Scholar] [CrossRef] [Green Version]
- Sbrana, F.; Malacarne, P.; Viaggi, B.; Costanzo, S.; Leonetti, P.; Leonildi, A.; Casini, B.; Tascini, C.; Menichetti, F. Carbapenem-sparing antibiotic regimens for infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae in intensive care unit. Clin. Infect. Dis. 2013, 56, 697–700. [Google Scholar] [CrossRef] [Green Version]
- Al-Hasan, M.N.; Lahr, B.D.; Eckel-Passow, J.E.; Baddour, L.M. Predictive scoring model of mortality in Gram-negative bloodstream infection. Clin. Microbiol. Infect. 2013, 19, 948–954. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez-Gutiérrez, B.; Salamanca, E.; de Cueto, M.; Hsueh, P.R.; Viale, P.; Paño-Pardo, J.R.; Venditti, M.; Tumbarello, M.; Daikos, G.; Pintado, V. Investigators from the REIPI/ESGBIS/INCREMENT Group. A Predictive Model of Mortality in Patients with Bloodstream Infections due to Carbapenemase-Producing Enterobacteriaceae. Mayo Clin. Proc. 2016, 91, 1362–1371. [Google Scholar] [CrossRef]
- Cano, Á.; Gutiérrez-Gutiérrez, B.; Machuca, I.; Torre-Giménez, J.; Frutos-Adame, A.; García-Gutiérrez, M.; Gallo-Marín, M.; Gracia-Ahufinger, I.; Artacho, M.J.; Natera, A.M.; et al. Association between rectal colonization by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae and mortality: A prospective, observational study. J. Glob. Antimicrob. Resist. 2022, 29, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, Z.A.; Paterson, D.L.; Potoski, B.A.; Kilayko, M.C.; Sandovsky, G.; Sordillo, E.; Polsky, B.; Adams-Haduch, J.M.; Doi, Y. Treatment outcome of bacteremia due to KPC-producing Klebsiella pneumoniae: Superiority of combination antimicrobial regimens. Antimicrob. Agents Chemother. 2012, 56, 2108–2113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadimitriou-Olivgeris, M.; Fligou, F.; Bartzavali, C.; Zotou, A.; Spyropoulou, A.; Koutsileou, K.; Vamvakopoulou, S.; Sioulas, N.; Karamouzos, V.; Anastassiou, E.D.; et al. Carbapenemase-producing Klebsiella pneumoniae bloodstream infection in critically ill patients: Risk factors and predictors of mortality. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1125–1131. [Google Scholar] [CrossRef] [PubMed]
- Tumbarello, M.; Trecarichi, E.M.; De Rosa, F.G.; Giannella, M.; Giacobbe, D.R.; Bassetti, M.; Losito, A.R.; Bartoletti, M.; Del Bono, V.; Corcione, S.; et al. Infections caused by KPC-producing Klebsiella pneumoniae: Differences in therapy and mortality in a multicentre study. J. Antimicrob. Chemother. 2015, 70, 2133–2143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Gutiérrez, B.; Salamanca, E.; de Cueto, M.; Hsueh, P.-R.; Viale, P.; Paño-Pardo, J.R.; Venditti, M.; Tumbarello, M.; Daikos, G.; Cantón, R.; et al. Effect of appropriate combination therapy on mortality of patients with bloodstream infections due to carbapenemase-producing Enterobacteriaceae (INCREMENT): A retrospective cohort study. Lancet Infect. Dis. 2017, 17, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.; Carmeli, Y.; Durante-Mangoni, E.; Mouton, J.W.; Tacconelli, E.; Theuretzbacher, U.; Mussini, C.; Leibovici, L. Combination therapy for carbapenem-resistant Gram-negative bacteria. J. Antimicrob. Chemother. 2014, 69, 2305–2309. [Google Scholar] [CrossRef] [Green Version]
- Tumbarello, M.; Trecarichi, E.M.; Corona, A.; DE Rosa, F.G.; Bassetti, M.; Mussini, C.; Menichetti, F.; Viscoli, C.; Campoli, C.; Venditti, M.; et al. Efficacy of ceftazidime-avibactam salvage therapy in patients with infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae. Clin. Infect. Dis. 2019, 68, 355–364. [Google Scholar] [CrossRef] [Green Version]
- Tumbarello, M.; Raffaelli, F.; Giannella, M.; Mantengoli, E.; Mularoni, A.; Venditti, M.; De Rosa, F.G.; Sarmati, L.; Bassetti, M.; Brindicci, G.; et al. Ceftazidime-Avibactam Use for Klebsiella pneumoniae Carbapenemase-Producing, K. pneumoniae Infections: A Retrospective Observational Multicenter Study. Clin. Infect. Dis. 2021, 73, 1664–1676. [Google Scholar] [CrossRef] [PubMed]
- SAS Institute Inc. SAS 9.1.3 Help and Documentation; SAS Institute Inc.: Cary, NC, USA, 2004; pp. 20015–22017. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 28.0; IBM Corp.: Armonk, NY, USA, 2021. [Google Scholar]
- Giannella, M.; Pascale, R.; Gutiérrez-Gutiérrez, B.; Cano, A.; Viale, P. The use of predictive scores in the management of patients with carbapenem-resistant Klebsiella pneumoniae infection. Expert Rev. Anti-Infect. Ther. 2019, 17, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Bassetti, M.; Tiseo, G.; Giordano, C.; Nencini, E.; Russo, A.; Graziano, E.; Tagliaferri, E.; Leonildi, A.; Barnini, S.; et al. Time to appropriate antibiotic therapy is a predictor of outcome in patients with bloodstream infection caused by KPC-producing Klebsiella pneumoniae. Crit. Care 2020, 24, 29. [Google Scholar] [CrossRef]
- Timsit, J.F.; Ruppé, E.; Barbier, F.; Tabah, A.; Bassetti, M. Bloodstream infections in critically ill patients: An expert statement. Intensive Care Med. 2020, 46, 266–284. [Google Scholar] [CrossRef] [PubMed]
- Timsit, J.-F.; Rupp, M.; Bouza, E.; Chopra, V.; Kärpänen, T.; Laupland, K.; Lisboa, T.; Mermel, L.; Mimoz, O.; Parienti, J.-J.; et al. A state of the art review on optimal practices to prevent, recognize, and manage complications associated with intravascular devices in the critically ill. Intensive Care Med. 2018, 44, 742–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnham, J.P.; Rojek, R.P.; Kollef, M.H. Catheter removal and outcomes of multidrug-resistant central-line-associated bloodstream infection. Medicine 2018, 97, e12782. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.; Carrara, E.; Retamar, P.; Tängdén, T.; Bitterman, R.; Bonomo, R.A.; de Waele, J.; Daikos, G.L.; Akova, M.; Harbarth, S.; et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European society of intensive care medicine). Clin. Microbiol. Infect. 2022, 28, 521–547. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America 2022 Guidance on the Treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin. Infect. Dis. 2022, 75, 187–212. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Appropriate Empirical Monotherapy (n = 36) | Appropriate Empirical Combination Therapy (n = 165) | Targeted Therapy (N = 112) | Total (n = 435) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||
| Sex | |||||||||
| Male | 24 | 66.67 | 102 | 61.82 | 68 | 60.71 | 273 | 62.76 | 0.92 |
| Female | 12 | 33.33 | 63 | 38.18 | 44 | 39.29 | 162 | 37.24 | |
| Age | |||||||||
| <50 | 7 | 19.44 | 34 | 20.61 | 16 | 14.29 | 74 | 17.01 | 0.33 |
| 50–59 | 5 | 13.89 | 35 | 21.21 | 27 | 24.11 | 82 | 18.85 | |
| 60–69 | 8 | 22.22 | 45 | 27.27 | 25 | 22.32 | 114 | 26.21 | |
| 70–79 | 13 | 36.11 | 40 | 24.24 | 32 | 28.57 | 126 | 28.97 | |
| 80+ | 3 | 8.33 | 11 | 6.67 | 12 | 10.71 | 39 | 8.97 | |
| Ward of admission | |||||||||
| Medical ward | 15 | 41.67 | 48 | 29.09 | 28 | 25 | 146 | 33.56 | 0.009 |
| Surgical ward | 9 | 25 | 61 | 36.97 | 52 | 46.43 | 162 | 37.24 | |
| Intensive care unit | 12 | 33.33 | 56 | 33.94 | 32 | 28.57 | 127 | 29.2 | |
| Charlson Comorbility index | |||||||||
| 0 | 3 | 8.33 | 8 | 4.85 | 3 | 2.68 | 21 | 4.83 | |
| 1 | 4 | 11.11 | 24 | 14.55 | 15 | 13.39 | 48 | 11.03 | |
| 2 | 6 | 16.67 | 28 | 16.97 | 20 | 17.86 | 67 | 15.4 | |
| 3 | 5 | 13.89 | 30 | 18.18 | 21 | 18.75 | 87 | 20 | |
| ≥4 | 18 | 50 | 75 | 45.45 | 53 | 47.32 | 212 | 48.74 | |
| KPC-Kp colonization | 25 | 69.44 | 138 | 83.64 | 78 | 69.64 | 324 | 74.48 | 0.004 |
| Probable source of KPC-Kp BSI: | |||||||||
| respiratory | 10 | 27.78 | 61 | 36.97 | 28 | 25 | 118 | 27.13 | 0.001 |
| urinary catheter | 29 | 80.56 | 142 | 86.06 | 100 | 89.29 | 362 | 83.22 | 0.001 |
| abdominal | 4 | 11.11 | 15 | 9.09 | 12 | 10.61 | 58 | 13.33 | 0.012 |
| Appropriate Empirical Monotherapy | Appropriate Empirical Combination Therapy | |
|---|---|---|
| Days | OS | OS |
| 0 | 1 | 1 |
| 7 | 0.9167 | 0.9148 |
| 14 | 0.8575 | 0.7881 |
| 21 | 0.7468 | 0.7186 |
| 28 | 0.7001 | 0.6511 |
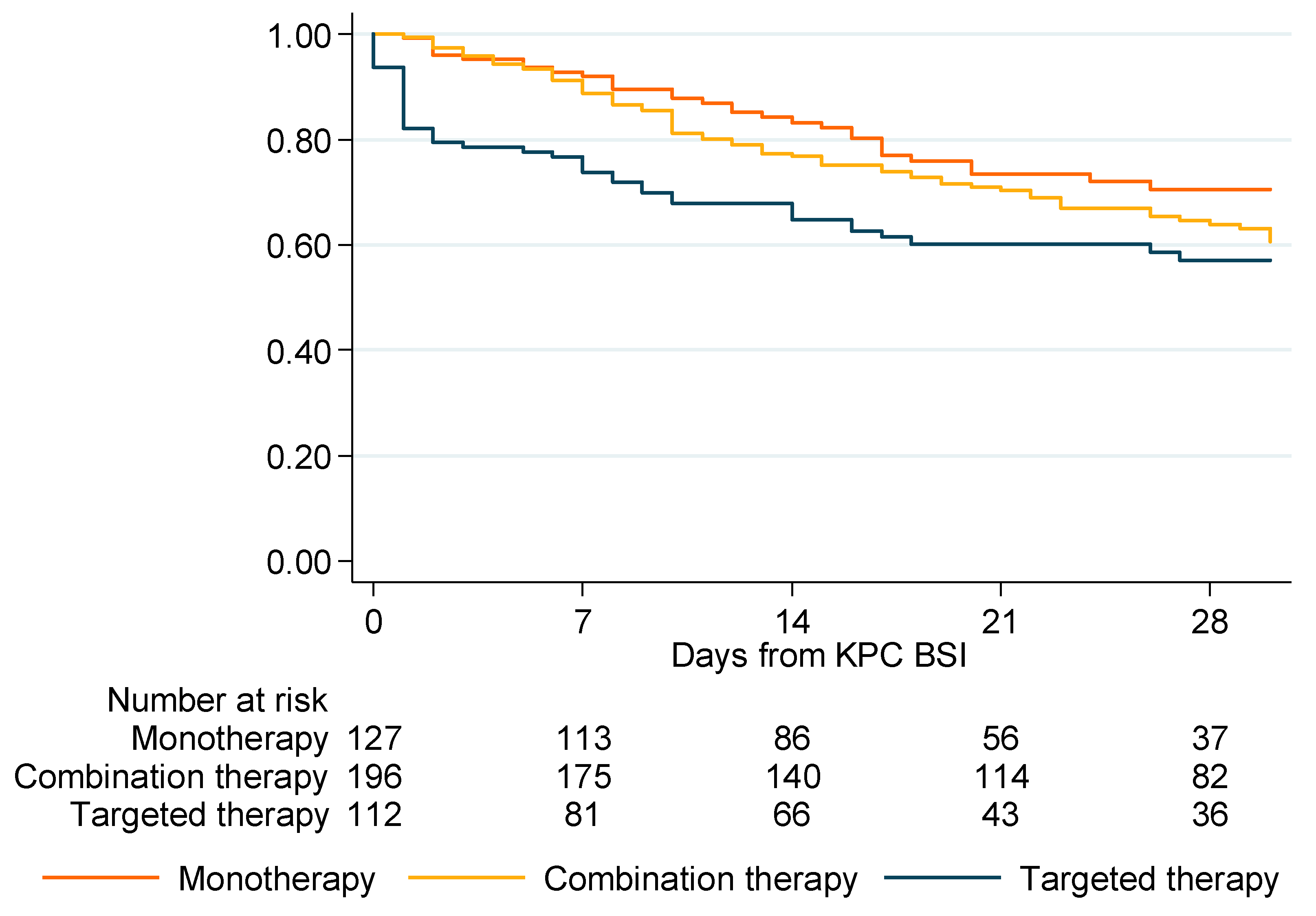
| Empirical Monotherapy | Empirical Combination Therapy | Targeted Therapy | |
|---|---|---|---|
| Days | OS | OS | OS |
| 0 | 1 | 1 | 1 |
| 7 | 0.9203 | 0.887 | 0.7381 |
| 14 | 0.8324 | 0.7684 | 0.6482 |
| 21 | 0.7347 | 0.703 | 0.6022 |
| 28 | 0.7045 | 0.6388 | 0.5705 |
| Crude Effect | Adjusted Effect | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | aHR | 95% CI | p | |
| Female sex | 0.92 | [0.68–1.24] | 0.572 | 1.01 | [0.75–1.38] | 0.929 |
| ICU admission | 1.02 | [0.75–1.39] | 0.892 | 0.96 | [0.70–1.31] | 0.799 |
| Age (every 10 years) | 1.05 | [0.95–1.17] | 0.322 | 1.04 | [0.93–1.18] | 0.473 |
| Charlson comorbidity index | ||||||
| 0 | 1 | 1 | ||||
| 1 | 0.81 | [0.36–1.81] | 0.612 | 0.69 | [0.30–1.54] | 0.362 |
| 2 | 0.91 | [0.43–1.94] | 0.814 | 0.9 | [0.43–1.89] | 0.785 |
| 3 | 1.11 | [0.54–2.29] | 0.781 | |||
| ≥4 | 1.14 | [0.57–2.25] | 0.716 | |||
| Probable source of KPC-Kp BSI otherthan urinary, CVC or abdominal | 1.78 | [1.31–2.42] | 0.000 | 1.64 | [1.15–2.34] | 0.006 |
| Source control | 0.62 | [0.44–0.86] | 0.005 | 0.77 | [0.52–1.13] | 0.179 |
| KPC-Kp colonization | 0.91 | [0.65–1.29] | 0.611 | 0.98 | [0.69–1.39] | 0.914 |
| Appropriate empirical therapy | ||||||
| Yes | 1 | |||||
| No | 0.8 | [0.55–1.15] | 0.226 | |||
| Only targeted therapy | 1.31 | [0.93–1.82] | 0.119 | |||
| Appropriate empirical therapy | 0.97 | [0.73–1.30] | 0.855 | 0.94 | [0.70–1.26] | 0.684 |
| Empirical monotherapy | ||||||
| Yes | 1 | |||||
| No | 1.3 | [0.90–1.88] | 0.164 | |||
| Only targeted therapy | 1.67 | [1.12–2.51] | 0.013 | |||
| Type of therapy | ||||||
| Appropriate empirical monotherapy | 1 | |||||
| Appropriate empirical combination therapy | 1.09 | [0.62–1.93] | 0.765 | |||
| Targeted therapy | 1.4 | [0.78–2.53] | 0.258 | |||
| Ceftazidime/avibactam in empirical therapy | 0.4 | [0.22–0.74] | 0.004 | |||
| Adjusted Effect | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Overall (n = 435) | Empirical Monotherapy (n = 127) | Empirical Combination Therapy (n = 196) | |||||||
| aHR | 95% CI | p | aHR | 95% CI | p | aHR | 95% CI | p | |
| Female | 1.01 | 0.74–1.37 | 0.969 | 2.61 | 1.30–5.25 | 0.007 | 0.68 | 0.43–1.09 | 0.107 |
| Age (every 10 years) | 1.04 | 0.93–1.18 | 0.484 | 1.32 | 0.99–1.76 | 0.063 | 0.95 | 0.81–1.12 | 0.558 |
| ICU admission | 0.93 | 0.68–1.27 | 0.648 | 1.39 | 0.69–2.79 | 0.36 | 0.76 | 0.49–1.20 | 0.237 |
| Charlson comorbidity index | |||||||||
| 0 | 1.00 | 1.00 | |||||||
| 1 | 0.65 | 0.28–1.46 | 0.294 | 0.15 | 0.01–1.47 | 0.103 | 1.55 | 0.41–5.86 | 0.52 |
| ≥2 | 0.86 | 0.41–1.82 | 0.701 | 0.24 | 0.07–0.88 | 0.031 | 2.08 | 0.57–7.52 | 0.266 |
| Probable source of KPC-Kp BSI other than urinary, CVC or abdominal | 1.65 | 1.17–2.33 | 0.005 | 1.82 | 0.91–3.62 | 0.09 | 1.64 | 0.95–2.83 | 0.077 |
| Source control | 0.72 | 0.49–1.06 | 0.099 | 1.01 | 0.48–2.11 | 0.981 | 0.63 | 0.35–1.11 | 0.112 |
| KPC-Kp colonization | 1.10 | 0.77–1.57 | 0.598 | 1.47 | 0.70–3.06 | 0.308 | 1.14 | 0.62–2.10 | 0.676 |
| Ceftazidime/avibactam in empirical therapy | 0.37 | 0.20–0.68 | 0.002 | 0.26 | 0.07–1.02 | 0.054 | 0.36 | 0.17–0.76 | 0.007 |
| No Nephrotoxicity | Nephrotoxicity | |
|---|---|---|
| Days | OS | OS |
| 0 | 1 | 1 |
| 7 | 0.9039 | 0.7184 |
| 14 | 0.8311 | 0.6203 |
| 21 | 0.7853 | 0.5330 |
| 28 | 0.6934 | 0.4565 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corcione, S.; De Benedetto, I.; Shbaklo, N.; Ranzani, F.; Mornese Pinna, S.; Castiglione, A.; Scabini, S.; Bianco, G.; Cavallo, R.; Mirabella, S.; et al. Ten Years of KPC-Kp Bloodstream Infections Experience: Impact of Early Appropriate Empirical Therapy on Mortality. Biomedicines 2022, 10, 3268. https://doi.org/10.3390/biomedicines10123268
Corcione S, De Benedetto I, Shbaklo N, Ranzani F, Mornese Pinna S, Castiglione A, Scabini S, Bianco G, Cavallo R, Mirabella S, et al. Ten Years of KPC-Kp Bloodstream Infections Experience: Impact of Early Appropriate Empirical Therapy on Mortality. Biomedicines. 2022; 10(12):3268. https://doi.org/10.3390/biomedicines10123268
Chicago/Turabian StyleCorcione, Silvia, Ilaria De Benedetto, Nour Shbaklo, Fabio Ranzani, Simone Mornese Pinna, Anna Castiglione, Silvia Scabini, Gabriele Bianco, Rossana Cavallo, Stefano Mirabella, and et al. 2022. "Ten Years of KPC-Kp Bloodstream Infections Experience: Impact of Early Appropriate Empirical Therapy on Mortality" Biomedicines 10, no. 12: 3268. https://doi.org/10.3390/biomedicines10123268