
Three-Dimensional Constructive Interference in Steady State (3D CISS) Imaging and Clinical Applications in Brain Pathology

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
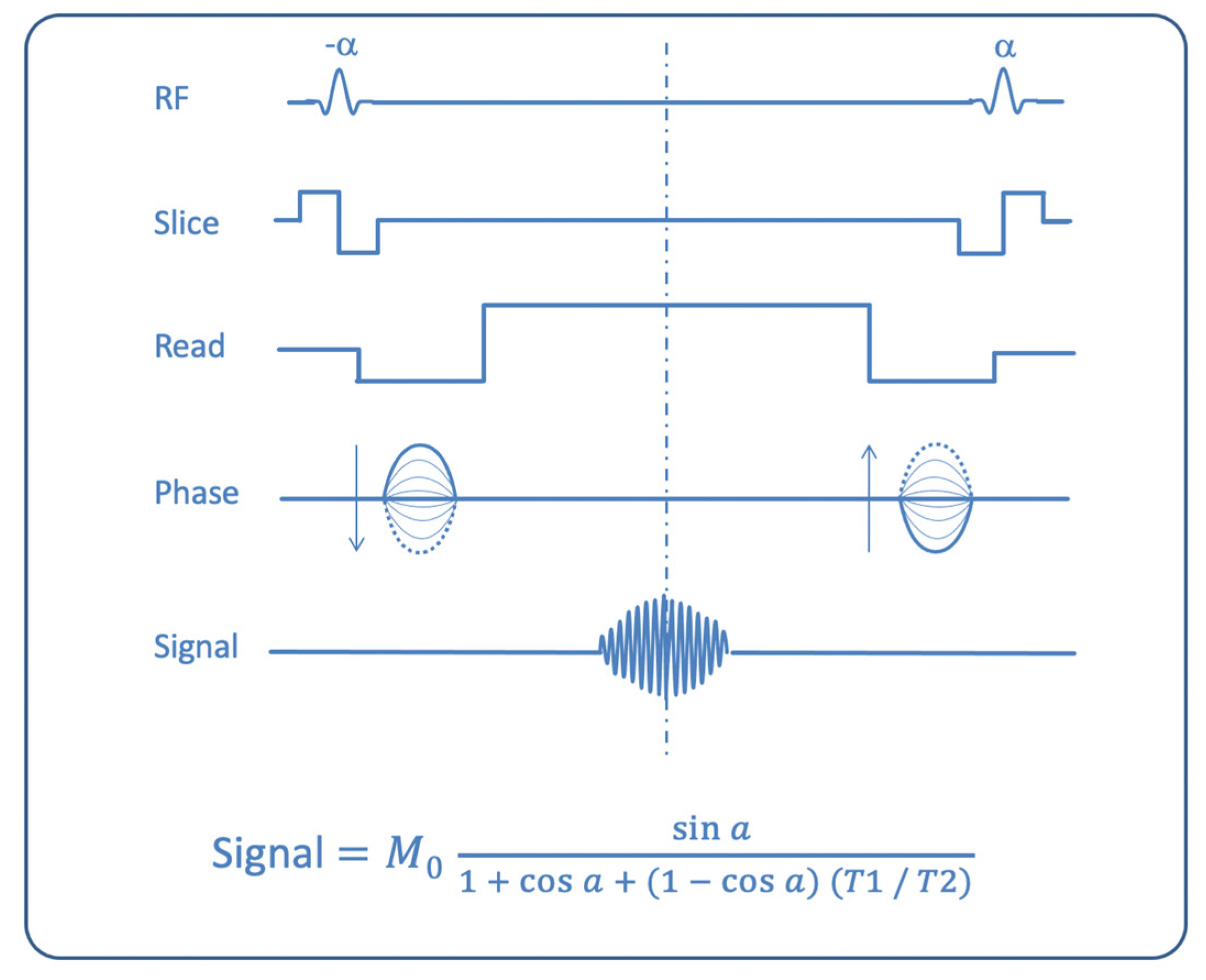
1.1. CISS Properties
1.2. CISS Advantages and Limitations
2. Literature Review
3. Clinical Applications
3.1. Evaluation of Cranial Nerves
3.1.1. Olfactory Nerve (I)
3.1.2. Optic Nerve (II) and Orbital Masses
3.1.3. Ocular Motor Nerves (III–IV–VI)
3.1.4. Trigeminal Nerve (V)
3.1.5. Facial and Vestibulocochlear Nerves (VII–VIII Complex)
3.1.6. The Lower Cranial Nerves: Glossopharyngeal, Vagus, Accessory and Hypoglossal Nerves (IX–X–XI–XII)
- -
- the recess for the cochlear aqueduct
- -
- the recess for the glossopharyngeal nerve
- -
- the recess for the vagus nerve and the accessory nerve [42].
3.2. Virchow–Robin Spaces
3.3. CSF Fistulae
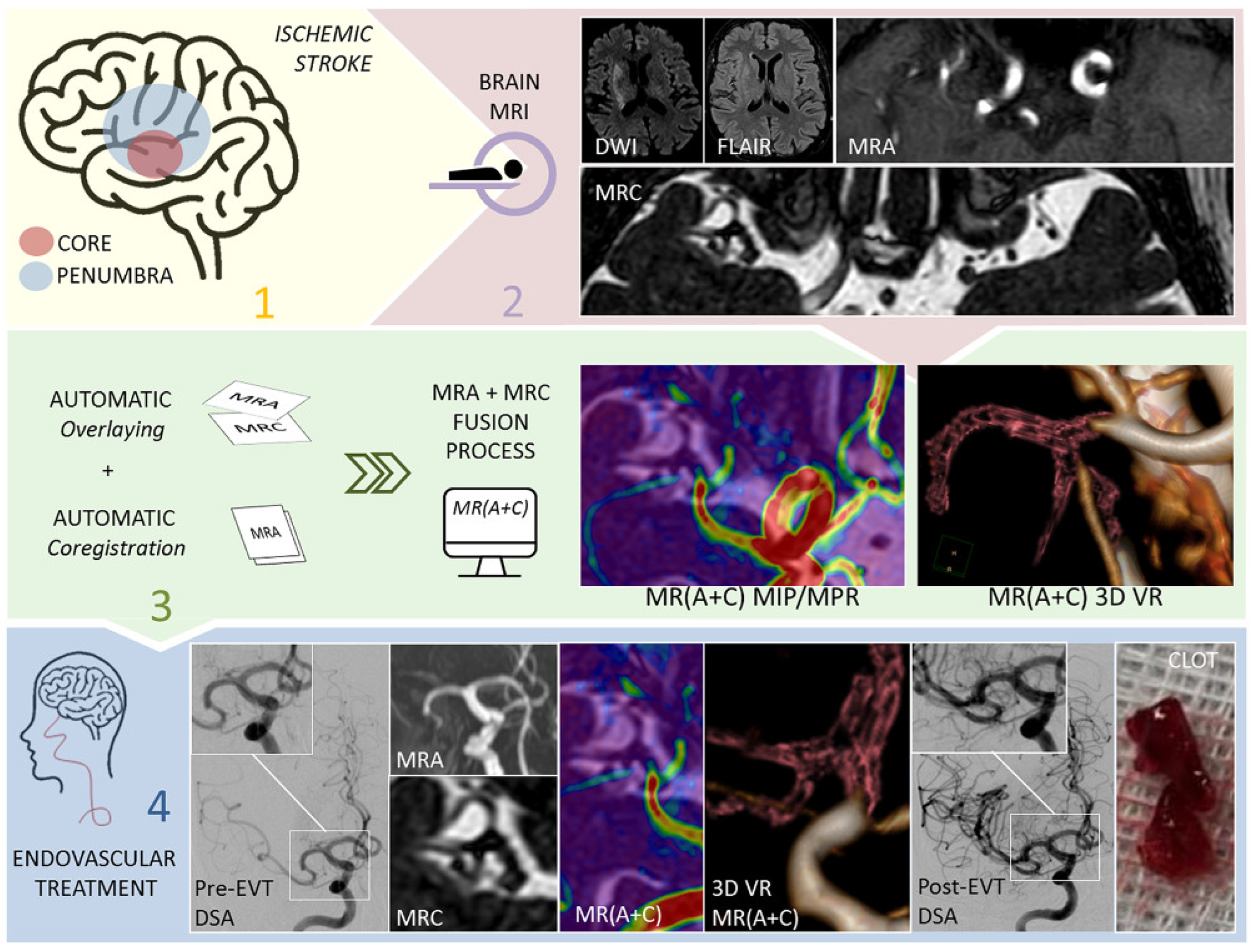
3.4. Cerebrovascular Pathology
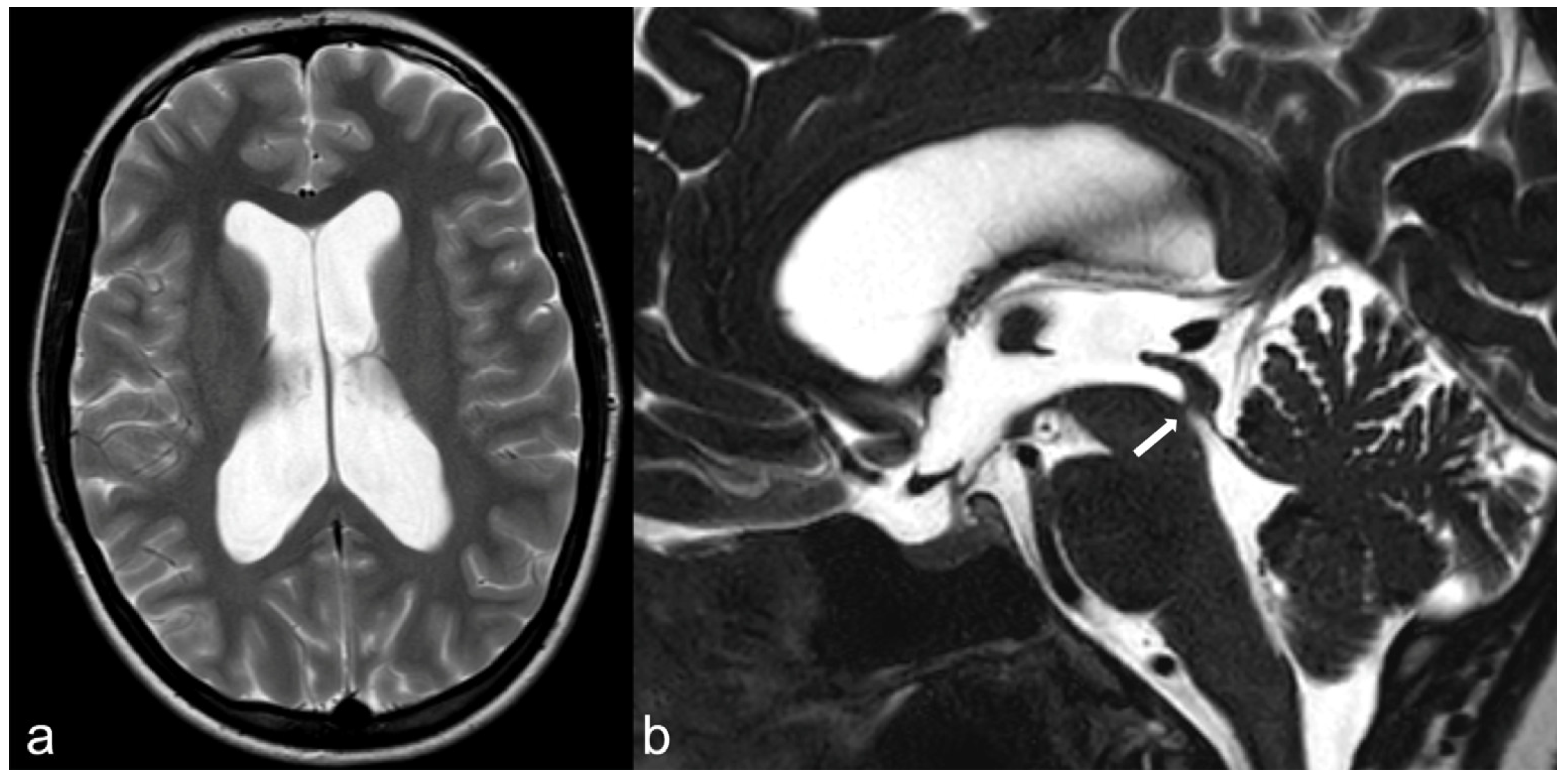
3.5. Hydrocephalus, Ventricular System and Subarachnoid Cisterns
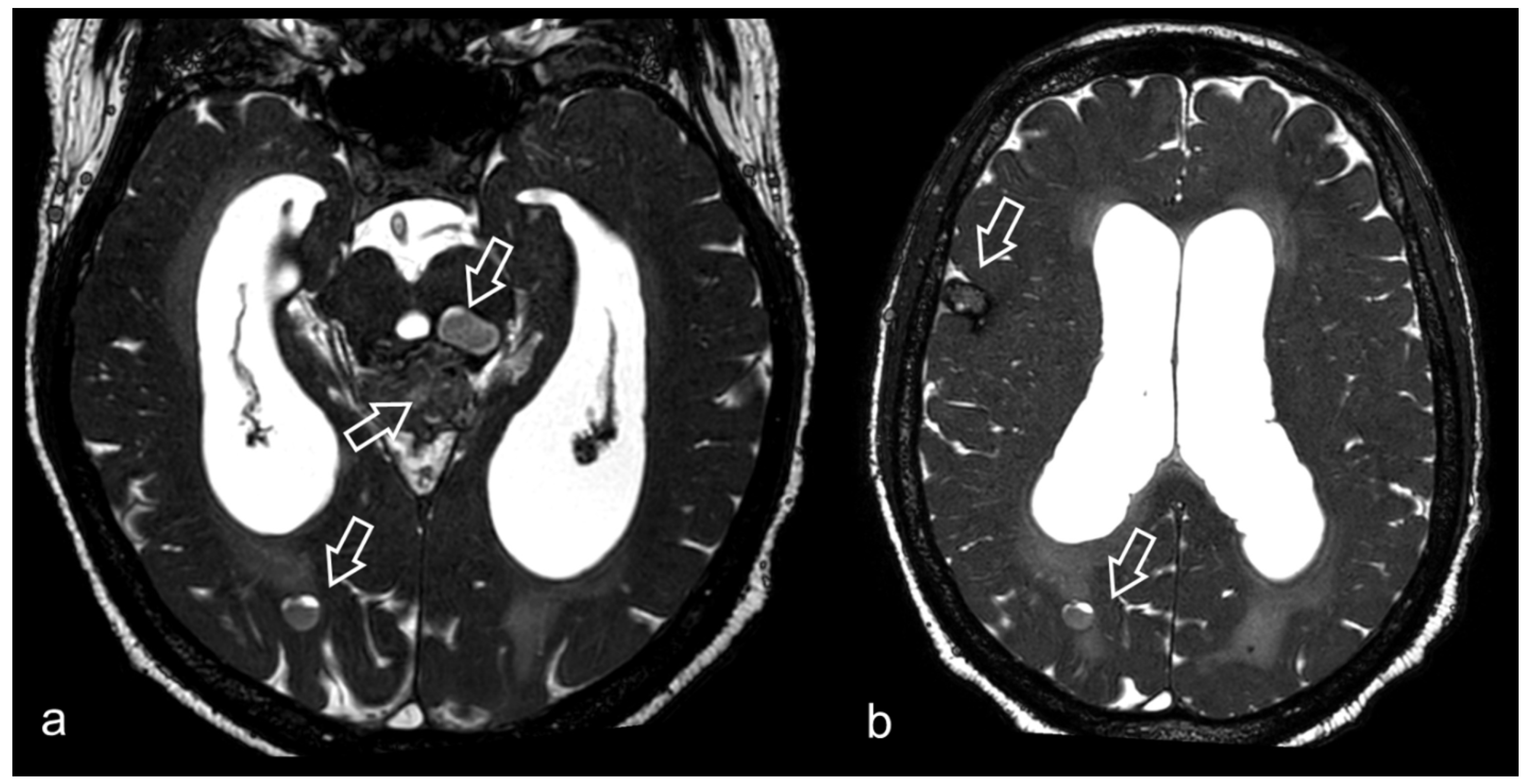
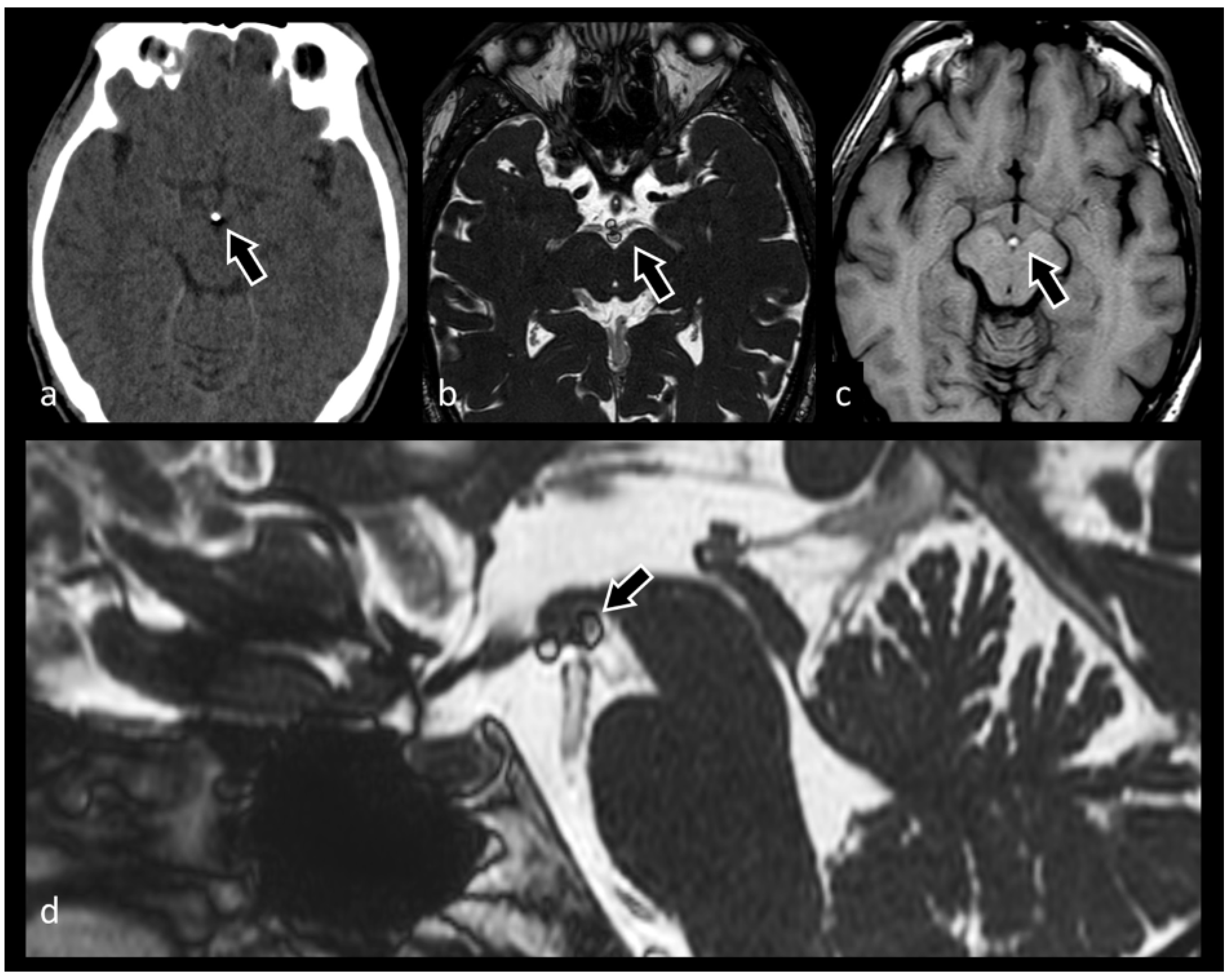
3.6. Neurocysticercosis
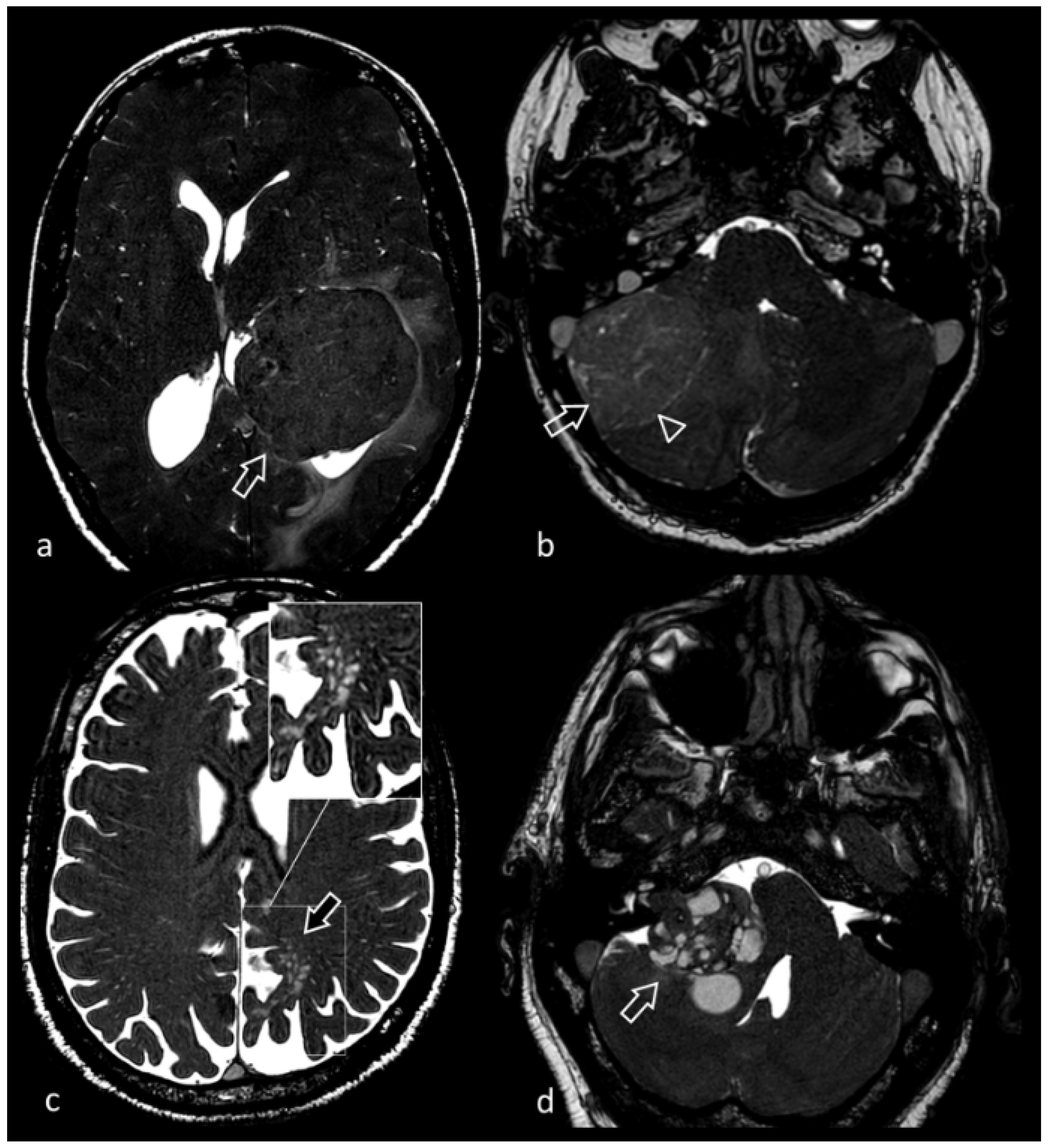
3.7. Evaluation of Brain Tumors
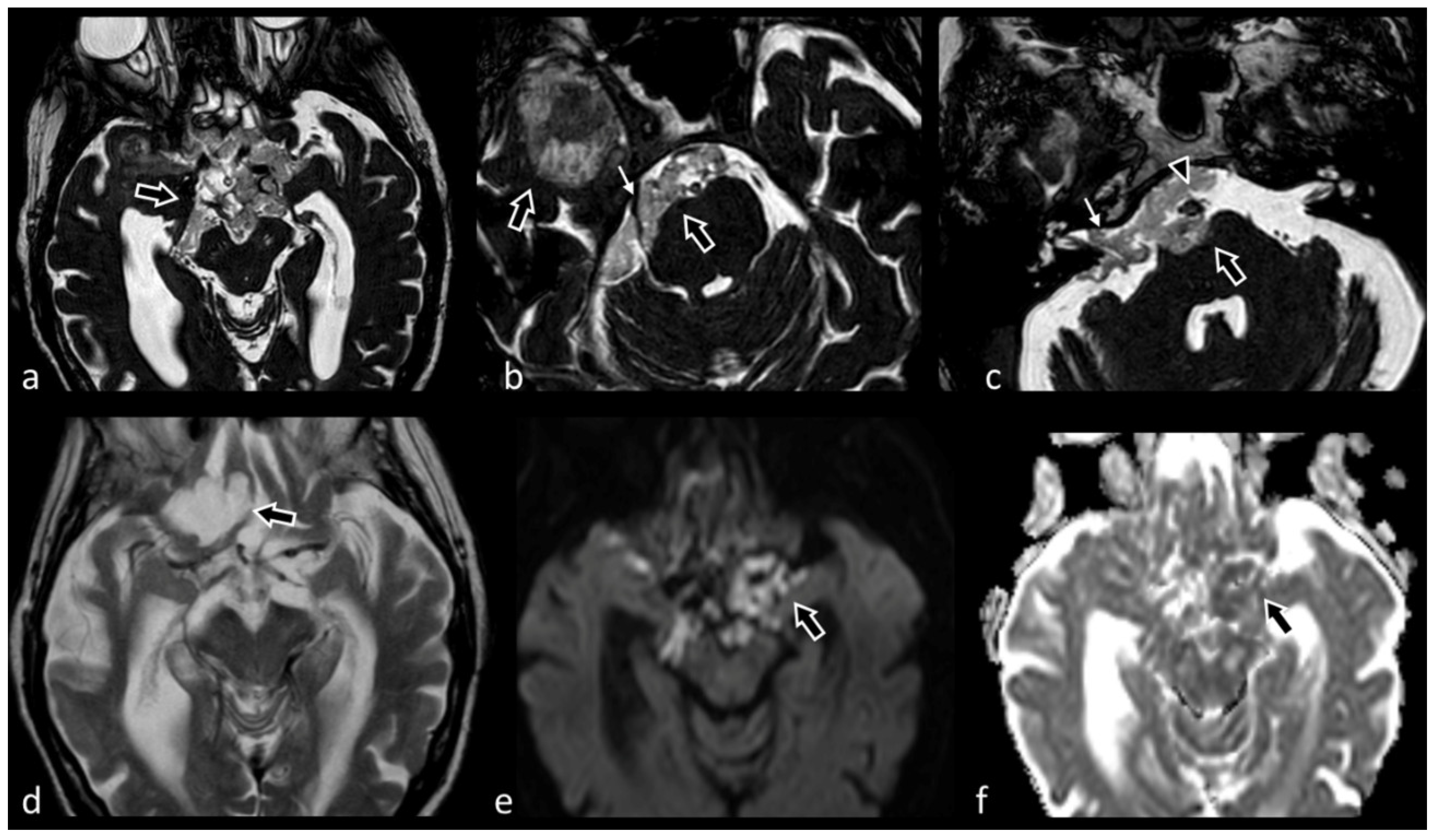
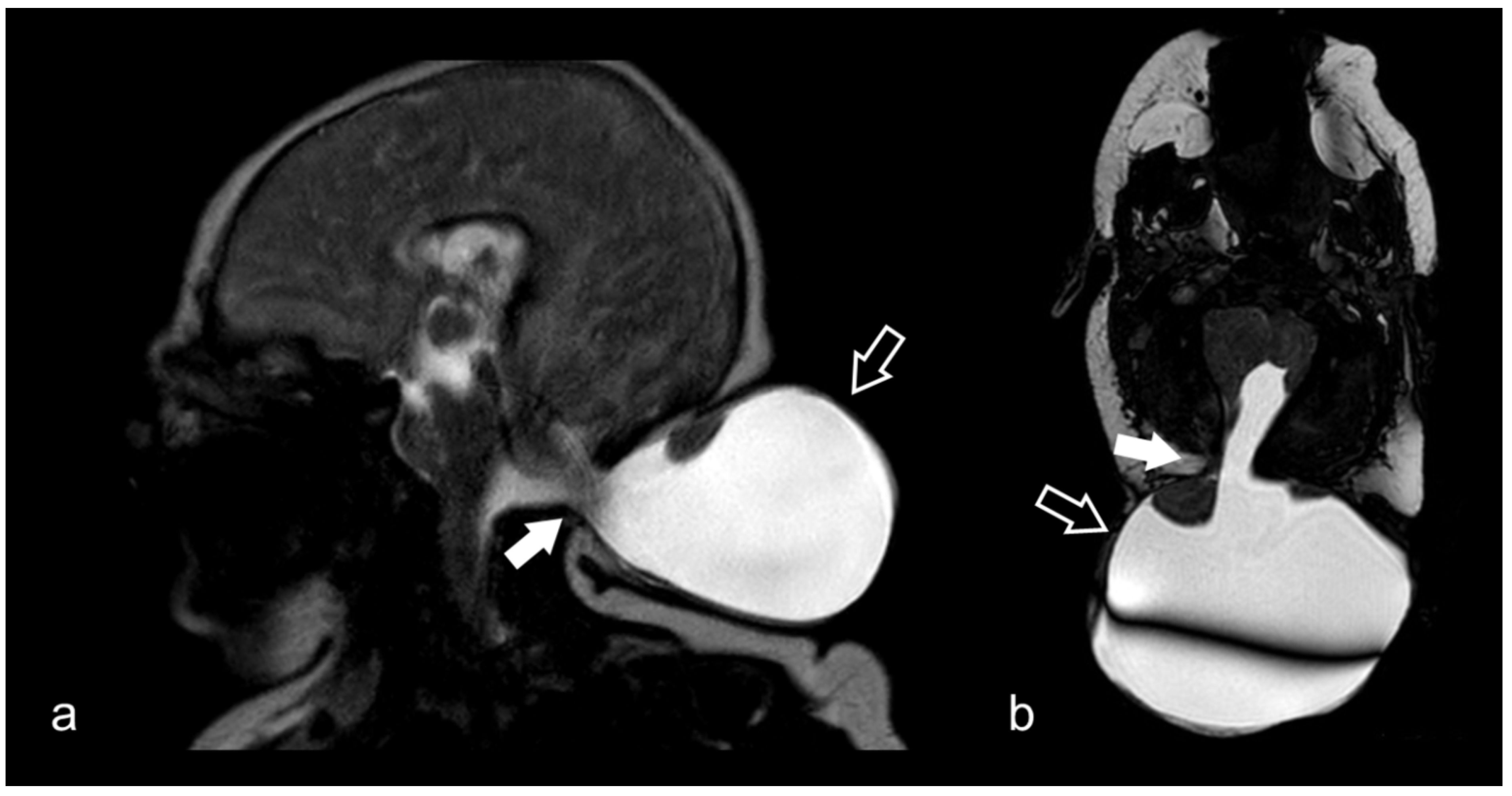
3.8. Cerebellopontine Angle Lesions
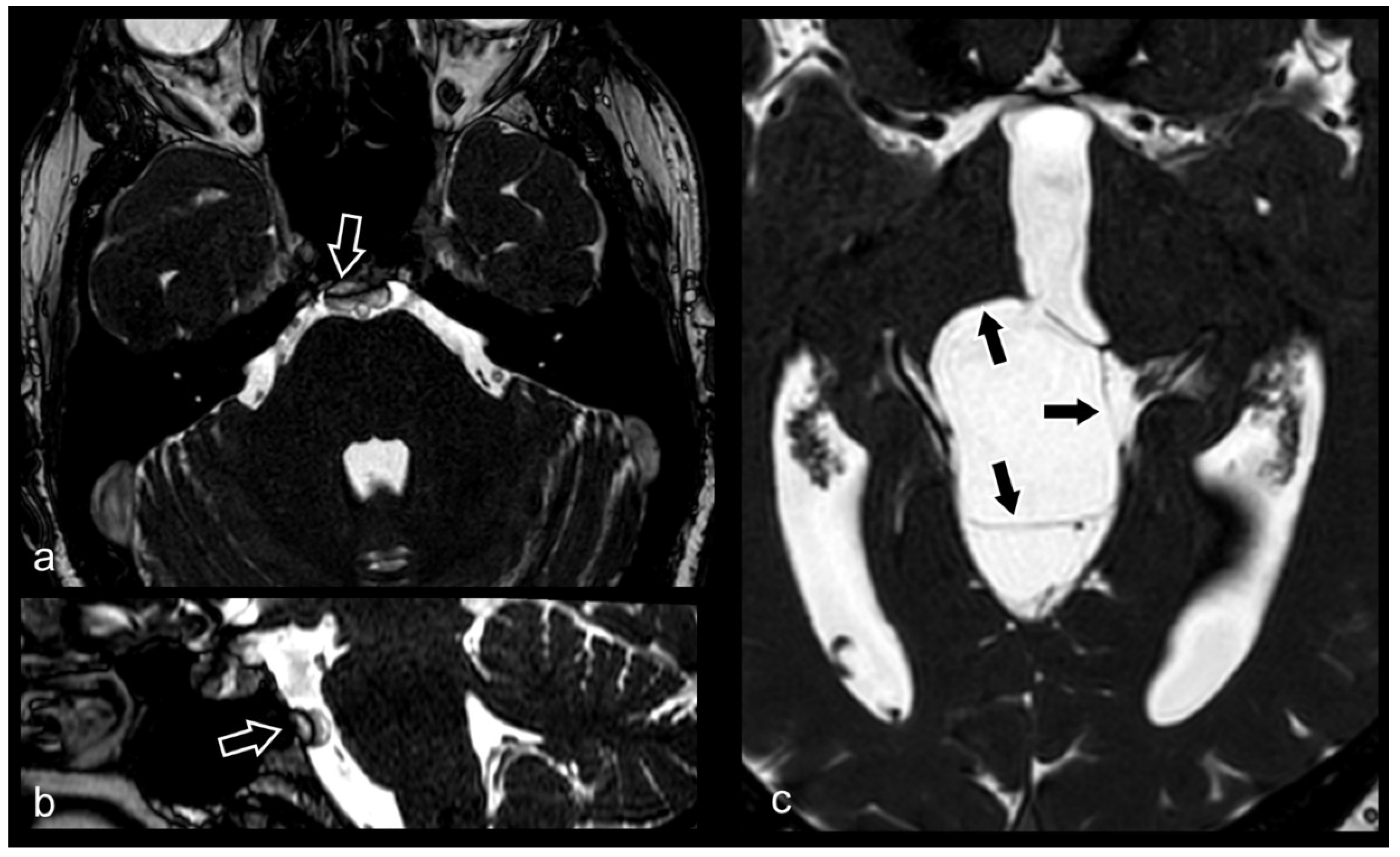
3.9. Hypothalamic–Pituitary Disorders
3.10. Cranio-Cervical Malformations (Chiari I)
3.11. Evaluation of Internal Auditory Canal and Inner Ear Structures
3.12. Neonatal and Fetal MRI
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| b-SSFP | balanced steady-state free precession |
| CISS | constructive interference in steady state |
| CN | cranial nerve |
| CNR | contrast-to-noise ratio |
| CPA | cerebellopontine angle |
| CSF | cerebrospinal fluid |
| ETV | endoscopic third ventriculostomy |
| IAC | internal auditory canal |
| MRA | magnetic resonance angiography |
| MRC | magnetic resonance cisternography |
| MRI | magnetic resonance imaging; |
| SNR | signal-to-noise ratio |
| TOF | time-of-flight |
References
- Carr, H.Y. Stady-state Free Precession in Nuclear Magnetic Resonance. Phys. Rev. 1958, 112, 1693–1701. [Google Scholar] [CrossRef]
- Bieri, O.; Scheffler, K. Fundamentals of balanced steady state free precession MRI. J. Magn. Reson. Imaging JMRI 2013, 38, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Gaeta, M.; Cavallaro, M.; Vinci, S.L.; Mormina, E.; Blandino, A.; Marino, M.A.; Granata, F.; Tessitore, A.; Galletta, K.; D’Angelo, T.; et al. Magnetism of materials: Theory and practice in magnetic resonance imaging. Insights Imaging 2021, 12, 179. [Google Scholar] [CrossRef] [PubMed]
- Chavhan, G.B.; Babyn, P.S.; Jankharia, B.G.; Cheng, H.L.; Shroff, M.M. Steady-state MR imaging sequences: Physics, classification, and clinical applications. Radiographics 2008, 28, 1147–1160. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.Y.; Huang, I.J.; Chen, C.Y.; Scheffler, K.; Chung, H.W.; Cheng, H.C. Are TrueFISP images T2/T1-weighted? Magn. Reson. Med. 2002, 48, 684–688. [Google Scholar] [CrossRef] [PubMed]
- Besta, R.; Shankar, Y.U.; Kumar, A.; Rajasekhar, E.; Prakash, S.B. MRI 3D CISS—A Novel Imaging Modality in Diagnosing Trigeminal Neuralgia—A Review. J. Clin. Diagn. Res. JCDR 2016, 10, ZE01–ZE03. [Google Scholar] [CrossRef]
- Hingwala, D.; Chatterjee, S.; Kesavadas, C.; Thomas, B.; Kapilamoorthy, T.R. Applications of 3D CISS sequence for problem solving in neuroimaging. Indian J. Radiol. Imaging 2011, 21, 90–97. [Google Scholar] [CrossRef]
- Gonçalves, F.G. Constructive Interference in Steady State Imaging in the Central Nervous System. Eur. Neurol. Rev. 2011, 6, 138–142. [Google Scholar] [CrossRef] [Green Version]
- Yang, D.; Shen, J.; Xia, X.; Lin, Y.; Yang, T.; Lin, H.; Jin, Y.; Zhou, K.; Li, Y. Preoperative evaluation of neurovascular relationship in trigeminal neuralgia by three-dimensional fast low angle shot (3D-FLASH) and three-dimensional constructive interference in steady-state (3D-CISS) MRI sequence. Br. J. Radiol. 2018, 91, 20170557. [Google Scholar] [CrossRef]
- Li, Z.; Chen, Y.A.; Chow, D.; Talbott, J.; Glastonbury, C.; Shah, V. Practical applications of CISS MRI in spine imaging. Eur. J. Radiol. Open 2019, 6, 231–242. [Google Scholar] [CrossRef]
- Hashiguchi, K.; Morioka, T.; Fukui, K.; Miyagi, Y.; Mihara, F.; Yoshiura, T.; Nagata, S.; Sasaki, T. Usefulness of constructive interference in steady-state magnetic resonance imaging in the presurgical examination for lumbosacral lipoma. J. Neurosurg. 2005, 103, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Roser, F.; Ebner, F.H.; Danz, S.; Riether, F.; Ritz, R.; Dietz, K.; Naegele, T.; Tatagiba, M.S. Three-dimensional constructive interference in steady-state magnetic resonance imaging in syringomyelia: Advantages over conventional imaging. J. Neurosurg. 2008, 8, 429–435. [Google Scholar] [CrossRef] [PubMed]
- ElKhamary, S.M.; Riad, W. Three dimensional MRI study: Safety of short versus long needle peribulbar anesthesia. Saudi J. Ophthalmol. 2014, 28, 220–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Do Amaral, L.L.; Ferreira, R.M.; da Rocha, A.J.; Ferreira, N.P. Neurocysticercosis: Evaluation with advanced magnetic resonance techniques and atypical forms. Top. Magn. Reson. Imaging TMRI 2005, 16, 127–144. [Google Scholar] [CrossRef]
- Tsuchiya, K.; Aoki, C.; Hachiya, J. Evaluation of MR cisternography of the cerebellopontine angle using a balanced fast-field-echo sequence: Preliminary findings. Eur. Radiol. 2004, 14, 239–242. [Google Scholar] [CrossRef]
- Liang, C.; Du, Y.; Xu, J.; Wu, L.; Liu, C.; Wang, X.; Wang, H.; Yu, F. MR imaging of the cisternal segment of the posterior group of cranial nerves: Neurovascular relationships and abnormal changes. Eur. J. Radiol. 2010, 75, 57–63. [Google Scholar] [CrossRef]
- Sheth, S.; Branstetter, B.F.t.; Escott, E.J. Appearance of normal cranial nerves on steady-state free precession MR images. Radiographics 2009, 29, 1045–1055. [Google Scholar] [CrossRef]
- Burmeister, H.P.; Baltzer, P.A.; Möslein, C.; Bitter, T.; Gudziol, H.; Dietzel, M.; Guntinas-Lichius, O.; Kaiser, W.A. Visual grading characteristics (VGC) analysis of diagnostic image quality for high resolution 3 Tesla MRI volumetry of the olfactory bulb. Acad. Radiol. 2011, 18, 634–639. [Google Scholar] [CrossRef]
- Negoias, S.; Croy, I.; Gerber, J.; Puschmann, S.; Petrowski, K.; Joraschky, P.; Hummel, T. Reduced olfactory bulb volume and olfactory sensitivity in patients with acute major depression. Neuroscience 2010, 169, 415–421. [Google Scholar] [CrossRef]
- Li, J.; Gu, C.; Su, J.; Zhu, L.; Zhou, Y.; Huang, H.; Liu, C. Changes in Olfactory Bulb Volume in Parkinson’s Disease: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0149286. [Google Scholar] [CrossRef]
- Duprez, T.; Rombaux, P. Imaging the olfactory tract (cranial nerve #1). Eur. J. Radiol. 2010, 74, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Nagarajan, K.; Venkataraman, A. Thin-section 3D Steady-State MRI in Optic Nerve Coloboma. Neuro-Ophthalmology 2021, 45, 281–282. [Google Scholar] [CrossRef] [PubMed]
- Seitz, J.; Held, P.; Strotzer, M.; Müller, M.; Völk, M.; Lenhart, M.; Djavidani, B.; Feuerbach, S. Magnetic resonance imaging in patients diagnosed with papilledema: A comparison of 6 different high-resolution T1- and T2(*)-weighted 3-dimensional and 2-dimensional sequences. J. Neuroimaging 2002, 12, 164–171. [Google Scholar] [CrossRef]
- Rosahl, S.K.; Kassem, O.; Piepgras, U.; Hellwig, D.; Samii, M. High-resolution constructive interference in steady-state imaging in tethered cord syndrome: Technical note. Surg. Neurol. 2005, 63, 372–374. [Google Scholar] [CrossRef] [PubMed]
- Alafaci, C.; Granata, F.; Cutugno, M.; Marino, D.; Conti, A.; Tomasello, F. Glossopharyngeal neuralgia caused by a complex neurovascular conflict: Case report and review of the literature. Surg. Neurol. Int. 2015, 6, 19. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Liang, C.; Liu, C.; Liu, S.; Deng, K.; He, J. Oculomotor paralysis: 3D-CISS MR imaging with MPR in the evaluation of neuralgic manifestation and the adjacent structures. Eur. J. Radiol. 2010, 73, 221–223. [Google Scholar] [CrossRef]
- Blitz, A.M.; Northcutt, B.; Shin, J.; Aygun, N.; Herzka, D.A.; Theodros, D.; Goodwin, C.R.; Lim, M.; Seeburg, D.P. Contrast-Enhanced CISS Imaging for Evaluation of Neurovascular Compression in Trigeminal Neuralgia: Improved Correlation with Symptoms and Prediction of Surgical Outcomes. AJNR. Am. J. Neuroradiol. 2018, 39, 1724–1732. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.P.; Acar, F.; Hamilton, B.E.; Burchiel, K.J. Radiographic evaluation of trigeminal neurovascular compression in patients with and without trigeminal neuralgia. J. Neurosurg. 2009, 110, 627–632. [Google Scholar] [CrossRef]
- Held, P.; Fründ, R.; Seitz, J.; Nitz, W.; Haffke, T.; Hees, H. Comparison of 2-D turbo spin echo and 3-D gradient echo sequences for the detection of the trigeminal nerve and branches anatomy. Eur. J. Radiol. 2001, 37, 18–25. [Google Scholar] [CrossRef]
- Lak, A.M.; Khan, Y.S. Cerebellopontine Angle Cancer; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Cho, Y.S.; Choi, J.E.; Lim, J.H.; Cho, Y.S. Management of facial nerve schwannoma: When is the timing for surgery. Eur. Arch. Oto-Rhino-Laryngol. 2022, 279, 1243–1249. [Google Scholar] [CrossRef]
- Jia, J.M.; Guo, H.; Huo, W.J.; Hu, S.W.; He, F.; Sun, X.D.; Lin, G.J. Preoperative Evaluation of Patients with Hemifacial Spasm by Three-dimensional Time-of-Flight (3D-TOF) and Three-dimensional Constructive Interference in Steady State (3D-CISS) Sequence. Clin. Neuroradiol. 2016, 26, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Granata, F.; Vinci, S.L.; Longo, M.; Bernava, G.; Caffo, M.; Cutugno, M.; Morabito, R.; Salamone, I.; Tomasello, F.; Alafaci, C. Advanced virtual magnetic resonance imaging (MRI) techniques in neurovascular conflict: Bidimensional image fusion and virtual cisternography. Radiol. Med. 2013, 118, 1045–1054. [Google Scholar] [CrossRef] [PubMed]
- Mittal, P.; Mittal, G. Painful tic convulsif syndrome due to vertebrobasilar dolichoectasia. J. Neurosci. Rural Pract. 2011, 2, 71–73. [Google Scholar] [CrossRef] [PubMed]
- Held, P.; Fellner, C.; Fellner, F.; Seitz, J.; Graf, S.; Strutz, J. Correlation of 3D MRI and clinical findings in the patients with sensorineural hearing loss and/or vertigo. Clin. Imaging 1998, 22, 309–322. [Google Scholar] [CrossRef]
- McDermott, A.L.; Dutt, S.N.; Irving, R.M.; Pahor, A.L.; Chavda, S.V. Anterior inferior cerebellar artery syndrome: Fact or fiction. Clin. Otolaryngol. Allied Sci. 2003, 28, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.; Naraghi, R.; Zumbrunn, T.; Rösch, J.; Hastreiter, P.; Dörfler, A. High-resolution 3D-constructive interference in steady-state MR imaging and 3D time-of-flight MR angiography in neurovascular compression: A comparison between 3T and 1.5T. AJNR. Am. J. Neuroradiol. 2012, 33, 1251–1256. [Google Scholar] [CrossRef] [Green Version]
- Henneberger, A.; Ertl-Wagner, B.; Reiser, M.; Gürkov, R.; Flatz, W. Morphometric evaluation of facial and vestibulocochlear nerves using magnetic resonance imaging: Comparison of Menière’s disease ears with normal hearing ears. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 3029–3039. [Google Scholar] [CrossRef]
- Peng, L.; Xiao, Y.; Liu, L.; Mao, Z.; Chen, Q.; Zhou, L.; Liao, B.; Liu, A.; Wang, X. Evaluation of cochlear nerve diameter and cross-sectional area in ANSD patients by 3.0-Tesla MRI. Acta Oto-Laryngol. 2016, 136, 792–799. [Google Scholar] [CrossRef]
- Özdemir, M.; Kavak, R.P. Morphometric analysis of facial and cochlear nerves in normal-hearing ears using 3D-CISS. J. Otol. 2019, 14, 136–140. [Google Scholar] [CrossRef]
- Nishihara, M.; Noguchi, T.; Kawashima, M.; Azama, S.; Matsushima, K.; Irie, H. Magnetic Resonance (MR) Imaging Assessment for Glossopharyngeal Neuralgia: Value of Three-Dimensional T2-Reversed MR Imaging (3D-T2R) in Conjunction with Other Modes of 3D MR Imaging. Pol. J. Radiol. 2017, 82, 638–644. [Google Scholar] [CrossRef]
- Moon, W.J.; Roh, H.G.; Chung, E.C. Detailed MR imaging anatomy of the cisternal segments of the glossopharyngeal, vagus, and spinal accessory nerves in the posterior fossa: The use of 3D balanced fast-field echo MR imaging. AJNR. Am. J. Neuroradiol. 2009, 30, 1116–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yousry, I.; Moriggl, B.; Schmid, U.D.; Wiesman, M.; Fesl, G.; Brückmann, H.; Naidich, T.P.; Yousry, T.A. Detailed anatomy of the intracranial segment of the hypoglossal nerve: Neurovascular relationships and landmarks on magnetic resonance imaging sequences. J. Neurosurg. 2002, 96, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, B.E.; Khafagi, A. Combined HRCT and MRI in the detection of CSF rhinorrhea. Skull Base 2004, 14, 157–162, discussion 162. [Google Scholar] [CrossRef] [Green Version]
- Vemuri, N.V.; Karanam, L.S.P.; Manchikanti, V.; Dandamudi, S.; Puvvada, S.K.; Vemuri, V.K. Imaging review of cerebrospinal fluid leaks. Indian J. Radiol. Imaging 2017, 27, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Ye, G.; Liu, Y.; Wang, Q.; Li, S.; Wang, Y. Clinical application of high-resolution MRI in combination with digital subtraction angiography in the diagnosis of vertebrobasilar artery dissecting aneurysm: An observational study (STROBE compliant). Medicine 2019, 98, e14857. [Google Scholar] [CrossRef] [PubMed]
- Almaghrabi, N.; Fatani, Y.; Saab, A. Cavernous internal carotid artery aneurysm presenting with ipsilateral oculomotor nerve palsy: A case report. Radiol. Case Rep. 2021, 16, 1339–1342. [Google Scholar] [CrossRef]
- Hirai, T.; Kai, Y.; Morioka, M.; Yano, S.; Kitajima, M.; Fukuoka, H.; Sasao, A.; Murakami, R.; Nakayama, Y.; Awai, K.; et al. Differentiation between paraclinoid and cavernous sinus aneurysms with contrast-enhanced 3D constructive interference in steady- state MR imaging. AJNR. Am. J. Neuroradiol. 2008, 29, 130–133. [Google Scholar] [CrossRef] [Green Version]
- Zausinger, S.; Yousry, I.; Brueckmann, H.; Schmid-Elsaesser, R.; Tonn, J.C. Cavernous malformations of the brainstem: Three-dimensional-constructive interference in steady-state magnetic resonance imaging for improvement of surgical approach and clinical results. Neurosurgery 2006, 58, 322–330. [Google Scholar] [CrossRef]
- Sparing, R.; Harrer, J.U.; Spuentrup, E.; Krings, T. MR-imaging of thrombus in extra- and intracranial arteries employing balanced fast-field echo MRI. Neuroradiology 2004, 46, 973–977. [Google Scholar] [CrossRef]
- Mormina, E.; Caragliano, A.A.; Tessitore, A.; Cavallaro, M.; Buonomo, O.; Visalli, C.; Pitrone, A.; Velo, M.; Galletta, K.; Longo, M.; et al. Fusion of magnetic resonance angiography and cisternography in acute ischemic stroke reveals the vessel anatomy ahead of the clot: A technical note to see beyond obstacles. Neuroradiology 2022, 64, 1457–1460. [Google Scholar] [CrossRef]
- Mormina, E.; Tessitore, A.; Cavallaro, M.; Caragliano, A.A.; Buonomo, O.; Longo, M.; Granata, F.; Caponnetto, M.; Vinci, S.L. Magnetic Resonance Angiography and Cisternography fused images in acute ischemic stroke may save time during endovascular procedure revealing vessel anatomy. Heliyon 2022, 8, e10288. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Kashiwazaki, D.; Uchino, H.; Saito, H.; Akioka, N.; Kuwayama, N.; Noguchi, K.; Kuroda, S. Stenosis Severity-Dependent Shrinkage of Posterior Cerebral Artery in Moyamoya Disease. World Neurosurg. 2019, 126, e661–e670. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Kashiwazaki, D.; Akioka, N.; Kuwayama, N.; Noguchi, K.; Kuroda, S. Progressive Shrinkage of Involved Arteries in Parallel with Disease Progression in Moyamoya Disease. World Neurosurg. 2019, 122, e253–e261. [Google Scholar] [CrossRef] [PubMed]
- Morioka, T.; Hashiguchi, K.; Samura, K.; Yoshida, F.; Miyagi, Y.; Yoshiura, T.; Suzuki, S.O.; Sasaki, T. Detailed anatomy of intracranial venous anomalies associated with atretic parietal cephaloceles revealed by high-resolution 3D-CISS and high-field T2-weighted reversed MR images. Child’s Nerv. Syst. 2009, 25, 309–315. [Google Scholar] [CrossRef]
- Pandolfo, I.; Vinci, S.; Salamone, I.; Granata, F.; Mazziotti, S. Evaluation of the anterior ethmoidal artery by 3D dual volume rotational digital subtraction angiography and native multidetector CT with multiplanar reformations. Initial findings. Eur. Radiol. 2007, 17, 1584–1590. [Google Scholar] [CrossRef]
- Ucar, M.; Guryildirim, M.; Tokgoz, N.; Kilic, K.; Borcek, A.; Oner, Y.; Akkan, K.; Tali, T. Evaluation of aqueductal patency in patients with hydrocephalus: Three-dimensional high-sampling-efficiency technique (SPACE) versus two-dimensional turbo spin echo at 3 Tesla. Korean J. Radiol. 2014, 15, 827–835. [Google Scholar] [CrossRef] [Green Version]
- Kurihara, N.; Takahashi, S.; Tamura, H.; Higano, S.; Furuta, S.; Jokura, H.; Umetsu, A. Investigation of hydrocephalus with three-dimensional constructive interference in steady state MRI. Neuroradiology 2000, 42, 634–638. [Google Scholar] [CrossRef]
- Algin, O.; Hakyemez, B.; Parlak, M. Phase-contrast MRI and 3D-CISS versus contrast-enhanced MR cisternography on the evaluation of the aqueductal stenosis. Neuroradiology 2010, 52, 99–108. [Google Scholar] [CrossRef]
- Spennato, P.; Chiaramonte, C.; Cicala, D.; Donofrio, V.; Barbarisi, M.; Nastro, A.; Mirone, G.; Trischitta, V.; Cinalli, G. Acute triventricular hydrocephalus caused by choroid plexus cysts: A diagnostic and neurosurgical challenge. Neurosurg. Focus 2016, 41, E9. [Google Scholar] [CrossRef] [Green Version]
- Arslan, A.; Başarır, M.; Özek, M.M.; Dinçer, A. Postoperative patency assessment of Cystocisternostomy and Cystoventriculostomy stomas in cases with Arachnoidal cyst. Child’s Nerv. Syst. 2020, 36, 1415–1423. [Google Scholar] [CrossRef]
- Shi, J.; Fu, W.; Wu, Q.; Zhang, H.; Zheng, Z.; Zhu, J. Endoscopic third ventriculostomy associated 3D-construcive inference steady state MRI for obstructed hydrocephalus: A retrospective study. Clin. Neurol. Neurosurg. 2013, 115, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Da Costa Val Filho, J.A.; da Silva Gusmão, S.N.; Furtado, L.M.F.; de Macedo Machado Filho, G.; Maciel, F.L.A. The role of the Liliequist membrane in the third ventriculostomy. Neurosurg. Rev. 2021, 44, 3375–3385. [Google Scholar] [CrossRef] [PubMed]
- Fushimi, Y.; Miki, Y.; Ueba, T.; Kanagaki, M.; Takahashi, T.; Yamamoto, A.; Haque, T.L.; Konishi, J.; Takahashi, J.A.; Hashimoto, N.; et al. Liliequist membrane: Three-dimensional constructive interference in steady state MR imaging. Radiology 2003, 229, 360–365, discussion 365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, D.A.; Castro, F.L.; Yared, J.H.; Lucas Júnior, A.; Ferreira Filho, L.A.; Ferreira, N.F. Liliequist membrane: Radiological evaluation, clinical and therapeutic implications. Radiol. Bras. 2014, 47, 182–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madhugiri, V.S.; Gundamaneni, S.K.; Yadav, A.K.; Sasidharan, G.M.; Roopesh, K.V. Idiopathic intraventricular aneurysm presenting with intraventricular hemorrhage: Case report and review of the literature. Pediatr. Neurosurg. 2012, 48, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Carrillo Mezo, R.; Lara García, J.; Arroyo, M.; Fleury, A. Relevance of 3D magnetic resonance imaging sequences in diagnosing basal subarachnoid neurocysticercosis. Acta Trop. 2015, 152, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Govindappa, S.S.; Narayanan, J.P.; Krishnamoorthy, V.M.; Shastry, C.H.; Balasubramaniam, A.; Krishna, S.S. Improved detection of intraventricular cysticercal cysts with the use of three-dimensional constructive interference in steady state MR sequences. AJNR. Am. J. Neuroradiol. 2000, 21, 679–684. [Google Scholar] [PubMed]
- Tamura, R.; Miwa, T.; Ohira, T.; Yoshida, K. Diagnosis and treatment for pure aqueductal tumor. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2017, 44, 260–263. [Google Scholar] [CrossRef]
- Granata, F.; Morabito, R.; Mormina, E.; Alafaci, C.; Marino, S.; Laganà, A.; Vinci, S.L.; Briguglio, M.; Calamuneri, A.; Gaeta, M.; et al. 3T Double Inversion Recovery Magnetic Resonance Imaging: Diagnostic advantages in the evaluation of cortical development anomalies. Eur. J. Radiol. 2016, 85, 906–914. [Google Scholar] [CrossRef]
- Samii, M.; Gerganov, V.M. Tumors of the cerebellopontine angle. Handb. Clin. Neurol. 2012, 105, 633–639. [Google Scholar] [CrossRef]
- Agarwal, A. Intracranial trigeminal schwannoma. Neuroradiol. J. 2015, 28, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakai, T.; Yamamoto, H.; Tanaka, K.; Koyama, J.; Fujita, A.; Taniguchi, M.; Hosoda, K.; Kohmura, E. Preoperative detection of the facial nerve by high-field magnetic resonance imaging in patients with vestibular schwannoma. Neuroradiology 2013, 55, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Unel, S.; Yilmaz, M.; Albayram, S.; Kiris, A.; Isik, Z.; Ceyhan, E.; Isildak, H.; Savas, Y.; Keser, Z. A Radiological Study on the Topographical Relationships between the Vestibular, Cochlear and Facial Nerves. Eurasian J. Med. 2012, 44, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Backer-Grøndahl, T.; Moen, B.H.; Torp, S.H. The histopathological spectrum of human meningiomas. Int. J. Clin. Exp. Pathol. 2012, 5, 231–242. [Google Scholar]
- Huang, R.Y.; Bi, W.L.; Griffith, B.; Kaufmann, T.J.; la Fougère, C.; Schmidt, N.O.; Tonn, J.C.; Vogelbaum, M.A.; Wen, P.Y.; Aldape, K.; et al. Imaging and diagnostic advances for intracranial meningiomas. Neuro-Oncology 2019, 21, i44–i61. [Google Scholar] [CrossRef]
- Ikushima, I.; Korogi, Y.; Hirai, T.; Sugahara, T.; Shigematsu, Y.; Komohara, Y.; Okuda, T.; Takahashi, M.; Ushio, Y. MR of epidermoids with a variety of pulse sequences. AJNR Am. J. Neuroradiol. 1997, 18, 1359–1363. [Google Scholar]
- Awaji, M.; Okamoto, K.; Nishiyama, K. Magnetic resonance cisternography for preoperative evaluation of arachnoid cysts. Neuroradiology 2007, 49, 721–726. [Google Scholar] [CrossRef]
- Brodsky, J.R.; Smith, T.W.; Litofsky, S.; Lee, D.J. Lipoma of the cerebellopontine angle. Am. J. Otolaryngol. 2006, 27, 271–274. [Google Scholar] [CrossRef]
- Gombert, M.; Mailleux, P. Cerebellopontine Angle Lipoma Associated to Dysplastic Labyrinth. J. Belg. Soc. Radiol. 2018, 102, 43. [Google Scholar] [CrossRef] [Green Version]
- Hirai, T.; Korogi, Y.; Shigematsu, Y.; Sugahara, T.; Takahashi, M.; Ushio, Y.; Uemura, S. Evaluation of syringomyelia with three-dimensional constructive interference in a steady state (CISS) sequence. J. Magn. Reson. Imaging JMRI 2000, 11, 120–126. [Google Scholar] [CrossRef]
- Yamura, M.; Hirai, T.; Korogi, Y.; Kitajima, M.; Hayashida, Y.; Ikushima, I.; Endo, F.; Yamashita, Y. Evaluation of small hypothalamic hamartomas with 3D constructive interference in steady state (CISS) sequence. Neuroradiology 2005, 47, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Godano, E.; Morana, G.; Di Iorgi, N.; Pistorio, A.; Allegri, A.E.M.; Napoli, F.; Gastaldi, R.; Calcagno, A.; Patti, G.; Gallizia, A.; et al. Role of MRI T2-DRIVE in the assessment of pituitary stalk abnormalities without gadolinium in pituitary diseases. Eur. J. Endocrinol. 2018, 178, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Dawes, B.H.; Lloyd, R.A.; Rogers, J.M.; Magnussen, J.S.; Bilston, L.E.; Stoodley, M.A. Cerebellar Tissue Strain in Chiari Malformation with Headache. World Neurosurg. 2019, 130, e74–e81. [Google Scholar] [CrossRef] [PubMed]
- Byun, J.S.; Kim, H.J.; Yim, Y.J.; Kim, S.T.; Jeon, P.; Kim, K.H.; Kim, S.S.; Jeon, Y.H.; Lee, J. MR imaging of the internal auditory canal and inner ear at 3T: Comparison between 3D driven equilibrium and 3D balanced fast field echo sequences. Korean J. Radiol. 2008, 9, 212–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.J.; Song, J.W.; Chon, K.M.; Goh, E.K. Common crus aplasia: Diagnosis by 3D volume rendering imaging using 3DFT-CISS sequence. Clin. Radiol. 2004, 59, 830–834. [Google Scholar] [CrossRef]
- Fadzli, F.; Ramli, N.M.; Rahmat, K.; Ganesan, D. Neonatal post-hemorrhagic hydrocephalus resulting in foraminal septae-radiological technique and surgical implications. Child’s Nerv. Syst. 2013, 29, 159–162. [Google Scholar] [CrossRef]
- Siow, T.Y.; Chuang, C.C.; Toh, C.H.; Castillo, M. Persisting Embryonal Infundibular Recess: Case Report and Imaging Findings. World Neurosurg. 2018, 117, 11–14. [Google Scholar] [CrossRef]












Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavallaro, M.; Coglitore, A.; Tessitore, A.; Galletta, K.; Frosina, L.; Cuffari, A.; Ingrassia, R.; Scarcella, S.C.; Caponnetto, M.; Longo, M.; et al. Three-Dimensional Constructive Interference in Steady State (3D CISS) Imaging and Clinical Applications in Brain Pathology. Biomedicines 2022, 10, 2997. https://doi.org/10.3390/biomedicines10112997
Cavallaro M, Coglitore A, Tessitore A, Galletta K, Frosina L, Cuffari A, Ingrassia R, Scarcella SC, Caponnetto M, Longo M, et al. Three-Dimensional Constructive Interference in Steady State (3D CISS) Imaging and Clinical Applications in Brain Pathology. Biomedicines. 2022; 10(11):2997. https://doi.org/10.3390/biomedicines10112997
Chicago/Turabian StyleCavallaro, Marco, Alessandra Coglitore, Agostino Tessitore, Karol Galletta, Luciano Frosina, Antonino Cuffari, Roberta Ingrassia, Sarah Caroline Scarcella, Michele Caponnetto, Mirta Longo, and et al. 2022. "Three-Dimensional Constructive Interference in Steady State (3D CISS) Imaging and Clinical Applications in Brain Pathology" Biomedicines 10, no. 11: 2997. https://doi.org/10.3390/biomedicines10112997