
Effects of a Telerehabilitation Program in Women with Fibromyalgia at 6-Month Follow-Up: Secondary Analysis of a Randomized Clinical Trial
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
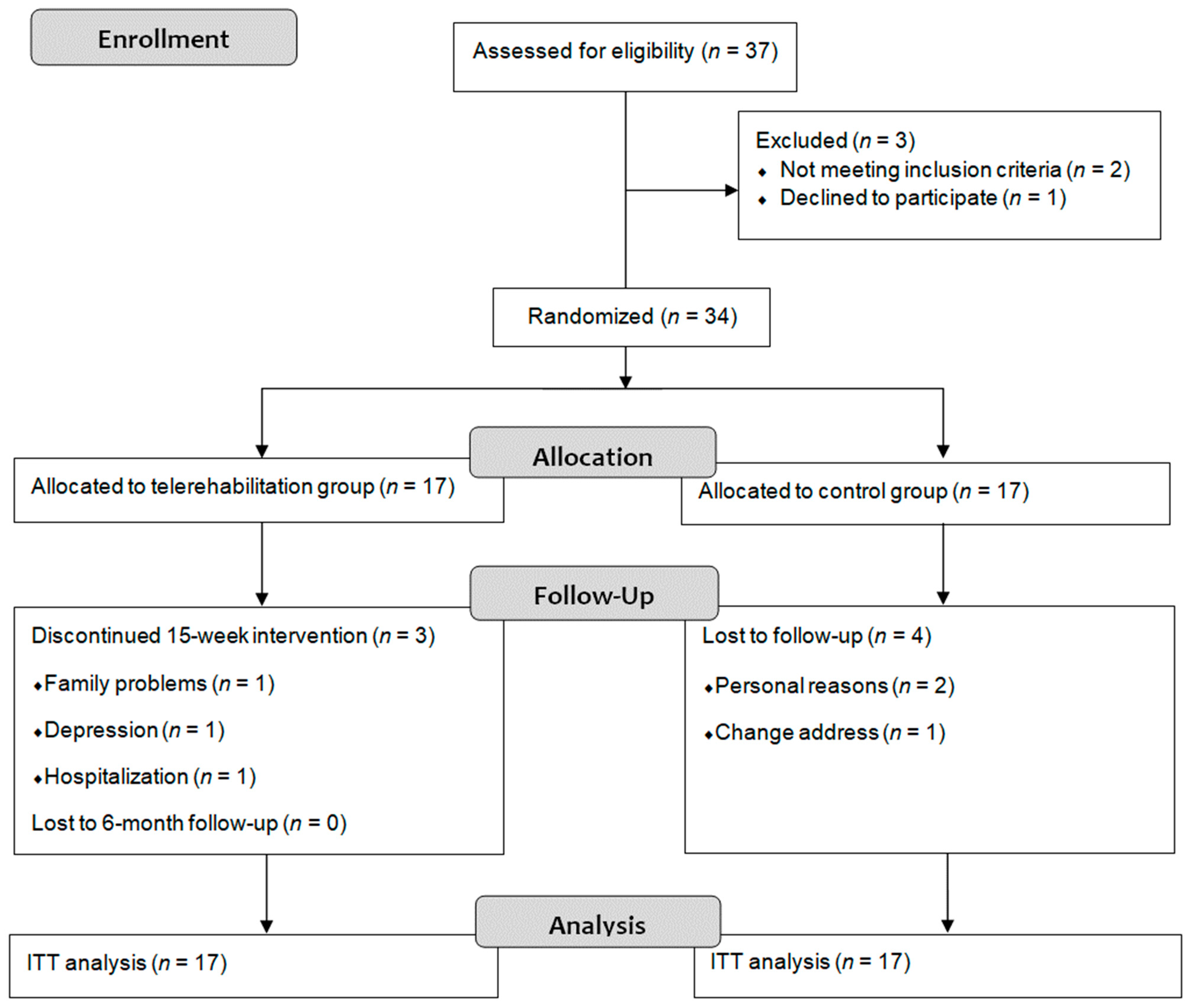
2.2. Participants
2.3. Sample Size
2.4. Randomization
2.5. Intervention
2.6. Outcome Measures
Secondary Outcomes
- Chair Stand Test (30-s CST): the number of times that participants were able to get up and sit on a chair without armrests within 30 s was measured.
- 6-Minute Walk Test (6MWT): the distance that the participants could walk in 6 min along a corridor of 20 m was measured.
- Arm Curl Test (ACT): the number of flexion–extension elbow movements that participants were able to perform holding a 2.3 kg weight with the dominant arm within 30 s was recorded.
- Timed Up and Go (TUG): the time that the participants took to stand up from a chair, walk 3 m, return and sit down again was recorded.
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, J.L. Fibromyalgia: Prevalence, epidemiologic profiles and economic costs. Med. Clin. 2017, 149, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Sluka, K.A.; Clauw, D.J. Neurobiology of fibromyalgia and chronic widespread pain. Neuroscience 2016, 338, 114–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Björnsdóttir, S.V.; Jónsson, S.H.; Valdimarsdóttir, U.A. Functional limitations and physical symptoms of individuals with chronic pain. Scand. J. Rheumatol. 2013, 42, 59–70. [Google Scholar] [CrossRef]
- de Miquel, C.A.; Campayo, J.G.; Flórez, M.T.; Arguelles, J.M.G.; Tarrio, E.B.; Montoya, M.G.; Martin, Á.P.; Salio, A.M.; Fuentes, J.V.; Alberch, E.A.; et al. Interdisciplinary consensus document for the treatment of fibromyalgia. Actas Esp. Psiquiatr. 2010, 38, 108–120. [Google Scholar] [PubMed]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Sosa-Reina, M.D.; Nunez-Nagy, S.; Gallego-Izquierdo, T.; Pecos-Martín, D.; Monserrat, J.; Álvarez-Mon, M. Effectiveness of Therapeutic Exercise in Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. BioMed Res. Int. 2017, 2017, 2356346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mun, C.J.; Campbell, C.M.; McGill, L.S.; Aaron, R.V. The Early Impact of COVID-19 on Chronic Pain: A Cross-Sectional Investigation of a Large Online Sample of Individuals with Chronic Pain in the United States, April to May, 2020. Pain Med. 2021, 22, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Mohabbat, A.B.; Mohabbat, N.M.L.; Wight, E.C. Fibromyalgia and Chronic Fatigue Syndrome in the Age of COVID-19. Mayo Clin. Proc. Innov. Qual. Outcomes. 2020, 4, 764–766. [Google Scholar] [CrossRef] [PubMed]
- Peretti, A.; Amenta, F.; Tayebati, S.K.; Nittari, G.; Mahdi, S.S. Telerehabilitation: Review of the State-of-the-Art and Areas of Application. JMIR Rehabil. Assist. Technol. 2017, 4, e7. [Google Scholar] [CrossRef] [PubMed]
- Hernando-Garijo, I.; Ceballos-Laita, L.; Mingo-Gómez, M.; Medrano-De-La-Fuente, R.; Estébanez-De-Miguel, E.; Martínez-Pérez, M.; Jiménez-Del-Barrio, S. Immediate Effects of a Telerehabilitation Program Based on Aerobic Exercise in Women with Fibromyalgia. Int. J. Environ. Res. Public Health. 2021, 18, 2075. [Google Scholar] [CrossRef] [PubMed]
- Cobos-Carbó, A.; Augustovski, F. Declaración CONSORT 2010: Actualización de la lista de comprobación para informar ensayos clínicos aleatorizados de grupos paralelos. Med. Clin. 2011, 137, 213–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tubach, F.; Ravaud, P.; Baron, G.; Falissard, B.; Logeart, I.; Bellamy, N.; Bombardier, C.; Felson, D.; Hochberg, M.; van der Heijde, D.; et al. Evaluation of clinically relevant changes in patient reported outcomes in knee and hip osteoarthritis: The minimal clinically important improvement. Ann. Rheum. Dis. 2005, 64, 29–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Alfonsin, M.M.; Chapon, R.; de Souza, C.A.B.; Genro, V.K.; Mattia, M.M.C.; Cunha-Filho, J.S. Correlations among algometry, the visual analogue scale, and the numeric rating scale to assess chronic pelvic pain in women. Eur. J. Obstet. Gynecol. Reprod. Biol. X 2019, 3, 100037. [Google Scholar] [CrossRef] [PubMed]
- Monterde, S.; Salvat, I.; Montull, S.; Fernández-Ballart, J. Validación de la versión española del Fibromyalgia Impact Questionnaire. Rev. Española. Reumatol. 2004, 31, 507–513. [Google Scholar]
- Langhammer, B.; Stanghelle, J.K. The Senior Fitness Test. J. Physiother. 2015, 61, 163. [Google Scholar] [CrossRef]
- Buckinx, F.; Croisier, J.-L.; Reginster, J.-Y.; Dardenne, N.; Beaudart, C.; Slomian, J.; Leonard, S.; Bruyere, O. Reliability of muscle strength measures obtained with a hand-held dynamometer in an elderly population. Clin. Physiol. Funct. Imaging 2017, 37, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Mentiplay, B.F.; Perraton, L.G.; Bower, K.J.; Adair, B.; Pua, Y.-H.; Williams, G.P.; McGaw, R.; Clark, R.A. Assessment of lower limb muscle strength and power using hand-held and fixed dynamometry: A reliability and validity study. PLoS ONE 2015, 10, e0140822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteve-Vives, J.; Batlle-Gualda, E.; Reig, A. Spanish version of the Health Assessment Questionnaire: Reliability, validity and transcultural equivalency. Grupo para la Adaptación del HAQ a la Población Española. J. Rheumatol. 1993, 20, 2116–2122. [Google Scholar] [PubMed]
- Da Costa, D.; Abrahamowicz, M.; Lowensteyn, I.; Bernatsky, S.; Dritsa, M.; Fitzcharles, M.-A.; Dobkin, P.L. A randomized clinical trial of an individualized home-based exercise programme for women with fibromyalgia. Rheumatology 2005, 44, 1422–1427. [Google Scholar] [CrossRef]
- Evcik, D.; Yigit, I.; Pusak, H.; Kavuncu, V. Effectiveness of aquatic therapy in the treatment of fibromyalgia syndrome: A randomized controlled open study. Rheumatol. Int. 2008, 28, 885–890. [Google Scholar] [CrossRef]
- Segura-Jiménez, V.; Álvarez-Gallardo, I.C.; Estévez-López, F.; Soriano-Maldonado, A.; Delgado-Fernández, M.; Ortega, F.B.; Aparicio, V.A.; Carbonell-Baeza, A.; Mota, J.; Silva, P.; et al. Differences in sedentary time and physical activity between female patients with fibromyalgia and healthy controls: The al-Ándalus project. Arthritis Rheumatol. 2015, 67, 3047–3057. [Google Scholar] [CrossRef]
- Mannerkorpi, K.; Nordeman, L.; Cider, A.; Jonsson, G. Does moderate-to-high intensity Nordic walking improve functional capacity and pain in fibromyalgia? A prospective randomized controlled trial. Arthritis Res. Ther. 2010, 12, R189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooten, W.M.; Qu, W.; Townsend, C.O.; Judd, J.W. Effects of strength vs. aerobic exercise on pain severity in adults with fibromyalgia: A randomized equivalence trial. Pain 2012, 153, 915–923. [Google Scholar] [CrossRef]
- Jones, C.J.; Rakovski, C.; Rutledge, D.; Gutierrez, A. A comparison of women with fibromyalgia syndrome to criterion fitness standards: A pilot study. J. Aging Phys. Act. 2015, 23, 103–111. [Google Scholar] [CrossRef]
- Ickmans, K.; Meeus, M.; De Kooning, M.; Lambrecht, L.; Pattyn, N.; Nijs, J. Associations between cognitive performance and pain in chronic fatigue syndrome: Comorbidity with fibromyalgia does matter. Pain Physician 2015, 18, E841–E852. [Google Scholar] [CrossRef]
- Larsson, A.; Palstam, A.; Löfgren, M.; Ernberg, M.; Bjersing, J.; Bileviciute-Ljungar, I.; Gerdle, B.; Kosek, E.; Mannerkorpi, K. Pain and fear avoidance partially mediate change in muscle strength during resistance exercise in women with fibromyalgia. J. Rehabil. Med. 2017, 49, 744–750. [Google Scholar] [CrossRef] [Green Version]
- Álvarez-Gallardo, I.C.; Soriano-Maldonado, A.; Segura-Jiménez, V.; Estévez-López, F.; Moirón, D.C.; A Aparicio, V.; Herrador-Colmenero, M.; Castro-Piñero, J.; Ortega, F.B.; Delgado-Fernández, M.; et al. High Levels of Physical Fitness Are Associated with Better Health-Related Quality of Life in Women with Fibromyalgia: The al-Ándalus Project. Phys. Ther. 2019, 99, 1481–1494. [Google Scholar] [CrossRef]


{kind=link}
| TR Group Mean ± SD | Control Group Mean ± SD | Significance | |
|---|---|---|---|
| Age (years) | 51.81 ± 9.05 | 55.06 ± 8.51 | 0.304 a |
| Height (cm) | 158 ± 6.29 | 161.81 ± 5.13 | 0.191 b |
| Weight (kg) | 68.19 ± 16.88 | 68.13 ± 15.10 | 0.836 b |
| BMI (kg/cm2) | 27.25 ± 7.30 | 25.93 ± 5.27 | 0.598 b |
| Medication n (%) | 17 (100) | 17 (100) | 0.224 c |
| Anxiolytics n (%) | 9 (53) | 7 (41) | |
| Antidepressants n (%) | 9 (53) | 9 (53) | |
| Anti-inflammatory n (%) | 14 (82) | 8 (47) | |
| Analgesics n (%) | 11 (65) | 12 (71) | |
| Muscle relaxants n (%) | 4 (24) | 2 (12) |
| Baseline Mean ± SD | 6-Month Follow-Up Mean ± SD | Within-Group Changes (p Value) | Effect Size (Cohen d) | Between-Group Changes (p Value) | Between-Group Effect Size (Cohen d) | |
|---|---|---|---|---|---|---|
| VAS (0–10) | ||||||
| TR group | 7.08 ± 1.45 | 6.15 ± 1.25 | 0.93 (0.08;1.79) 0.034 | 0.7 | F = 0.02 0.873 | 0.2 |
| Control group | 7.29 ± 1.07 | 6.52 ± 2.06 | 0.77 (−0.48; 2.03) 0.205 | 0.4 | ||
| FIQ-R | ||||||
| TR group | 59.44 ± 9.04 | 53.26 ± 9.40 | 6.18 (1.70; 10.44) 0.010 | 0.7 | F = 0.25 0.612 | 0.2 |
| Control group | 55.36 ± 16.46 | 50.34 ± 19.45 | 5.01 (−4.46; 15.08) 0.261 | 0.2 | ||
| 30s-CST | ||||||
| TR group | 7.46 ± 2.66 | 8.92 ± 2.46 | −1.46 (−2.40; −0.51) 0.006 | 0.6 | F = 0.46 0.494 | 0.3 |
| Control group | 7.14 ± 4.20 | 8.00 ± 4.31 | −0.85 (−2.03; 0.31) 0.139 | 0.2 | ||
| 6MWT | ||||||
| TR group | 403.57 ± 107.13 | 458.93 ± 67.40 | −55.36 (−22.13; −85.50) <0.001 | 0.6 | F = 2.29 0.115 | 0.6 |
| Control group | 407.01 ± 137.09 | 374.94 ± 173.33 | 32.07 (−14.78; 61.22) 0.316 | 0.2 | ||
| ACT | ||||||
| TR group | 9.60 ± 4.31 | 11.61 ± 3.12 | −2.23 (−4.32; −0.13) 0.039 | 0.5 | F = 0.95 0.338 | 0.4 |
| Control group | 10.06 ± 5.56 | 10.00 ± 5.14 | −0.05 (−1.77; 0.77) 0.413 | 0.0 | ||
| TUG | ||||||
| TR group | 9.19 ± 2.98 | 7.72 ± 1.17 | 1.47 (0.05; 2.88) 0.042 | 0.6 | F =2.52 0.109 | 0.7 |
| Control group | 10.69 ± 4.73 | 10.26 ± 5.15 | 0.43 (−1.63; 2.49) 0.657 | 0.1 | ||
| Right elbow strength | ||||||
| TR group | 7.36 ± 4.14 | 9.29 ± 4.21 | −1.92 (−3.69; −0.16) 0.035 | 0.5 | F = 0.75 0.393 | 0.3 |
| Control group | 7.85 ± 3.31 | 7.95 ± 3.75 | −0.10 (−1.28; 1.08) 0.857 | 0.0 | ||
| Left elbow strength | ||||||
| TR group | 7.56 ± 3.34 | 9.49 ± 3.55 | −1.92 (−3.70; −0.14) 0.036 | 0.6 | F = 1.06 0.312 | 0.4 |
| Control group | 8.40 ± 3.58 | 8.06 ± 3.65 | 0.34 (−1.54; 2.23) 0.697 | 0.1 | ||
| Right knee strength | ||||||
| TR group | 7.86 ± 3.39 | 9.96 ± 2.69 | −2.10 (−3.28; −0.91) 0.002 | 0.7 | F = 0.04 0.845 | 0.1 |
| Control group | 9.13 ± 4.22 | 9.66 ± 4.69 | −0.53 (−2.47; 1.40) 0.557 | 0.1 | ||
| Left knee strength | ||||||
| TR group | 7.14 ± 2.68 | 9.78 ± 3.02 | −2.64 (−3.28; −0.91) 0.002 | 0.9 | F = 0.33 0.580 | 0.2 |
| Control group | 9.30 ± 4.53 | 8.95 ± 4.26 | 0.34 (−1.06; 1.74) 0.604 | 0.1 | ||
| HAQ | ||||||
| TR group | 1.64 ± 0.63 | 1.31 ± 0.61 | 0.32 (0.07; 0.57) 0.015 | 0.5 | 0.871 | 0.0 |
| Control group | 1.48 ± 0.56 | 1.30 ± 0.72 | 0.18 (−0.05; 0.49) 0.108 | 0.2 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernando-Garijo, I.; Medrano-de-la-Fuente, R.; Jiménez-del-Barrio, S.; Mingo-Gómez, M.T.; Hernández-Lázaro, H.; Lahuerta-Martin, S.; Ceballos-Laita, L. Effects of a Telerehabilitation Program in Women with Fibromyalgia at 6-Month Follow-Up: Secondary Analysis of a Randomized Clinical Trial. Biomedicines 2022, 10, 3024. https://doi.org/10.3390/biomedicines10123024
Hernando-Garijo I, Medrano-de-la-Fuente R, Jiménez-del-Barrio S, Mingo-Gómez MT, Hernández-Lázaro H, Lahuerta-Martin S, Ceballos-Laita L. Effects of a Telerehabilitation Program in Women with Fibromyalgia at 6-Month Follow-Up: Secondary Analysis of a Randomized Clinical Trial. Biomedicines. 2022; 10(12):3024. https://doi.org/10.3390/biomedicines10123024
Chicago/Turabian StyleHernando-Garijo, Ignacio, Ricardo Medrano-de-la-Fuente, Sandra Jiménez-del-Barrio, María Teresa Mingo-Gómez, Héctor Hernández-Lázaro, Silvia Lahuerta-Martin, and Luis Ceballos-Laita. 2022. "Effects of a Telerehabilitation Program in Women with Fibromyalgia at 6-Month Follow-Up: Secondary Analysis of a Randomized Clinical Trial" Biomedicines 10, no. 12: 3024. https://doi.org/10.3390/biomedicines10123024