
Clinical Significance of Serum Elafin in Children with Inflammatory Bowel Disease

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study and Control Group
2.2. Methods
2.3. Statistical Analysis
2.4. Ethical Approval and Funding
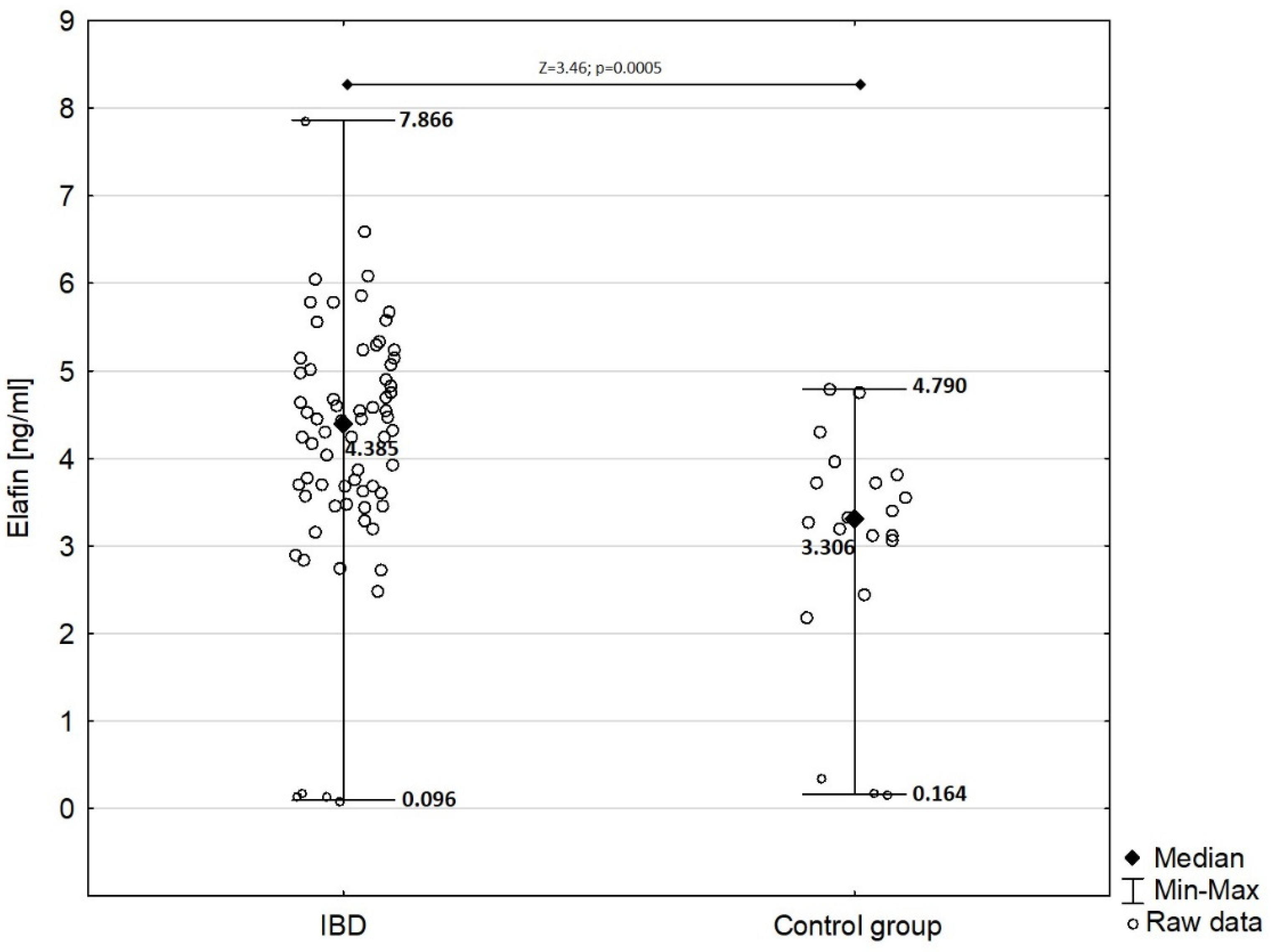
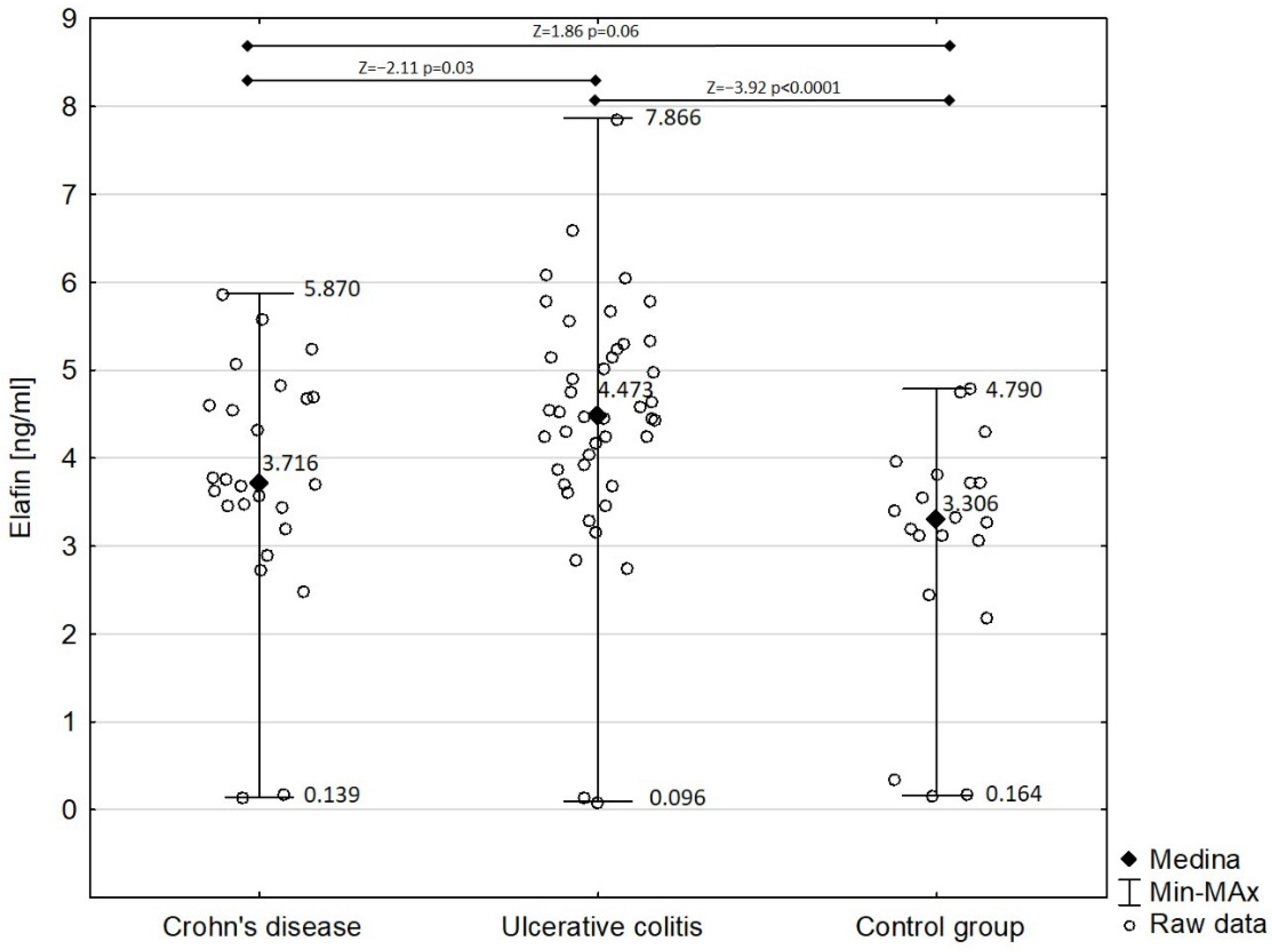
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ye, Y.; Manne, S.; Treem, W.R.; Bennett, D. Prevalence of Inflammatory Bowel Disease in Pediatric and Adult Populations: Recent Estimates from Large National Databases in the United States, 2007–2016. Inflamm. Bowel Dis. 2020, 26, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Duricova, D.; Burisch, J.; Jess, T.; Gower-Rousseau, C.; Lakatos, P.L.; ECCO-EpiCom. Age-related differences in presentation and course of inflammatory bowel disease: An update on the population-based literature. J. Crohns. Colitis 2014, 8, 1351–1361. [Google Scholar] [CrossRef]
- Collaborators, G.I.B.D. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 17–30. [Google Scholar] [CrossRef] [Green Version]
- Mackner, L.M.; Greenley, R.N.; Szigethy, E.; Herzer, M.; Deer, K.; Hommel, K.A. Psychosocial issues in pediatric inflammatory bowel disease: Report of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 449–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackner, L.M.; Sisson, D.P.; Crandall, W.V. Review: Psychosocial issues in pediatric inflammatory bowel disease. J. Pediatr. Psychol. 2004, 29, 243–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luther, J.; Dave, M. Rising Inflammatory Bowel Disease Prevalence Highlights the Need for Effective, Cost-Effective Therapies. Inflamm. Bowel Dis. 2020, 26, 626–627. [Google Scholar] [CrossRef]
- Kim, D.H.; Cheon, J.H. Pathogenesis of Inflammatory Bowel Disease and Recent Advances in Biologic Therapies. Immune Netw. 2017, 17, 25–40. [Google Scholar] [CrossRef] [Green Version]
- Prasad, S.V.; Fiedoruk, K.; Daniluk, T.; Piktel, E.; Bucki, R. Expression and Function of Host Defense Peptides at Inflammation Sites. Int. J. Mol. Sci. 2019, 21, 104. [Google Scholar] [CrossRef] [Green Version]
- Lei, J.; Sun, L.; Huang, S.; Zhu, C.; Li, P.; He, J.; Mackey, V.; Coy, D.H.; He, Q. The antimicrobial peptides and their potential clinical applications. Am. J. Transl. Res. 2019, 11, 3919–3931. [Google Scholar]
- van der Does, A.M.; Hiemstra, P.S.; Mookherjee, N. Antimicrobial Host Defence Peptides: Immunomodulatory Functions and Translational Prospects. Adv. Exp. Med. Biol. 2019, 1117, 149–171. [Google Scholar] [CrossRef]
- Wehkamp, J.; Schmid, M.; Stange, E.F. Defensins and other antimicrobial peptides in inflammatory bowel disease. Curr. Opin. Gastroenterol. 2007, 23, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Shaw, L.; Wiedow, O. Therapeutic potential of human elafin. Biochem. Soc. Trans. 2011, 39, 1450–1454. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.E.; Brown, T.I.; Roghanian, A.; Sallenave, J.M. SLPI and elafin: One glove, many fingers. Clin. Sci. 2006, 110, 21–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verrier, T.; Solhonne, B.; Sallenave, J.M.; Garcia-Verdugo, I. The WAP protein Trappin-2/Elafin: A handyman in the regulation of inflammatory and immune responses. Int. J. Biochem. Cell Biol. 2012, 44, 1377–1380. [Google Scholar] [CrossRef] [PubMed]
- Wiedow, O.; Schroder, J.M.; Gregory, H.; Young, J.A.; Christophers, E. Elafin: An elastase-specific inhibitor of human skin. Purification, characterization, and complete amino acid sequence. J. Biol. Chem. 1990, 265, 14791–14795. [Google Scholar] [CrossRef]
- Elgharib, I.; Khashaba, S.A.; Elsaid, H.H.; Sharaf, M.M. Serum elafin as a potential inflammatory marker in psoriasis. Int. J. Dermatol. 2019, 58, 205–209. [Google Scholar] [CrossRef]
- Chun, H.J.; Yu, P.B. Elafin in pulmonary arterial hypertension. Beyond targeting elastases. Am. J. Respir. Crit. Care Med. 2015, 191, 1217–1219. [Google Scholar] [CrossRef] [Green Version]
- Olewicz-Gawlik, A.; Trzybulska, D.; Graniczna, K.; Kuznar-Kaminska, B.; Katulska, K.; Batura-Gabryel, H.; Frydrychowicz, M.; Danczak-Pazdrowska, A.; Mozer-Lisewska, I. Serum alarm antiproteases in systemic sclerosis patients. Hum. Immunol. 2017, 78, 559–564. [Google Scholar] [CrossRef]
- Flach, C.F.; Eriksson, A.; Jennische, E.; Lange, S.; Gunnerek, C.; Lonnroth, I. Detection of elafin as a candidate biomarker for ulcerative colitis by whole-genome microarray screening. Inflamm. Bowel Dis. 2006, 12, 837–842. [Google Scholar] [CrossRef]
- Schmid, M.; Fellermann, K.; Fritz, P.; Wiedow, O.; Stange, E.F.; Wehkamp, J. Attenuated induction of epithelial and leukocyte serine antiproteases elafin and secretory leukocyte protease inhibitor in Crohn’s disease. J. Leukoc. Biol. 2007, 81, 907–915. [Google Scholar] [CrossRef]
- Motta, J.P.; Bermúdez-Humarán, L.G.; Deraison, C.; Martin, L.; Rolland, C.; Rousset, P.; Boue, J.; Dietrich, G.; Chapman, K.; Kharrat, P.; et al. Food-grade bacteria expressing elafin protect against inflammation and restore colon homeostasis. Sci. Transl. Med. 2012, 4, 158ra144. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Teng, G.; Wu, T.; Tian, Y.; Wang, H. Expression and Clinical Significance of Elafin in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2017, 23, 2134–2141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Ortiz, C.; Fontenot, L.; Xie, Y.; Ho, W.; Mattai, S.A.; Shih, D.Q.; Koon, H.W. High circulating elafin levels are associated with Crohn’s disease-associated intestinal strictures. PLoS ONE 2020, 15, e0231796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krawiec, P.; Pac-Kożuchowska, E. Cathelicidin—A Novel Potential Marker of Pediatric Inflammatory Bowel Disease. J. Inflamm. Res. 2021, 14, 163–174. [Google Scholar] [CrossRef]
- Krawiec, P.; Pac-Kożuchowska, E. Serum interleukin 17A and interleukin 17F in children with inflammatory bowel disease. Sci. Rep. 2020, 10, 12617. [Google Scholar] [CrossRef]
- Levine, A.; Koletzko, S.; Turner, D.; Escher, J.C.; Cucchiara, S.; de Ridder, L.; Kolho, K.L.; Veres, G.; Russell, R.K.; Paerregaard, A.; et al. ESPGHAN revised porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 795–806. [Google Scholar] [CrossRef] [Green Version]
- Levine, A.; Griffiths, A.; Markowitz, J.; Wilson, D.C.; Turner, D.; Russell, R.K.; Fell, J.; Ruemmele, F.M.; Walters, T.; Sherlock, M.; et al. Pediatric modification of the Montreal classification for inflammatory bowel disease: The Paris classification. Inflamm. Bowel Dis. 2011, 17, 1314–1321. [Google Scholar] [CrossRef]
- Hyams, J.S.; Ferry, G.D.; Mandel, F.S.; Gryboski, J.D.; Kibort, P.M.; Kirschner, B.S.; Griffiths, A.M.; Katz, A.J.; Grand, R.J.; Boyle, J.T.; et al. Development and validation of a pediatric Crohn’s disease activity index. J. Pediatr. Gastroenterol. Nutr. 1991, 12, 439–447. [Google Scholar] [CrossRef]
- Turner, D.; Otley, A.R.; Mack, D.; Hyams, J.; de Bruijne, J.; Uusoue, K.; Walters, T.D.; Zachos, M.; Mamula, P.; Beaton, D.E.; et al. Development, validation, and evaluation of a pediatric ulcerative colitis activity index: A prospective multicenter study. Gastroenterology 2007, 133, 423–432. [Google Scholar] [CrossRef]
- Hyams, J.S.; Di Lorenzo, C.; Saps, M.; Shulman, R.J.; Staiano, A.; van Tilburg, M. Functional Disorders: Children and Adolescents. Gastroenterology 2016, 150, 1456–1468. [Google Scholar] [CrossRef]
- Motta, J.-P.; Martin, L.; Vergnolle, N. Proteases/Antiproteases in Inflammatory Bowel Diseases. In Proteases and Their Receptors in Inflammation; Springer: Basel, Switzerland, 2011; pp. 173–215. [Google Scholar]
- Motta, J.P.; Magne, L.; Descamps, D.; Rolland, C.; Squarzoni-Dale, C.; Rousset, P.; Martin, L.; Cenac, N.; Balloy, V.; Huerre, M.; et al. Modifying the protease, antiprotease pattern by elafin overexpression protects mice from colitis. Gastroenterology 2011, 140, 1272–1282. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, P.A.; Hitt, M.; Xing, Z.; Wang, J.; Haslett, C.; Riemersma, R.A.; Webb, D.J.; Kotelevtsev, Y.V.; Sallenave, J.M. Adenoviral gene delivery of elafin and secretory leukocyte protease inhibitor attenuates NF-kappa B-dependent inflammatory responses of human endothelial cells and macrophages to atherogenic stimuli. J. Immunol. 2004, 172, 4535–4544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitch, P.M.; Roghanian, A.; Howie, S.E.; Sallenave, J.M. Human neutrophil elastase inhibitors in innate and adaptive immunity. Biochem. Soc. Trans. 2006, 34, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, P.A.; Devitt, A.; Kotelevtsev, Y.; Sallenave, J.M. Gene delivery of the elastase inhibitor elafin protects macrophages from neutrophil elastase-mediated impairment of apoptotic cell recognition. FEBS Lett. 2004, 574, 80–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, A.J.; Cunningham, G.A.; Porteous, D.J.; Haslett, C.; Sallenave, J.M. Regulation of adenovirus-mediated elafin transgene expression by bacterial lipopolysaccharide. Hum. Gene Ther. 2001, 12, 1395–1406. [Google Scholar] [CrossRef]
- McMichael, J.W.; Roghanian, A.; Jiang, L.; Ramage, R.; Sallenave, J.M. The antimicrobial antiproteinase elafin binds to lipopolysaccharide and modulates macrophage responses. Am. J. Respir. Cell Mol. Biol. 2005, 32, 443–452. [Google Scholar] [CrossRef] [Green Version]
- Sallenave, J.M.; Cunningham, G.A.; James, R.M.; McLachlan, G.; Haslett, C. Regulation of pulmonary and systemic bacterial lipopolysaccharide responses in transgenic mice expressing human elafin. Infect. Immun. 2003, 71, 3766–3774. [Google Scholar] [CrossRef] [Green Version]
- Roghanian, A.; Williams, S.E.; Sheldrake, T.A.; Brown, T.I.; Oberheim, K.; Xing, Z.; Howie, S.E.; Sallenave, J.M. The antimicrobial/elastase inhibitor elafin regulates lung dendritic cells and adaptive immunity. Am. J. Respir. Cell Mol. Biol. 2006, 34, 634–642. [Google Scholar] [CrossRef]
- Greuter, T.; Manser, C.; Pittet, V.; Vavricka, S.R.; Biedermann, L.; on behalf of Swiss IBDnet, an official working group of the Swiss Society of Gastroenterology. Gender Differences in Inflammatory Bowel Disease. Digestion 2020, 101 (Suppl. 1), 98–104. [Google Scholar] [CrossRef]
- Wędrychowicz, A.; Tomasik, P.; Kowalska-Duplaga, K.; Pieczarkowski, S.; Fyderek, K. Plasma elafin, cathelicidin, and α-defensins are increased in paediatric inflammatory Crohn’s disease and reflect disease location. Arch. Med. Sci. 2021, 17, 1114–1117. [Google Scholar] [CrossRef]
- Liu, Y.; Tian, Y.; Wu, T.; Dai, Y.; Wang, W.; Teng, G. High Expression and Clinical Significance of Elafin in Colorectal Cancer. Gastroenterol. Res. Pract. 2019, 2019, 4946824. [Google Scholar] [CrossRef] [PubMed]
- Labidi-Galy, S.I.; Clauss, A.; Ng, V.; Duraisamy, S.; Elias, K.M.; Piao, H.Y.; Bilal, E.; Davidowitz, R.A.; Lu, Y.; Badalian-Very, G.; et al. Elafin drives poor outcome in high-grade serous ovarian cancers and basal-like breast tumors. Oncogene 2015, 34, 373–383. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Groups | Mean ± SD | Median | Range | Statistical Analysis |
|---|---|---|---|---|---|
| Elafin [ng/mL] | Crohn’s disease: active phase | 3.890 ± 1.655 | 4.448 | 0.139–5.870 | *†‡¥§ |
| Crohn’s disease: remission | 3.497 ± 0.737 | 3.479 | 2.484–5.088 | ||
| Ulcerative colitis: active phase | 4.795 ± 1.188 | 4.537 | 2.845–7.866 | ||
| Ulcerative colitis: remission | 4.054 ± 1.536 | 4.374 | 0.096–5.795 | ||
| Control group | 3.029 ± 1.366 | 3.306 | 0.164–4.790 |
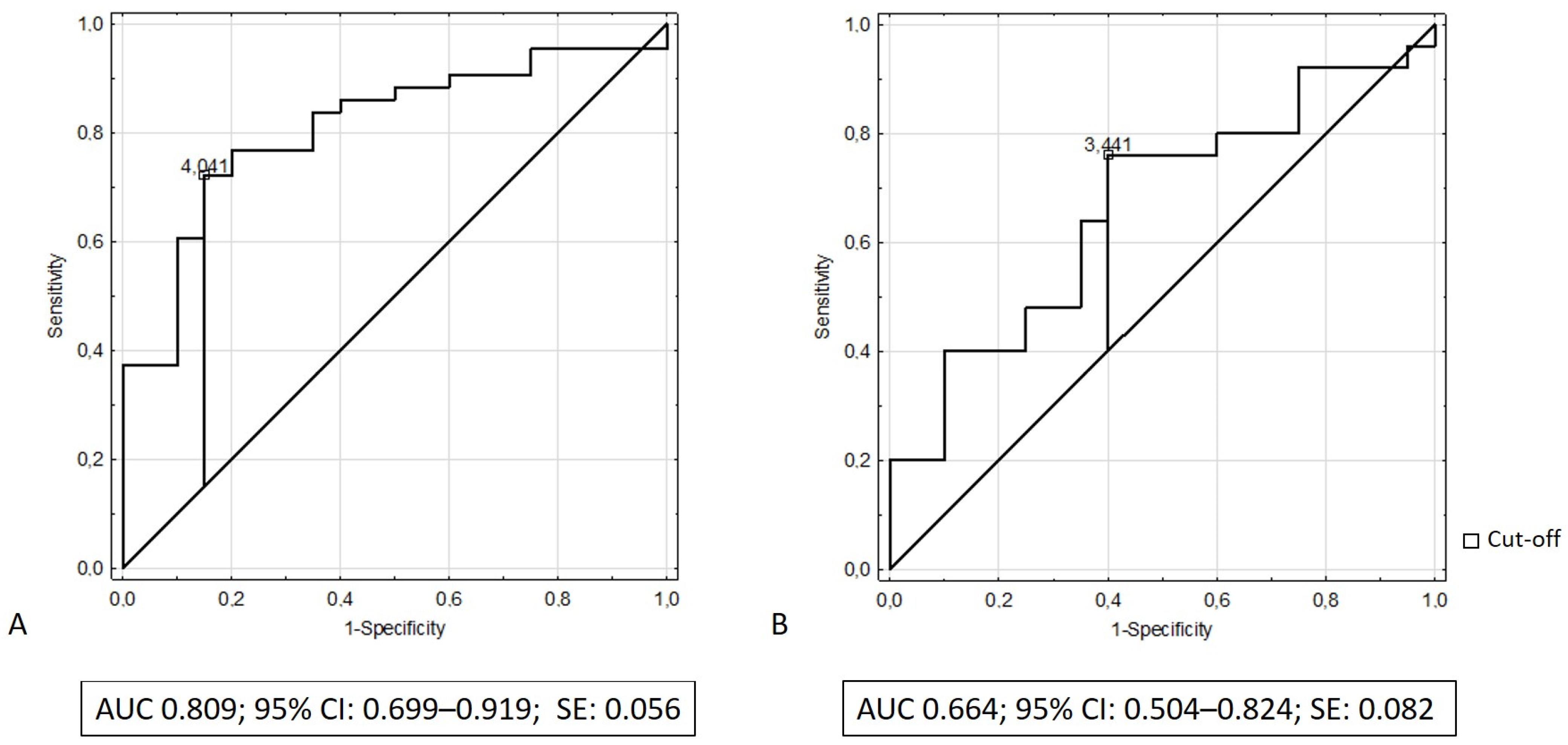
| Parameter | Cut-off | Sensitivity | Specificity | Accuracy | Positive Predictive Value | Negative Predictive Value |
|---|---|---|---|---|---|---|
| Elafin to distinguish ulcerative colitis from controls | 4.041 ng/mL | 0.721 | 0.850 | 0.762 | 0.912 | 0.586 |
| Elafin to distinguish Crohn’s disease from controls | 3.441 ng/mL | 0.760 | 0.600 | 0.689 | 0.704 | 0.667 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krawiec, P.; Pac-Kożuchowska, E. Clinical Significance of Serum Elafin in Children with Inflammatory Bowel Disease. Biomedicines 2022, 10, 3267. https://doi.org/10.3390/biomedicines10123267
Krawiec P, Pac-Kożuchowska E. Clinical Significance of Serum Elafin in Children with Inflammatory Bowel Disease. Biomedicines. 2022; 10(12):3267. https://doi.org/10.3390/biomedicines10123267
Chicago/Turabian StyleKrawiec, Paulina, and Elżbieta Pac-Kożuchowska. 2022. "Clinical Significance of Serum Elafin in Children with Inflammatory Bowel Disease" Biomedicines 10, no. 12: 3267. https://doi.org/10.3390/biomedicines10123267